
Abstract
Cerebral palsy is caused by early damage to the developing brain, as the most common pediatric neurological disorder. Hemiplegia (unilateral spastic cerebral palsy) is the most common subtype, and the resulting impairments, lateralized to one body side, especially affect the upper extremity, limiting daily function. This chapter first describes the pathophysiology and mechanisms underlying impaired upper extremity control of cerebral palsy. It will be shown that the severity of impaired hand function closely relates to the integrity of the corticospinal tract innervating the affected hand. It will also shown that the developing corticospinal tract can reorganize its connectivity depending on the timing and location of CNS injury, which also has implications for the severity of hand impairments and rehabilitation. The mechanisms underlying impaired motor function will be highlighted, including deficits in movement execution and planning and sensorimotor integration. It will be shown that despite having unimanual hand impairments, bimanual movement control deficits and mirror movements also impact function. Evidence for motor learning-based therapies including Constraint-Induced Movement Therapy and Bimanual Training, and the possible pathophysiological predictors of treatment outcome and plasticity will be described. Finally, future directions for rehabilitations will be presented.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Sensorimotor integration
- Constraint-induced movement therapy
- Bimanual
- Jense-Taylor test
- Hand function
- Corticospinal pathways (CST)
- Object-release coordination
- Motor planning
- Thalamocortical
- Stereognosis
- Mirror movements
Introduction
Cerebral palsy (CP) is the most common pediatric neurological disorder. CP is caused by damage to the brain during early development. Unilateral spastic cerebral palsy (USCP) (often referred to as hemiplegic CP), with motor impairments mainly lateralized to one body side, is the most common subtype, accounting for 30–40 % of newly diagnosed cases (Himmelmann et al. 2005). In this chapter, the pathophysiology and mechanisms underlying impaired upper extremity (UE) control of USCP will be reviewed. The specific pathophysiology will be related to the severity of UE impairments, where clear relationships between the type and the extent of early brain damage and/or the resulting reorganization of the developing nervous system will be demonstrated. The evidence for motor-learning based therapies will be discussed, including possible pathophysiological predictors of treatment outcome and the associated neuroplasticity.
Pathophysiology of Unilateral Spastic CP
Corticospinal (CST) pathways from motor areas, especially the primary motor cortex (M1), develop in a corticofugal manner, approaching the spinal cord by the 20th week of gestation during typical development (see Staudt 2010). Thereafter these pathways undergo synaptogenesis, with targeted projections to the spinal–segmental level. The motor cortices are initially believed to develop bilateral projections (i.e., projections to both the contralateral and ipsilateral UEs) (Eyre et al. 2001). There is a gradual weakening of ipsilateral projections, and strengthening of contralateral projections via synaptic competition during continuing development (Staudt 2010), which is driven by M1 activity (see Friel et al. 2013). This is evidenced by studies of the developing CST in kittens, whereby blockade of M1 activity either by injection of a GABA-agonist or restraint of a forelimb, prevents the CST from establishing spinal connectivity, and results in permanent motor impairments (Friel et al. 2013). In humans, this intricate process is susceptible to prenatal and perinatal brain damage. Since the CST directly innervate hand motoneurons, which provide the capacity for selective UE movement control (Lawrence and Kuypers 1968), permanent impairments in manual dexterity may occur following damage to this developing system.
USCP is often the result of periventricular lesions, middle cerebral artery infarct, hemi-brain atrophy, brain malformation or posthemorrhagic porencephaly (e.g., Uvebrandt 1988; Cioni et al. 1999). As described above, motor areas and CST integrity are often compromised (e.g., Staudt et al. 2004; Bleyenheuft et al. 2007). The specific etiology may drastically influence subsequent development of CST pathways (Staudt 2010). The severity of upper extremity impairments largely depends on the extent of damage to the CST (e.g., Bleyenheuft et al. 2007; Scheck et al. 2012). The damage can be approximated using both conventional MRIs and diffusion tensor imaging, by measuring the asymmetry in the cross-sectional area of the cerebral peduncles through which the CST passes through (e.g., Bleyenheuft et al. 2007; Friel et al. 2014), or measuring the fractional anisotropy (Bleyenheuft et al. 2007). The asymmetry in the CST innervating each hand is strongly related to severity of manual dexterity impairments. This can be seen in Fig. 1A, where the index of asymmetry (ratio of the affected to unaffected peduncle size) is highly correlated to manual dexterity, as measured by the time to complete the Jebsen-Taylor Test of Hand Function (Friel et al. 2014). The timing of CST damage is also predictive of outcome. Cortical malformation in the first two trimesters typically results in less severe upper extremity impairments than periventricular lesions in the early, and MCA later, in the third trimester (Fig. 1b, Staudt et al. 2004). Disruptions during the intrauterine period can reduce or abolish neuronal activity in CST projections originating in the affected hemisphere. The altered activity can result in ipsilateral being maintained and strengthened during further development, with contralateral projections being partly or completely eliminated (Staudt et al. 2004; Eyre et al. 2007; see Staudt 2010) (Fig. 1c). On average, individuals who undergo such ipsilateral reorganization have more severely affected upper extremity function Fig. 1d, Holmström et al. (2010) and often the persistence of mirror movements. This reorganization may represent functional compensation of the affected hemisphere by the unaffected hemisphere. The extent to which this ipsilateral reorganization is able to compensate for the absent contralateral projections decreases with age at the time of damage (Staudt et al. 2004). CST projections from M1 to spinal interneurons, thus indirectly innervating hand muscles, are also impaired, further affecting coordination and reflex control (Harrison 1988). The net result of the early brain damage is impairments in movement execution, movement planning, sensorimotor control and the ability to coordinate the two hands together (bimanual control). These impairments are described below in relation to the pathophysiology of CP.

a Peduncle asymmetry predicts baseline unimanual dexterity (Jebsen-Taylor Test). Inset t1-weighted MRI showing cerebral peduncles, outlined. Modified from Friel et al. (2014). b Comparison of hand motor dysfunction scores among patients with congenital brain injuries acquired during the trimesters of gestation (malformations of cortical development [MCD], first and second trimester of pregnancy; periventricular [PV] lesions, early third trimester of pregnancy; middle cerebral artery [MCA] infarctions, late third trimester of pregnancy). Open circles, individuals with preserved crossed corticospinal projections from the affected hemispheres; filled circles, individuals with reorganized ipsilateral projections from the contralesional hemispheres; half-filled circles, individuals with both preserved contralateral and reorganized ipsilateral corticospinal projections to the more affected hand. Modified from Staudt et al. (2004). c Relation between box and blocks score (higher score represents greater dexterity) using the more affected hand and the CST motor projection pattern to the hand, assessed using transcranial magnetic stimulation (TMS). Modified from Holmström et al. (2010)
Movement Execution Impairments
As a result of damage to the developing motor pathways, there are impairments in the execution of upper extremity movements. For example, the upper extremity is often weak, and the lack of selective finger movements, limits the ability to achieve many grasp forms (e.g., precision grip). Thus movements are unskilled, slow and clumsy (Brown et al. 1987).
