
Abstract
Cognitive dysfunction syndrome (CDS) or canine dementia represents a serious health problem for aged dogs, regardless of breed. CDS is characterised by deficits in learning, memory and spatial awareness, as well as changes to social interaction and sleeping patterns. Several studies, using owner-based observational questionnaires, have been performed to assess the severity of the disease or to identify first clinical symptoms before the onset of full-fledged dementia. Questionnaires include a broad range of items measuring appetite, drinking behaviour, barking, elimination behaviour, day/night rhythms, aimless behaviour, adaptive capabilities, social behaviour, perceptual ability, disorientation, memory, and personality changes. It is important to note that canine dementia probably does not represent a single disease entity; rather, it may have various phenotypic presentations. Generally, the cognitive impairment and other clinical features of CDS gradually worsen as the disease progresses. It is generally accepted that at least three main stages of the disease—mild, moderate, and severe—can be recognised. Despite this fact, there is no consensus regarding the thresholds for discrimination of various stages. This chapter will guide the reader through the current knowledge on the clinical variability and staging of canine dementia.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Cognitive dysfunction syndrome (CDS) or canine dementia represents a serious health problem for aged dogs, regardless of breed. CDS is characterised by deficits in learning, memory and spatial awareness, as well as changes to social interaction and sleeping patterns. Several studies, using owner-based observational questionnaires, have been performed to assess the severity of the disease or to identify first clinical symptoms before the onset of full-fledged dementia. Questionnaires include a broad range of items measuring appetite, drinking behaviour, barking, elimination behaviour, day/night rhythms, aimless behaviour, adaptive capabilities, social behaviour, perceptual ability, disorientation, memory, and personality changes. It is important to note that canine dementia probably does not represent a single disease entity; rather, it may have various phenotypic presentations. Generally, the cognitive impairment and other clinical features of CDS gradually worsen as the disease progresses. It is generally accepted that at least three main stages of the disease—mild, moderate, and severe—can be recognised. Despite this fact, there is no consensus regarding the thresholds for discrimination of various stages. This chapter will guide the reader through the current knowledge on the clinical variability and staging of canine dementia.
3.1 The Clinical Picture of Canine Dementia in a Nutshell
The cognitive decline and behavioural presentation of canine cognitive dysfunction syndrome (CDS) indicates similarity in dementia syndromes between pets and humans (Landsberg and Araujo 2005). The classic clinical signs of CDS are disorientation, interaction changes (such as decline in response to learned commands), sleep and wakefulness cycle changes, change in hygiene habits and house soiling, and activity changes (DISHA) (Landsberg et al. 2012). A drop in capability and adaptability is evident, generally accompanied by increased rates of anxiety and repetitive behaviour (Gunn-Moore 2011). Unambiguous identification of behavioural characteristics for cognitive decline can allow early intervention, delaying progression of the disease (Dowling and Head 2012).
3.1.1 Disorientation and Activity Changes
Demented dogs display aimless wandering and pacing, which, along with a reduction of spatial orientation and growing confusion, can cause the animal to become trapped in corners or behind furniture (Gonzalez-Martinez et al. 2011). A commonly seen problem is distinguishing between internal and external doors, such as going to the wrong side of the door upon arrival and departure (Landsberg and Araujo 2005). Dogs often ask to go out, but, once outside, disorientation becomes apparent once the impaired animal is a short distance from its home, manifesting in anxiety and confusion about the return route (Landsberg et al. 2012).
