
Abstract
70-year-old man was evaluated with secretin-stimulated magnetic resonance cholangiopancreatography (MRCP).
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
Clinical History
70-year-old man was evaluated with secretin-stimulated magnetic resonance cholangiopancreatography (MRCP).
Imaging Findings
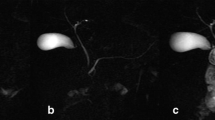
Thick-slab coronal magnetic resonance cholangiopancreatography (MRCP) images before and after the intravenous administration of secretin (Fig. 1) demonstrate progressive increased signal in the pancreas (Fig. 1, thin arrows) over 5 min. There is increase in, and subsequent distal transit of, fluid within the proximal small bowel (thick arrows) as well as progressive increase in diameter of the main pancreatic duct.

Fig. 1
Differential Diagnosis
Normal exocrine pancreatic response to secretin and abnormal “acinarization” of the pancreas in response to secretin.
Diagnosis
Abnormal acinarization of the pancreas in response to secretin.
Discussion
There are a number of important complications of chronic pancreatitis. Some of these complications are well evaluated by secretin-stimulated magnetic resonance cholangiopancreatography (MRCP) imaging, including pancreatic exocrine dysfunction and pancreatic ductal abnormalities. Secretin is an endogenous peptide hormone (commercially available in synthetic form) that induces increased secretions from the stomach and pancreas. The intravenous administration of secretin has been shown to improve the diagnostic yield of MRCP imaging being performed for evaluation of patients with recurrent or chronic pancreatitis [1,2,3].
A normal secretin-stimulated MRCP examination will demonstrate an increase in secretion from the pancreas into the proximal small bowel such that fluid signal in the small bowel lumen will increase and gradually involve more distal aspects of the small bowel on serial dynamic images. During secretin stimulation, the main pancreatic duct may slightly enlarge as the volume of secretions passing through the duct increases. Changes that can be observed in secretin-stimulated studies include loss of exocrine function with consequent decrease in amount or progression of fluid within the small bowel lumen, accentuation of the main pancreatic duct upstream from a stricture or other intraductal obstructing lesion, and enlargement of cystic lesions that communicate with the pancreatic duct [4].
Acinarization refers to increased T2 signal on either side of the main pancreatic duct in response to exogenous secretin on a secretin-stimulated MRCP examination (Fig. 1). Acinarization may occur when the duct fluid is unable to freely pass into the duodenum in the presence of adequate secretin response by the acinar cells [3]. This phenomenon was initially described with ERCP when the filling of contrast exceeds the ductal capacity and is associated with an increased incidence of post-ERCP pancreatitis [5]. Faint acinarization can be seen as a part of the normal pancreatic response to secretin. However, intense acinarization may occur in patients with increased pressure in the pancreatic duct in patients with sphincter of Oddi dysfunction, ampullary obstruction due to ductal strictures, obstructing lesions such as ampullary neoplasms or calculi, or patients with pancreas divisum [3].
The patient illustrated above was diagnosed with ampullary stenosis.
Teaching Point
Intense acinarization may occur in patients with increased pressure in the pancreatic duct in patients with sphincter of Oddi dysfunction, ampullary obstruction due to ductal strictures, obstructing lesions such as ampullary tumors or calculi, or patients with pancreas divisum.
References
Manikkavasakar S, AlObaidy M, Busireddy KK, Ramalho M, Nilmini V, Alagiyawanna M, et al. Magnetic resonance imaging of pancreatitis: an update. World J Gastroenterol. 2014;20(40):14760–77. doi:10.3748/wjg.v20.i40.14760.
Sanyal R, Stevens T, Novak E, Veniero JC. Secretin-enhanced MRCP: review of technique and application with proposal for quantification of exocrine function. AJR Am J Roentgenol. 2012;198(1):124–32. doi:10.2214/AJR.10.5713.
Sandrasegaran K, Bodanapally U, Cote GA, Benzinger S, Patel AA, Akisik FM, et al. Acinarization (parenchymal blush) observed during secretin-enhanced MRCP: clinical implications. AJR Am J Roentgenol. 2014;203(3):607–14. doi:10.2214/AJR.13.11414.
Tirkes T, Sandrasegaran K, Sanyal R, Sherman S, Schmidt CM, Cote GA, et al. Secretin-enhanced MR cholangiopancreatography: spectrum of findings. Radiographics. 2013;33(7):1889–906. doi:10.1148/rg.337125014.
Manes G, Di Giorgio P, Repici A, Macarri G, Ardizzone S, Porro GB. An analysis of the factors associated with the development of complications in patients undergoing precut sphincterotomy: a prospective, controlled, randomized, multicenter study. Am J Gastroenterol. 2009;104(10):2412–7. doi:10.1038/ajg.2009.345.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Rowe, S.P. (2017). Case 94: Abnormal Acinarization of the Pancreas in Response to Secretin. In: Zaheer, A., Fishman, E., Pittman, M., Hruban, R. (eds) Pancreatic Imaging. Springer, Cham. https://doi.org/10.1007/978-3-319-52680-5_94
Download citation
DOI: https://doi.org/10.1007/978-3-319-52680-5_94
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-52678-2
Online ISBN: 978-3-319-52680-5
eBook Packages: MedicineMedicine (R0)