
Abstract
Radial head fractures are common following traumatic injuries to the elbow. They may occur in isolation or associated with several complex injuries of the elbow. The Mason classification is commonly used to classify radial head fractures. Treatment of isolated nondisplaced radial head fractures is often nonoperative. Operative treatment involved radial head resection, open reduction and internal fixation, or radial head arthroplasty.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
Overview
-
Occur in approximately 20% of elbow trauma [1]
-
Associated elbow injuries [1]
-
Terrible triad – elbow dislocation, radial head fracture, and coronoid fracture
-
Carpal fractures
-
Essex-Lopresti – distal radioulnar joint and interosseous membrane disruption
-
Monteggia fracture-dislocation
-
Capitellar fracture
-
Associated ligamentous injury about the elbow
-
Anatomy
-
Inherent stability of the elbow conferred with bony articulation.
-
Radial head serves as an important valgus stabilizer of the elbow.
-
Radial head has two articulations, the radiocapitellar joint and proximal radioulnar joint.
-
Medial collateral ligamentous complex and the lateral collateral ligamentous complex are important stabilizers to the elbow.
-
Musculotendinous structures, fascia, and capsule also contribute to stability.
Classification
-
Mason classification [2] – has been subsequently modified by many authors

Mason type II partial articular fracture of the radial head

Mason type III comminuted and displaced fracture of the radial head
Evaluation
History
-
Vast majority of radial head fractures result from a fall onto an outstretched hand [1].
Physical Examination
-
Inspection for ecchymosis, edema, or open wounds over the lateral aspect of the elbow
-
Palpation over the radial head may elicit pain
-
Limitation of elbow range of motion secondary to pain or mechanical block may be present
-
Neurovascular examination
-
Radiocapitellar joint aspiration of hematoma and injection of local anesthetic can be helpful to determine if there is a mechanical block to range of motion [1].
Imaging
-
Typically orthogonal plain radiographs are sufficient for diagnosis and determining treatment.
-
On the lateral radiograph, elevation of the anterior or posterior fat pad from intra-articular hemarthrosis may be the only indication of a nondisplaced radial head fracture [1].
-
Radiocapitellar view can be helpful to evaluate for radial head fractures.
-
CT scan can be useful to evaluate associated injuries.
Treatment
Nonoperative
-
Indicated in isolated nondisplaced to minimally displaced isolated radial head fractures with no mechanical block to range of motion
-
Fractures involving less than one third of the articular surface may be treated with early mobilization [1].
-
Fractures involving more than one third of the articular surface should be treated with a splint or sling for 2 weeks followed by progressive functional activity [1].
Operative
-
Resection of the radial head
-
Open reduction and internal fixation (Fig. 23.3)
-
Indicated for minimally comminuted fractures with three or fewer articular fragments [5]
-
Approaches
-
Kocher approach [2]
-
Interval between the anconeus and the extensor carpi ulnaris
-
Provides greater protection of the posterior interosseous nerve than Kaplan approach
-
Lateral collateral ligament complex is at risk
-
-
Kaplan approach [2]
-
Interval between the extensor carpi radialis brevis and extensor digitorum communis
-
Posterior interosseous nerve is at risk
-
-
Common extensor tendon splitting approach [2]Incise the extensor digitorum communisThe radial collateral and annular ligaments are divided longitudinally at the midportion of the radial headInternal Fixation
-
Small screws used for internal fixation should be countersunk to avoid impinging at the proximal radioulnar joint.
-
Small plates are available for comminuted head or neck fractures.
-
The safe area for placement of implants on the nonarticular surface of the radial head can be defined as the area of the proximal radius corresponding to the region between Lister’s tubercle and the radial styloid of the distal radius [6].
-
-
-
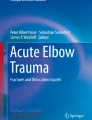
Radial head arthroplasty (Fig. 23.4)
-

Open reduction and internal fixation of the radial head (a) AP and (b) lateral

Radial head arthroplasty (a) and (b) lateral
Complications
-
Elbow stiffness
-
Heterotopic ossification
-
Posterior interosseous nerve – iatrogenic injury during exposure, may be minimized by maintain the forearm in pronated position [8]
-
Avascular necrosis
-
Nonunion
References
McKee MD, Jupiter JB. Trauma to the adult elbow and fractures of the distal humerus part I trauma to the adult elbow. In: Browner BD, et al., editors. Skeletal trauma. 4th ed. Philadelphia: Saunders Elsevier; 2009. p. 1503–41.
Ring D. Elbow fractures and dislocations. In: Bucholz RW, Heckman JD, et al., editors. Rockwood and green’s fractures in adults. 7th ed. Philadelphia: Lippincott Williams & Wilkins; 2010. p. 905–44.
Van Riet RP, et al. Radial head fracture. In: Morrey BF, editor. The elbow and its disorders. 4th ed. Philadelphia: Saunders Elsevier; 2009. p. 359–88.
Beingessner DM, et al. The effect of radial head excision and arthroplasty on elbow kinematics and stability. J Bone Joint Surg Am. 2004;86:1730–9.
Ring D, et al. Open reduction and internal fixation of fractures of the radial head. J Bone Joint Surg Am. 2002;84:1811–5.
Caputo AE, et al. The nonarticulating portion of the radial head: anatomic and clinical correlations for internal fixation. J Hand Surg [Am]. 1998;23:1082–90.
Doornberg JN, et al. Reference points for radial head prosthesis size. J Hand Surg Am. 2006;31:53–7.
Diliberti T, et al. Anaromical considerations regarding the posterior interosseous nerve during posterolateral approaches to the proximal part of the radius. J Bone Joint Surg Am. 2000;82:809–13.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Bryan, T.P., Duquin, T. (2017). Radial Head Fracture. In: Eltorai, A., Eberson, C., Daniels, A. (eds) Orthopedic Surgery Clerkship. Springer, Cham. https://doi.org/10.1007/978-3-319-52567-9_23
Download citation
DOI: https://doi.org/10.1007/978-3-319-52567-9_23
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-52565-5
Online ISBN: 978-3-319-52567-9
eBook Packages: MedicineMedicine (R0)