
Abstract
Chylous disorders are uncommon but serious and frequently life-threatening conditions. Chylous reflux through incompetent abdominal and pelvic lymphatics causes lymphatic congestion and lymphedema; chylous effusion results when dilated lymph vessels rupture and chyle accumulates in body cavities or in joints. Rupture of skin lymphatics results in chylous leak. Conservative therapy is usually the first line of treatment using dietary manipulation and aspiration of the effusion. In patients with primary chylous disorders who fail conservative management, the selective use of ligation of lymphatic fistulas, excision of dilated lymphatics, sclerotherapy, lympho-venous reconstruction (LVR), and placement of a peritoneovenous shunt (PVS) are additional treatment options suggested. Specifically, for chylothorax, ligation of the leaking lymphatics or the thoracic duct (TD) along with pleurodesis via thoracotomy or VATS is frequently effective; LVR may be considered as a surgical option in selected patients. Ligation of the incompetent retroperitoneal lymphatics and oversewing ruptured lymphatics can produce long-term improvement in lymphangiectasia and lymphatic reflux. Chylous ascites can be treated with ligation of the mesenteric or retroperitoneal lymphatic fistula, or LVR or bypass grafting in cases with large lymph vessel and patent venous system, or PVS, although the role of PVSs in the treatment of chylous ascites remains controversial. Endovascular treatment such as percutaneous embolization is increasingly used, but surgical treatment still plays an essential role especially in patients who fail to or not eligible for endovascular therapy. Individualized treatment based on the etiology, the site of lymph leaks, the amount of drainage volume, and the extent of chylous disease is required to achieve treatment success. In this chapter we review principles, indications, results, and problems of these surgical techniques.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


-
Chylous disorders are rare.
-
Conservative therapy is usually the first-line treatment option, but endovascular and surgical treatments are available as are peritoneovenous shunts (PVSs) to direct chyle into the central venous system.
-
The outcomes depend on etiology, the site of lymph leaks, the amount of drainage volume, and the extent of chylous disease. Also, the increasingly performed endovascular treatment such as percutaneous embolization has challenged the use of traditional open surgeries.
-
Principles, indications, results, and problems of surgical techniques are reviewed in this chapter.
Chylous reflux is the term used to describe retrograde flow in the incompetent lymphatic system secondary to lymphangiectasia and loss of lymphatic valve function. Chylous effusion results when dilated lymph vessels rupture and chyle accumulates in body cavities or in joints. Rupture of skin lymphatics results in chylous leak. Chylous effusions are uncommon but serious and frequently life-threatening conditions. The etiology of chylous effusions includes primary developmental abnormalities of the lymph vessels, such as lymphangiectasia, atresia, or hypoplasia [1], or secondary causes due to trauma, surgery, or tumor [6, 7]. Disruption of the lymphatics can cause chylous effusions such as chylothorax, chylous ascites, chyloperitoneum, or chylopericardium. Management of chylous reflux alone is usually conservative. Treatment of chylous effusions largely depends on the underlying cause and the amount of drainage volume. Conservative therapy including nutritional and medical management is the mainstay of treatment, and it is effective in many patients, especially in those with postoperative chylous effusions [2, 3, 7]. Therapeutic paracentesis or thoracentesis is indicated in patients with severe dyspnea and/or abdominal discomfort, to drain the accumulated chyle [8].
Although percutaneous endovascular therapy has been increasingly used recently [9,10,11,12,13,14,15], open surgical ligation of the lymphatic leaks or the thoracic duct (TD), with pleurodesis for chylothorax [7, 16], is still frequently performed in patients who fail to conservative management but not eligible for endovascular treatment or in those who fail to endovascular management. In some patients, lympho-venous reconstruction (LVR) with lympho-venous anastomosis (LVA) or grafting can be performed using microsurgical techniques, while, in others, a peritoneovenous shunt (PVS) can be placed to shunt the chyle from the abdominal cavity into the central veins [3, 4, 7]. Surgical management of chylous effusions is challenging due to the diversity of the disorders in terms of etiology, site of lymph leaks and extent, and the frequently high surgical risk; in addition, some procedures are technically demanding, requiring microsurgical techniques.
Conservative management of chylous disorders is discussed in ► Chap. 63. In this chapter, we review principles, indications, results, and problems of the surgical interventions. Since chylous effusions occur rarely, the literature is sparse and consists of case reports and observational series with evidence of low or very low quality.
1 Principles
Management of a chylous effusion depends on the underlying cause; conservative therapy should be the first-line treatment option unless there is a life-threatening condition caused by high volume of chyle leak. In some instances, treatment of the underlying causes can also improve chylous effusions.
Medical treatment as discussed in ► Chap. 63 should be initiated when diet or nutritional measures prove ineffective or served as an adjunctive method to nutritional management. Therapeutic paracentesis or thoracentesis is indicated in patients with severe dyspnea and/or abdominal discomfort. If the chyle flow rate is <500 ml for chylothorax, conservative measures can be applied, and spontaneous closure of the leak may occur in 28–90% of the patients. Conservative management is effective particularly for postoperative chylous ascites, with success rates ranging from 67% to 100% [2, 3, 17].
