
Abstract
Abusive head trauma (AHT) is a form of child maltreatment that involves intentional injury to a child’s skull and/or brain caused by inflicted blunt impact, violent shaking, or both. It is the most common cause of serious or fatal brain injuries in children less than 2 years of age, and most deaths occur in infants younger than 6 months. Determining that a child is the victim of AHT can be challenging as the presenting signs and symptoms are often nonspecific and the history provided by caregiver(s) may be absent or inaccurate. Classic injuries associated with AHT include subdural hemorrhage, retinal hemorrhages, and rib fractures, but this triad of injuries is not always present. Associated injuries include additional brain hemorrhages and parenchymal injuries, as well as other bone fractures. A multidisciplinary team approach to the management of the child suffering AHT is paramount and the family will need psychosocial support. Survivors of AHT may have lifelong disabilities; thus, the development and implementation of effective preventative strategies are vital.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
10.1 Introduction
10.1.1 Overview
The Centers for Disease Control and Prevention defines abusive head trauma (AHT) as an injury to the skull or intracranial contents of an infant or child younger than age 5, which is caused by inflicted blunt impact, violent shaking, or both (Parks et al. 2012). The child with AHT may present with cerebral, cervical, or cranial injuries as a result of inflicted injury to the head (Sieswerda-Hoogendoorn et al. 2012). The classic triad of injuries depicting AHT includes subdural hemorrhage (SDH), retinal hemorrhage (RH), and fractures, especially in the ribs and long bones, although not all victims will present with this triad (Kemp 2011; Piteau et al. 2012). It is of vital importance that pediatric nurses understand the epidemiology and pathophysiology of AHT, recognize the signs and symptoms, and maintain a high level of suspicion for these types of injuries in young children.
10.1.2 Historical Context
Children have not always been recognized as being the victims of abuse or inflicted traumatic injury. It was not until the middle of the nineteenth century that French pathologist Auguste Ambroise Tardieu first described injuries he saw in 32 young children in Paris and attributed the cause of their trauma to their caretakers (Roche et al. 2005). Nearly 100 years later, pediatric radiologist John Caffey reported on the association between long bone fractures in children who had chronic subdural hemorrhages but who had no history of trauma or other systemic diseases (Caffey 1946). Additionally, he identified trauma as the possible cause of the retinal hemorrhages that were observed in several of these cases.
The term “battered child syndrome” was coined in 1962 to describe a child with a pattern of injuries including fractures, subdural hematoma, skin bruising, soft tissue swelling, and failure to thrive (Kempe et al. 1962). These injuries were identified in children who either had no history of trauma or in whom the degree and type of injuries were not adequately accounted for with the history provided. Parents and other caregivers were identified as the probable perpetrators of these injuries. Over time the medical community increasingly accepted the concept of child abuse as a legitimate cause of injury, and multiple case reports continued to be published, which associated the presence of concurrent subdural hemorrhages, retinal hemorrhages, and fractures in young children without external signs of trauma (Narang and Clarke 2014). Further work subsequently proposed shaking or whiplash-type injury as a possible mechanism for these injuries because of an infant’s relatively large head and weak neck muscles (Caffey 1972; Guthkelch 1971). Also known by such descriptors as shaken baby syndrome, inflicted brain injury, and non-accidental trauma, the term now preferred by the American Academy of Pediatrics is abusive head trauma, because it is a better descriptor of the clinical findings, rather than the mechanism of injury (Christian et al. 2009).
10.1.3 Epidemiology
The annual incidence of abusive head trauma in the United States is 33.4–38.8 cases per 100,000 children under the age of 1 (Shanahan et al. 2013). This estimate is likely low because not all abused infants will come into contact with the medical system or need/seek medical help. The United Kingdom’s estimated incidence of AHT ranges 12.5–24.1 per 100,000 children (Hobbs et al. 2005). Children in other countries also experience AHT, with reported rates of 14.7–19.6 per 100,000 children in New Zealand (Kelly and Farrant 2008) and 24.6 per 100,000 children in Scotland (Barlow and Minns 2000). The challenge with comparing statistics across countries arises from the varying definitions and terms used to identify AHT.
It is estimated that over 1,600 children die yearly in the United States as the result of child maltreatment and AHT accounts for nearly 80% of these deaths (US Department of Health and Human Services et al. 2012). A vast majority of the child maltreatment victims that die of their injuries are under the age of 3 years (US Department of Health and Human Services et al. 2012), and when the primary cause is AHT, children tend to be less than 6 months of age (Sieswerda-Hoogendoorn et al. 2012). Fifty-one percent of children with fatal injuries are likely to have been evaluated in a clinic or emergency department in the previous 2 months (Ortega et al. 2013), and up to 27% of abused infants under 1 year of age have a previous injury reported in their medical history that was suspicious for abuse because the baby was not mobile or the explanation for the injury was unlikely (Sheets et al. 2013). This represents missed opportunities for intervention prior to a child being severely or fatally injured.
10.1.4 Risk Factors
Several factors have been associated with an increased risk for AHT, and these can be described as arising from the child, the caregiver or adult perpetrator, and the environment (Christian and Committee on Child Abuse and Neglect. 2015; Liley et al. 2012; Narang and Clarke 2014). These factors are not the cause of child abuse, but rather it is the dynamic interrelatedness of these factors that result in AHT. Child factors include male gender and younger child age, particularly those under 6 months. Other risk factors include premature birth, physical or developmental disabilities, and being from an unwanted pregnancy (Sieswerda-Hoogendoorn et al. 2012). Caregiver factors, such as a young mother, unmarried/unrelated caregivers, male caregiver, substance abuse, and caregiver mental health disease, have been identified as being associated with an increased risk for AHT, as has caregivers having unrealistic developmental expectations for the child (Christian and Committee on Child Abuse and Neglect 2015; Lopes et al. 2013; Narang and Clarke 2014). Race and ethnicity have not been consistently linked to an increased risk of AHT (Narang and Clarke 2014). Among the environmental factors are lower socioeconomic status, social isolation, and other domestic violence (Lopes et al. 2013; Narang and Clarke 2014). Additionally, a triggering event, such as crying and the caregiver’s resultant anger and frustration, can create an environment where abuse occurs (Adamsbaum et al. 2010; Narang and Clarke 2014).
