
Abstract
Several approaches have been described for thyroid and parathyroid surgery to avoid a visible neck incision, which is of a concern especially in young females with history of healing with keloid or hypertrophic scar. Herein, we are discussing promising novel techniques in providing a hidden incision, with reported safety and technical superiority utilizing robotic technology. Several remote access robotic approaches have been described, including transaxillary, retroauricular, and bilateral axillobreast (BABA) approaches. In this chapter, we focused on perioperative planning utilizing the transaxillary approach.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others



Keywords
Introduction
Over the last decade, there has been increased interest in improving quality of life as well as healthcare overall. Patients are more aware and active in the decision-making process, which has led to an increase in focusing on quality of life issues such as early return to normal activity and cosmetic appearance after a treatment. As a result, there has been an increased adoption of minimally invasive surgery in various surgical fields. In the area of head and neck surgery, minimally invasive and endoscopic surgical techniques were slow to be adopted due to some spatial and anatomical limitations, such as the lack of a pre-existing working space, the hypervascularities of target organs, and abundance of critical nerves and major vessels. However, using the features of the surgical robotic system, such as a three-dimensional magnified surgical view, hand-tremor filtration, fine-motion scaling, and precise and multiarticulated hand-like motions, scarless thyroid and parathyroid surgery using a remote site incision overcame many of the previous limitations. Since the first introduction of robotic thyroidectomy using transaxillary approach in 2007, many studies have examined the technical aspects and surgical outcomes for robotic thyroid surgery and reported similar outcome. As a result, the robotic technique has become a promising remote access approach for the treatment of thyroid and parathyroid gland pathology in a select group of patients.
In this chapter, the robot-assisted transaxillary approach for thyroid and parathyroid surgery will be described.
Indications and Patient Selection
Thyroidectomy
Robotic approach can be considered in patients who have concerns of a visible neck scar, due to cosmetic impact or a previous history of healing with keloid or hypertrophic scar. The body build of the patient, volume of the thyroid gland, and the nodule size are factors that need to be assessed preoperatively as they can affect the decision to proceed with a robotic approach. Proper positioning is an essential part of the procedure, so certain conditions that can interfere with patients’ positioning, such as limitation of neck or arm mobility, should also be considered preoperatively. Patient selection is based on the following criteria set by high volume centers, as there are no clearly established guidelines yet:
-
Contraindications:
-
Absolute contraindication:
-
History of radiation to the neck.
-
Previous neck surgery.
-
Substernal goiter.
-
Thyroid cancer with invasion to adjacent structures.
-
Metastatic thyroid cancer to the retropharyngeal or substernal lymph nodes.
-
Poorly differentiated thyroid cancer.
-
-
Relative contraindication:
-
Nodules more than 4 cm.
-
Thyroid volumes more than 40 ml.
-
Advanced thyroiditis.
-
Conditions affecting neck or shoulder mobility, e.g., rotator cuff injury.
-
Morbid obesity.
-
-
With experience, the surgeons might gradually extend their surgical indications for robotic thyroidectomy to include obese patients, cases of thyroiditis, Graves’ disease [1], large thyroid nodules more than 4 cm, and lateral neck dissection [2]. However, it is advisable to be conservative at the beginning of the learning curve. The best candidates for the beginner surgeon are young female patients with small body build (BMI < 35) without any thyroiditis.
Parathyroidectomy
Robotic parathyroidectomy is only indicated in patients with preoperatively well-localized primary hyperparathyroidism having a single gland disease. This procedure currently cannot be offered to patients with multi-gland disease or preoperatively poorly localized parathyroid glands, as it would require bilateral neck exploration, which is technically difficult to perform using a one side approach.
-
Absolute contraindication:
-
Failure to localize the parathyroid gland preoperatively.
-
Preoperative biochemical or radiological evidence of multiglandular disease.
-
Previous neck surgery.
-
Previous radiation to the neck.
-
-
Relative contraindication:
-
Parathyroid carcinoma.
-
Associated large goiter, or Graves’ disease.
-
Equipment and Instruments
A shoulder roll is required for neck extension and soft pillows are required for the arm positioning. For the flap creation, monopolar electro-cautery with long tip, long vascular Debakey forceps, two army-navy retractors, two lighted breast retractors (Fig. 26.1), and a vessel-sealing device are needed. An external retractor is required to maintain the working space during the procedure (Marina Medical, Sunrise, FL, USA) (Fig. 26.2).