Open surgical treatment of chylous effusion today is reserved for those who are refractory to conservative management and who are not candidates or fail to endovascular treatment. Open surgical treatment includes ligation of the lymph leaks or vessels, excision of the incompetent lymphatics, LVRs, or placement of a PVS, with simultaneous pleurodesis or sclerotherapy, based on the site and extent of chylous effusion. Ligation of TD under video-assisted thoracoscopy (VATS) or LVR using microsurgical techniques is usually performed to facilitate the procedure.
The goal of surgical treatment of chylous effusion is to obliterate persistent lymph leak which may cause malnutrition, immunocompromised state, and severe electrolyte abnormalities, by ligation or excision of the lymph leaks or vessels or incompetent lymphatics, or promote chylous fluid drainage by LVR or PVS.
2 Indications
Surgical treatment is indicated for all patients who have high-output lymph leaks that result in refractory chylous effusions or in patients who do not benefit from conservative treatment or who fail to minimally invasive management. Surgical treatment options are varied and individualized based on the etiology, site, extent, and severity of chylous disorders.
Surgical indications for chylothorax have been well described in several studies. Cerfolio et al. [18] recommended early reoperation and ligation of the TD when drainage was more than 1000 mL/day based on their experience on 47 chylothoraces developed after thoracic operations. Browse et al. suggested surgery if the fluid loss exceeded 1.5 L per day for more than 5–7 days in an adult or more than 100 mL per day in a child with chylothorax [6]. Schild et al. [12] reviewed literature on chylothorax published between 1995 and 2013 and recommended surgical treatment if: ① More than 1000–1500 mL chyle is drained every day (>100 mL/kg body weight in children); ② Drain output is up to 1000 mL/day for five treatment days (100 mL/year of age in children); ③ A chyle leak (100 mL/day) persists for more than 2 weeks; ④ Drain output remains unchanged over 1–2 weeks; and ⑤ Clinical deterioration such as malnutrition or metabolic problems occur. Early surgical treatment is recommended in young patients with high-volume chyle leaks and in children with body weight below 4 kg. In patients with chylothorax after esophagectomy, a delay of 2–4 weeks is recommended to avoid to put the anastomoses at risk [12]. Takuwa and colleagues [19] suggested surgical treatment for chylothorax that developed after mediastinal lymph node dissection and resection of primary lung cancer, if the drainage exceeds 500 ml during the first 24 h after initiation of a low-fat diet.
Early intervention with VATS is recommended for most patients with a high-output fistula (>1000 mL/24 h), although some authors recommend at least a 1-week trial of conservative therapy. If the chylous output remains greater than 200 mL/24 h after 1 week, VATS intervention is considered [7, 20].
In patients with postoperative chylous ascites, surgical treatment is considered only in those refractory to conservative treatment. In a grading system for chylous ascites after pancreaticoduodenectomy proposed by van der Gaag et al., Grade C patient may require surgical intervention; in this category, the duration of chylous ascites is usually longer than 14 days despite of the treatment [21].
3 Open Surgical Treatments
Currently, there are no strong recommendations regarding management of chylous effusions. In patients with primary chylous disorders who fail conservative or endovascular management, the selective use of ligation of lymphatic fistulas, excision of dilated lymphatics, sclerotherapy, lymphatic reconstruction, and placement of a PVS are considered [3].
3.1 Ligation of the Thoracic Duct and Sclerotherapy for Chylothorax
Traditionally, TD ligation was performed via open thoracotomy. Since VATS has been introduced in the early 1990s, TD ligation with VATS is increasingly used due to its advantage of minimally invasive technique, magnification of the thoracic structures which can facilitate the ligation, efficacy, low expense, and low morbidity. This minimally invasive procedure can also avoid a lengthy conservative course with concomitant loss of chyle and a long hospital stay.
3.1.1 Technique
Preoperative lymphangiography may localize the site of the chylous fistula or document occlusion of the TD. Although percutaneous or tube pleurodesis may be effective in other forms of nonmalignant chylothorax, it is less effective for primary chylothorax. Surgical pleurodesis, either with open thoracotomy [22, 23] or with VATS [7, 24,25,26,27,28,29], with excision of the parietal pleura is the optimal treatment. After a fatty meal, thoracotomy or VATS is performed and the lymphatics are oversewn or clipped. In most cases, this is followed by talc or mechanical pleurodesis.
Ligation of the TD far above the diaphragm may be more successful than clipping of the TD near the diaphragm when VATS is performed. Additionally, if extensive fibrosis is present and the TD is not easily identified, VATS may be used to ligate the mass of tissue between the azygos vein and the aorta with good success [7, 20].