Manual motor control has been quantified for more than three decades via the examination of fingertip forces during precision grasping. Fingertip coordination in typically developing (TD) children reaches near adult-like coordination by 6–8 years of age (see Gordon 2001). Conversely, children with CP at this age often have infantile-like force coordination, with prolonged delays between movement phases (e.g., between grasp contact and force initiation) and reduced coupling of grip and load force (Eliasson et al. 1991; Prabhu et al. 2011). While most children with CP are capable of adjusting their fingertip forces to the object’s weight and texture, their forces are often excessive and variable, with reduced adaptation to the object’s weight and texture compared to TD children (Eliasson et al. 1992). Object release coordination is also impaired (Eliasson and Gordon 2000), which is exacerbated when speed and accuracy constraints are imposed (Gordon et al. 2003). Fortunately, precision grip in children with CP does improve with development (Eliasson et al. 2006) and extensive practice (Gordon and Duff 1999a), which has helped inspired the development of intensive rehabilitation protocols (e.g., constraint-induced movement therapy; CIMT) (Gordon 2011, 2014).
Motor Planning Impairments
Perhaps an unappreciated aspect of the motor control deficits is that individuals with unilateral spastic CP also have higher level impairments in motor planning (see Steenbergen et al. 2013). These impairments can impact precision grasping. Due to delays in feedback, the development of fingertip forces during grasp must be planned before initiation. Furthermore, sensory information about some object properties (e.g., weight) is not available until after lift off. Motor planning for grasp control involves the formation and utilization of internal models of objects based on previous experience manipulating the object (see Gordon and Duff 1999a). Children with unilateral spastic CP have an impaired ability to scale the amplitude of the force development to the known object properties in their more affected hand (Gordon et al. 1999). The impairments in force planning are reduced following extensive practice (Gordon and Duff 1999a), providing a template for intensive rehabilitation training. The planning deficits may partially reflect impaired motor learning, involving extracting appropriate sensory information to form internal models, and integrating it with motor commands during subsequent actions.
Children with unilateral spastic CP often demonstrate ‘global planning’ impairments that are independent of the effector used (see Steenbergen et al. 2013). Oddly, the force scaling deficits during object lifting (Eliasson et al. 1992; Gordon and Duff 1999a) and grip force coupling (Gordon et al. 2006a, b) are effector dependent, where deficits are solely seen in the more affected, and not the less affected UE. A similar finding during load force perturbations has been observed, with participants unable to anticipate the consequences of a dynamic perturbations (Bleyenheuft and Thonnard 2010). An interesting, and potentially transformative, finding is that following several lifts with the less affected hand, anticipatory planning, reflected by the rate of force development matching the object’s weight, is immediately present in the more affected hand; i.e., there is a transfer of sensorimotor information and improvement in motor function (Gordon et al. 1999). In a subsequent study (Gordon et al. 2006a, b), we found that despite the normal of anticipatory force scaling during successive lifts with the more affected hand, anticipatory force scaling is transferred from the more affected to the less affected hand. Thus, the lack of anticipatory control during normal use of the more affected hand is not due to impaired sensation, yielding insufficient internal models. Instead, these findings suggest that the impaired planning may be due to an inability to integrate sensory information with the motor output in the more affected hand. Simultaneous grasp and lift of an object in each hand improved some aspects of grip performance as well (Steenbergen et al. 2008), although the grip-lift movements became slower, likely due to the requirement to divide attention between the two hands. These findings helped motivate the development of intensive bimanual training approaches (e.g., Hand-arm bimanual intensive therapy; HABIT) described below (Gordon 2011, 2014).
Sensorimotor Impairments
Thalamocortical somatosensory projections achieve connectivity in their cortical termination sites during the third trimester. These connections normally are not damaged by PVL, or they may circumvent the lesion to terminate in the postcentral gyrus (see Staudt 2010). In contrast, MCA lesions, occurring later and in many instances affecting the postcentral gyrus, are more likely to affect the somatosensory system (Staudt 2010). Thus, children with USCP, especially of MCA origin, often have accompanying sensory impairments, which may further compromise fine motor coordination (Brown et al. 1987; Moberg 1962). Tactile perception and discrimination, stereognosis and proprioception are often disturbed (e.g., Gordon and Duff 1999b, Bleyenheuft and Thonnard 2011) with the amount of impairment related to the integrity of afferent pathways (see Scheck et al. 2012). These sensory impairments may contribute to precision grip impairments found in CP (Gordon and Duff 1999b) as they resemble precision grip impairments following digital anesthesia in healthy adults; i.e., higher and more variable grasping forces (e.g., Johansson and Westling 1984). Although there appears to be improvements in both sensory acuity and motor function following training, the relationship between sensory and motor abilities is not fixed. Such relationships have been established between stereognosis and motor function (Gordon and Duff 1999b), but conflicting results are reported for other modalities.
Bimanual Coordination Impairments
Children with unilateral spastic CP have deficits in bimanual coordination above and beyond unimanual dexterity deficits (e.g., Steenbergen et al. 1996, 2000; see Gordon and Steenbergen 2008). Similar to motor planning, the relation between the type and timing of the lesion and bimanual coordination impairments are not known. During symmetrical, bimanual reaching tasks, children with unilateral spastic CP do coordinate their bimanual movements by compensating with their noninvolved hand, as long as the accuracy demands or task complexity are not increased. In one recent study, participants were instructed to hold a grip device in each hand and place one device on top of the other while the grip and load force were recorded in each hand (Islam et al. 2011). Children with USCP initiated the task by decreasing grip force in the releasing hand before increasing the grip force in the holding hand during the preparation phase, with the subsequent grip force increase in the holding hand being reduced and occurring later (transition phase) than that of TD children. The impairments were unrelated to presence of mirror movements, and the impairment was greater when the less affected hand served as the holding hand.
In another series of studies (Hung et al. 2004, 2010), children were asked to open a drawer with one hand and manipulate its contents with the other hand. Children with USCP were less coordinated, with reduced movement overlap of the drawer opening hand and manipulating hand (and sequential completion of opening the drawer and manipulating its contents (Hung et al. 2010). Interestingly, as described later in this chapter, bimanual training improved some aspects of this coordination more than unimanual training (Hung et al. 2011).
While emphasis has been placed on CST connectivity to the affected hands in relation hand function (e.g., Bleyenheuft et al. 2007; Friel et al. 2014). However, the cause of hand impairments may not be as simple. For example, one study showed that reduced structural integrity of the corpus callosum in USCP was associated with reduced function of both the more- and less affected hands (Green et al. 2013). Interestingly, the corpus callosum integrity was also related to the quality of bimanual hand use (Fig. 2), which as described below, may be functionally more important.

Tractography of the corpus callosum (genu blue, midbody orange, splenium red) in a a TD child and b a child with unilateral CP. c Relationship between # of fibres in the splenium of the corpus callosum and Assisting Hand Assessment scores. Modified from Weinstein et al. (2013)
Mirror Movements
Many individuals with USCP have unintentional imitation of voluntary movement of the contralateral limb, known as mirror movements (Woods and Teuber, 1978). Conceivably, mirror movements could negatively impact effective performance of asymmetrical bimanual activities (e.g., tying shoes). They are believed to be caused by the ipsilateral CST projecting from the less affected M1 that innervates bilateral UEs (e.g., Carr et al. 1993; Farmer et al. 1991; Staudt et al. 2004) as described above, and/or impaired interhemispheric inhibition between the two M1s (Koerte et al. 2011).
