
Abstract
The prevention and management of antiviral drug resistance remain central aspects of treatment strategies against infection with the hepatitis B virus (HBV). Whilst current therapeutic options for the de novo treatment of chronic hepatitis B (CHB) carry a low risk of selecting for drug resistance, indefinite treatment is commonly required. Importantly, many patients have accumulated HBV drug resistance and cross-resistance through previous, less efficacious therapy and have limited treatment options. Large numbers also continue to be at risk of drug resistance due to limited access to effective antiviral compounds in middle- and low-income settings.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Keywords
- Hepatitis B
- Hepatitis B virus (HBV)
- Quasispecies
- Lamivudine monotherapy (LAM)
- Probe assay
- Reverse hybridization
- Genome sequencing
- Next Generation Sequencing (NGS)
- Chronic hepatitis B (CHB)
1 Introduction
There have been major advances in the prevention and management of antiviral drug resistance in the treatment strategies against HBV infection in the past two decades [1]. Currently, interferon alfa-2b and pegylated interferon-a (pegIFN-α), and several oral inhibitors of the HBV polymerase enzyme are approved for the treatment of CHB [1–5]. Polymerase inhibitors, comprising both nucleoside and nucleotide analogues (NAs), are generally more effective than IFN-based treatment and cause fewer side effects. Whilst current therapeutic options for the de novo treatment of chronic hepatitis B (CHB) carry a low risk of selecting for drug resistance, long-term and indefinite treatment is commonly required to sustain viral suppression. The demand for better treatments heightens with the fact that many patients have accumulated HBV drug resistance and cross-resistance through previous, less efficacious therapy, and have limited treatment options. Even more so, large numbers also continue to be at risk of drug resistance due to limited access to effective antiviral compounds in middle and low-income settings. Several novel compounds are under development that may pave the way for therapeutic regimens of finite duration and, potentially, for HBV eradication [5–7].
The overall short-term and long-term efficacy of NA-based therapy for CHB is influenced by several factors, including drug potency and treatment adherence as key determinants (Table 74.1). Even in optimally adherent patients, some NAs, when used as single agents, can be insufficiently able to suppress virus replication, particularly in the context of a high HBV DNA load. Due to the plasticity of the HBV genome, ongoing virus replication in the presence of drug pressure can lead to the emergence of HBV variants carrying mutations that reduce drug susceptibility. Although some HBV drug-resistant mutants may show a significant loss of fitness and replicative capacity, others replicate efficiently, can cause progression of liver disease, and can be transmitted.
2 Mechanisms of HBV Drug Resistance
2.1 Emergence of Drug Resistance
HBV is a DNA virus that replicates via an RNA intermediate. The viral polymerase enzyme, which also has reverse transcriptase (RT) activity, displays a high error rate and lacks the proofreading function required to repair incorrectly incorporated bases [8, 9]. HBV has a high replication rate, resulting in the production of ~1012 virions per day. This combines with a mutational rate of ~10−5 substitutions per base and replication cycle [10, 11]. In individuals with ongoing viral replication, approximately 1010–11 point mutations are estimated to occur per day across the entire viral genome. Some mutations cause a severe loss of function, impairing viral fitness to the extent that the mutant stops replicating. Other mutants display variable degree of fitness impairment. Thus, in an infected host, HBV exists as variety of diverse strains that constitute the viral quasispecies. At any given time, and subjected to the influence of modulating factors including immune-mediated and drug-mediated selective pressure, certain mutant species are dominant, whereas others exist only as rarer, low-frequency variants.
HBV mutations that confer reduced drug susceptibility arise spontaneously in the targets of antiviral therapy and circulate within the viral quasispecies prior to the introduction of therapy. Given the overall functional cost, in the absence of drug pressure, HBV drug-resistant variants circulate at low frequency, typically as single mutants, and escape detection by both routine and sensitive methods. Under drug-selective pressure, if virus replication continues, the variants acquire a selective advantage and gradually emerge as dominant species. With continued virus replication under drug pressure, the single mutants evolve genetically, acquiring additional primary and secondary mutations, including compensatory changes that restore viral fitness and increase pathogenicity [12–14].