3.1.2 Results
Cerfolio et al. [18] from Mayo Clinic reported 47 patients in whom chylothorax developed after thoracic operations. Nonoperative therapy was successful in one third of the patients, but 32 patients required ligation of the TD, and 2 were treated with mechanical pleurodesis and fibrin glue. Surgery was successful in 31 of the 34 patients (91%). In a series of Browse et al. [6], a total of 20 patients were treated for primary or secondary chylothorax; pleurectomy was performed in 7 patients with primary and in 4 patients with secondary chylothorax, with good outcomes. The authors concluded that open pleurectomy was the most successful treatment to prevent recurrence of the effusion when no distinct chylous leak can be identified. Our earlier experience in 8 procedures for chylothorax included thoracotomy with decortication and pleurodesis (n = 4), ligation of TD (n = 3), and resection of a TD cyst (patient = 1), showing excellent early results in all patients [4]. Bender et al. summarized literature on the surgical management of chylothoraces published between 1981 and 2009; surgical ligation of the TD was successful in 67–100% of the cases, with the best results after treatment for traumatic chylothorax [17].
For postoperative chylothorax following esophagectomy and supradiaphragmatic ligation of the TD for esophageal cancer, Brinkmann and colleagues reported an incidence of 1.9%. In patients with high-output chylous fistula, an early rethoracotomy with repeat ligation of the TD was safe and effective [30].
A summary paper from Kumar and Pawar in 2004 reported a total of 21 VATS cases for the treatment of chylothorax (n = 16), chylopericardium (n = 4), and cervical chylous leak (n = 1), without postoperative complications [20]. Other case reports have demonstrated that VATS is an accepted technique for the management of chylothorax when the occlusion of TD is located between the azygos vein and the descending thoracic aorta [24,25,26,27,28].
Slater et al. [29] reported on the largest case series of TD ligation using VATS, applying a combination of tissue sealer (5 mm LigaSure®, Covidien Energy, Boulder, CO; 3 mm, Justright Surgical, Boulder, CO) and/or sutures, along with mechanical pleurodesis and administration of fibrin glue for the management of chylothorax. Twenty-one patients were treated, all through the right chest with 3 ports. Technical success was 90%; two patients who failed to respond had successful thoracoscopic pleurectomy and chemical pleurodesis.
3.2 Ligation, Excision, and Sclerotherapy of the Incompetent Lymph Vessels for Chylous Ascites and Chylous Reflux
In patients with chylous ascites or reflux of chyle to the genitalia or the limbs, ligation, oversewing, excision, and sclerotherapy of the incompetent or ruptured lymph vessels or lymphatics can be performed, with or without LVR or lymphatic bypass grafting [31].
3.2.1 Technique
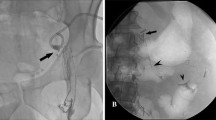
Patients are fed with 60 g of butter or 16 oz. of whipping cream 4 h before the procedure. For lower extremity lymphedema due to chylous reflux, the lymphatics are approached retroperitoneally through a flank incision. The fatty meal allows ready visualization of the retroperitoneal lymphatics during exploration. Dilated and ruptured lymphatics can be oversewn, ligated, or clipped. Careful ligation of the lymph vessels should be done in order to avoid further lymphatic avulsion and leak (◘ Fig. 64.1a–d).

a Right lower extremity lymphoscintigraphy in a 16-year-old girl with lymphangiectasia and severe reflux into the genitalia and left lower extremity. Injection of the isotope into the right foot reveals reflux into the pelvis at 3 h and into the left lower extremity at 4 h. b Intraoperative photograph reveals dilated incompetent retroperitoneal lymphatics in the left iliac fossa containing chyle. c Radical excision and ligation of the lymph vessels were performed. In addition, two lympho-venous anastomoses were also performed between two dilated lymphatics and two lumbar veins. d Postoperative lymphoscintigram performed in a similar fashion reveals no evidence of reflux at 4 h. The patient has no significant reflux 4 years after surgery (From Gloviczki et al. [33])
For chylous ascites caused by ruptured abdominal or pelvic lymphatics, a midline transabdominal approach is used. Chylous cysts, when found, are excised. The most involved segments of the small bowel can be resected in those patients who have severe protein-losing enteropathy due to primary lymphangiectasia. Success of the exploration is improved if a well-defined abdominal fistula because of a ruptured lymphatic vessel or cyst is identified. Sclerotherapy, as an adjunctive procedure, is performed by injecting tetracycline or doxycycline solution, 500–1000 mg diluted in 20 mL of normal saline, directly into the dilated retroperitoneal and pelvic lymph vessels to provoke obstructive lymphangitis.
3.2.2 Results
Servelle published excellent and durable results from ligation and excision of the dilated refluxing lymphatics in 55 patients [32]. In a series of 19 patients who underwent ligation of the retroperitoneal lymphatics for chylous reflux to the limbs and genitalia (anti-reflux procedure) by Kinmonth [1], permanent cure was achieved in five patients and alleviation of symptoms, frequently after several operations, in 12 patients. No improvement or failure was noted in two cases.