Early studies examined the relationship between the timing of the brain injury, CST and mirror movements, quantifying mirror movements using various measures (Woods and Teuber 1978; Carr et al. 1993; Farmer et al. 1991). More recent studies demonstrated a negative impact on unimanual and bimanual hand function (Islam et al. 2011; Sukal-Moulton et al. 2013; Klingels et al. 2016; Kuhtz-Buschbeck et al. 2000; Adler et al. 2015). While individuals are able to voluntarily reduce the amplitude of mirror movements with attention (Kuhtz-Buschbeck et al. 2000), it is unknown whether mirror movements impact the ability to treat impaired hand function, or whether treatments can diminish their impact on function.
Rehabilitation of Upper Extremity Function
Motor Learning Approaches to Rehabilitation
A recent review of evidence supporting the clinical implementation of various therapeutic approaches identified only six approaches with sufficient evidence of efficacy (Novak et al. 2013). These were Constraint-induced movement therapy (CIMT), Intensive bimanual training, Goal-directed training, Context-specific training, Occupational therapy post botoxulinum toxin injections, and Home training. There were two commonalities across these approaches: all involved active movement of the participant using principles of motor learning, and all involved intensive practice.
Motor learning approaches to rehabilitation (often referred to as task-oriented or goal training) focuses on the effectiveness and efficiency of motor performance in specific actions, with activity limitations being an important aspect of CP (Bax et al. 2005) rather than on normalization of movement patterns or prevention of compensations (Carr and Shepherd 1989; Trombly 1995; Winstein and Wolf 2009). This approach is based on integrated models of motor learning and control and behavioral neuroscience. The focus is on participation and acquisition of skills and involves targeted physical and mental activity. The late eminent scholar, Ann Gentile, noted that: “The behaviour that dominates our daily lives is directed toward the accomplishment of goals. It is aimed at a specific purpose or end that we are trying to achieve” (Gentile 2000; p. 112). The approach recognizes task performance as being influenced by the person, the task and the environment (Gordon and Magill 2012). Problem solving is a key component, with the notion that the brain selects movement patterns that are available based on the constraints of the patient (Latash and Anson 1996). The associated behavioral demands of the tasks and motor skill training may be used to “shape” the desired movement pattern, and results in cortical reorganization (Plautz et al. 2000) underlying concurrent functional outcomes. For maximal efficacy, the training must be challenging, with progressively increasing behavioral demands, and involve active participation and problem solving. Skilled training in animals shows increased plasticity of UE cortical representations, whereas unskilled training did not (Kleim et al. 1998; Friel et al. 2012).
Constraint-Induced Movement Therapy
CIMT is an obvious choice for eliciting intensive unimanual practice. There was a strong scientific rationale based on animal models underlying the application of intensive practice-based approaches to human upper extremity (UE) rehabilitation (Tower 1940; Taub and Shee 1980). Starting with ‘forced use’ in adult stroke patients, in which the less affected UE was physically restrained to incentivize practice of the more affected UE (Wolf et al. 1989), subsequent efforts incorporated principles of behavioral psychology (shaping) and motor learning to elicit active practice of the affected UE. This active training approach along with the restraint become known as ‘Constraint-induced movement therapy’ (CIMT) (Taub and Wolf 1997). The first adaptation of the approach for the pediatric population leading to a case study was published more 15 years ago (Charles et al. 2001). Since then there have been many studies of CIMT to date, including more than 30 RCTs, with nearly all studies providing evidence of efficacy (see Dong et al. 2013; Eliasson et al. 2014).
The best age to conduct CIMT is unknown. Most studies include children from 2 to 7 years, although CIMT studies have included infants as young as 7 months (e.g., Lowes et al. 2014) to adolescence (Eliasson et al. 2003; Gordon et al. 2006a, b; Sakzewski et al. 2011a). Given the very early age in which brain damage occurs in children with CP, we could surmise that there is tremendous potential for recovery (Kennard 1936) and that “earlier treatment is better”. However, the relationship is not as clear as one might hope (Eliasson et al. 2005; Hoare et al. 2013; Gordon et al. 2006a, b; Sakzewski et al. 2011a). Nevertheless, the studies to date indicate that children of all ages may benefit.
Animal models suggest that the best time to start treatments eliciting movements of the more affected UE, such as CIMT, may well be during the first few months of life. The as described above (Martin et al. 2011; Eyre 2007). Development of the CST requires activity-dependent competition between the two sides of the developing motor system. Transcranial magnetic stimulation studies in human infants (Eyre 2003, 2007; Eyre et al. 2001; Staudt et al. 2004) are consistent with these findings. Pharmacologically inhibiting activity of the contralesional side, thus balancing activity of the two hemispheres, immediately after unilateral brain injury in the kitten, restores motor function, normal anatomical connectivity of the CST and the motor representational map in primary motor cortex (Martin et al. 2011). A feline model of CIMT (Friel et al. 2012) examined the effects of CIMT at age 8 to 13 weeks and 20-24 weeks (Fig. 3). The earlier training restored motor function, CST connections in the spinal cord and the motor cortical representation of the forelimb, and increased cholinergic spinal interneuron density on the contralateral side. The later training (age 20–24 weeks) did not restore motor function or contralateral spinal cholinergic neuronal density, although it did increase CST connectivity and the motor cortical representation of the forelimb. Restraint alone (forced use without specific, skilled training) only restored CST connectivity (Friel et al. 2012). This alludes to the importance of increasing skilled activity of the involved UE, a principle embedded in both CIMT and bimanual training (see below), to balance the neural activity between the two hemispheres before the less affected CST “outcompetes” the affected CST (i.e., at an early age).

Summary of effects constraint only (forced use), constraint plus motor training in a in a feline model of unilateral spastic cerebral palsy induced by inactivation of the motor cortex. Early training was in a kitten age 8–13 weeks, late training 20–24 weeks. Gray rectangles, conditions in which an effect was noted. Corticospinal tract (CST) plasticity is defined as the presence of axons/varicosities within the spinal intermediate gray matter or more ventrally. An effect of treatment on the M1 motor map is defined as an increase in the number of sites from which stimulation evoked a limb motor response. A filled light gray rectangle in the cholinergic interneuron (INs) column indicates the presence of robust increases in the ratio of spinal cholinergic interneurons on the affected and unaffected sides. The dark rectangle in the motor recovery column indicates am improvement in stepping accuracy while walking over a horizontal ladder. From Friel et al. (2013)
Intensive Bimanual Training
The efficacy CIMT lead to the obvious question of whether similar improvements could be achieved without physically restraining the less affected upper extremity. Bimanual training is developmentally focused and takes into account principles of motor learning (Thorndike 1914) (practice specificity) to train use of the more affected hand as a functional (nondominant) assist rather than as a dominant hand as done in CIMT. It uses the environment (task) to “force use the more affected hand”. One child-friendly form of intensive bimanual training was developed, “Hand-arm bimanual intensive therapy” (HABIT) (Charles and Gordon 2006), with the focus improving the amount and quality of involved UE use during bimanual tasks. HABIT retains the intensive structured practice of CIMT and typically it is provided in a day camp environment 6 h/day for 10–15 days (i.e., 60–90 h). A small randomized control trial of HABIT was initially conducted (Gordon et al. 2007) demonstrating that children who received HABIT had improved quality of affected hand use during bimanual activities and frequency of UE use. HABIT has also been shown to be effective using a themed (learning magic tricks) approach (Green et al. 2013).
