
Abstract
Monitoring (“to monitor”) is a term that involves the observation, actions, measuring, and understanding of many human activities in time. Historically, monitoring started as a physiological measurement problem and probably will end up as an overall assessment of the patient in intensive care. Monitoring is an activity that involves the entire ICU staff: nurses, doctors, respiratory therapists and rehabilitation therapists, and dietitians too. Monitoring is based on different operational models implemented in different countries of the world. Nurses, wherever present 24 h a day, often play the role of liaison between the various staff components, ensuring security, continuity, and harmony and coordinating and communicating all aspects of treatment and care that patient needs. Nurses also provide continuous monitoring and caring for patients and equipment and for their interactions.
Monitoring can be instrumental by the use of various technologies, or it can be derived by observation and the use of scales: both systems provide “bed monitoring” that represents the base of all intensive care unit activity.
We purposed MAGIS, a conceptual model to describe intensive care nursing monitoring which will be explained in later chapters.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
Monitoring (“to monitor”) is a term that involves the observation, actions, measuring, and understanding of many human activities in time. The origin of the word “monitoring” comes from the Latin monitor, -oris, derived from the verb monēre (literally, to warn) and means a continuous or repeated observation, measurement, and evaluation of health and/or environmental or technical data for defined purposes, in accordance with predetermined programs in space and time. Monitoring can be implemented using comparable methods for the detection and collection of data [1]. The term originated in industrial environment, to indicate the continuous control of an operating machine, with appropriate instruments which measure some characteristic parameters (speed, consumption, production, etc.). The original meaning was later expanded: from the machine to the whole process, for an operational structure, and also human resources. Monitoring is widespread used in technical and in social sciences, with the general meaning of “data collections” significant for context.
Historically, monitoring started as a physiological measurement problem (Table 1.1) and probably will end up as an overall assessment of intensive care unit (ICU) patient. This chapter has an introductory function for the first section: the concept of generality of instrumental monitoring, the monitoring carried out through applying scales at patient’s bed, to propose a new monitoring model for ICU patient.
ICUs are very different, such as medical and surgical wards, because of different staff availability (especially nurses) and expertise, skills, technologies, and environments. Monitoring activity involves the entire ICU staff (nurses, physician, respiratory therapists and rehabilitation therapists, dietitians) and is based on different operational models implemented in several countries around the world. Nurses, wherever present 24 h a day, often act as liaison between the various staff components, ensuring security, continuity, and harmony and coordinating and communicating all aspects of treatment and care the patient needs. Nurses also provide continuous monitoring and caring for patients and equipment and for their interactions [3].
2 Instrumental Monitoring
Technology is extremely pervasive and is continuously increasing in ICU. It is commonly used in a multitude of tools for monitoring and supporting patient’s vital functions: the brain, lung, heart, and kidney. The widespread use of electronic monitoring and support to vital function has probably helped to prevent errors and to improve outcomes [4].
The monitoring tools are able to detect multiple parameters, such as continuous electrocardiogram (ECG), end-tidal carbon dioxide (EtCO)2, various measurements of peripheral oxygen saturation (SpO2), cardiac output, and intracranial and cerebral perfusion pressure. The supporting devices can affect the respiratory system (noninvasive mechanical ventilation), circulatory (pacemakers, intra-aortic balloon pump, ventricular devices), cardiorespiratory (extracorporeal membrane oxygenation—ECMO), and kidney (continuous renal replacement therapy (CRRT) and slow low-efficiency daily dialysis (SLEDD)). All these supporting systems contextually also provide monitoring parameters (e.g., the ventilator). Understanding the functions of the devices commonly used in ICU can help in caring for patients in critical conditions [5].
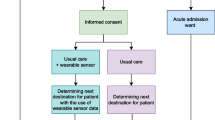
The monitoring technique in intensive care has risks and benefits. Intensive monitoring provides a high data value and information, but it can increase some risks of complications. For example, intensive monitoring could be useful in acute medical interventions aiming to maintain the essential variables within a narrow physiological range and improve the outcome in people with acute stroke [6] (Fig. 1.1).

Conceptual framework-related value of data
At the same time, continuous monitoring can increase unnecessary medical interventions and limit patient’s mobility, thus increasing the risk of complications related to forced immobility as bedsores, stasis pneumonia, deep vein thrombosis (DVT), thromboembolism (TE), and pain [7].
All recorded data must be evaluated in the clinical context. The value of data must be compared with the accuracy of the instrument, its need for calibration, artifacts, and fictitious events (such as a cough during ventilation). As told it is essential to treat patients and their disease instead of numbers. All monitored parameters must be considered in relation to the disease as the best method to treat the same.