Browse et al. [22] reported on a series of 45 patients with chylous ascites. The age at presentation ranged from 1 to 80 (median 12) years; 23 patients were aged 15 years or younger. The chylous ascites was primary in 35 patients and secondary in 10 patients including non-Hodgkin’s lymphoma in six. Other associated lymphatic abnormalities were present in 36 patients, lymphedema of the leg being the most common (26 patients). All patients were initially treated conservatively with dietary manipulation with best results in patients with leaking small bowel lymphatics. Closure of a retroperitoneal or mesenteric fistula, when present, was the most successful operation, curing 7 of the 12 patients. If chylous ascites reaccumulates, reoperation with ligation of the fistula was the most effective treatment. Mean follow-up was 50 months (range 1 month–17 years), 10 patients were cured, and 11 were improved [22].
In 35 patients with primary chylous disorders we treated over a 24-year period [33], 10 patients underwent resection of retroperitoneal lymphatics with or without sclerotherapy of lymphatics, 4 had LVA or grafts, 4 had PVSs, and 1 patient had a hysterectomy for periuterine lymphangiectasia. All patients improved initially, but five had recurrence of some symptoms at a mean of 25 months (range 1–43 months). In three patients with leg swelling, postoperative lymphoscintigraphy confirmed improved lymphatic transport and diminished reflux.
In a retrospective single-center study, Campisi et al. [5] reported on the surgical results of primary chylous ascites in 12 patients with a mean follow-up of 5 years (range 3–7 years). They found laparoscopy was advantageous for confirming the diagnosis, draining the ascites, and evaluating the extension of dysplasia. Carbon dioxide laser was also used as an adjunct for “welding” lymphatic vessels with a low degree of dilatation in 75% of the patients. Eight patients had no relapse of ascites, three had mild recurrence, one of which was treated effectively with a PVS, and one patient died 1 year after surgery from an unrelated cause.
In a recent systemic review of treatment options for postoperative chylous ascites following major abdominal surgery [2], of 36 papers analyzed, surgical treatment was described in case series in nine papers [34,35,36,37,38,39,40,41,42]. In the study by Pabst et al., 5 patients underwent surgical lymphatic fistula closure, all had chylous ascites resolved although one patient required reintervention for a second fistula closure [34]. In another study, the attempt to surgical identification and ligation of the cisterna chyli was failed in all three patients refractory to conservative management; of these patients, lymph leak was not identified on preoperative lymphangiogram or lymphoscintigraphy [39].
3.3 Lympho-Venous Reconstruction
LVR is performed either with a direct anastomosis between a large lymph vessel or the TD and a vein or using a vein interposition graft between the lymphatic and the venous system. LVR works well if a patent TD or large lymphatic vessel is available for a microsurgical anastomosis with the venous system.
3.3.1 Technique
This procedure is technically demanding and requires microscope enhancement to complete the anastomosis. If the upper TD is occluded on lymphangiography, resulting in reflux of chyle into the pleural, pericardial, or peritoneal cavity, LVR with TD–azygos vein anastomosis can be attempted to reconstruct the TD and improve lymphatic transport. Through a right posterolateral thoracotomy, an anastomosis between the lower TD and the azygos vein is performed in an end-to-end fashion, with 8–0 or 10–0 nonabsorbable interrupted sutures and magnification using loupes or the operating microscope (◘ Fig. 64.2a–c). Kinmonth [1], who performed this operation in several patients, suggested that the anastomosis alone is not effective for decompressing the TD; ligation of the abnormal mediastinal lymphatics and oversewing of the sites of the lymphatic leak are also necessary. For terminal TD occlusion, LVR with TD–internal jugular vein (IJV) anastomosis can be considered [43,44,45].

a, b Thoracic duct–azygos vein anastomosis performed through a right posterolateral thoracotomy in an end-to-end fashion with interrupted 8–0 Prolene sutures. c Chest radiograph 2 years later confirms the absence of chylothorax (From Gloviczki et al. [31].)
In patients with chylous reflux, LVA can also be performed, although reflux of blood into the incompetent lymphatics may be a problem; a competent valve on the venous side using a saphenous vein graft will avoid reflux and increase the chance of successful lymphatic drainage [4].
3.3.2 Results
Varying results after LVR have been obtained from case reports. Browse et al. reported on three patients who underwent TD–azygos vein anastomosis for primary (n = 2) or secondary (n = 1) chylothorax, but all anastomoses occluded at 1 year [6]. Our previous study reported on primary chylous disorders that included LVAs (n = 2) or saphenous vein interposition grafting (n = 2) (◘ Fig. 64.3) in addition to retroperitoneal lymphatic ligation. During a median follow-up of 40 months, three of the four LVR patients (75%) were symptomatically improved; additionally, in three patients, improved lymphatic transport and diminished reflux was confirmed on postoperative lymphoscintigraphy [4].

Lympho-venous anastomosis using a saphenous vein graft between a large retroperitoneal lymph vessel (end-to-end) and the right common iliac vein (end-to-side). The competent valve in the vein prevents reflux of blood into the dilated and incompetent lymph vessel (From Huang et al. [3])
LVR can be applied to the treatment of a TD cyst. In a patient with persistent cervical swelling with spontaneous chylothorax and chyloperitoneum caused by a TD cyst with a terminal obstruction of the TD, which was confirmed on lymphangiography, LVA with a side-to-side anastomosis between the cyst and the IJV was performed. Postoperative course was unremarkable, there was no recurrence or vein thrombosis on cervical ultrasound at 3 months, the patient remained symptom-free at 3 years [45].