10.1.5 Etiology
Inconsolable crying is often a trigger for shaking an infant (Adamsbaum et al. 2010). The caregiver becomes frustrated by failed attempts to console the baby, loses emotional control, and grabs the infant either by the arms, under the arms, or by the chest and proceeds to violently shake the baby. This shaking episode may range from a few to several seconds and may involve shaking alone or shaking and then an impact against a surface, such as a bed, table, or wall. Perpetrators who confess often describe violently shaking the child on repeated episodes over a time period of days to months (Adamsbaum et al. 2010).
10.2 Pathophysiology
10.2.1 Brain Injury
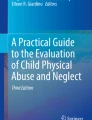
Shaking with acceleration/deceleration and rotational forces applied to the child’s head and neck, along with a sudden angular deceleration of the child’s head at the time of an impact, causes stretching of the veins that bridge from the dura to the brain. Once these vessels exceed their elasticity, they tear and bleed. These veins are normally fixed to the inside of the skull and when torn the resultant bleeding creates subdural and/or subarachnoid hemorrhages. Subdural hemorrhage is the most common intracranial finding associated with AHT, occurring in 77–89% of patients (Kemp et al. 2011; Maguire et al. 2009, 2011; Sieswerda-Hoogendoorn et al. 2012) (Fig. 10.1). The presence of multiple SDH and those within the interhemispheric fissure or over the convexities is often found with AHT (Kemp et al. 2011). SDH with mixed density on CT imaging is more frequently associated with AHT, while accidental SDH will appear as homogeneous hyperdensity (Roach et al. 2014). Other than birth-related SDH, which resolves by 4–6 weeks of age, SDH in children is most commonly due to trauma, and the presence of a SDH in an infant with a history inadequate to explain the injury is highly suspicious for AHT (Kemp et al. 2011; Maguire et al. 2009, 2011).

Subdural hemorrhage. Left-sided moderate subdural hemorrhage observed in a 4-month-old who experienced abusive head trauma
During shaking, the brain strikes the inner surfaces of the skull which causes direct trauma to the brain itself and can result in parenchymal hemorrhages. The deeper axons can twist and shear during shaking, and may ultimately break off, resulting in diffuse axonal injury. Secondary brain injury subsequently results from ischemia, hypoxia, and the cascade of metabolic disruptions in the brain cells, which includes oxidative stress. The damaged cells of the brain take up water and swell, with resultant cerebral edema and increases in intracranial pressure (ICP). Death results from intracranial hypertension and brain herniation.
10.2.2 Spine Injury
Victims of AHT may also have cervical spinal and ligamentous injuries. Infants have a proportionally larger head and weaker neck muscles, making them vulnerable to cervical injuries that result from high-energy rotational forces as the head moves violently back and forth. Cervical injuries observed with AHT include cervicomedullary junction injury, vertebral body subluxations or fractures, traumatic axonal damage of the cervical spine, and primary cervical cord injury (Kadom et al. 2014; Narang and Clarke 2014).
10.2.3 Retinal Hemorrhages
Another common injury related to AHT are retinal hemorrhages, which results from the violent rotational movements of the eyes during shaking that causes the vitreous humor to exert extreme traction on the retina (Yamazaki et al. 2014). Retinal hemorrhages occur in 50–95% of children who are victims of AHT (Binenbaum and Forbes 2014) and have a 71% positive predictive value (Maguire et al. 2009). These hemorrhages tend to be bilateral, widespread to the outer margins of the retina, too numerous to count, and present in all layers of the retina (Maguire et al. 2013) (Fig. 10.2). Retinal hemorrhages also occur in other pediatric conditions, including unidirectional/blunt head trauma, infections, bleeding disorders, metabolic disorders, vaginal births, and after cardiopulmonary resuscitation (Shaahinfar et al. 2015). However, these hemorrhages are usually unilateral, fewer in number, and localized to the optic disks and posterior pole of the retina (Shaahinfar et al. 2015). The majority of RH associated with vacuum-assisted birth resolve within 1 week and all resolve within 4 weeks of age (Laghmari et al. 2014). Up to 15% of non-abused children in the pediatric intensive care unit may have RH, but these are mild, located only on the posterior pole, and found only in the retinal layer (Agrawal et al. 2012; Longmuir et al. 2014). In the absence of a documented history of major trauma, retinal hemorrhages should be considered highly suspicious for AHT.

(a, b) Fundoscopic exam. (a) Right eye with normal retinal image. (b) Left eye with multiple small preretinal and intraretinal hemorrhages in the macula with innumerable preretinal and intraretinal hemorrhages extending from the posterior pole throughout the midperiphery and far periphery
10.2.4 Fractures
Fractures may occur as a result of child maltreatment, and rib fractures are strongly associated with AHT, having a 73% positive predictive value (Maguire et al. 2009). These fractures are thought to occur from squeezing around the infant’s chest during shaking. Healing rib fractures may be seen when the abuse has occurred over time. Other fractures, such as metaphyseal injuries, may occur along with AHT, with the most common type of long bone fractures associated with AHT being those of the humerus and femur, particularly in nonmobile infants. Osteogenesis imperfecta, prematurity, vitamin and mineral deficiencies, and previous injuries can make a child vulnerable to bone fractures, and these should be considered on the list of differential diagnoses (Table 10.1) when evaluating the child for AHT and abuse (Flaherty et al. 2014).