Lighted breast retractor

Modified robotic thyroidectomy retractor (Marina Medical, Sunrise, FL, USA)
For the robotic dissection portion of the procedure, the da Vinci S, Si, or Xi system (Intuitive, Inc., Sunnyvale, CA, USA) can be used along with a 30-degree down looking scope, 5 mm Maryland dissector (Intuitive, Inc.), and 8 mm Prograsp forceps (Intuitive, Inc.). A 5 mm harmonic curved shear (Intuitive, Inc.) is used as the robotic vessel-sealing device. Four trocars can be inserted through the single axillary incision: two 5 mm trocars, one 8 mm trocar, and one 12 mm trocar. During the procedure a 5 mm laparoscopic suction and irrigation can be used by the assisting surgeon to retract structures such as sternocleidomastoid (SCM) muscle or trachea. Rolled gauze can be used for hemostasis during the procedure.
Instruments and surgical equipment |
|---|
Flap creation and maintenance of working space |
2 Army-navy retractors |
2 Lighted breast retractors |
Long Vascular Debakey forceps |
Monopolar electrocautery (short and long tips) |
Vessel sealing device |
Special modified robotic thyroidectomy retractor (Marina Medical, Sunrise, FL, USA) |
Robotic instruments |
DaVinci Si or Xi robot system |
Two 5-mm trocars |
8-mm trocar |
12-mm trocar |
5-mm Maryland dissector |
8-mm Prograsp forceps |
5-mm Harmonic curved shear |
30 degree endoscope |
Laparoscopic suction/irrigation |
Surgical Technique
Positioning
The patient is placed in the supine position and is intubated using one of the nerve integrity monitor endotracheal tubes to enable intraoperative monitoring of the recurrent laryngeal nerve. The neck is extended using a shoulder roll. The ipsilateral arm on the same side of the lesion is raised and flexed at the elbow with the forearm resting over the forehead, and secured in place with proper padding using soft pillows and foam (Fig. 26.3). By raising the arm, the distance between the incision and anterior neck will be shortened. The contralateral arm is tucked in on the side of the patient. Caution has to be taken not to overextend the shoulder in order to avoid traction injury of the brachial plexus. Nerve monitoring of the radial, median, and ulnar nerves using somatosensory evoked potential (SSEP) (Biotronic, Ann Arbor, MI) can be used to help avoid stretching of any of these nerves.

Patient positioning in transaxillary approach; the arm is raised and flexed at the elbow resting comfortably over the patients face. Preoperative ultrasound is performed to assess the relation of the internal jugular vein and carotid to the thyroid
Intraoperative ultrasound is usually performed at the beginning of the procedure to assess the relation of the thyroid to the internal jugular vein and carotid artery. In cases of robotic-assisted parathyroidectomy, the location of the pathological parathyroid gland can be confirmed by performing intraoperative ultrasound.
Incision and Flap Creation
Incision
-
The neck, anterior chest, and the ipsilateral axilla are prepped and draped.
-
The incision location landmarks are the thyroid prominence, sternal notch, and the anterior axillary line. A 60° oblique line is drawn from the thyroid prominence to the axilla and a transverse line is drawn from the sternal notch to the axilla. Afterward, a 5–6 cm skin incision can be made between the two lines at the anterior axillary line along the lateral border of pectoralis major muscle. This will create a completely hidden incision in the axillary folds (Fig. 26.4).
Fig. 26.4 
The skin incision landmarks, it is placed at the anterior axillary line between two lines, an oblique line from the thyroid prominence and a transverse line from the sternal notch