Bimanual training and CIMT result in similar improvements in both unimanual capacity and bimanual performance outcomes in CP populations (Sakzewski et al. 2011a, b; Hoare et al. 2013; Gordon et al. 2008, 2011; Facchin et al. 2011; Deppe et al. 2013; Dong et al. 2013) (Fig. 4). Bimanual training has been shown to result in better improvement in functional activities and play goals meaningful to participants and caregivers (Gordon et al. 2011; Brandão et al. 2012) largely since most goals are bimanual (Gordon et al. 2011). During a bimanual task where children are asked to open a drawer with one hand and manipulate its contents with the other hand, improvements in both the CIMT and HABIT groups were observed despite not being practiced during the training (Hung et al. 2011). However greater improvements in movement overlap (the percentage of time with both hands engaged in the task) and goal synchronization (reduced time between each hand completing the task goals) were found for the HABIT group. Together these findings are in agreement with the principle of practice specificity.

a Mean ± SEM time to complete the 6 timed items (writing excluded) of the Jebsen-Taylor Test of Hand Function. Faster times correspond to better performance. b. Mean ± SEM scaled logit scores (AHA units) on the Assisting Hand Assessment; higher scores represent better performance. Abbreviations: CIMT Constraint-induced movement therapy; HABIT Hand-arm intensive bimanual therapy; AHA Assisting hand assessment. From Gordon et al. (2011)
Despite the advantages and disadvantages of each approach, CIMT and HABIT are not mutually exclusive. They can be performed concurrently with sufficient intensity (Aarts et al. 2010; Cohen-Holzer et al. 2011; Taub et al. 2007) or CIMT could be followed with a bimanual training program (i.e., sequentially) where gains in unimanual capacity are translated into bimanual activities (Case-Smith et al. 2012; Taub et al. 2007). These might combine the benefits of both approaches, although comparison studies to either isolated approach have not been conducted (but see Gordon 2011).
Neurophysiological Predictors and Responses to Training
Although the above intensive training protocols have demonstrated great promise, a major limitation is that the neurological damage and subsequent recovery in cerebral palsy is extremely diverse. Studies of these approaches have largely ignored this issue and tend to lump participants together and look at the group effects. There has been large variability in the response to treatment as well (e.g., Sakzewski et al. 2011b). It may be that depending on the specific lesions and brain reorganization, one approach may be more efficacious than another. For example, Staudt and colleagues (Kuhnke et al. 2008) showed that children with a contralateral CST increased manual dexterity after CIMT, whereas children with an ipsilateral CST did not. The two groups also showed differences in neuroplasticity associated with the training (Juenger et al. 2013). In contrast, Islam et al. (2014) concluded that improvements in hand use after CIMT were present in all participants, irrespective of their CST connectivity pattern. Only one case study of two children with USCP has examined the effect of CST connectivity pattern on efficacy of bimanual therapy, with improvements seen regardless of CST organization (Bleyenheuft et al. 2015) (Fig. 5).

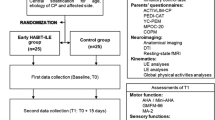
Determinist diffusion tensor imaging tracking was made from the 3 mm spheres (123 voxels) created symmetrically in both CST tracts, with their middle centered on the CST fibers as visualized in a transversal plane passing through the middle cerebellar peduncle. a child 1 with ipsilateral connectivity, b child 2 with contralateral connectivity. Pretest and posttest data for each child for the c Jebsen-Taylor test of hand function (JTTHF), d ABILHAND-Kids and e Canadian occupational performance measure (COPM) performance rating. Modified from Bleyenheuft et al. (2015)
A recent study of the neural predictors of bimanual training showed that children with greater overall severity of brain injury at baseline (higher radiological score) and decreased cortical activation of the lesional hemisphere on fMRI, showed greater improvement on bilateral hand function but less improvement on unimanual function (Schertz et al. 2016). Similarly, greater white matter damage (DTI of the posterior limb of the internal capsule and the CST were also associated with greater improvement on bimanual function but no improvement on unimanual assessment. However, the amount of damage to the CSTs alone did not relate improvement after CIMT (Rickards et al. 2014) or bimanual training (Friel et al. 2014).
One study showed increases in activation and size of the motor areas controlling the affected hand using TMS, DTI and fMRI (Bleyenheuft et al. 2015). The later study found increased activation in cortical areas involved in reward circuits, suggesting an intriguing possibility that the training may engage circuits involved with achieving self-efficacy. Another study showed that changes in DTI and fMRI parameters were seen when comparing pre- and post intervention following bimanual training. Despite variable patterns of brain plasticity, a change toward a more unilateral brain activation pattern was consistently associated with greater motor improvements. Another (TMS) study showed that the map size and amplitude of motor evoked potential (MEP) amplitudes of the affected hand motor map increased significantly after bimanual training regardless of whether the representation was in the lesional or contralesional hemisphere (Friel et al. 2016) (Fig. 6). The amount of change in these measures correlated with improvements in hand function. Finally, one study examined differences in cortical reorganization following CIMT depending on CST organization (Juenger et al. 2013). Both groups exhibited increases in sensorimotor cortical activation, which is consistent with a report of better sensory function after intensive training (Kuo et al. 2016). Interestingly TMS showed a decrease in M1 excitability in children with an ipsilateral CST pattern, whereas it showed an increase in M1 excitability in children with preserved contralateral CST organization.

Changes in magnitude of motor evoked potentials in TMS maps after structured training in child A and unstructured practice in child B. Maps are of the affected hand located contralateral to the affected hemisphere. Red color indicates stronger MEP response. Not that the maps indicate a larger hand representation with stronger MEPS after structured practice only. Plotted from data in Friel et al. 2016
Recently the question of training ingredients, specifically progressive skill training, was addressed. Skill progression has been shown to be important for inducing plasticity in animal models of learning (Kleim et al. 2002; Nudo 2003). Furthermore, in a feline model of unilateral CP, restriction of the nonparetic forelimb alone (analogous to forced use) did not drive CST development, cortical reorganization or improvements in stepping accuracy, whereas the addition to active training (analogous to CIMT) did. Children with USCP were either provided intensive bimanual training (HABIT) that included progressive increases in the difficulty of activities as hand function improved, or practice of the same activities without skill progression (bimanual play). At first glance, it appeared that both approaches lead to equal improvements in hand function as assessed with standard clinical assessments (Brandao et al. 2014). However, upon examination of progress on functional and play goals identified by caregivers, children in the skilled practice group had greater improvements (Brandao et al. 2014) and improved their movement coordination patterns as seen using kinematic analysis on the functional drawer opening task described above. Furthermore, we used TMS to probe the hand representation plasticity (Friel et al. 2016). It was shown that children in the skill progression group that the size and motor evoked potential (MEP) amplitudes of the affected hand motor map increased significantly after therapy, whereas training of the same activities without skill progression did not (Fig. 6). Thus, skill progression appears to be an important ingredient for changing motor patterns and inducing plasticity in M1.