In medical literature there are many studies concerning the false alarm rates in the critical patient monitoring. These studies show more than 90% of ICU alarms are false flags. In many cases, these are caused by measurement errors and by patient’s movement. The majority of ICU alarms have no real clinical impact on patient care [8].
A too sensitive monitoring can create “panic” within the team. Staff alarm fatigue can determine inadequate and routine alarm settings. Alarms settings should be tailored on patients individual clinical needs and targets [9]. However, the biggest danger is given by turning off the alarms without understanding events actually occurring to patients. Alarm management is a part of the skills that intensive care staff need to learn at the beginning of their professional careers.
3 Monitoring and Scales
Through the use of a variety of assessment scales (mono-dimensional or multidimensional, according to the complexity of the construct they want to observe), it is possible to obtain measures of many functional states that cannot be described by any instrumental monitoring systems.
Some aspects have been carefully studied by many authors such as pain, sedation, delirium, and state of consciousness. Other authors made comparisons between tools to determine their adequacy in psychometric characteristics, becoming recommended in international guidelines [10].
An example of the use of scales (and their variations) is represented by functional evaluation. ICU patients frequently experience prolonged immobilization and tend to lose their functional ability. In these patients functional skills assessment during ICU stay and prior ICU discharge becomes crucial to prevent damage from immobility. Many scales have been used for the evaluation of functional abilities, impairments, and/or patients’ disabilities. The extent of these outcomes includes different measurement scales. The choice of the right one will depend on the specific cohort of patients, the diagnosis, the stage of rehabilitation, and the available measure sets [11]. These scales are summarized in Table 1.2. Their applicability in ICU environments (including the follow-up period) is indicated in the last column.
4 Bedside Monitoring: An Overview
The ICU monitoring is a component of critical area skill set, featuring as neurological monitoring, respiratory, hemodynamic, renal, hepatic, and nutritional. Each function can be both assessed using validated tools and/or instrumental monitoring [12,13,14].
The rating scales are mostly developed in the assessment of psychosocial functions (neurologic evaluation, pain, sedation, and delirium) and the instrumental monitoring for detection of biological parameters (respiration, hemodynamics, temperature, and metabolism).
The main monitoring variables “to read and feel” are summarized in Table 1.3.
A useful example of the effectiveness of the interpretation of monitoring takes us outside the ICU with Early Warning Score (EWS) in the National Early Warning Score (NEWS) variants and Modified Early Warning Score (MEWS) (Table 1.4). The basic principle is the collection of common physical parameters and variables in a score that allows a fast and shared evaluation of clinical status. In hospitalized patients, addressing the deterioration of physiological functions before they precipitate and to define the intensity of required care can be helpful. In the community, the numerical values expressed by NEWS provide a clear indication of the severity level and help to find the limit for referral to the emergency department and urgent.
In general, the NEWS score provides a universal standard for the evaluation of the clinical course, with the sole exception of obstetrical and pediatric cases, and end of life care [22]. The comparison of the two instruments is reported in Table 1.4.
5 A New Monitoring Model
Which point of view can we provide with the monitoring for an interpretation pace with the expectations of nurses who study, who approach, and who are eventually working in intensive care? What we propose with this text is a more holistic view of the event “monitoring”: a nursing activity that concerns first the person as a whole and, then, individual organ parameters and vital signs.
Monitoring can be defined in a conceptual area bounded by the level of invasiveness and objectivity of the systems that we use in the “measurement.” Increasing the level of invasiveness and objectivity of the measures will also increase the precision level of the measured variables. Collected information must be sufficient and necessary to determine the diagnosis, the performance of the clinical status, and the response to therapies, but, the collection of unnecessary data (such as the execution of ECG 12 times a day in people without cardiac problems, performing unnecessary blood tests, or even the advanced hemodynamic monitoring in patients with only slightly altered parameters) worsens costs without improving outcomes. In a context of limited resources, the selection of the right level of monitoring should be based on proven systems that maximize the cost-benefit ratio [23].
The concept can be expressed in a diagram (Fig. 1.2) in which the operator is bounded by increasing levels of invasiveness and objectivity of the measures, resulting in three different monitoring levels:
-
Level 1: intuitive observational monitoring
-
Level 2: discontinuous monitoring
-
Level 3: continuous monitoring

The MAGIS (acronym of the initials of authors’ names) model of intensive care nursing monitoring
The effective observation of hospitalized patients is the first step to identify the patient’s concerns and the effectiveness of care management. In all contexts, it is vital for nurses to understand the dataset collected, for a positive impact on outcome of patients through the prevention of problems, which otherwise can drive to acute illness, ICU readmission, or death [24].
Poor technology leads to nurse’s feelings play an important role in the perception of patient’s deterioration, and vital parameters are used to support the “gut” feelings [25], that is, highly complex and influenced by many factor process, including the experience and preparation of nurses as well as their ability to relate to the medical staff.