LVR was reported successful in treating a young lady with persistent chylous vaginal discharge, which was considered secondary. LVA to the right external iliac vein along with meticulous ligation of all visible megalymphatics in the pelvis, parametrium, and iliac region was performed, and the patient remained asymptomatic at 4-year follow-up [46].
LVR was also reported to treat idiopathic lymphatic effusions in neonates. Mihara et al. reported five cases treated with LVA at the extremities in neonates aged 0.5–7 months, based on indocyanine green lymphography. Postoperatively, chylous effusion ended in two of the five cases and decreased in one case [47].
3.4 Peritoneovenous Shunt
PVS is performed for chylous ascites using LeVeen shunt (Becton Dickinson, Franklin Lakes, NJ) or Denver shunt (CareFusion, San Diego, CA). This technique is also considered in patients with fibrosed, aplastic, or hypoplastic mesenteric lymphatic trunks, when diffuse exudation of the chyle is the main source of the ascites [3]. LeVeen shunt was introduced in 1974 [48], but it was withdrawn from the market in the late 1990s and it is no longer available. Denver shunt (CareFusion, San Diego, CA) was introduced in 1970, for the treatment of hydrocephalus [49], and received interest in the management of ascites thereafter. The Denver shunt is offered in two French sizes (11.5 and 15.5 Fr), with either a single or a double valve. The one-way valve prevents the reflux of blood into the venous limb of the shunt, and the second valve acts as a check valve to prevent reflux of ascites or blood from the venous limb of the shunt into the valve chamber while it is refilling after compression pumping.
3.4.1 Technique
The right IJV is accessed, with the help of a 16-Fr peel-away sheath that is placed into the superior vena cava (SVC) and through the right atrium into the inferior vena cava (IVC). The tip of the catheter is positioned between the SVC and the right atrium. The container of the shunt is placed over the edge of the eighth and ninth ribs. In cases of IJV or SVC occlusion, catheter-based shunt placement can be performed from the peritoneal cavity through the great saphenous vein (GSV) and common femoral vein (CFV) into the IVC. Before shunt placement, the ascites should be drained, leaving only a small amount of ascites with which to prime the shunt. In some patients, resection or ligation of pleural, retroperitoneal, and mesenteric lymphatics with or without sclerotherapy of lymphatics or sclerotherapy of lymphatics alone can be performed simultaneously [3].
3.4.2 Results
Results with PVS have been mixed; patency is usually judged by recurrence of ascites. In the study by Browse et al. [6], the nine PVSs were all occluded within 3–6 months after placement. We reported previously on using the LeVeen shunt in three patients with good results, although one patient developed symptomatic superior vena cava syndrome due to thrombosis around the shunt [4].
In the systemic review of postoperative chylous ascites following major abdominal surgery [2], case reports of PVS were described only in five papers [34, 35, 37,38,39]. Pabst et al. reported a mortality rate of 20% and chylous ascites resolution rate of 80% in five patients with PVS; cause of death of the patient was shunt infection [34]. In the study by Kaas et al., three patients underwent PVS, at 1 month, one patient developed sepsis, and the shunt was found nonfunctional [35]. Evan and colleagues reported a shunt replacement rate of 80% in five patients requiring PVS [37].
There were few scattered case reports on Denver shunt in the management of chylous ascites; the results have been varied, showing efficacy [50,51,52,53,54,55,56] or adverse events including loss of the shunt patency [35, 57,58,59], gastrointestinal bleed [52], and sepsis [34, 35]. The most recent publication on 28 patients with PVS is by far the largest series of using Denver shunt in the management of chylous ascites. Causes of chylous ascites in these patients were postoperative chylous ascites following retroperitoneal lymph node dissection (RLND) for cancer in 17 patients and cancer related in 11 patients. Ascites were resolved in 92% (26/28) of patients. Complications included shunt malfunction or occlusion (n = 6), SVC thrombosis (n = 2), subclinical disseminated intravascular coagulopathy (DIC, n = 2), and systemic infection (n = 1), resulting in a complication rate of 37% [60]. Due to the etiology of chylous ascites, the effectiveness of Denver shunt in the management of chylous ascites continues to be controversial.
4 Problems with Surgical Treatments
Currently, there is no evidence-based guideline regarding optimal management of chylous effusions, and management is recommended by the American Venous Forum based on expert consensus opinion as best practice (◘ Table 64.1). Although the increasingly performed endovascular treatment such as percutaneous embolization of TD has challenged the use of traditional open surgery [9,10,11,12,13,14,15], surgical therapy remains the treatment of choice in patients who fail or who are not eligible for endovascular treatment. Outcomes after surgical management of chylous effusions largely depend on the underlying cause, the site of lymph leaks, the amount of drainage volume, and the extent of chylous disease. Therefore, individualized treatment is mandatory.