Together these studies highlight the variations in CNS damage underlying CP. It is essential to understand the underlying behavioral and neural mechanisms as to better target them with interventions. However, the variability complicates story and may limit the extent to which new treatments may be generalized across individuals. In fact, they highlight the notion that there cannot be a “one-size-fits-all approach” to rehabilitation.
Brain Stimulation
As we begin to understand the activity-dependent reorganization of the brain following intensive training, the exciting prospect of stimulating the brain directly using rTMS or transcranial direct current stimulation (tDCS). Stimulating the CST after M1 inactivation in a feline model of hemiparesis has been shown stimulate its normal development and improve motor function (Salimi et al. 2008). Stimulating the brain using tDCS has been shown to enhance motor learning (Reis et al. 2009). In hemiplegia due to adult stroke, short bouts of inhibitory, contralesional rTMS improves hand function (Hsu et al. 2012; Lefaucheur et al. 2014). A preliminary trial of contralesional inhibitory rTMS found the procedure to be safe and feasible for patients with hemiplegia due to arterial ischaemic stroke (Kirton et al. 2008). A recent trial of contralesional rTMS in participants with unilateral CP suggested favorable tolerability and functional improvements as well (Gillick et al. 2014). In a RCT of 45 participants with USCP due to perinatal stroke examined inhibitory contralesional rTMS on hand function (Kirton et al. 2016). They found that participating in intensive rehabilitation programs alone can result in sustained functional gains. However the addition of CIMT and rTMS increases the chances of significant improvement. An important caveat is that this study did not examine CST organization in relation to the outcomes (see Staudt and Gordon 2016).
It should be noted that since almost all studies of intensive training or brain stimulation have been conducted in children in children age 2 and above. This is thought to be beyond the age in which normal contralateral CST organization is established (i.e., within the first 6 months, Eyre et al. 2007). In fact while most studies have demonstrated improvements in hand function, none have reported “curing” the impaired hand. An important remaining question is whether early treatment during this “critical period” can alter the development of CST connectivity, and possibly thwart the emergence of CP. In this regards, given the limited attention spans and movement repertoires of infants, brain stimulation may eventually hold considerable promise to this effect. Furthermore, given the potential impact of tDCS on motor learning, a key question is whether the addition of this technique in conjunction with intensive training can decrease the required dose, and thus cost, associated with these programs.
Take Home Message
The pathophysiology and mechanisms underlying impaired upper extremity control of USCP will be reviewed. It was shown that the integrity of the CST tract closely relates to the extent of upper extremity impairments. It was also shown that the developing CST tract can reorganize its connectivity depending on the timing and locating of CNS injury. The reorganization is also predictive of the resulting severity of impairments. Mechanisms underlying impaired motor function were highlighted, including movement execution, movement planning, sensorimotor integration, bimanual movement control and mirror movements. Evidence for motor-learning based therapies was presented, including Constraint-Induced Movement Therapy and Bimanual Training, and possible pathophysiological predictors of treatment outcome were presented. Finally future possibilities of stimulating the development of the nervous system were presented.
References
Aarts PB, Jongerius PH, Geerdink YA et al (2010) Effectiveness of modified constraint-induced movement therapy in children with unilateral spastic cerebral palsy: a randomized controlled trial. Neurorehabil Neural Repair 24:509–518
Adler C, Berweck S, Lidzba K, Becher T, Staudt M (2015) Mirror movements in unilateral spastic cerebral palsy: Specific negative impact on bimanual activities of daily living. Eur J Paediatr Neurol 19:504–509
Bax M, Goldstein M, Rosenbaum P, Leviton A, Paneth N, Dan B, Jacobsson B, Damiano D (2005) Proposed definition and classification of cerebral palsy. Dev Med Child Neurol 47:571–576
Bleyenheuft Y, Grandin CB, Cosnard G, Olivier E, Thonnard JL (2007) Corticospinal dysgenesis and upper-limb deficits in congenital hemiplegia: a diffusion tensor imaging study. Pediatrics 120:e1502–e1511
Bleyenheuft Y, Thonnard JL (2010) Predictive and reactive control of precision grip in children with congenital hemiplegia. Neurorehabil Neural Repair 24:318–327
Bleyenheuft Y, Thonnard JL (2011) Tactile spatial resolution in unilateral brain lesions and its correlation with digital dexterity. J Rehabil Med 43:251–256
Bleyenheuft Y, Dricot L, Gilis N, Kuo HC, Grandin C, Bleyenheuft C, Gordon AM, Friel KM (2015) Capturing neuroplastic changes after bimanual intensive rehabilitation in children with unilateral spastic cerebral palsy: a combined DTI, TMS and fMRI pilot study. Res Dev Dis 43–44:136–149
Brandão M, Gordon AM, Mancini MC (2012) Functional impact of constraint therapy and bimanual training in children with cerebral palsy: a randomized controlled trial. Am J Occup Ther 66:672–681
Brandao M, Ferre CL, Kuo H-C, Rameckers E, Bleyenheuft Y, Hung Y-C, Friel K, Gordon AM (2014) Comparison of structured skill and unstructured practice during intensive bimanual training in children with unilateral spastic cerebral palsy. Neural Rehab Neur Repair 28:452–461
Brown JK, van Rensburg E, Walsh G, Lakie M, Wright GW (1987) A neurological study of hand function of hemiplegic children. Dev Med Child Neurol 29:287–304
Carr LJ, Harrison LM, Evans AL, Stephens JA (1993) Patterns of central motor reorganization in hemiplegic cerebral palsy. Brain 116:1223–1247
Carr J, Shepherd RB (1989) A motor learning model for stroke rehabilitation. Physiotherapy 75:372–380
Case-Smith J, DeLuca SC, Stevenson R, Ramey SL (2012) Multicenter randomized controlled trial of pediatric constraint-induced movement therapy: 6-month follow-up. Am J Occup Ther 66:15–23
Charles J, Lavinder G, Gordon AM (2001) The effects of constraint induced therapy on hand function in children with hemiplegic cerebral palsy. Ped Phys Ther 13:68–76