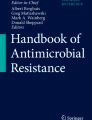
The partially double-stranded circular HBV genome is organized into four overlapping reading frames (ORFs) (Fig. 74.1). Overlapping of the polymerase ORF with the surface ORF has two important consequences. Firstly, there is a reciprocal impact of genetic changes driven by selective pressure, including changes in HBsAg antigenic determinates which create potential for vaccine and diagnostic escape [15, 16]. Secondly, genetic evolution under drug pressure is constrained by the simultaneous impact on polymerase and surface functionality. These constrains are illustrated by comparing the emergence of resistance to lamivudine (LAM) monotherapy in HBV and HIV infection. In HIV-positive subjects, resistant strains emerge as dominant within a few weeks of LAM monotherapy. In contrast, months are required for the emergence of LAM-resistant strains in HBV-positive subjects. Nonetheless, sensitive methodologies have revealed that HBV resistance to LAM can emerge more rapidly than previously appreciated. In a study of patients with HIV and HBV co-infection starting LAM-containing antiretroviral therapy (ART) without additional HBV-active agents, most patients with detectable serum HBV DNA after 6 months had evidence of LAM resistance when evaluated by deep sequencing (Fig. 74.2) [12].

The HBV genome. The relaxed partially double-stranded circular DNA has a size of ~3.2-kilobases and comprises four overlapping reading frames: polymerase (blue), surface (preS1, preS2, and S domains; orange, yellow, and red, respectively), X (purple), and pre-core/core (green). Complete genome numbering starts from TTC and ends at GAA

Emergence of HBV drug resistance during lamivudine monotherapy. A total of 133 HIV and HBV co-infected subjects starting lamivudine-containing antiretroviral therapy without additional HBV-active agents underwent testing for the presence of lamivudine resistance-associated mutations (RAMs) in HBV polymerase. Testing was performed at baseline and after 6 and 12 months of therapy using Sanger sequencing and deep sequencing. Resistance rates are presented as total and by baseline HBeAg status (Adapted from [12])
2.2 Persistence of Drug Resistance
HBV RAMs that emerge as dominant during antiviral therapy lose their replicative advantage once therapy is discontinued, and are outgrown by fitter, drug-sensitive (“wild-type”) strains. In patients who have discontinued therapy for more than a few weeks, it is usually no longer possible to detect the resistant mutants using routine technology. The disappearance of resistance is only apparent however; treatment-enriched mutants persist as low-frequency circulating variants and rapidly re-emerge if suboptimal treatment is restarted. In addition, HBV establishes an archive of genetic variants within the covalently closed circular DNA (cccDNA) that persists in infected hepatocytes [17]. HBV cccDNA is generated from the relaxed circular DNA genome of incoming virions and persists long-term in episomal form in the nucleus of hepatocytes [18]. Whilst effective in suppressing HBV replication, NAs have limited efficacy in reducing the cccDNA reservoir [19–21]. Current research aims at targeting the reservoir and potentially cure HBV infection [5, 18]. Meanwhile, HBV cccDNA retains a long-term memory of any selected resistant strain, from which new replicating strains can re-emerge [1, 5, 18, 20, 22].
2.3 Nomenclature
A nomenclature for describing HBV drug resistance-associated mutations (RAMs) was established in 2001 [23]. The HBV polymerase gene is divided into four functional units (Fig. 74.3). Resistance is defined by the presence of one or more nucleotide substitutions in the RT domain of the polymerase gene, resulting in amino acid substitutions within the enzyme. Primary or major RAMs play a key role in conferring a drug-resistant phenotype by directly reducing drug susceptibility. Secondary and compensatory RAMs play an accessory role by increasing the level of resistance or restoring the functional defects caused by major RAMs [13]. Mutations are reported with the letters rt followed by the wild-type amino acid, the codon numbered position relative to the start of the rt region, followed by the mutant amino acid. For example, rtM204V describes the major LAM RAM, whereby methionine at RT codon 204 is replaced by valine.