3.1.2 Changes in Social Interactions
Social interaction between dog and man is one of the pivotal aspects where canine dementia becomes apparent (Madari et al. 2015). Interactions of the dog with family members become less frequent and/or less intense. Social behaviour abnormalities become apparent in the expression of greetings or in association with feeding behaviours. Greeting behaviour patterns are incomplete in their expression, with pets showing disorientation in response to owners’ attempts to interact with them or repeating greeting behaviour without previous separation time. Dogs may appear confused or even frightened by welcoming rituals. Dogs may beg for food but refuse to eat, begging to be fed once more a few minutes later. Behavioural patterns lasting a few minutes, sometimes hours or even the whole day, are repeated, which is especially noticeable with vocalisation and destructive behaviours. These social changes are manifestations of confusion and anxiety, similar to human dementia (Gunn-Moore et al. 2007). Confusion is considered to be one of the main features of CDS (Azkona et al. 2009).
3.1.3 Sleep and Wakefulness Cycle Changes
Sleep-wake cycle changes may be observed especially in later stages of the disease. Dogs might sleep more during the day but are active during the night. These changes are often associated with excessive anxiety-driven vocalisation, such as barking or howling. Demented dogs may wander, pace, or even scratch the ground. This behaviour is especially burdensome to owners and their surroundings (Landsberg and Araujo 2005; Landsberg et al. 2012).
3.1.4 Changes in Hygiene Habits
The loss of learned behaviours, such as toilet training, represents the most common sign attributable to CDS. Uncontrolled indoor elimination occurs in the absence of apparent medical problems or environmental changes (such as lack of access to an appropriate area) that would prevent the dog from following its toilet training. The dog may eliminate even when the owner is present. Soiling may occur in random locations (Neilson et al. 2001; Azkona et al. 2009; Landsberg and Araujo 2005).
To summarise, CDS represents a disorder with a very broad spectrum of clinical symptoms, ranging from memory impairment to changes in hygiene habits. These changes profoundly disturb the bond between dog and human by diminishing meaningful interaction between them (whether it was for the purpose of companionship or for professional use) on one hand and, on the other hand, by increasing the incidence of unmanageable disturbing behaviour (such as house soiling) (Osella et al. 2007; Salvin et al. 2011; Landsberg et al. 2012).
3.2 Questionnaires: A Double-Edged Sword in the Diagnostics of CDS
A variety of scales and questionnaires are used to diagnose and evaluate cognitive decline in pets. Generally, they constitute useful tools for the acquisition of information about the cognitive function of aged dogs and prevalence of cognitive decline in the domestic canine population. Many different questionnaires have been created (Colle et al. 2000; Neilson et al. 2001; Osella et al. 2007; Azkona et al. 2009, Salvin et al. 2011; Landsberg et al. 2012; Madari et al. 2015) since initial efforts by Ruehl et al. (1995). Questionnaires include a broad range of items measuring appetite, drinking behaviour, barking, elimination behaviour, day/night rhythms, aimless behaviour, adaptive capabilities, social behaviour, perceptual ability, disorientation, memory and personality changes (Table 3.1).
One of the main weaknesses of the questionnaires is the subjective evaluation of the dog’s cognitive status made by a pet owner (Salvin et al. 2011). The use of the pet owner as untrained evaluator of behavioural changes represents an impactful source of inaccurateness. Several extensive studies on CDS were based either on phone consultations with dog owners (Neilson et al. 2001) or on distribution of a questionnaire via online or hard copy formats (Salvin et al. 2011). While the advantage of these approaches lies in large datasets, the main limitations of this approach are a lack of systematic control for potential impact of other disorders on the cognitive decline, and the subjective nature of evaluations performed by pet owners (Madari et al. 2015).
Another issue that should be taken into consideration is how individual items addressed by the questionnaire are quantified. Some authors prefer to use item scoring that reflects the degree of abnormal behaviour (Colle et al. 2000; Pugliese et al. 2005), while others aim to quantify the frequency of their occurrence using either four- or five-point frequency scales (Osella et al. 2007; Salvin et al. 2011). Salvin et al. (2011) proposed a 5-point scale based on the frequency of abnormal behaviour: 1 point—never, 2 points—once a month, 3 points—once a week, 4 points—once a day and 5 points—more than once a day. Similarly, we have proposed a 5-point scale for easy evaluation of behaviour: 0 point—abnormal behaviour of the dog was never observed, 2 points—abnormal behaviour of the dog was detected at least once within the last 6 months, 3 points—abnormal behaviour appeared at least once per month, 4 points—abnormal behaviour was seen several times per month, and 5 points—abnormal behaviour was observed several times a week (Madari et al. 2015).