Ligation and/or excision of the incompetent and leaking lymph vessels frequently has good results for patients with lymphangiectasia and lymphatic reflux [1, 32] or for postoperative chylous effusions [6, 17, 18, 34]. However, the procedure may fail when the site of the leak is not seen on preoperative imaging [39]. For patients with chylothorax, TD ligation via VATS is recommended by most authors if the site of the chylous effusion is not well visualized [17]. LVR is technically demanding and can be performed only in microsurgical centers of excellence. Besides, the success of LVR depends on the caliber and patency of the lymph vessel and the vein and the etiology of chylous disease as well. LVR is suggested in selected patients with obstructive, secondary chylous effusion, early in the course of the disease. Simultaneous excision of the incompetent or ruptured lymphatics is needed to achieve better results.
Finally, results after PVS are inconsistent; the efficacy of PVSs in the treatment of chylous ascites still remains controversial. In addition, Denver shunt is currently the only available shunt to be used in PVS, and in our experience, durability of these shunts is strictly limited. Improvements in technology to design new shunts or invent other drainage techniques to treat chylous effusions are needed.
Conclusions
Chylous disorders are fortunately rare. Conservative therapy is the first line of treatment unless there is a life-threatening condition caused by loss of high volume of chyle. Surgical treatment is indicated in patients refractory to conservative therapy or who fail to endovascular management. For chylothorax, ligation of the leaking lymphatics and the TD along with pleurodesis via thoracotomy or VATS is frequently effective. In selected patients with chylothorax, LVR with a TD–azygos vein or TD–IJV anastomosis may be considered. Ligation of the incompetent retroperitoneal lymphatics and oversewing ruptured lymphatics can produce long-term improvement in lymphangiectasia and lymphatic reflux. Chylous ascites can be treated with ligation of the mesenteric or retroperitoneal lymphatic fistulae or with LVR or bypass grafting in cases with larger lymph vessel and patent adjacent venous system. The role of PVSs in the treatment of chylous ascites remains controversial because the Denver shunt in most reports has limited durability of patency in patients with chylous ascites. Individualized treatment based on the etiology, site of lymph leaks, the amount of drainage volume, and the extent of chylous reflux and effusions is mandatory to achieve treatment success.
Highlighted References
Kinmonth JB. Chylous diseases and syndromes, including references to tropical elephantiasis. In: Kinmonth JB, editor. The Lymphatics: surgery, lymphography and diseases of the chyle and lymph systems. 2nd ed. London: Edward Arnold; 1982. p. 221–68.
Weniger M, D'Haese JG, Angele MK, Kleespies A, Werner J, Hartwig W. Treatment options for chylous ascites after major abdominal surgery: a systematic review. Am J Surg. 2016;211:206–13.
Huang Y, Duncan AA, Oderich GS, Gloviczki P. Medical, open surgical and endovascular treatment of chylous disorders. In: Gloviczki P, editor. Handbook of venous disorders: guidelines of the American venous forum. 4th ed. Abingdon: CRC Press; 2016. p. 747–59.
Noel AA, Gloviczki P, Bender CE, Whitley D, Stanson AW, Deschamps C. Treatment of symptomatic primary chylous disorders. J Vasc Surg. 2001;34:785–91.
Campisi C, Bellini C, Eretta C, et al. Diagnosis and management of primary chylous ascites. J Vasc Surg. 2006;43:1244–8.
References
Browse NL, Allen DR, Wilson NM. Management of chylothorax. Br J Surg. 1997;84:1711–6.
Duncan AA. Local complications: lymphatic. In: Cronenwett JL, Johnston KW, editors. Rutherford's vascular surgery. Philadelphia: Sauders; 2014. p. 723–31.
Lall P, Duncan AA, Gloviczki P. The management of chylous disorders. In: Gloviczki P, editor. Handbook of venous disorders: guidelines of the American venous forum. 3rd ed. Boca Raton: CRC Press; 2008. p. 665–72.
Binkert CA, Yucel EK, Davison BD, Sugarbaker DJ, Baum RA. Percutaneous treatment of high-output chylothorax with embolization or needle disruption technique. J Vasc Interv Radiol. 2005;16:1257–62.
Itkin M, Kucharczuk JC, Kwak A, Trerotola SO, Kaiser LR. Nonoperative thoracic duct embolization for traumatic thoracic duct leak: experience in 109 patients. J Thorac Cardiovasc Surg. 2010;139:584–9; discussion 589–590.
Campisi CC, Boccardo F, Piazza C, Campisi C. Evolution of chylous fistula management after neck dissection. Curr Opin Otolaryngol Head Neck Surg. 2013;21:150–6.
Schild HH, Strassburg CP, Welz A, Kalff J. Treatment options in patients with chylothorax. Dtsch Arztebl Int. 2013;110:819–26.
Pamarthi V, Stecker MS, Schenker MP, et al. Thoracic duct embolization and disruption for treatment of chylous effusions: experience with 105 patients. J Vasc Interv Radiol. 2014;25:1398–404.
Marthaller KJ, Johnson SP, Pride RM, Ratzer ER, Hollis HW Jr. Percutaneous embolization of thoracic duct injury post-esophagectomy should be considered initial treatment for chylothorax before proceeding with open re-exploration. Am J Surg. 2015;209:235–9.