Organisation of the HBV polymerase open reading frame, showing the reverse transcriptase (RT) region and its catalytic domains. The sequence corresponds to HBV genotype A (subtype adw2) (GenBank accession number AM282986); numbering is given according to the standardized nomenclature
3 Pathways of HBV Drug Resistance
Current treatment strategies for CHB are guided by a number of viral- and host-related parameters and mainly comprise (1) 1 year of treatment with peg-IFN-α or (2) long-term treatment with NAs [1, 2, 4, 5, 24]. Combination strategies of peg-IFN-α plus potent NAs are under evaluation [1]. Peg-IFN-α exerts both direct antiviral and immune modulatory functions by regulating the expression of interferon-stimulated genes (ISGs) [25]. In CHB, IFN-α causes immune activation, inhibition of HBV genome transcription, intracellular destabilization of viral nucleocapsid, and degradation of intracellular cccDNA via APOBEC3A [26–28]. A number of host genetic determinants have been shown to modulate IFN susceptibility, including an effect of viral genotype on the rate and kinetics of HBeAg and HBsAg loss. Generally, patients infected with HBV genotypes A and B show better responses to IFN-based therapy than patients with genotypes C and D, whilst responses to NAs appear to be comparable across different HBV genotypes [29]. Additionally, several mutations in the HBV genome (especially in pre-core and basal core promoter) have been shown to modulate responses to IFN-based treatment [30].
NAs compete with the natural substrate for binding to the active site of the HBV polymerase enzyme [31]. NAs must be phosphorylated to their nucleoside triphosphates or nucleotide di-phosphate derivatives in order to exert antiviral activity. Phosphorylation is mediated by cellular kinases and the initial phosphorylation is the rate-limiting step of the process, considered to modulate some of the differences in efficacy observed among NAs [8, 32]. Once phosphorylated, NAs are incorporated by the viral polymerase in the growing viral DNA chain, and act as chain terminators, inhibiting negative and positive HBV DNA strand synthesis. Based on the similarities between the HBV and HIV polymerase enzymes, it is not surprising that several NAs have dual antiviral activity [33]. Among available agents, LAM, emtricitabine (FTC), and tenofovir disoproxil (TDF) have significant activity against HIV. Entecavir (ETV) has a low residual antiretroviral activity and potential for selection of HIV drug resistance if used in isolation [34]. Adefovir dipivoxil (ADF) at HBV dosing and telbivudine (LdT) are not thought to exert anti-HIV activity.
NAs are classified into three structural groups: (1) l-nucleosides, (2) d-cyclopentanes, and (3) Acyclic (or alkyl) phosphonates (nucleotides). The classification corresponds to distinct pathways of resistance (Table 74.2) [5, 19, 21, 35]. Four major pathways are recognized: (1) the rtM204 pathway with l-nucleosides; (2) the rtN236T pathway with alkyl phosphonates; (3) the rtA181T/V pathway shared between the l-nucleosides and alkyl phosphonates; and (4) the d-cyclopentante pathway.
3.1 l-Nucleosides
l-Nucleosides comprise LAM and LdT, which are widely available worldwide; FTC, which is available in combination with TDF for the treatment of HIV and HBV co-infection; and clevudine, which is currently available in South Korea and the Philippines. The compounds have a similar molecular structure and bind to the same region of the viral polymerase, which results in shared resistance pathways and extensive cross-resistance [5, 8, 14, 19, 21, 35–50].
Resistant mutants generally remain susceptible to ADV and TDF [37, 51] and may retain partial susceptibility to ETV. The rtA181T/V mutation in domain B can emerge in treated patients and reduce susceptibility to both l-nucleosides and acyclic phosphonates [52–57].