Skull fractures can occur with and without intracranial bleeding, and intracranial bleeding can be present without associated related skull fracture. Skull fractures that result from accidental injuries tend to be unilateral, be linear, and occur in the thinner parietal bones, as the mechanism of injury is generally from lateral movement during accidental falls. Skull fractures in other locations and those that cross suture lines are associated with more severe impact, result in significant brain injury, and thus may be indicative of AHT (Roach et al. 2014) (Fig. 10.3).

Skull fracture. Skull fracture that originates in the occipital bone (large arrow) and crosses the lambdoid suture to the parietal bone (small arrow). This fracture occurred as a result of significant energy forces when a 6-month-old baby was violently shaken before his head impacted a wood table
10.2.5 Seizures
Both clinical and subclinical seizures may arise from cellular injury in the brain (Narang and Clarke 2014). Over 50% of victims of AHT develop seizures (Hasbani et al. 2013), and younger age and intraaxial bleeding are risk factors for both status epilepticus and subclinical status epilepticus (Arndt et al. 2013). Seizures are best determined when the child undergoes continuous electroencephalographic (cEEG) monitoring as soon as possible after admission for suspected AHT (Paul and Adamo 2014).
10.3 Clinical Presentation
Presenting signs and symptoms of AHT will vary depending on the extent of brain injury and the type and severity of accompanying injuries. Manifestations may include nonspecific clinical findings such as an altered level of consciousness, lethargy, irritability, seizures, poor feeding, vomiting, and respiratory changes, including apnea. Apnea is a critical distinguishing feature for AHT compared to accidental head injury, having a positive predictive value of 93% (Maguire et al. 2009). Other conditions that may be associated with AHT include expanding head circumference, failure to thrive, and developmental delay. Since AHT is the most common cause of brain injury in children less than 2 years old, it should be suspected in all children who present with signs of neurologic trauma, unless that trauma is unquestionably accidental (Narang and Clarke 2014). Bruising may be observed, depending on the mechanism of injury, with patterned bruising being more commonly associated with child maltreatment. However, since bruising occurs <50% of the time in AHT, the absence of bruises does not rule out AHT (Fanconi and Lips 2010). Bruising in nonmobile infants and bruising of the head and neck are concerning for AHT (Pierce et al. 2010). It can be challenging to differentiate inflicted from accidental injuries. Table 10.2 further compares injury patterns common to accidental versus abusive injuries (Maguire et al. 2009; Piteau et al. 2012).
10.4 History
10.4.1 History of the Event
A detailed and thorough history must be obtained when evaluating the child who presents with possible AHT. The history given by caregivers may be incomplete or even incorrect. A changing history, particularly when key factors change, is also common with AHT (Christian and Committee on Child Abuse and Neglect 2015; Hettler and Greenes 2003). Caregivers of victims of AHT often describe a relatively small trauma, such as falling from arms or falling from a short height, or they deny any trauma at all (Narang and Clarke 2014). If an accident is described, the caregiver(s) should be asked about when and where the injury occurred, who was present with the child at the time, what happened right before the event, and to describe the response to the injury. As detailed a timeline as possible should be obtained, including how much time elapsed between the incident and seeking medical assistance. If no trauma or accident is described, or if the child is portrayed as suddenly appearing in a poor condition or being found in such a state, the caregiver(s) should be asked about the last time the child was in good condition and how much time elapsed between those states. AHT should also be suspected in the child who presents with a history that does not match the observed injuries. Certain other historical indicators may raise concerns for AHT and these are further detailed in Table 10.3.
10.4.2 Medical History
The child’s medical history, including prior traumas, or symptoms attributed to injury, should be obtained. The child’s growth curve history, medical history of siblings, history of family violence, and previous contact with child protective services should be assessed. A detailed history will aid in quickly eliminating many items on the list of differential diagnoses, which can include accidental trauma, bleeding disorders, and other genetic and metabolic disorders (Table 10.1). Most of these conditions are rare, can be identified from the medical history, and are accompanied by other signs and symptoms or can be ruled out by laboratory tests.
10.5 Diagnosis
10.5.1 Physical Examination
The initial physical examination should include the child’s general appearance, level of consciousness, and a primary survey for life-threatening injuries. Injury location and description should be assessed and documented. The injury location and other factors, such as multiple fractures, burns, injuries in various stages of healing, and patterned injuries/marks, should raise concern for child maltreatment and the possibility of AHT. Pattern marks on the skin may reflect the object which caused the injury and patterned injuries generally do not occur as a result of normal play. Additional examination will also differentiate conditions that may mimic child maltreatment and AHT.
10.5.2 Medical Imaging
The American College of Radiology recommends non-contrast head computed tomography (CT) as the initial study of choice for suspected AHT (Campbell et al. 2015; Christian and Committee on Child Abuse and Neglect 2015; Ryan et al. 2014). This exam can quickly diagnose life-threatening brain injuries that require urgent intervention. Brain magnetic resonance imaging (MRI) may be used to detect small extra-axial fluid collections not seen on CT, to observe diffuse axonal injury and determine the extent of parenchymal brain injuries, while more accurately estimating the time of injury (Campbell et al. 2015; Christian and Committee on Child Abuse and Neglect. 2015; Ryan et al. 2014). MRI can distinguish between fresh blood in an acute SDH and older blood that is undergoing resorption in subacute and chronic SDH. MRI of the spine may be needed to determine associated injuries.
The American Academy of Pediatrics recommends that a skeletal survey, which is a complete set of radiographs with examination of each bone for possible fracture, be completed for all children under 2 years of age who are being evaluated for possible physical abuse (Campbell et al. 2015; Christian and Committee on Child Abuse and Neglect. 2015; Ryan et al. 2014). To detect healing fractures and those not visible on the initial radiographs, the skeletal survey is often repeated 2 weeks after the initial study.
10.5.3 Retinal Examination
A dilated fundoscopic exam is the accepted standard for identifying retinal hemorrhages. A pediatric ophthalmologist should be consulted whenever possible to examine the retinas for hemorrhage (Campbell et al. 2015). In some situations a susceptibility-weighted MRI can also detect RH when fundoscopic exam is not possible, for instance, when eyelids are swollen shut or when pupil dilation would interfere with serial neurological exams (Zuccoli et al. 2013).