To sum up, questionnaires serve as valuable tool for detection of disease severity and are a helpful screening tool for identification of early behavioural changes. Finally, they can quantify the level of impairment of various cognitive domains.
3.3 CDS Clinical Staging
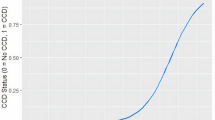
As mentioned above, CDS may progress through several stages. A few studies have focused on clinical staging of cognitive decline. Based on the level of cognitive impairment, Pugliese et al. (2005) divided dogs into three groups: normal, light cognitive deficits and severe cognitive deficits. Unfortunately, this approach does not reflect the frequency of abnormal behaviour. Azkona et al. (2009) classified cognitive impairment into mild (one behavioural domain), moderate (two domains) or severe (three or four domains). This classification could be sometimes misleading, because the number of impaired categories does not necessarily precisely reflect the degree of cognitive decline. We found that two and sometimes three categories of cognition can be slightly impaired already in cognitively normal or mildly affected dogs (see Table 3.2).
We have proposed criteria for discrimination of three stages of the disease: mild cognitive impairment, moderate cognitive impairment, and severe cognitive impairment (the last stage being full-fledged canine dementia). For evaluation of the severity of the disease, we have used a universally applicable scale for diagnostics of the canine cognitive dysfunction syndrome—CADES—which contains 17 items distributed into four domains (spatial orientation, social interactions, sleep-wake cycles, and house soiling) related to changes in dogs' behaviour. Staging criteria for detection of the severity of disease were based on the severity of behavioural changes, the number of affected domains, and total scores (Madari et al. 2015).
We have described normal ageing as a clinical status when dog owners usually do not notice any apparent changes in their pets’ behaviour. The number of affected domains varies from 0 to 2. Early behavioural changes appear occasionally (Table 3.3).
Similarly, in the case of mild cognitive impairment, pet owners often do not recognise any changes in their pets’ behaviour. Evaluation and interview by a veterinary clinician can identify very mild changes of the dog’s behaviour, particularly alterations in interaction with owners or other pets, reduction in activity during the day and increased activity at night and, rarely, inappropriate indoor elimination. The number of slightly affected domains varies from 2 to 4.
When CDS progresses into the stage of moderate cognitive impairment, pet owners may observe salient behavioural changes, such as undesirable indoor elimination (urination, defaecation) or hyperactivity through the night. At this stage, dogs require more care than ever before. The number of affected domains varies from 2 to 4.
In the final stage, severe cognitive impairment or canine dementia, pet owners report severe detrimental changes in behaviour, which markedly impair the quality of the coexistence between owner and dog. All four domains were affected, some of them heavily. A majority of animals shows apparent decline (over 10 points per domain) either in three or four domains. The CADES score was higher than 45 points.
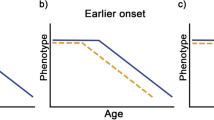
3.4 The Phenotypic Variability of CDS
CDS encompasses a broad spectrum of clinical symptoms, and not all of them are present in all senior dogs. The variability in the clinical presentation is most probably caused by selective damage to various brain areas. Variations in phenotype were described in some studies (Madari et al. 2015; Schutt et al. 2015). Although the authors used different questionnaires, both studies demonstrated the existence of a range of individual phenotypic patterns. In our study, we found that 57.1% of dogs suffering from moderate cognitive impairment had severely impaired social interactions and sleep-wake cycles, 26% were impaired only in social interactions, 8.2% displayed impairment of both spatial orientation and social interaction, and 8.2% showed impairment exclusively in sleep-wake cycles. Of the 38 dogs suffering from severe cognitive dysfunction included in the study, 26.7% demonstrated concurrent impairment in spatial orientation, social interaction and sleep-wake cycles, and 26.7% in all four domains. Our results showed that social interactions and sleep-wake cycles were the most impaired categories (Madari et al. 2015). These findings indicate CDS is a multifarious disorder affecting various behavioural domains; with increasing severity of the disorder, more domains become affected.