Dinc H, Oguz S, Sari A. A novel technique in the treatment of retroperitoneal lymphatic leakage: direct percutaneous embolization through the leakage pouch. Diagn Interv Radiol. 2015;21:419–22.
Lopez-Gutierrez JC, Tovar JA. Chylothorax and chylous ascites: management and pitfalls. Semin Pediatr Surg. 2014;23:298–302.
Bender B, Murthy V, Chamberlain RS. The changing management of chylothorax in the modern era. Eur J Cardiothorac Surg. 2016;49:18–24.
Cerfolio RJ, Allen MS, Deschamps C, Trastek VF, Pairolero PC. Postoperative chylothorax. J Thorac Cardiovasc Surg. 1996;112:1361–5; discussion 1365–1366.
Takuwa T, Yoshida J, Ono S, et al. Low-fat diet management strategy for chylothorax after pulmonary resection and lymph node dissection for primary lung cancer. J Thorac Cardiovasc Surg. 2013;146:571–4.
Kumar S, Kumar A, Pawar DK. Thoracoscopic management of thoracic duct injury: is there a place for conservatism? J Postgrad Med. 2004;50:57–9.
van der Gaag NA, Verhaar AC, Haverkort EB, Busch OR, van Gulik TM, Gouma DJ. Chylous ascites after pancreaticoduodenectomy: introduction of a grading system. J Am Coll Surg. 2008;207:751–7.
Browse NL, Wilson NM, Russo F, Al-Hassan H, Allen DR. Aetiology and treatment of chylous ascites. Br J Surg. 1992;79:1145–50.
Peillon C, D'Hont C, Melki J, et al. Usefulness of video thoracoscopy in the management of spontaneous and postoperation chylothorax. Surg Endosc. 1999;13:1106–9.
Takeo S, Yamazaki K, Takagi M, Nakashima A. Thoracoscopic ultrasonic coagulation of thoracic duct in management of postoperative chylothorax. Ann Thorac Surg. 2002;74:263–5.
Hirata N, Ueno T, Amemiya A, Shigemura N, Akashi A, Kido T. Advantage of earlier thoracoscopic clipping of thoracic duct for post-operation chylothorax following thoracic aneurysm surgery. Jpn J Thorac Cardiovasc Surg. 2003;51:378–80.
Ohtsuka T, Ninomiya M, Kobayashi J, Kaneko Y. VATS thoracic-duct division for aortic surgery-related chylous leakage. Eur J Cardiothorac Surg. 2005;27:153–5.
Christodoulou M, Ris HB, Pezzetta E. Video-assisted right supradiaphragmatic thoracic duct ligation for non-traumatic recurrent chylothorax. Eur J Cardiothorac Surg. 2006;29:810–4.
Watanabe A, Koyanagi T, Nakashima S, Higami T. Supradiaphragmatic thoracic duct clipping for chylothorax through left-sided video-assisted thoracoscopic surgery. Eur J Cardiothorac Surg. 2007;31:313–4.
Slater BJ, Rothenberg SS. Thoracoscopic thoracic duct ligation for congenital and acquired disease. J Laparoendosc Adv Surg Tech A. 2015;25:605–7.
Crucitti P, Mangiameli G, Petitti T, et al. Does prophylactic ligation of the thoracic duct reduce chylothorax rates in patients undergoing oesophagectomy? A systematic review and meta-analysis. Eur J Cardiothorac Surg. 2016;50:1019–24.
Gloviczki P, Noel AA. Surgical treatment of chronic lymphedema and primary chylous disorders. In: Rutherford RB, editor. Rutherford’s vascular surgery. 6th ed. Philadelphia: Elsevier; 2005. p. 2428–45.
Servelle M. Surgical treatment of lymphedema: a report on 652 cases. Surgery. 1987;101:485–95.
Gloviczki P, Calcagno D, Schirger A, et al. Noninvasive evaluation of the swollen extremity: experiences with 190 lymphoscintigraphic examinations. J Vasc Surg. 1989;9:683–9; discussion 690.
Pabst TS 3rd, McIntyre KE Jr, Schilling JD, Hunter GC, Bernhard VM. Management of chyloperitoneum after abdominal aortic surgery. Am J Surg. 1993;166:194–8; discussion 198–199.
Kaas R, Rustman LD, Zoetmulder FA. Chylous ascites after oncological abdominal surgery: incidence and treatment. Eur J Surg Oncol. 2001;27:187–9.
Huang Q, Jiang ZW, Jiang J, Li N, Li JS. Chylous ascites: treated with total parenteral nutrition and somatostatin. World J Gastroenterol. 2004;10:2588–91.
Evans JG, Spiess PE, Kamat AM, et al. Chylous ascites after post-chemotherapy retroperitoneal lymph node dissection: review of the M. D. Anderson experience. J Urol. 2006;176:1463–7.
Malik HZ, Crozier J, Murray L, Carter R. Chyle leakage and early enteral feeding following pancreatico-duodenectomy: management options. Dig Surg. 2007;24:418–22.