Flap Creation
-
1.
Using electrocautery, the subcutaneous flap is created superficial to the pectoralis major muscle fascia up to the clavicle. The army-navy and lighted breast retractors are used to facilitate this step (Fig. 26.5).
Fig. 26.5 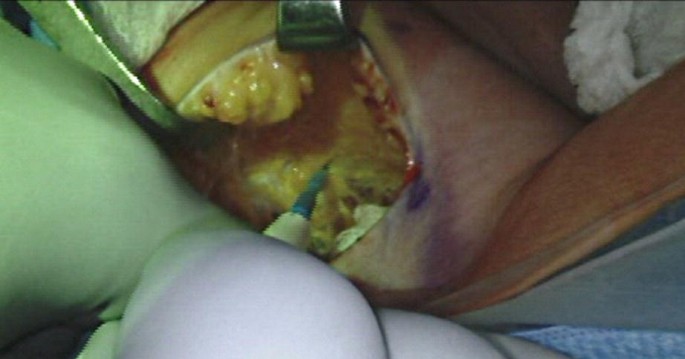
Flap creation superficial to the pectoralis major muscle fascia
-
2.
Subplatysmal dissection is performed after crossing the clavicle until the two heads of (SCM) are identified. The flap dissection is continued medially to the medial border of the SCM.
-
3.
The avascular plane between the clavicular and sternal heads of the SCM is created. The omohyoid muscle is considered a great landmark of the superior pole of the thyroid gland. Great care should be taken to avoid injury to the internal and external jugular vein during this dissection (Fig. 26.6, 26.7, and 26.8).
Fig. 26.6 
Opening of the avascular plane between the two heads of SCM
Fig. 26.7 
The omohyoid muscle, which is a landmark of the upper pole, is identified after opening the plane between the two heads of SCM
Fig. 26.8 
After dividing the omohyoid muscle the strap muscles, thyroid, and internal jugular vein are exposed
-
4.
The superior belly of omohyoid muscle is retracted or divided and then the thyroid is separated from the overlying strap muscles using the electrocautery or a vessel-sealing device until the contra lateral side of the thyroid gland is fully exposed.
-
5.
The blade of the special thyroid modified self-retaining retractor is placed through the axillary incision retracting the flap, the sternal head of SCM, and the strap muscles. It is mounted to the bed from the contralateral side of the operating table. Appropriate maintenance of the working space is an important aspect during the procedure. A suction tube should be attached to the suction channel of the retractor to remove the smoke during the procedure (Fig. 26.9).
Fig. 26.9 
The external modified robotic thyroidectomy retractor is placed and connected to suction to eliminate the smoke during the procedure





Robot Docking
The robot is docked from the contralateral side of the table. A 30-degree down view endoscope and three robotic instruments are secured to the robotic arms and inserted through the single axillary incision. The 12 mm trocar is placed in the middle of the axillary incision on the lower edge and the camera is inserted in an upward direction (Fig. 26.10). The 8 mm trocar is placed at the upper edge of the incision, and the Prograsp forceps is inserted in downward direction. The two 5 or 8 mm trocars are placed as far apart as possible at the lateral ends of the incision, and the Maryland dissector is inserted at the non-dominant side of the surgeon in an upward direction and the Harmonic curved shear is inserted so it can be used by the dominant hand of the surgeon. Proper placement of the instruments and maintaining appropriate space between the arms is a crucial step of the procedure to avoid collision of the robotic arms (Fig. 26.11, 26.12, 26.13, and 26.14).