There is a lot of difference in the world regarding “ICU numbers”: the number of ICU beds for 100 hospital beds or for 100,000 people and technologies and health staff as well as the level of education [26]. But feeling and observation are available for all.
The evaluation of EWS facilitated the early identification of a critical condition. Nurses are called to act professionally and responsibly, to understand the meaning of the observations collected on patients and recorded during time. With a partnership approach to problem-solving, nurses can be effective in communicating with the multidisciplinary team and in bringing the most appropriate care [24, 27].
Discontinuous measurements are often carried out with the rating scales. Continuous ones are instead often obtained with electronic instruments appropriately alerted. These are a lot of tools able to ensure the safety and reliability of the monitoring that arises at the base of support of the ICU quality.
We believe that the nurse who approaches in intensive care cannot think in terms of machine/scale dualism as happened for many years. The MAGIS model (Fig. 1.2) is the operationalization of monitoring construct shown in this text. It suggests a systematic approach to monitoring that begins by insights and observation of clinical variables and appearance of the patient and deepens the clinical trial on rating scales and instrumental monitoring.
Monitoring is a dynamic process, a set of details that, correctly linked and interpreted, describe the entirety of the person in relation to his state of health in the moment of observation and over time, through the evolution of trends. The multimodal monitoring offered by different equipments require high levels of expertise within nursing staff to find answers that are not wasteful and respect the proper use of resources in terms of cost/effectiveness.
In conclusion, the new monitoring technologies are to be built up and have to demonstrate a positive impact on the result before being used. We believe that there is no easy answer to this question. Most hospital administrators require outcome data before purchasing any new and expensive technology. This approach, however, could delay application of useful technologies.
There are few studies that have analyzed the impact of monitoring on results. For example, the oximeter has shown no impact on patients’ outcomes [28], and the role of intracranial pressure routine monitoring in comatose patients with acute trauma fails to provide evidence in support of the operation [29]. Despite of these results, those systems are considered essential in monitoring.
A more reflective evaluation of clinical indications and the training of doctors in the area of Swan-Ganz catheter and hemodynamic management would have avoided many patients the unnecessary placement of the cardiac catheter-related damage [30].
Daily challenges will come from deep knowledge of monitoring technologies and appropriate choice according to patient’s condition, available resources, and staff expertise.
References
Nič M, Jirát J, Košata B, Jenkins A, McNaught A. IUPAC compendium of chemical terminology—the gold book. Research Triagle Park, NC: International Union of Pure and Applied Chemistry; 2009.
Patient Care and Monitoring Systems. 2013. http://www.eng.tau.ac.il/~gannot/MI/file2.ppt. Accessed 12 May 2016.
Welch JR, Theaker C. Ruolo infermieristico in terapia intensiva. In: Bersten AD, Soni N, editors. Oh Manuale di terapia intensiva. sesta edizione ed. Milano: Elsevier Health Sciences Italy; 2010. p. 3197–647.
Vincent JL, Singer M. Critical care: advances and future perspectives. Lancet. 2010;376(9749):1354–61. https://doi.org/10.1016/S0140-6736(10)60575-2.
Schallom M. Monitoring and support devices in the Intensive Care Unit. Support Line. 2014;36(6):20–5. 10.21037/jtd.2016.05.37.
Ciccone A, Celani MG, Chiaramonte R, Rossi C, Righetti E. Continuous versus intermittent physiological monitoring for acute stroke. Cochrane Database Syst Rev 2013;(5):CD008444. doi: https://doi.org/10.1002/14651858.CD008444.pub2.
Adams HP Jr, del Zoppo G, Alberts MJ, Bhatt DL, Brass L, Furlan A, et al. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Circulation. 2007;115(20):e478–534.
Imhoff M, Kuhls S. Alarm algorithms in critical care monitoring. Anesth Analg. 2006;102(5):1525–37.
ECRI Institute. Top 10 technology hazards for 2012. The risks that should be at the top of your prevention list. Health Devices. 2011;40(11):358–73.
Tomasi CD, Grandi C, Salluh J, Soares M, Giombelli VR, Cascaes S, et al. Comparison of CAM-ICU and ICDSC for the detection of delirium in critically ill patients focusing on relevant clinical outcomes. J Crit Care. 2012;27(2):212–7. https://doi.org/10.1016/j.jcrc.2011.05.015.
Christakou A, Papadopoulos E, Patsaki E, Sidiras G, Nanas S. Functional Assessment Scales in a general intensive care unit. Hosp Chron. 2013;8(4):164.
Gentili A. Il paziente critico. Clinica e assistenza infermieristica in anestesia e rianimazione. Milano: CEA; 1993.