10.5.4 Laboratory Evaluation
Initial laboratory evaluation should include a comprehensive metabolic panel, complete blood count, and basic coagulation panel to include prothrombin time (PT) and partial thromboplastin time (PTT) (Christian and Committee on Child Abuse and Neglect. 2015; Narang and Clarke 2014). Subsequent testing will vary depending on the child’s specific injuries and may include liver and pancreatic enzymes to detect any occult abdominal trauma and bleeding studies to rule out any bleeding disorders that may predispose the child to intracranial bleeding (Campbell et al. 2015). Metabolic and bone health studies, such as serum amino acids, phosphorous, and vitamin D 25-OH levels, may be needed as the injury evaluation progresses (Christian and Committee on Child Abuse and Neglect 2015; Narang and Clarke 2014). A routine urinalysis and urine toxicology screen are indicated in the child who presents with an altered level of consciousness.
10.6 Management of Abusive Head Trauma
10.6.1 Medical Interventions
Interventions to stabilize the child’s cardiorespiratory status are given immediate attention. Then the child is taken for radiographic imaging to determine life-threatening intracranial bleeding or injuries that may be amenable to neurosurgical intervention. Potential indications for urgent surgery include large hematomas with a size greater than 10 mm, signs of intracranial hypertension, and low Glasgow Coma Scale (GCS) score ≤12 (Shaahinfar et al. 2015). Interventions include placement of an intraventricular drain and/or intracranial pressure monitor, depressive craniectomy, and craniotomy (Melo et al. 2014). Further management of AHT does not differ from the management of accidental head injury. Chapter 8 further details the specific management of traumatic brain injury.
10.6.2 Collaboration
Each case of suspected abusive head trauma should be managed using a multidisciplinary team approach in order to collect information on the facts that led to the clinical manifestations and appropriately manage the child’s physical and emotional needs, as well as the needs of the family. Team members include bedside nurses and physicians and advance practice nurses with specialty in child abuse pediatrics, pediatric critical care, neurosurgery, trauma, neurology, ophthalmology, and radiology. Social workers and the child protection team, which may include members from law enforcement, will facilitate the legal investigation.
The healthcare team’s primary role is to evaluate and respond to a child’s medical needs. This evaluation and treatment is a part of the entire child maltreatment investigation, which goes beyond the healthcare evaluation and includes the child’s environment and the people and situations to which the child is exposed. The role of the healthcare team is not to determine who was the abuser or perpetrator but, along with the child protection team, to identify the medical problems, determine what injuries are present and treat those injuries, and offer honest medical information to parents and families. Caring for the victim of AHT can be emotionally challenging for the entire healthcare team. Nurses should confront their own perceptions and beliefs about AHT and child abuse, as it may have an impact on the care provided to abused children and their families. Nurses must treat this patient and family the same as the other patient and family with a different diagnosis.
10.6.3 Legal Implications
All 50 states in the United States have statutes that require the reporting of suspected child abuse or neglect by all healthcare providers, including nurses, though the process for making such reports may vary by state. There need only be suspicion of inflicted injury or abuse, and not certainty of proof, to meet mandatory reporting requirements. All states have eliminated the right of confidentiality when child abuse is suspected. Failure to report suspected abuse leaves the child at risk for further physical abuse and death and may potentially put other children at risk for abuse (Hornor 2012). Healthcare providers who fail to report suspicions of abuse place themselves at risk of professional liability.
Other nations such as Australia, Brazil, Canada, and most of the European Union also have reporting requirements. Nurses should be familiar with their local laws and advocate for the enactment of such laws where they don’t exist.
10.7 Care of the Family
10.7.1 Patient and Family Education
The family of the child experiencing AHT will need information to help them understand the child’s condition, medical plan, and anticipated prognosis. Because the investigation required when AHT is suspected evolves over time, families will need anticipatory guidance about what to expect and the roles of the various healthcare team members. Social services or other family support workers may be needed to assist with managing emotional family dynamics.
10.7.2 Siblings
Any siblings of the patient will need special consideration. After their safety has been assured, they will likely need to undergo a physical examination to make certain they are not also injured. As possible witnesses to abuse and violence, siblings will need developmentally appropriate support and interventions to meet their emotional needs. Nurses, child life therapists, and social workers are in prime positions to provide this type of care.
10.8 Prevention Efforts
The personal costs to the victim, coupled with the financial costs to society, make preventing child abuse and abusive head trauma a priority.
10.8.1 Primary Prevention
Primary prevention activities are those designed to raise the awareness of the general public about the scope and magnitude of the problems associated with AHT. For instance, parental education should take place in the newborn nursery and at routine newborn examinations (Allen 2014; Altman et al. 2011; Dias et al. 2005; Simonnet et al. 2014). These are ideal opportunities to provide anticipatory guidance about dealing with the frustration of a crying baby and the harm that can result from shaking an infant (Flaherty et al. 2010). The Period of PURPLE Crying (http://purplecrying.info) is an intervention that can educate parents about why infants cry, what increases the infant’s risk of trauma, and skills adult caregivers can use to soothe a crying baby and manage their frustration and anger (Allen 2014). Many states also have telephone hot lines that parents can call if they are feeling stressed and overwhelmed. Emphasis should also be placed on the importance of leaving a young infant or toddler in the care of adults whom the parents trust will not harm their child.