Placement of the endoscope, the trocar is placed at the center of the lower edge and the scope is inserted in an upward direction

Placement of trocars in a left side approach; the scope is placed at the middle of the lower edge of the incision, the prograsp placed taround the upper middle area of incision, the Maryland to the right lateral end of the incision and harmonic curved shear at the left lateral end

Room setup for Si robot, left side approach

Room setup for Xi robot, right side approach

Robotic arms configuration for Si robot
Thyroidectomy
-
1.
The vagus nerve is stimulated initially using the nerve monitor probe, which is introduced into the field by the assistant.
-
2.
The laparoscopic suction/irrigation is introduced by the assistant through the axillary incision, and used to downward retract the internal jugular vein and clavicular head of the SCM.
-
3.
The upper pole of thyroid is retracted medially and inferiorly using the Prograsp forceps. The superior thyroid vessels are dissected and divided using the Harmonic curved shear. Care has to be taken to divide them closer to the thyroid to avoid injury of the external branch of the superior laryngeal nerve. Further dissection of the upper pole is continued until it is dissected from the cricothyroid muscle. This will allow identification and preservation of the superior parathyroid gland.
-
4.
The Prograsp forceps is repositioned and the thyroid is retracted medially, then the thyroid middle vein is dissected and divided using the Harmonic curved shears.
-
5.
Meticulous dissection at the tracheoesophageal groove is performed until the recurrent laryngeal nerve (RLN) is identified and its functional integrity is confirmed using the nerve monitor probe. Dissection of the RLN is carried until its insertion into the cricothyroid muscle.
-
6.
The inferior pedicle is dissected and divided using the Maryland and Harmonic curved shear after careful dissection of the RLN.
-
7.
The thyroid is dissected carefully medial to the RLN. It is shaved from the trachea until reaching the contralateral side. Caution has to be taken at Berry’s ligament region to avoid direct and indirect thermal injury to the RLN by the Harmonic curved shear active blade.
-
8.
The thyroid lobe and isthmus are divided from the remaining thyroid lobe and the specimen is extracted through the axillary incision (Video 26.1).
-
9.
In cases of total thyroidectomy, after performing ipsilateral lobectomy, subcapsular dissection of the contralateral lobe is performed. The RLN and parathyroid glands are identified. The superior pedicle is then dissected and divided followed by dissection of the inferior pedicle. Then, the remaining thyroid is separated from the trachea and extracted through the axillary incision. In some cases, such as in a prominent trachea or male patient, tilting the operating table 10–15° can help to achieve better exposure of the contralateral tracheoesophageal groove.
-
10.
The vagus nerve and RLN are re-stimulated using the nerve monitor probe at the end of the procedure. Hemostasis is secured and confirmed prior to completion of the procedure.
-
11.
The external retractor is removed followed by careful inspection for hemostasis at the flap. A drain is inserted through a separate incision below the axillary incision, then the incision is closed in two layers: interrupted subcutaneous closure followed by a continuous subcuticular closure .
Parathyroidectomy
-
1.
The vagus nerve is initially stimulated using the nerve stimulator probe.
-
2.
The thyroid is retracted medially using the Prograsp forceps; the pathological parathyroid gland is identified with careful dissection.
-
3.
Meticulous dissection in the tracheoesophageal groove is performed until the recurrent laryngeal nerve is identified and its functional integrity is confirmed by nerve stimulation using the nerve monitor probe.
-
4.
Circumferential dissection of the parathyroid gland is performed via the utilization of Harmonic curved shears and Maryland dissectors until the pedicle of the inferior thyroid artery branches is identified and divided.
-
5.
The specimen is extracted using an endo-catch bag through the axillary incision and sent for frozen section for confirmation.
-
6.