Besso J, Lumb PD, Williams G. Intensive and critical care medicine. WFSICCM World Federation of Societies of Intensive and Critical Care Medicine. Milano: Springer; 2009.
Bersten AD, Soni N. Oh Manuale di terapia intensiva. London: Elsevier Health Sciences Italy; 2010.
Citerio G, Oddo M, Taccone FS. Recommendations for the use of multimodal monitoring in the neurointensive care unit. Curr Opin Crit Care. 2015;21(2):113–9. https://doi.org/10.1097/MCC.0000000000000179.
Schomer AC, Hanafy K. Neuromonitoring in the ICU. Int Anesthesiol Clin. 2015;53(1):107–22. https://doi.org/10.1097/AIA.0000000000000042.
Barr J, Fraser GL, Puntillo K, Ely EW, Gelinas C, Dasta JF, et al. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit Care Med. 2013;41(1):263–306. https://doi.org/10.1097/CCM.0b013e3182783b72.
Stammet P, Collignon O, Werer C, Sertznig C, Devaux Y. Bispectral index to predict neurological outcome early after cardiac arrest. Resuscitation. 2014;85(12):1674–80. https://doi.org/10.1016/j.resuscitation.2014.09.009.
Kipnis E, Ramsingh D, Bhargava M, Dincer E, Cannesson M, Broccard A, Vallet B, Bendjelid K, Thibault R. Monitoring in the intensive care. Crit Care Res Pract. 2012;2012:473507. https://doi.org/10.1155/2012/473507.
Bulleri E, Fusi C. Manuale di monitoraggio grafico della ventilazione meccanica. Guida pratica alla rilevazione delle asincronie. FareLibri; 2015.
Poulia KA, Yannakoulia M, Karageorgou D, Gamaletsou M, Panagiotakos DB, Sipsas NV, Zampelas A. Evaluation of the efficacy of six nutritional screening tools to predict malnutrition in the elderly. Clin Nutr. 2012;31(3):378–85. https://doi.org/10.1016/j.clnu.2011.11.017.
Berni G, Francois C, Tonelli L. National Early Warning Score (NEWS) Misurazione standardizzata della gravità della malattia. 2016. http://www.regione.toscana.it/documents/10180/320308/National+early+warning+score+(NEWS)/072cf23a-213e-4dac-9ad3-4070579417fa. Accessed 16 Jun 2016.
Rando K, Niemann CU, Taura P, Klinck J. Optimizing cost-effectiveness in perioperative care for liver transplantation: a model for low- to medium-income countries. Liver Transpl. 2011;17(11):1247–78. https://doi.org/10.1002/lt.22405.
Odell M, Victor C, Oliver D. Nurses’ role in detecting deterioration in ward patients: systematic literature review. J Adv Nurs. 2009;65(10):1992–2006.
Cabrera D, Thomas JF, Wiswell JL, Walston JM, Anderson JR, Hess EP, et al. Accuracy of ‘My Gut Feeling:’ comparing system 1 to system 2 decision-making for acuity prediction, disposition and diagnosis in an Academic Emergency Department. West J Emerg Med. 2015;16(5):653–7. https://doi.org/10.5811/westjem.2015.5.25301.
Adhikari NKJ, Fowler RA, Bhagwanjee S, Rubenfeld GD. Critical care and the global burden of critical illness in adults. Lancet. 2010;376(9749):1339–46. https://doi.org/10.1016/S0140-6736(10)60446-1.
Kisiel M. Nursing observations: knowledge to help prevent critical illness. Br J Nurs. 2006;15(19):1052–6. 10.12968/bjon.2006.15.19.22105.
Moller JT, Johannessen NW, Espersen K, Ravlo O, Pedersen BD, Jensen PF, et al. Randomized evaluation of pulse oximetry in 20,802 patients; II. Perioperative events and postoperative complications. J Am Soc Anesthesiol. 1993;78(3):445–53.
Forsyth RJ, Raper J, Todhunter E. Routine intracranial pressure monitoring in acute coma. Cochrane Database Syst Rev. 2015;(11):CD002043. doi: https://doi.org/10.1002/14651858.CD002043.pub3.
Cannesson M, Broccard A, Vallet B, Bendjelid K. Monitoring in the intensive care unit: its past, present, and future. Crit Care Res Pract. 2012;2012:452769. https://doi.org/10.1155/2012/452769.
Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Manici, M., Torbinio, C. (2018). Monitoring Patients: What’s New in Intensive Care Setting?. In: Nursing in Critical Care Setting. Springer, Cham. https://doi.org/10.1007/978-3-319-50559-6_1
Download citation
DOI: https://doi.org/10.1007/978-3-319-50559-6_1
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-50558-9
Online ISBN: 978-3-319-50559-6
eBook Packages: MedicineMedicine (R0)