Home-visiting programs focus on educating parents on child development and parenting skills, so they can provide a safe home environment. One example is the Nurse-Family Partnership (http://nursefamilypartnership.org), which is a free, voluntary program that partners first-time parents with a nurse, who visits the home until the child is 2 years of age (Nurse-Family Partnership 2016). There are locations in over 43 states and the US Virgin Islands. Additional education services include the National Center on Shaken Baby Syndrome (http://dontshake.org), which has a mission to “Prevent shaken baby syndrome and promote the well-being of infants generally through the development and implementation of programs, policy and research; and to support and educate families, caregivers and professionals” (National Center on Shaken Baby Syndrome 2016). The center serves as a resource for prevention programs, training courses, and public education campaigns for professionals and families.
10.8.2 Secondary Prevention
Secondary prevention involves initiatives that are geared toward children and families who are known to be at higher risk for maltreatment and AHT. Those considered at risk include substance-abusing parents, young mothers, those with developmental disabilities, and those living in socioeconomic stress (Chevignard and Lind 2014). For example, because of the high concordance between domestic violence and child maltreatment, families should be screened for domestic violence at every entry into the healthcare system. Screening can and should occur during well-child visits, as a part of routine social histories, and when a child presents with findings or a history worrisome for possible maltreatment (Institute of Medicine and National Research Council 2014).
10.8.3 Tertiary Prevention
Finally tertiary prevention focuses on families in which abuse or neglect has already occurred. The goal at this point is to prevent the recurrence of maltreatment and reduce the long-term consequences and burden of abuse. Activities can include counseling, parent mentor programs, and programs designed to improve family communication and functioning (Institute of Medicine and National Research Council 2014).
10.9 Outcomes
10.9.1 Victim Outcomes
Outcomes for children experiencing AHT range from mild disability to death, depending on the severity of the head injury and other concomitant injuries. Factors associated with an increased risk of dying from AHT include an initial GCS of ≤5, retinal hemorrhage, intraparenchymal hemorrhage and cerebral edema, and refractory intracranial hypertension with cerebral hypoperfusion (Miller Ferguson et al. 2016; Shein et al. 2012). Of survivors, approximately one third will have a good outcome. The remaining two thirds will experience some level of disability, with half of those having severe problems, such as microcephaly, chronic subdural hematoma, obstructive hydrocephalus, epilepsy, hemiparesis, quadriparesis, psychomotor impairment, and visual deficit, including blindness (Fanconi and Lips 2010; Miller et al. 2014). Many of these severely affected children become dependent on technology such as tracheostomy tubes, ventilators, and gastrostomy tubes. More than half of severely injured victims of AHT die before the age of 21 (Miller et al. 2014). Other effects of child abuse and AHT include delayed development, poor school performance, and other mental health problems such as depression, suicidal ideation, and post-traumatic stress disorder.
10.9.2 Costs
All of these outcomes carry tremendous family and society costs. The dollar value attributed to AHT for one child over the first 4 years following diagnosis is nearly $48,000 (Peterson et al. 2014). It is estimated that it costs over $69 million yearly in the United States to care for victims of AHT (Peterson et al. 2015). These estimates do not include related nonmedical costs such as special education, and many children will need extensive medical care for the remainder of their lives. Victims of AHT have greater need for medical services, are more frequently hospitalized, and require more medication than non-abused children, all of which have financial implications (Peterson et al. 2014).
Box 10.1 Abusive Head Trauma: Case Study
History:
CP was a previously healthy 6-month-old male who by history was found limp after his father returned from outside where he had been smoking a cigarette around 8:00 pm. The father indicates he was watching the child while the mother was at work and that he had placed the baby in a bouncy seat prior to going outside. After finding the baby unresponsive, he ran two blocks to a convenience store and called 911. On arrival, EMS noted decerebrate posturing. Oxygen was applied and the child was transported from the scene to a pediatric emergency room.
Physical exam findings:
-
General: Well nourished, high-pitched irritable weak cry
-
HEENT: Pupils equal and reactive, right eye deviation
-
Lungs: Irregular respiratory pattern with periods of apnea, RR 16–30
-
CV: HR 140, sinus tachycardia, BP 96/42, capillary refill <2 s
-
Abdomen: Soft, non-tender, no organomegaly or palpable masses
-
Extremities: Decerebrate posturing of all extremities
-
Neurologic: Fontanel full, weak cry, GCS 8 (eye opening to pain only, 2 points; verbal response irritable cry, 4 points; motor response decerebrate (abnormal extension) posture, 2 points)
-
Skin: Bruising on left temporal area and soft tissue swelling over left parietal and occipital areas, mucus membranes moist
Diagnostic findings:
-
Head CT: Left subdural and subarachnoid hemorrhages, nondisplaced left posterior skull fracture (Fig. 10.3), loss of gray-white differentiation consistent with hypoxic injury and cerebral edema
-
Abdominal/pelvic CT: Normal
-
Skeletal survey: Left second rib with healing posterior fracture
-
Ophthalmology: Bilateral preretinal and intraretinal hemorrhages too numerous to count, extending from the posterior pole
-
Laboratory: Complete metabolic panel normal. Hemoglobin and hematocrit, platelet count, and urinalysis all normal
Assessment:
Abusive head trauma with severe traumatic brain injury
Additional information:
The baby’s father was detained at the scene by law enforcement and was then taken to the police station for further questioning. His initial story was vague, describing the child as suddenly becoming unresponsive. During further questioning, he gave various and changing stories about how the baby was injured.
When the child’s mother arrived at the hospital, she was visibly upset and concerned about her son’s condition. She was initially supported by the social worker in the emergency department and interviewed in further detail later in the pediatric intensive care unit (PICU).
The baby is the result of an unplanned pregnancy. The parents are in their early 20s and unmarried, though they have been in a relationship for 2.5 years. They have no other children. The mother works second shift full-time at a grocery store, while the father provides child care. The father is unemployed but is looking for a job. There are no other caretakers and the baby is not in daycare. In terms of stressors, the mother reports some financial strain since the father is unemployed. She also reports that the father suffers from ADHD and bipolar disorder and is supposed to be on medication, which he takes inconsistently. She indicates that she and the baby’s father regularly drink alcohol but denies drug use. There is also a reported history of domestic violence by the father against the mother, but she states that she has never witnessed the father being violent with the baby.