3.1.1 Lamivudine
LAM was the first direct-acting antiviral agent to become available for the treatment of HBV infection. LAM was already used for the treatment of HIV infection and in this context codon M184 in the HIV RT catalytic site (YMDD motif) was identified as the major resistance site. Reflecting sequence homology between the two viral polymerases, the major HBV LAM resistance site is located at the corresponding codon 204 in the catalytic site (C domain) of the RT region of HBV polymerase. A single mutation that results in the substitution in YMDD of methionine by isoleucine (rtM204I), valine (rtM204V), or rarely serine (rtM204S) is sufficient to confer high-level LAM resistance. rtM204Q is an additional LAM RAM, conferring moderate drug resistance and displaying higher replication capacity than rtM204I [58].
During LAM treatment, M204I mutants are typically detected first, and subsequently replaced by rtM204V [12]. The mutants display reduced viral fitness. Molecular modelling indicates that rtM204I/V induce both steric hindrance and electrostatic repulsion for the incoming LAM tri-phosphate [8, 37, 59–61]. The catalytic activity of the polymerase is also reduced as a result, due to altered alignment of the natural substrate with respect to template and primer. With ongoing virus replication under LAM pressure, compensatory mutations occur in domain A (codon 80), domain B (codons 169, 173, 180), interdomain B-C (codon 184), and domain C (codons 202 and 215) [14, 21, 35, 38, 45–47, 50]. Compensatory mutations are insufficient to confer LAM resistance in isolation, but combined with rtM204 mutations they enhance resistance and improve enzymatic function and HBV replication. The negative electrical charge of rtL180M/C, for instance, decreases binding affinity for LAM-triphosphate, allowing better discrimination between the drug and the natural substrate [14, 60, 62]. In clonal and single genome sequences, LAM resistance and compensatory mutations typically coexist on the same viral genome [12].
3.1.2 Telbivudine
LdT is more potent than LAM in reducing serum HBV DNA levels in vivo [63, 64] and is also more potent than ADV [65]. LdT has an improved genetic barrier to the emergence of resistance relative to LAM, but shares a similar resistance profile, with rtM204I being the RAM most commonly observed in patients with virological breakthrough [19, 35, 42, 48, 49, 66–69].
3.2 d-Cyclopentanes
ETV, a synthetic analogue of 2-deoxyguanosine, displays a high genetic barrier to resistance in treatment-naïve patients, as resistance requires multiple substitutions to emerge [70–76]. ETV has high potency in both HbeAg-positive and HBeAg-negative treatment-naïve subjects [70, 71, 73, 74]. Due to shared resistance pathways however, ETV activity is reduced in LAM-experienced patients, requiring higher treatment doses and overall reducing the genetic barrier so that evolution of further resistance is facilitated [34, 45, 50, 77–81].
3.3 Acyclic Phosphonates (Nucleotides)
Alkyl nucleoside phosphonates comprise ADV and TDF. These compounds are structurally similar and possess a phosphonate group, requiring two rather than three phosphorylation steps to become intracellularly active [82]. Their structural similarity to the natural substrate deoxyadenosine triphosphate and the small, flexible phosphonate linker favour access to the HBV polymerase active site and high affinity for the enzyme [31, 32, 82].
3.3.1 Adefovir
ADV was initially developed for the treatment of HIV infection, but use was discontinued due to renal toxicity [8]. ADF suppresses HBV replication at significantly lower doses than those required to suppress HIV, and is safe at HBV dosing [83, 84] and putatively inactive against HIV. Development of HBV resistance to ADV occurs more slowly than seen with LAM, and is associated with mutations outside the YMDD motif, most commonly rtA181T (B domain) and rtN236T (D domain) [5, 8, 21, 35, 85–87]. The rtN236T mutant shows 7-fold resistance to ADV in vitro, which increases to 18-fold with the rtA181V + rtN236T double mutant [86]. The N236T mutation also has resistance effects for TDF, but confers no resistance to LAM and ETV. Molecular modelling reveals a possible mechanism of action for rtN236T. In wild-type HBV polymerase, the rtN236 amino acid may be hydrogen bonded to the adjacent rtS85 residue, and may interact directly with the γ-phosphate of ADF di-phosphate. The rtN236T mutation disrupts the hydrogen bond, thereby decreasing the binding affinity for ADF [88].