The variety of clinical manifestations can be explained by variation in the distribution of pathological changes in different brain areas and selective vulnerability of said areas. From a plethora of studies on human dementia patients (Braak and Braak 1991; Neary et al. 1998; Mackenzie et al. 2010; Josephs et al. 2011), we know that the frontal and temporal cortices, as well as the hippocampus and entorhinal cortex represent the brain areas that are most vulnerable to neurodegeneration. Further studies are warranted to explore the direct relationship between the extent of the damage in specific brain areas and phenotypic patterns of canine dementia.
3.5 Summary
Canine dementia constitutes an unmet medical need. The number of dogs suffering from dementia rises quickly because we have prolonged the lifespan of dogs and cats. Current diagnostic approaches utilise various forms of questionnaires that can identify the disease in early stages of development. CDS passes through several stages from mild, moderate to severe cognitive impairment. CDS seems to have a slightly variable phenotype, which may differ between demented dogs. Taking these findings into consideration allows therapy to be started in the earliest stages of the disease.
References
Azkona G, Garcia-Belenguer S, Chacon G, Rosado B, Leon M, Palacio J (2009) Prevalence and risk factors of behavioural changes associated with age-related cognitive impairment in geriatric dogs. J Small Animal Pract 50(2):87–91
Braak H, Braak E (1991) Neuropathological staging of Alzheimer-related changes. Acta Neuropathol 82(4):239–259
Colle MA, Hauw JJ, Crespeau F, Uchihara T, Akiyama H, Checler F, Pageat P, Duykaerts C (2000) Vascular and parenchymal A beta deposition in the aging dog: correlation with behavior. Neurobiol Aging 21:695–704
Dowling ALS, Head E (2012) Antioxidants in the canine model of human aging. Biochimica Et Biophysica Acta-Mol Basis Dis 1822(5):685–689
Fast R, Schutt T, Toft N, Moller A, Berendt M (2013) An observational study with long-term follow-up of canine cognitive dysfunction: clinical characteristics, survival, and risk factors. J Veterinary Intern Med 27(4):822–829
Golini L, Colangeli R, Tranquillo V, Mariscoli M (2009) Association between neurologic and cognitive dysfunction signs in a sample of aging dogs. J Veterinary Behav-Clin Appl Res 4:25–30
Gonzalez-Martinez A, Rosado B, Pesini P, Suarez ML, Santamarina G, Garcia-Belenguer S, Villegas A, Monleon I, Sarasa M (2011) Plasma beta-amyloid peptides in canine aging and cognitive dysfunction as a model of Alzheimer’s disease. Exp Gerontol 46(7):590–596
Gunn-Moore DA (2011) Cognitive dysfunction in cats: clinical assessment and management. Topics Companion Animal Med 26(1):17–24
Gunn-Moore D, Moffat K, Christie LA, Head E (2007) Cognitive dysfunction and the neurobiology of ageing in cats. J Small Animal Pract 48(10):546–553
Josephs KA, Hodges JR, Snowden JS, Mackenzie IR, Neumann M, Mann DM, Dickson DW (2011) Neuropathological background of phenotypical variability in frontotemporal dementia. Acta Neuropathol 122:137–153
Landsberg G, Araujo JA (2005) Behavior problems in geriatric pets. Veterinary Clin N Am-Small Animal Pract 35(3):675–698