Before the baby’s mother went to work on the day of the event, she noted that the child was playful and happy. She did not notice any bruising and said that she was not aware of any injuries the baby might have sustained over the past several days.
Management:
Because of the child’s periodic breathing and low GCS, he was intubated in the emergency room and subsequently received a 20 mL/kg normal saline bolus. After completing medical imaging, the baby was admitted to the PICU where central venous and arterial catheters were placed for invasive monitoring. Neurosurgical intervention consisted of placement of a ventriculostomy with ICP monitoring. The ICP was initially in the single digits, but the child developed intracranial hypertension over the next few days, which was treated with appropriate traumatic brain injury management interventions, including sedation and cerebral spinal fluid drainage. The baby developed seizures within 24 h of admission, was placed on cEEG monitoring, and started on antiepileptic medication. He was ultimately placed on pentobarbital and hypertonic saline infusions to control the seizures and refractory intracranial hypertension.
The child slowly improved and required ICP monitoring for 15 days. After 3 weeks of intubation, he was successfully extubated without the need for a tracheostomy tube. During hospitalization enteral nutrition was delivered via a transpyloric feeding tube, and he was subsequently transferred out of the PICU to the general pediatric unit with this tube still in place.
Outcomes:
The baby remained hospitalized for just over 3 months. During that time, it was determined that he could not eat by mouth and a gastrostomy tube was placed for enteral nutrition. His vision is questionable and he does not focus or track. He has hypertonia and does not sit up, does not hold his head up unassisted, and does not grasp toys. He continues to need antiepileptic medication. The baby’s mother received ongoing support from the hospital social worker and pediatric nurses and she was taught to care for her son so he could be discharged home. He will continue to need ongoing physical, occupational, and speech therapy and will need an early intervention program and ongoing support indefinitely. The child’s father ultimately plead guilty to child endangering, was fined $10,000, and sentenced to 4 years in prison.
Pearls
-
Accidental injury is uncommon in children under 2 years of age. Strongly consider an inflicted mechanism when the caregiver(s) explanation does not match the resultant injuries or when key aspects of the history/story change over time.
-
Classic injuries associated with abusive head trauma are subdural hematoma, retinal hemorrhages, and rib fractures. However, not all injuries may be present.
-
Be cognizant of potential opportunities to identify abusive injuries. Over half of children who are fatally abused are evaluated in a clinic or emergency department in the 2 months prior to their death. Detecting sentinel injuries early may prevent additional abusive events.
-
It can be difficult to distinguish accidental injury from abusive head trauma. Apnea is a critical distinguishing feature for AHT compared to accidental head injury, having a positive predictive value of 93%.
-
Preventing abusive head trauma is paramount, and additional research is needed to determine effective strategies for primary, secondary, and tertiary prevention.
References
Adamsbaum C, Grabar S, Mejean N, Rey-Salmon C (2010) Abusive head trauma: Judicial admissions highlight violent and repetitive shaking. Pediatrics 126(3):546–555. doi:10.1542/peds.2009-3647
Agrawal S, Peters MJ, Adams GG, Pierce CM (2012) Prevalence of retinal hemorrhages in critically ill children. Pediatrics 129(6):e1388–e1396. doi:10.1542/peds.2011-2772
Allen KA (2014) The neonatal nurse’s role in preventing abusive head trauma. Adv Neonatal Care Off J Natl Assoc Neonatal Nurses 14(5):336–342. doi:10.1097/ANC.0000000000000117
Altman RL, Canter J, Patrick PA, Daley N, Butt NK, Brand DA (2011) Parent education by maternity nurses and prevention of abusive head trauma. Pediatrics 128(5):e1164–e1172. doi:10.1542/peds.2010-3260
Arndt DH, Lerner JT, Matsumoto JH, Madikians A, Yudovin S, Valino H et al (2013) Subclinical early posttraumatic seizures detected by continuous EEG monitoring in a consecutive pediatric cohort. Epilepsia 54(10):1780–1788. doi:10.1111/epi.12369
Barlow KM, Minns RA (2000) Annual incidence of shaken impact syndrome in young children. Lancet 356(9241):1571–1572
Binenbaum G, Forbes BJ (2014) The eye in child abuse: key points on retinal hemorrhages and abusive head trauma. Pediatr Radiol 44(Suppl 4):S571–S577. doi:10.1007/s00247-014-3107-9
Caffey J (1946) Multiple fractures in the long bones of infants suffering from chronic subdural hematoma. Am J Roentgenol Radium Ther 56(2):163–173
Caffey J (1972) On the theory and practice of shaking infants. its potential residual effects of permanent brain damage and mental retardation. Am J Dis Child 124:161–169
Campbell KA, Olson LM, Keenan HT (2015) Critical elements in the medical evaluation of suspected child physical abuse. Pediatrics 136(1):35–43. doi:10.1542/peds.2014-4192
Chevignard MP, Lind K (2014) Long-term outcome of abusive head trauma. Pediatr Radiol 44(Suppl 4):S548–S558. doi:10.1007/s00247-014-3169-8