Assumpcao L, Cameron JL, Wolfgang CL, et al. Incidence and management of chyle leaks following pancreatic resection: a high volume single-center institutional experience. J Gastrointest Surg. 2008;12:1915–23.
Kim BS, Yoo ES, Kim TH, Kwon TG. Chylous ascites as a complication of laparoscopic nephrectomy. J Urol. 2010;184:570–4.
Cotte E, Passot G, Tod M, et al. Closed abdomen hyperthermic intraperitoneal chemotherapy with irinotecan and mitomycin C: a phase I study. Ann Surg Oncol. 2011;18:2599–603.
Tulunay G, Ureyen I, Turan T, et al. Chylous ascites: analysis of 24 patients. Gynecol Oncol. 2012;127:191–7.
Melduni RM, Oh JK, Bunch TJ, Sinak LJ, Gloviczki P. Reconstruction of occluded thoracic duct for treatment of chylopericardium: a novel surgical therapy. J Vasc Surg. 2008;48:1600–2.
Franceschi C, Gianesini S, Bahnini A, Laurian C, Menegatti E, Zamboni P. The recurrent cervical swelling syndrome. Phlebology. 2012;27:90–2.
Veziant J, Sakka L, Galvaing G, Tardy MM, Cassagnes L, Filaire M. Lymphovenous anastomosis for recurrent swelling syndrome and chylous effusion due to cervical thoracic duct cyst. J Vasc Surg. 2015;62:1068–70.
Joshi B, Mavuduru RS, Mandal AK, Bhattacharya A, Lal A, Jain V. Chylocolporrhea or chylous vaginal discharge: diagnostic conundrum with therapeutic challenge. Arch Gynecol Obstet. 2016;293:815–8.
Mihara M, Hara H, Shibasaki J, et al. Indocyanine green lymphography and lymphaticovenous anastomosis for generalized lymphatic dysplasia with pleural effusion and ascites in neonates. Ann Vasc Surg. 2015;29:1111–22.
Leveen HH, Christoudias G, Ip M, Luft R, Falk G, Grosberg S. Peritoneo-venous shunting for ascites. Ann Surg. 1974;180:580–91.
Kirsch WM, Newkirk JB, Predecki PK. Clinical experience with the Denver shunt: a new silicone-rubber shunting device for the treatment of hydrocephalus. Technical note. J Neurosurg. 1970;32:258–64.
Turner WW Jr. Chylous ascites: resolution after Denver peritoneovenous shunt. South Med J. 1983;76:539.
Selli C, Carini M, Mottola A, Barbagli G. Chylous ascites after retroperitoneal lymphadenectomy: successful management with peritoneovenous shunt. Urol Int. 1984;39:58–60.
Savlov ED. Chylous ascites following retroperitoneal lymph node dissection successfully treated with peritoneovenous shunt. J Surg Oncol. 1987;36:228–9.
Fleisher HL 3rd, Oren JW, Sumner DS. Chylous ascites after abdominal aortic aneurysmectomy: successful management with a peritoneovenous shunt. J Vasc Surg. 1987;6:403–7.
Manolitsas TP, Abdessalam S, Fowler JM. Chylous ascites following treatment for gynecologic malignancies. Gynecol Oncol. 2002;86:370–4.
Matsufuji H, Nishio T, Hosoya R. Successful treatment for intractable chylous ascites in a child using a peritoneovenous shunt. Pediatr Surg Int. 2006;22:471–3.
Makino Y, Shimanuki Y, Fujiwara N, et al. Peritoneovenous shunting for intractable chylous ascites complicated with lymphangioleiomyomatosis. Intern Med. 2008;47:281–5.
Chang JH, Newkirk J, Carlton G, Miller JD, Orsini E. Generalized lymphangiomatosis with chylous ascites--treatment by peritoneo-venous shunting. J Pediatr Surg. 1980;15:748–50.
Barakat HM, Shahin Y, McCollum P. Chylous ascites complicating elective abdominal aortic aneurysm repair: case report and review of treatment options. Vasc Endovasc Surg. 2012;46:682–5.
Kanou T, Nakagiri T, Minami M, Inoue M, Shintani Y, Okumura M. Peritoneovenous shunt for chylous ascites after lung transplantation for lymphangioleiomyomatosis. Transplant Proc. 2012;44:1390–3.
Yarmohammadi H, Brody LA, Erinjeri JP, et al. Therapeutic application of Percutaneous Peritoneovenous (Denver) shunt in treating chylous ascites in cancer patients. J Vasc Interv Radiol. 2016;27:665–73.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter
Cite this chapter
Huang, Y., Gloviczki, P. (2018). Surgical Management of Chylous Reflux and Effusions. In: Lee, BB., Rockson, S., Bergan, J. (eds) Lymphedema. Springer, Cham. https://doi.org/10.1007/978-3-319-52423-8_64
Download citation
DOI: https://doi.org/10.1007/978-3-319-52423-8_64
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-52421-4
Online ISBN: 978-3-319-52423-8
eBook Packages: MedicineMedicine (R0)