Landsberg GM, Nichol J, Araujo JA (2012) Cognitive dysfunction syndrome a disease of canine and feline brain aging. Veterinary Clin N Am-Small Animal Pract 42(4):749–768
Mackenzie IR, Neumann M, Bigio EH, Cairns NJ, Alafuzoff I, Kril J, Kovacs GG, Ghetti B, Halliday G, Holm IE, Ince PG, Kamphorst W, Revesz T, Rozemuller AJ, Kumar-Singh S, Akiyama H, Baborie A, Spina S, Dickson DW, Trojanowski JQ, Mann DM (2010) Nomenclature and nosology for neuropathologic subtypes of frontotemporal lobar degeneration: an update. Acta Neuropathol 119:1–4
Madari A, Farbakova J, Katina S, Smolek T, Novak P, Weissova T, Novak M, Zilka N (2015) Assessment of severity and progression of canine cognitive dysfunction syndrome using the CAnine DEmentia Scale (CADES). Appl Animal Behav Sci 171:138–145
Neary D, Snowden JS, Gustafson L, Passant U, Stuss D, Black S, Freedman M, Kertesz A, Robert PH, Albert M, Boone K, Miller BL, Cummings J, Benson DF (1998) Frontotemporal lobar degeneration: a consensus on clinical diagnostic criteria. Neurology 51:1546–1554
Neilson JC, Hart BL, Cliff KD, Ruehl WW (2001) Prevalence of behavioral changes associated with age-related cognitive impairment in dogs. J Am Veterinary Med Assoc 218(11):1787–1791
Osella MC, Re G, Odore R, Girardi C, Badino P, Barbero R, Bergamasco L (2007) Canine cognitive dysfunction syndrome: prevalence, clinical signs and treatment with a neuroprotective nutraceutical. Appl Animal Behav Sci 105(4):297–310
Pugliese M, Carrasco JL, Andrade C, Mas E, Mascort J, Mahy N (2005) Severe cognitive impairment correlates with higher cerebrospinal fluid levels of lactate and pyruvate in a canine model of senile dementia. Progr Neuro-Psychopharmacol Biol Psychiatry 29:603–610
Rosado B, Gonzalez-Martinez A, Pesini P, Garcia-Belenguer S, Palacio J, Villegas A, Suarez ML, Santamarina G, Sarasa M (2012) Effect of age and severity of cognitive dysfunction on spontaneous activity in pet dogs—part 1: locomotor and exploratory behaviour. Veterinary J 194(2):189–195
Ruehl WW, Bruyette DS, DePaoli A, Cotman CW, Head E, Milgram NW, Cummings BJ (1995) Canine cognitive dysfunction as a model for human age-related cognitive decline, dementia and Alzheimer’s disease: clinical presentation, cognitive testing, pathology and response to 1-deprenyl therapy. Curr Neurochem Pharmacol Aspects of Biogenic Amines 106:217–225
Salvin HE, McGreevy PD, Sachdev PS, Valenzuela MJ (2011) The canine cognitive dysfunction rating scale (CCDR): a data-driven and ecologically relevant assessment tool. Veterinary J 188:331–336
Schutt T, Toft N, Berendt M (2015) Cognitive function, progression of age-related behavioral changes, biomarkers, and survival in dogs more than 8 years old. J Veterinary Intern Med 29(6):1569–1577
Acknowledgement
The work was funded by APVV-15-0613 and APVV-14-0872 and VEGA grant 2/0164/16.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Mad’ari, A., Novak, P., Žilka, N. (2017). Phenotypic Variability and Clinical Staging of Canine Dementia. In: Landsberg, G., Maďari, A., Žilka, N. (eds) Canine and Feline Dementia. Springer, Cham. https://doi.org/10.1007/978-3-319-53219-6_3
Download citation
DOI: https://doi.org/10.1007/978-3-319-53219-6_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-53218-9
Online ISBN: 978-3-319-53219-6
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)