Christian CW, Committee on Child Abuse and Neglect (2015) The evaluation of suspected child physical abuse. Pediatrics 136(3):583–2010. doi:10.1542/peds.2015-2010
Christian CW, Block R, Committee on Child Abuse and Neglect, American Academy of Pediatrics (2009) Abusive head trauma in infants and children. Pediatrics 123(5):1409–1411. doi:10.1542/peds.2009-0408
Dias MS, Smith K, DeGuehery K, Mazur P, Li V, Shaffer ML (2005) Preventing abusive head trauma among infants and young children: a hospital-based, parent education program. Pediatrics 115(4):e470–7. doi:115/4/e470 [pii]
Fanconi M, Lips U (2010) Shaken baby syndrome in switzerland: results of a prospective follow-up study, 2002–2007. Eur J Pediatr 169(8):1023–1028. doi:10.1007/s00431-010-1175-x
Flaherty EG, Stirling J Jr, American Academy of Pediatrics, Committee on Child Abuse and Neglect (2010) Clinical report-the pediatrician’s role in child maltreatment prevention. Pediatrics 126(4):833–841
Flaherty EG, Perez-Rossello JM, Levine MA, Hennrikus WL, American Academy of Pediatrics Committee on Child Abuse and Neglect, Section on Radiology, American Academy of Pediatrics et al (2014) Evaluating children with fractures for child physical abuse. Pediatrics 133(2):e477–e489. doi:10.1542/peds.2013-3793
Guthkelch AN (1971) Infantile subdural haematoma and its relationship to whiplash injuries. Br Med J 2(5759):430–431
Hasbani DM, Topjian AA, Friess SH, Kilbaugh TJ, Berg RA, Christian CW et al (2013) Nonconvulsive electrographic seizures are common in children with abusive head trauma*. Pediatr Crit Care Med J Soc Crit Care Med World Feder Pediatr Intens Crit Care Soc 14(7):709–715. doi:10.1097/PCC.0b013e3182917b83
Hettler J, Greenes DS (2003) Can the initial history predict whether a child with a head injury has been abused? Pediatrics 111(3):602–607
Hobbs C, Childs AM, Wynne J, Livingston J, Seal A (2005) Subdural haematoma and effusion in infancy: an epidemiological study. Arch Dis Child 90(9):952–955. doi:90/9/952 [pii]
Hornor G (2012) Medical evaluation for child physical abuse: what the PNP needs to know. J Pediatr Health Care Off Publ Natl Assoc Pediatr Nurse Assoc Pract 26(3):163–70; quiz 171–3. doi:10.1016/j.pedhc.2011.10.001
Institute of Medicine, National Research Council (2014) New directions in child abuse and neglect research. The National Academies Press, Washington, DC
Kadom N, Khademian Z, Vezina G, Shalaby-Rana E, Rice A, Hinds T (2014) Usefulness of MRI detection of cervical spine and brain injuries in the evaluation of abusive head trauma. Pediatr Radiol 44(7):839–848. doi:10.1007/s00247-014-2874-7
Kelly P, Farrant B (2008) Shaken baby syndrome in new zealand, 2000–2002. J Paediatr Child Health 44(3):99–107
Kemp AM (2011) Abusive head trauma: Recognition and the essential investigation. Arch Dis Child Educ Pract Ed 96(6):202–208. doi:10.1136/adc.2009.170449
Kemp AM, Jaspan T, Griffiths J, Stoodley N, Mann MK, Tempest V, Maguire SA (2011) Neuroimaging: What neuroradiological features distinguish abusive from non-abusive head trauma? A systematic review. Arch Dis Child 96(12):1103–1112. doi:10.1136/archdischild-2011-300630
Kempe CH, Silverman FN, Steele BF, Droegemueller W, Silver HK (1962) The battered-child syndrome. JAMA 181:17–24
Laghmari M, Skiker H, Handor H, Mansouri B, Ouazzani Chahdi K, Lachkar R et al (2014) Birth-related retinal hemorrhages in the newborn: incidence and relationship with maternal, obstetric and neonatal factors. prospective study of 2,031 cases. [Hemorragies retiniennes liees a l’accouchement chez le nouveau-ne : frequence et relation avec les facteurs maternels, neonataux et obstetricaux. Etude prospective de 2031 cas]. J Fr D’Ophtalmol 37(4):313–319. doi:10.1016/j.jfo.2013.06.005
Liley W, Stephens A, Kaltner M, Larkins S, Franklin RC, Tsey K et al (2012) Infant abusive head trauma – incidence, outcomes and awareness. Aust Fam Physician 41(10):823–826
Longmuir SQ, McConnell L, Oral R, Dumitrescu A, Kamath S, Erkonen G (2014) Retinal hemorrhages in intubated pediatric intensive care patients. J AAPOS Off Publ Am Assoc Pediatr Ophthalmol Strabismus Am Assoc Pediatr Ophthalmol Strabismus 18(2):129–133. doi:10.1016/j.jaapos.2013.12.005
Lopes NR, Eisenstein E, Williams LC (2013) Abusive head trauma in children: a literature review. J Pediatr 89(5):426–433. doi:10.1016/j.jped.2013.01.011
Maguire S, Pickerd N, Farewell D, Mann M, Tempest V, Kemp AM (2009) Which clinical features distinguish inflicted from non-inflicted brain injury? A systematic review. Arch Dis Child 94(11):860–867. doi:10.1136/adc.2008.150110
Maguire SA, Kemp AM, Lumb RC, Farewell DM (2011) Estimating the probability of abusive head trauma: a pooled analysis. Pediatrics 128(3):e550–e564. doi:10.1542/peds.2010-2949
Maguire SA, Watts PO, Shaw AD, Holden S, Taylor RH, Watkins WJ et al (2013) Retinal haemorrhages and related findings in abusive and non-abusive head trauma: a systematic review. Eye (London, England) 27(1):28–36. doi:10.1038/eye.2012.213
Melo JR, Di Rocco F, Bourgeois M, Puget S, Blauwblomme T, Sainte-Rose C et al (2014) Surgical options for treatment of traumatic subdural hematomas in children younger than 2 years of age. J Neurosurg Pediatr 13(4):456–461. doi:10.3171/2014.1.PEDS13393