Serial blood samples are drawn for intra-operative parathyroid hormone (IOPTH) levels at scheduled interval; one baseline at the beginning of the procedure, one pre-excision followed by scheduled 10 and 15 min levels post-excision. A drop of 50% or more of the IOPTH level from the baseline or pre-excision level indicates a curative surgery by successful removal of the culprit parathyroid gland.
-
7.
Hemostasis is secured and the vagus nerve is re-stimulated at the end of the procedure, followed by undocking of the robot.
-
8.
The retractor is removed and a drain is inserted through a separate incision below the axillary incision. The incision is closed in two layers: interrupted subcutaneous and continuous subcuticular.
Postoperative Care
The drain is usually kept in place until the output is less than 30 ml/day. Most patients will have their drains removed in 2 or 3 days. Discharging the patient depends on the surgeons’ experience and preference; however, in our experience, most patients are discharged on the same day of surgery.
Precautions During the Procedure
Positioning
Neuropraxia of the brachial plexus is a rare possible risk that can happen during improper positioning, likely caused by overextension of the shoulder leading to traction of the brachial plexus. It usually causes temporary paralysis of the arm that recovers within a few weeks. This can be prevented by avoiding overextension and over medial-rotation of the shoulder while positioning the arm. In addition, the use of the nerve monitor of the radial, median, and ulnar nerves using SSEP can be very helpful, which can alert you if there was loss of signal of the nerve during the procedure allowing adjustment of the arm positioning when needed.
Flap Creation
During flap creation, injury to the skin flap by button-hole perforation or thermal injury should be avoided by following the proper surgical plane along the subplatysmal layer and using the lighted breast retractor. One should avoid injury to the internal jugular vein or carotid while opening the avascular plane between the two heads of SCM. The best way to avoid this complication is careful dissection following the anatomical plane and direct identification of these structures.
Robotic Dissection
One should avoid the rare risk of thermal tracheal or esophageal injuries by making sure all arms are in view during energy application.
Advantages of Robotic Thyroid and Parathyroid Surgery
Several studies have reported on the safety and feasibility of robotic thyroid and parathyroid surgery, with surgical outcomes comparable to conventional open and endoscopic approaches. In one meta-analysis study, we found no difference in the incidence of recurrent laryngeal nerve injury, permanent hypocalcaemia, hematoma, seroma, chyle leak, and tracheal injury in robotic approaches compared to open and endoscopic approaches [3].
Robotic surgery has several advantages compared to the conventional open approach. The main advantage is the cosmetic effect of a hidden scar in the axilla, which might be an important factor for young females where a visible neck scar might have significant cosmetic impact on them. Several studies reported greater cosmetic satisfaction in robotic approach compared to the open approach [4–7]. Technically, the robotic approach has several advantages compared to the endoscopic approaches. First, it provides a stable three-dimensional view that makes it easier to identify and preserve the recurrent laryngeal nerve and parathyroid gland. Additionally, the downscaling and tremor elimination features enable the surgeon to perform precise movements. The multiarticulated arms and endowrist instruments facilitate the work in deep and narrow places and enable wide range of movement. During robotic surgery, the surgeon is in control of the entire procedure, and is not depending on an assistant compared to the endoscopic approach [7–10].
The ergonomics provided by the robot reduces the musculoskeletal discomfort to the surgeon [9, 11]. A multicenter study by Lee et al. showed that surgeons’ neck and back pain were lower in robotic thyroidectomy compared to open and endoscopic thyroidectomy. This can be attributed to the position of the surgeon, as he or she sits at a console and performs the surgery with the aid of stereoscopic vision and robotically controlled instruments with the monitor placed at his eye level, which minimize the postural changes to the neck and shoulders [10].