Charles J, Gordon AM (2006) Development of hand-arm bimanual intensive therapy (HABIT) for improving bimanual coordination in children with hemiplegic cerebral palsy. Dev Med Child Neurol 48:931–936
Cioni G, Sales B, Paolicelli PB, Petacchi E, Scusa MF, Canapicchi R (1999) MRI and clinical characteristics of children with hemiplegic cerebral palsy. Neuroped 30:249–255
Cohen-Holzer M, Katz-Leurer M, Reinstein R et al (2011) The effect of combining daily restraint with bimanual intensive therapy in children with hemiparetic cerebral palsy: a self-control study. NeuroRehab 29:29–36
Deppe W, Thuemmler K, Fleischer J, Berger C, Meyer S, Wiedemann B (2013) Modified constraint-induced movement therapy versus intensive bimanual training for children with hemiplegia—a randomized controlled trial. Clin Rehabil 10:909–920
Dong VA-Q, Tung IH-H, Siu HW-Y et al (2013) Studies comparing the efficacy of constraint-induced movement therapy and bimanual training in children with unilateral cerebral palsy: a systematic review. Dev Neurorehabil 16:133–143
Eliasson AC, Bonnier B, Krumlinde-Sundholm L (2003) Clinical experience of constraint induced movement therapy in adolescents with hemiplegic cerebral palsy—a day camp model. Dev Med Child Neurol 45:357–359
Eliasson AC, Forssberg H, Hung YC, Gordon AM (2006) Development of hand function and precision grip control in individuals with cerebral palsy: a 13-year follow up study. Pediatrics 118:e1226–e1236
Eliasson AC, Gordon AM, Forssberg H (1991) Basic coordination of manipulative forces of children with cerebral palsy. Dev Med Child Neurol 33:659–668
Eliasson AC, Gordon AM, Forssberg H (1992) Impaired anticipatory control of isometric forces during grasping by children with cerebral palsy. Dev Med Child Neurol 34:216–225
Eliasson AC, Gordon AM (2000) Impaired force coordination during object release in children with hemiplegic cerebral palsy. Dev Med Child Neurol 42:228–234
Eliasson A-C, Krumlinde-sundholm L, Shaw K et al (2005) Effects of constraint-induced movement therapy in young children with hemiplegic cerebral palsy: an adapted model. Dev Med Child Neurol 47:266–275
Eliasson AC, Krumlinde-Sundholm L, Gordon AM, Feys H, Klingels K, Aarts P, Rameckers E, Autti-Rämö I, Hoare B (2014) Guidelines for future research in Constraint-induced movement therapy for children with unilateral cerebral palsy: an expert consensus. Dev Med Child Neurol 56:125–137
Eyre JA (2003) Development and plasticity of the corticospinal system in man. J Neural Transplant Plast 10:93–106
Eyre JA (2007) Corticospinal tract development and its plasticity after perinatal injury. Neurosci Biobehav Rev 31:1136–1149
Eyre JA, Smith M, Dabydeen L et al (2007) Is hemiplegic cerebral palsy equivalent to amblyopia of the corticospinal system? Ann Neurol 62:493–503
Eyre JA, Taylor JP, Villagra F et al (2001) Evidence of activity-dependent withdrawal of corticospinal projections during human development. Neurol 57:1543–1554
Facchin P, Rosa-Rizzotto M, Dalla Pozza LV et al (2011) Multisite trial comparing the efficacy of constraint-induced movement therapy with that of bimanual intensive training in children with hemiplegic cerebral palsy: Postintervention results. Am J Phys Med Rehabil 90:539–553
Farmer SF, Harrison LM, Ingram DA, Stephens JA (1991) Plasticity of central motor pathways in children with hemiplegic cerebral palsy. Neurology 41:1505–1510
Friel K, Chakrabarty S, Kuo H-C et al (2012) Using motor behavior during an early critical period to restore skilled limb movement after damage to the corticospinal system during development. J Neurosci 32:9265–9276
Friel KM, Chakrabarty S, Martin JH (2013) Pathophysiological mechanisms of impaired limb use and motor systems repair strategies after unilateral injury of the developing brain. Dev Med Child Neurol Suppl 4:27–31
Friel KM, Kuo HC, Carmel JB, Gordon AM (2014) Improvements in hand function after intensive bimanual training are not associated with corticospinal tract dysgenesis in children with hemiplegic cerebral palsy. Exp Brain Res 232:2001–2009
Friel K, Kuo H-C M, Ferre CL, Brandao M, Carmel J, Bleyenheuft Y, Gowatsky JL, Stanford AD, Rowny SB, Luber B, Bassi B, Murphy DLK, Lisanby SH, Gordon AM (2016) Skilled bimanual training drives motor cortex plasticity in children with unilateral cerebral palsy. Neural Rehab Neural Repair 30(9):834–844
Gentile AM (2000) Skill acquisition: action, movement, and neuromotor processes. In: Carr JH, Shepherd RD (eds) Movement science: foundations for physical therapy, 2nd edn. Aspen, Rockville, MD, pp 111–187
Gillick BT, Krach LE, Feyma T et al (2014) Primed low-frequency repetitive transcranial magnetic stimulation and constraint-induced movement therapy in pediatric hemiparesis: a randomized controlled trial. Dev Med Child Neurol 56:44–52
Gordon AM (2001) In: Kalverboer AF, Gramsbergen A (eds) Handbook of brain and behaviour in human development. Kluwer, Dordrecht, pp 513–537
Gordon AM (2011) To constrain or not to constrain, and other stories of intensive upper extremity training for children with unilateral cerebral palsy. Dev Med Child Neurol 53(Suppl. 4):56–61
Gordon AM (2014) In: Shepherd R (Ed) Cerebral Palsy in infancy. targeted activity to optimize early growth and development. Elsevier, pp 305–322
Gordon AM, Charles J, Schneider JA, Chinnan A (2007) Efficacy of a hand-arm bimanual intensive therapy (HABIT) for children with hemiplegic cerebral palsy: a randomized control trial. Dev Med Child Neurol 49:830–838
Gordon AM, Charles J, Duff SV (1999) Fingertip forces during object manipulation in children with hemiplegic cerebral palsy. II: Bilateral coordination. Dev Med Child Neurol Neurol 41:176–185
Gordon AM, Charles J, Steenbergen B (2006a) Movement planning is disrupted by impaired sensorimotor integration in children with hemiplegic cerebral palsy. Ped Res 60:587–591
Gordon AM, Charles J, Wolf SL (2006b) Efficacy of constraint-induced movement therapy on involved-upper extremity use in children with hemiplegic cerebral palsy is not age-dependent. Pediatrics 117:e363–e373
Gordon AM, Chinnan A, Gill S, Petr E, Hung YC, Charles J (2008) Both constraint-induced movement therapy and bimanual training lead to improved performance of upper extremity function in children with hemiplegia. Dev Med Child Neurol 50:957–958
Gordon AM, Duff SV (1999a) Fingertip forces during object manipulation in children with hemiplegic cerebral palsy. I: Anticipatory scaling. Dev Med Child Neurol 41:166–175
Gordon AM, Duff SV (1999b) Relation between clinical measures and fine manipulative control in children with hemiplegic cerebral palsy. Dev Med Child Neurol 41:586–591