Miller Ferguson N, Shein SL, Kochanek PM, Luther J, Wisniewski SR, Clark RS et al (2016) Intracranial hypertension and cerebral hypoperfusion in children with severe traumatic brain injury: thresholds and burden in accidental and abusive insults. Pediatr Crit Care Med J Soc Crit Care Med World Feder Pediatr Intens Crit Care Soc. doi:10.1097/PCC.0000000000000709
Miller TR, Steinbeigle R, Wicks A, Lawrence BA, Barr M, Barr RG (2014) Disability-adjusted life-year burden of abusive head trauma at ages 0–4. Am Acad Pediatr 134(6):1545–1550. doi:10.1542/peds.2014-1385
Narang S, Clarke J (2014) Abusive head trauma: past, present, and future. J Child Neurol 29(12):1747–1756. doi:10.1177/0883073814549995
National Center on Shaken Baby Syndrome (2016) National center on shaken baby syndrome: about us Retrieved from http://dontshake.org/about-us
Ortega HW, Vander Velden H, Kreykes NS, Reid S (2013) Childhood death attributable to trauma: is there a difference between accidental and abusive fatal injuries? J Emerg Med 45(3):332–337. doi:10.1016/j.jemermed.2013.03.020
Parks SE, Annest JL, Hill HA, Karch DL (2012) Pediatric abusive head trauma: recommended definitions for public health surveillance and research. Centers for Disease Control and Prevention, Atlanta
Nurse-Family Partnership (2016) Nurse-family partnership fact sheet Retrieved from http://www.nursefamilypartnership.org/getattachment/about/fact-sheets/NFP_February_2016_Snapshot-(6).pdf.aspx
Paul AR, Adamo MA (2014) Non-accidental trauma in pediatric patients: a review of epidemiology, pathophysiology, diagnosis and treatment. Transl Pediatr 3(3):195–207. doi:10.3978/j.issn.2224-4336.2014.06.01
Peterson C, Xu L, Florence C, Parks SE, Miller TR, Barr RG et al (2014) The medical cost of abusive head trauma in the united states. Pediatrics 134(1):91–99. doi:10.1542/peds.2014-0117
Peterson C, Xu L, Florence C, Parks SE (2015) Annual cost of U.S. hospital visits for pediatric abusive head trauma. Child Maltreat 20(3):162–169. doi:10.1177/1077559515583549
Pierce MC, Kaczor K, Aldridge S, O’Flynn J, Lorenz DJ (2010) Bruising characteristics discriminating physical child abuse from accidental trauma. Pediatrics 125(1):67–74. doi:10.1542/peds.2008-3632
Piteau SJ, Ward MG, Barrowman NJ, Plint AC (2012) Clinical and radiographic characteristics associated with abusive and nonabusive head trauma: a systematic review. Pediatrics 130(2):315–323. doi:10.1542/peds.2011-1545
Roach JP, Acker SN, Bensard DD, Sirotnak AP, Karrer FM, Partrick DA (2014) Head injury pattern in children can help differentiate accidental from non-accidental trauma. Pediatr Surg Int 30(11):1103–1106. doi:10.1007/s00383-014-3598-3
Roche AJ, Fortin G, Labbe J, Brown J, Chadwick D (2005) The work of ambroise tardieu: the first definitive description of child abuse. Child Abuse Negl 29(4):325–334
Ryan ME, Palasis S, Saigal G, Singer AD, Karmazyn B, Dempsey ME et al (2014) ACR appropriateness criteria head trauma – child. J Am Coll Radiol JACR 11(10):939–947. doi:10.1016/j.jacr.2014.07.017
Shaahinfar A, Whitelaw KD, Mansour KM (2015) Update on abusive head trauma. Curr Opin Pediatr 27(3):308–314. doi:10.1097/MOP.0000000000000207
Shanahan ME, Zolotor AJ, Parrish JW, Barr RG, Runyan DK (2013) National, regional, and state abusive head trauma: application of the CDC algorithm. Pediatrics 132(6):e1546–e1553. doi:10.1542/peds.2013-2049
Sheets LK, Leach ME, Koszewski IJ, Lessmeier AM, Nugent M, Simpson P (2013) Sentinel injuries in infants evaluated for child physical abuse. Pediatrics 131(4):701–707. doi:10.1542/peds.2012-2780
Shein SL, Bell MJ, Kochanek PM, Tyler-Kabara EC, Wisniewski SR, Feldman K et al (2012) Risk factors for mortality in children with abusive head trauma. J Pediatr 161(4):716–722.e1. doi:10.1016/j.jpeds.2012.03.046
Sieswerda-Hoogendoorn T, Boos S, Spivack B, Bilo RA, van Rijn RR (2012) Educational paper: abusive head trauma part I. clinical aspects. Eur J Pediatr 171(3):415–423. doi:10.1007/s00431-011-1598-z
Simonnet H, Laurent-Vannier A, Yuan W, Hully M, Valimahomed S, Bourennane M, Chevignard M (2014) Parents’ behavior in response to infant crying: abusive head trauma education. Child Abuse Negl 38(12):1914–1922. doi:10.1016/j.chiabu.2014.06.002
US Department of Health and Human Services, Administration for Children and Families, Administration on Children, Youth, and Families, Children’s Bureau (2012) Child maltreatment 2012. Government Printing Office, Washington, DC
Yamazaki J, Yoshida M, Mizunuma H (2014) Experimental analyses of the retinal and subretinal haemorrhages accompanied by shaken baby syndrome/abusive head trauma using a dummy doll. Injury 45(8):1196–1206. doi:10.1016/j.injury.2014.04.014
Zuccoli G, Panigrahy A, Haldipur A, Willaman D, Squires J, Wolford J et al (2013) Susceptibility weighted imaging depicts retinal hemorrhages in abusive head trauma. Neuroradiology 55(7):889–893. doi:10.1007/s00234-013-1180-7
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Mullen, J.E. (2017). Abusive Head Trauma. In: Cartwright, C., Wallace, D. (eds) Nursing Care of the Pediatric Neurosurgery Patient. Springer, Cham. https://doi.org/10.1007/978-3-319-49319-0_10
Download citation
DOI: https://doi.org/10.1007/978-3-319-49319-0_10
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-49318-3
Online ISBN: 978-3-319-49319-0
eBook Packages: MedicineMedicine (R0)