Interestingly, there is a reported rapid learning curve in robotic-assisted thyroidectomy in comparison to endoscopic approaches. One should perform 35–45 robotic cases compared to 55–70 in the endoscopic approach to reach the peak of their learning curve [12].
The high cost of robotic thyroid surgery compared to the open and endoscopic approaches is the main disadvantage, and this is due to the longer operative time and equipment cost [13]. However, there is less risk of complications, shorter hospitalizations, and lower cost when thyroid surgery is performed by high volume surgeons compared to low volume surgeons.
Conclusion
Robotic thyroid and parathyroid surgeries provide great functional and cosmetic benefits with acceptable surgical outcomes when compared to the conventional open procedure. We anticipate that with future improvements of the robotic technology the indications of robotic thyroid and parathyroid surgery will expand along with improved surgical outcomes.
References
Kandil E, Noureldine S, Abdel Khalek M, Alrasheedi S, Aslam R, Friedlander P, et al. Initial experience using robot- assisted transaxillary thyroidectomy for Graves’ disease. J Visc Surg. 2011;148(6):e447–51.
Kang SW, Lee SH, Ryu HR, Lee KY, Jeong JJ, Nam KH, et al. Initial experience with robot-assisted modified radical neck dissection for the management of thyroid carcinoma with lateral neck node metastasis. Surgery. 2010;148(6):1214–21.
Kandil E, Hammad AY, Walvekar RR, Hu T, Masoodi H, Mohamed SE, et al. Robotic thyroidectomy versus nonrobotic approaches: a meta-analysis examining surgical outcomes. Surg Innov. 2016;23(3):317–25.
Lee J, Nah KY, Kim RM, Ahn YH, Soh E, Chung WY. Differences in postoperative outcomes, function, and cosmesis: open versus robotic thyroidectomy. Surg Endosc. 2010;24(12):3186–94.
Tae K, Ji YB, Jeong JH, Lee SH, Jeong MA, Park CW. Robotic thyroidectomy by a gasless unilateral axillo-breast or axillary approach: our early experiences. Surg Endosc. 2011;25(1):221–8.
Tae K, Ji YB, Cho SH, Lee SH, Kim DS, Kim TW. Early surgical outcomes of robotic thyroidectomy by a gasless unilateral axillo-breast or axillary approach for papillary thyroid carcinoma: 2 years’ experience. Head Neck. 2012;34(5):617–25.
Kang SW, Jeong JJ, Nam KH, Chang HS, Chung WY, Park CS. Robot-assisted endoscopic thyroidectomy for thyroid malignancies using a gasless transaxillary approach. J Am Coll Surg. 2009;209(2):e1–7.
Kandil EH, Noureldine SI, Yao L, Slakey DP. Robotic transaxillary thyroidectomy: an examination of the first one hundred cases. J Am Coll Surg. 2012;214(4):558–64.
Kang SW, Lee SC, Lee SH, Lee KY, Jeong JJ, Lee YS, et al. Robotic thyroid surgery using a gasless, transaxillary approach and the da Vinci S system: the operative outcomes of 338 consecutive patients. Surgery. 2009;146(6):1048–55.
Lee J, Kang SW, Jung JJ, Choi UJ, Yun JH, Nam KH, et al. Multicenter study of robotic thyroidectomy: short-term postoperative outcomes and surgeon ergonomic considerations. Ann Surg Oncol. 2011;18(9):2538–47.
Lee YM, Yi O, Sung TY, Chung KW, Yoon JH, Hong SJ. Surgical outcomes of robotic thyroid surgery using a double incision gasless transaxillary approach: analysis of 400 cases treated by the same surgeon. Head Neck. 2014;36(10):1413–9.
Lee J, Yun JH, Choi UJ, Kang SW, Jeong JJ, Chung WY. Robotic versus endoscopic thyroidectomy for thyroid cancers: a multi-institutional analysis of early postoperative outcomes and surgical learning curves. J Oncol. 2012;2012:734541.
Cabot JC, Lee CR, Brunaud L, Kleiman DA, Chung WY, Fahey 3rd TJ, et al. Robotic and endoscopic transaxillary thyroidectomies may be cost prohibitive when compared to standard cervical thyroidectomy: a cost analysis. Surgery. 2012;152(6):1016–24.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Electronic Supplementary Material
Robotic-assisted right thyroid lobectomy (MP4 108512 kb)
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter
Cite this chapter
Ali, D.B., Kang, SW., Kandil, E. (2018). Robotic-Assisted Transaxillary Thyroid and Parathyroid Surgery. In: Patel, A.D., Oleynikov, D. (eds) The SAGES Manual of Robotic Surgery. Springer, Cham. https://doi.org/10.1007/978-3-319-51362-1_26
Download citation
DOI: https://doi.org/10.1007/978-3-319-51362-1_26
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-51360-7
Online ISBN: 978-3-319-51362-1
eBook Packages: MedicineMedicine (R0)