Gordon AM, Hung YC, Brandao M et al (2011) Bimanual training and constraint-induced movement therapy in children with hemiplegic cerebral palsy: a randomized trial. Neuro Rehab Neural Repair 25:692–702
Gordon AM, Lewis S, Eliasson AC, Duff SV (2003) Object release under varying task constraints in children with hemiplegic cerebral palsy. Dev Med Child Neurol 45:240–248
Gordon AM, Magill, RA (2012) Motor learning: Application of principles to pediatric rehabilitation. In: Campbell SK, Palisano RJ, Orlin MN (eds) Physical therapy for children. Elsevier (Saunders), St. Louis, pp 151–174
Gordon AM, Steenbergen B (2008) In: Eliasson AC and Burtner P (eds) Improving hand function in children with cerebral palsy: theory, evidence and intervention. Clinics in developmental medicine. Mac Keith Press, London, pp 160–75. https://www.ncbi.nlm.nih.gov/pubmed/24237277
Green D, Schertz M, Gordon AM, Moore A, Schejter M, Farquharson Y, Ben Bashat D, Winstein M, Lin J-P, Fattal-Valevski A (2013) A multi-site study of functional outcomes following a themed approach to hand-arm bimanual intensive therapy (HABIT) for children with hemiplegia. Dev Med Child Neurol 55:527–533
Harrison A (1988) Spastic cerebral palsy: possible spinal interneuronal contributions. Dev Med Child Neurol 30:769–780
Himmelmann K, Hagberg G, Beckung E, Hagberg B, Uvebrant P (2005) The changing panorama of cerebral palsy in Sweden. IX. Prevalence and origin in the birth-year period 1995–1998. Acta Paediatr 94:287–294
Hoare B, Imms C, Villanueva E et al (2013) Intensive therapy following upper limb botulinum toxin A injection in young children with unilateral cerebral palsy: a randomized trial. Dev Med Child Neurol 55:238–247
Holmström L, Vollmer B, Tedroff K et al (2010) Hand function in relation to brain lesions and corticomotor-projection pattern in children with unilateral cerebral palsy. Dev Med Child Neurol 52:145–152
Hsu WY, Cheng CH, Liao KK, Lee IH, Lin YY (2012) Effects of repetitive transcranial magnetic stimulation on motor functions in patients with stroke: a meta-analysis. Stroke 43:1849–1857
Hung Y-C, Casertano L, Hillman A, Gordon AM (2011) The effect of training specificity on bimanual coordination in children with hemiplegia. Res Dev Dis 32:2724–2731
Hung Y-C, Charles J, Gordon AM (2004) Bimanual coordination of arm movements in children with hemiplegia. Dev Med Child Neurol 46:746–753
Hung YC, Charles J, Gordon AM (2010) Influence of accuracy constraints on bimanual coordination during a goal-directed task in children with hemiplegic cerebral palsy. Exp Brain Res 201:421–428
Islam M, Gordon AM, Forssberg H, Sköld A, Eliasson AC (2011) Grip force coordination during a bimanual task in unilateral cerebral palsy. Dev Med Child Neurol 53:920–926
Islam M, Nordstrand L, Holmström L, Kits A, Forssberg H, Eliasson AC (2014) Is outcome of constraint-induced movement therapy in unilateral cerebral palsy dependent on corticomotor projection pattern and brain lesion characteristics? Dev Med Child Neurol 56:252–258
Johansson RS, Westling G (1984) Roles of glabrous skin receptors and sensorimotor memory in automatic control of precision grip when lifting rougher or more slippery objects. Exp Brain Res 56:550–564
Juenger H, Kuhnke N, Braun C, Ummenhofer F, Wilke M, Walther M, Koerte I, Delvendahl I, Berweck S, Mall V, Staudt M (2013) Two types of exercise-induced neuroplasticity in congenital hemiparesis: a TMS, fMRI and MEG study. Dev Med Child Neurol 55:941–951
Kennard MA (1936) Age and other factors in motor recovery from precentral lesions in monkeys. Am J Physiol 115:138–146
Kirton A, Chen R, Friefeld S, Gunraj C, Pontigon AM, deVeber G (2008) Contralesional repetitive transcranial magnetic stimulation for chronic hemiparesis in subcortical paediatric stroke: a randomised trial. Lancet Neurol 7:507–513
Kirton A, Andersen J, Herrero M, Nettel-Aguirre A, Carsolio L, Damji O, Keess J, Mineyko A, Hodge J, Hill MD (2016) Brain stimulation and constraint for perinatal stroke hemiparesis: The PLASTIC CHAMPS trial. Neurology 3(86):1659–1667
Kleim JA, Barbay S, Nudo RJ (1998) Functional reorganization of the rat motor cortex following motor skill learning. J Neurophysiol 80:3321–3325
Kleim JA, Barbay S, Cooper NR, Hogg TM, Reidel CN, Remple MS, Nudo RJ (2002) Motor learning-dependent synaptogenesis is localized to functionally reorganized motor cortex. Neurobiol Learn Mem 77:63–77
Klingels K, Jaspers E, Staudt M, Guzzetta A, Mailleux L, Ortibus E, Feys H (2016) Do mirror movements relate to hand function and timing of the brain lesion in children with unilateral cerebral palsy? Dev Med Child Neurol 58:735–742
Koert I, Pelavin P, Kirmess B, Fuchs T, Berweck S, Laubender RP, Heinen F (2011) Anisotropy of transcallosal motor fibres indicates functional impairment in children with periventricular leukomalacia. Dev Med Child Neurol 53:179–186
Kuhnke N, Juenger H, Walther M, Berweck S, Mall V, Staudt M (2008) Do patients with congenital hemiparesis and ipsilateral corticospinal projections respond differently to constraint-induced movement therapy? Dev Med Child Neurol 50:898–903
Kuo H-C, Gordon AM, Henrionnet A, Hautfenne S, Friel K, Bleyenheuft Y (2016) The effects of intensive bimanual training with and without tactile training on tactile function in children with unilateral spastic cerebral palsy. Res Dev Disabil 49–50:129–139
Kuo H-C, Ferre CL, Carmel JB, Gowatsky JL, Stanford AD, Rowny SB, Lisanby SH, Gordon AM, Friel KM (2016) Using diffusion tensor imaging to identify corticospinal tract projection patterns in children with unilateral spastic cerebral palsy. Dev Med Child Neurol. doi: 10.1111/dmcn.13192
Kuhtz-Buschbeck JP, Sundholm LK, Eliasson AC, Forssberg H (2000) Quantitative assessment of mirror movements in children and adolescents with hemiplegic cerebral palsy. Dev Med Child Neurol 42:728–736
Latash ML, Anson JG (1996) What are “normal movements” in atypical populations? Behav Brain Sci 19:55–106
Lawrence DG, Kuypers HGJM (1968) The functional organization of the motor system in the monkey. I. The effects of bilateral pyramidal lesions. Brain 91:1–14
Lefaucheur J-P, André-Obadia N, Antal A et al (2014) Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS). Clin Neurophysiol 125:2150–2206
Lowes LP, Mayhan M, Orr T, Batterson N, Tonneman JA, Meyer A, Alfano L, Wang W, Whalen CN, Nelin MA, Lo WD, Case-Smith J (2014) Pilot study of the efficacy of constraint-induced movement therapy for infants and toddlers with cerebral palsy. Phys Occup Ther Pediatr 34:4–21
Martin JH, Chakrabarty SS, Friel KM (2011) Harnessing activity-dependent plasticity to repair the damaged corticospinal tract in an animal model of cerebral palsy. Dev Med Child Neurol 53:9–13
Moberg E (1962) Criticism and study of methods for examining sensibility in the hand. Neurol 12:8–19
Novak I, McIntyre S, Morgan C, Campbell L, Dark L, Morton N, Stumbles E, Wilson SA, Goldsmith S (2013) A systematic review of interventions for children with cerebral palsy: state of the evidence. Dev Med Child Neurol 55:885–910
Nudo RJ (2003) Functional and structural plasticity in motor cortex: implications for stroke recovery. Phys Med Rehabil Clin N Am 14(Suppl):S57–S76
Plautz EJ, Milliken GW, Nudo RJ (2000) Effects of repetitive motor training on movement representations in adult squirrel monkeys: role of use versus learning. Neurobiol Learn Mem 74:27–55
Prabhu S, Diermayr G, Gysin P, Gordon AM (2011) Impaired anticipatory control of grasp during gait in children with hemiplegic cerebral palsy. Dev Med Child Neurol 53:865–869
Reis J, Schambra HM, Cohen LG, Buch ER, Fritsch B, Zarahn E, Celnik PA, Krakauer JW (2009) Noninvasive cortical stimulation enhances motor skill acquisition over multiple days through an effect on consolidation. Proc Natl Acad Sci USA 106:1590–1595
Rickards T, Sterling C, Taub E, Perkins-Hu C, Gauthier L, Graham M, Griffin A, Davis D, Mark VW, Uswatte G (2014) Diffusion tensor imaging study of the response to constraint-induced movement therapy of children with hemiparetic cerebral palsy and adults with chronic stroke. Arch Phys Med Rehabil 95:506–514
Sakzewski L, Ziviani J, Abbott DF et al (2011a) Randomized trial of constraint-induced movement therapy and bimanual training on activity outcomes for children with congenital hemiplegia. Dev Med Child Neurol 53:313–320
Sakzewski L, Ziviani J, Boyd RN (2011b) Best responders after intensive upper-limb training for children with unilateral cerebral palsy. Arch Phys Med Rehabil 92:578–584
Salimi I, Friel KM, Martin JH (2008) Pyramidal tract stimulation restores normal corticospinal tract connections and visuomotor skill after early postnatal motor cortex activity blockade. J Neurosci 28:7426–7434
Scheck SM, Boyd RN, Rose SE (2012) New insights into the pathology of white matter tracts in cerebral palsy from diffusion magnetic resonance imaging: a systematic review. Dev Med Child Neurol 54:684–696
Schertz M, Shiran S, Myers V, Weinstein M, Fattal-Valevski A, Artzi M, Ben Bashat D, Gordon AM, Green D (2016) Advanced imaging predictors of improvement from a motor learning based intervention for children with hemiplegia. Neural Rehab Neural Repair 30:647–660
Staudt M (2010) Brain plasticity following early life brain injury: insights from neuroimaging. Semin Perinatol 34:87–92
Staudt M, Gerloff C, Grodd W et al (2004) Reorganization in congenital hemiparesis acquired at different gestational ages. Ann Neurol 56:854–863
Staudt M, Gordon AM (2016) Combining rTMS and CIMT: A “one-size-fits-all” therapy for congenital hemiparesis? Neurology 3(86):1652–1654
Steenbergen B, Charles J, Gordon AM (2008) Fingertip force control during bimanual object lifting in hemiplegic cerebral palsy. Exp Brain Res 186:191–201
Steenbergen B, Hulstijn W, De Vries A, Berger M (1996) Bimanual movement coordination in spastic hemiparesis. Exp Brain Res 110:91–98
Steenbergen B, Jongbloed-Pereboom M, Spruijt S, Gordon AM (2013) Impaired motor planning and motor imagery in children with unilateral spastic cerebral palsy: challenges for the future of pediatric rehabilitation. Dev Med Child Neurol Suppl 4:43–46
Sukal-Moulton T, Murray TM, Dewald JP (2013) Loss of independent limb control in childhood hemiparesis is related to time of brain injury onset. Exp Brain Res 225(3):455–463
Steenbergen B, Van Thiel E, Hulstijn W, Meulenbroek RGJ (2000) The coordination of reaching and grasping in spastic hemiparesis. Hum Mov Sci 19:75–105
Taub E, Shee LP (1980) Somatosensory deafferentation research with monkeys: implications for rehabilitation medicine. In: Ince LP (ed) Behavioral psychology in rehabilitation medicine: clinical applications. Williams and Wilkins, Baltimore and London, pp 371–401
Taub E, Wolf SL (1997) Constraint induced movement techniques to facilitate upper extremity use in stroke patients. Top Stroke Rehabil 3:38–61
Taub E, Griffin A, Nick J et al (2007) Pediatric CI therapy for stroke-induced hemiparesis in young children. Dev Neurorehabil 10:3–18
Thorndike EL (1914) Educational psychology: briefer course. Columbia University Press, New York
Tower S (1940) Pyramidal lesion in the monkey. Brain 63:36–90
Trombly C (1995) Clinical practice guidelines for post-stroke rehabilitation and occupational therapy practice. Am J Occup Ther 49:711–714
Uvebrandt P (1988) Hemiplegic cerebral palsy. Aetiology and outcome. Acta Paediatr Scand Suppl 345:1–100
Weinstein M, Green D, Geva R, Schertz M, Fattal-Valevski A, Artzi M, Myers V, Shiran S, Gordon AM, Gross-Tsur V, Ben Bashat D (2013) Interhemispheric and intrahemispheric connectivity and manual skills in children with unilateral cerebral palsy. Brain Struct Funct 219:1025–1040
Weinstein M, Myers V, Green D, Schertz M, Shiran A, Geva R, Artzi M, Gordon AM, Fattal-Valevski A, Ben Bashat D (2015) Brain plasticity following intensive bimanual therapy in children with hemiplegia: preliminary evidence. Neural Plast :798481. doi: 10.1155/2015/798481
Winstein CJ, Wolf SL (2009) Task-oriented training to promote upper extremity recovery. In: Stein J, Harvey R, Macko R, Winstein CJ, Zorowitz R (eds) Stroke recovery and rehabilitation. Demos Medical Publishing, New York, NY
Wolf SL, Lecraw DE, Barton LA et al (1989) Forced use of hemiplegic upper extremities to reverse the effect of learned nonuse among chronic stroke and head-injured patients. Exp Neurol 104:125–132
Woods BT, Teuber HL (1978) Mirror movements after childhood hemiparesis. Neurol 28:1152–1157
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing AG
About this chapter
Cite this chapter
Gordon, A.M. (2016). Impaired Voluntary Movement Control and Its Rehabilitation in Cerebral Palsy. In: Laczko, J., Latash, M. (eds) Progress in Motor Control. Advances in Experimental Medicine and Biology, vol 957. Springer, Cham. https://doi.org/10.1007/978-3-319-47313-0_16
Download citation
DOI: https://doi.org/10.1007/978-3-319-47313-0_16
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-47312-3
Online ISBN: 978-3-319-47313-0
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)