3.3.2 Tenofovir
The use of ADV for the treatment of CHB is declining, reflecting the superior virological efficacy of TDF in both HBeAg-positive and HBeAg-negative subjects [19, 35, 83, 84, 89–94]. TDF in vivo is converted to tenofovir, an acyclic nucleoside phosphonate (nucleotide) analogue of adenosine 5′-monophosphate. TDF is structurally related to ADV but at the standard dose achieves higher intracellular concentrations and displays higher binding affinity for the HBV polymerase enzyme [95]. This results in a greater virological potency and higher genetic barrier to resistance than ADF. The genotypic resistance profile of TDF remains controversial. The rtA194T mutation has been associated with partial TDF resistance and a negative impact on replication capacity of HBV constructs in vitro [96]. The mutational profile comprising rtA194T plus the LAM RAMs rtL180M + rtM204V/I has been proposed to reduce TDF susceptibility by over tenfold [97], although the finding has not been consistently reproduced [98]. The rtL180M + rtM204V/I + rtA194T mutation profile has a significant fitness cost, reducing replicative capacity by >75 %. The fitness defect of both rtA194T alone and in combination with rtL180M + rtM204V/I however is at least partially compensated through mutations in the pre-core and basal core promoter regions [96, 98], suggesting that patients with HBeAg-negative CHB may be particularly at risk of TDF resistance. The rt181T/V mutation has been shown to confer low-level resistance to TDF (two- to threefold); resistance levels increase with the combination of rt181T/V + rtN236T, which can be co-localized on the same viral genome [54, 86]. A further proposed pathway comprises rtP177G and rtF249A, which confer enhanced resistance to TDF and reduced replication capacity both in vitro and in vivo [99].
Despite these findings, genotypic HBV resistance to TDF has not been seen to emerge in clinical studies, including subjects with slow HBV DNA kinetics [100–102], and subjects undergoing continued treatment for 6 [91], 7 [89], or 8 [103] years. TDF retains activity in LAM-experienced [94, 104–106] and ETV-experienced [29] subjects, and is also effective, although less so, in patients with suboptimal treatment responses to ADV [5, 29, 94, 107, 108]. It has been proposed however that the double rtA181T/V + rtN236T mutant in particular is associated with inadequate virological response to TDF [107].
3.4 Genetic Barrier
The genetic barrier to the emergence of drug resistance is the expression of the interaction between multiple factors (Table 74.3) [19, 21, 38, 45, 50, 62, 88, 95, 98, 109, 110]. In general terms, the genetic barrier is low with LAM and FTC, intermediate with LdT and ADV, and high with ETV (in naïve patients) and TDF (Fig. 74.4). With LAM monotherapy, prevalence of RAMs is ~70 % after 4–5 years of treatment [21, 41, 111–114]. The rate of HBV replication is a key modulating factor, with a substantially higher risk of resistance observed in subjects with positive HBeAg status and high HBV DNA levels at start of therapy [12, 106] (Fig. 74.2). LdT resistance emerges more slowly, but rates are substantial, reaching 11 % and 26 % after 2 years in HBeAg-negative and HBeAg-positive subjects, respectively [64]. The cumulative incidence of ADV is 29 % after 5 years [83, 84, 115]. In patients receiving first-line therapy with ETV, rates of resistance are 1.2 % after 5 years for both HBeAg-positive and HBeAg-negative subjects [71, 75], increasing to 2.1 % at 7 years [116]. No resistance has been reported in over 400 patients that received first-line TDF for 7 [89] or even 8 [103] years.

Potency and genetic barrier of available antiviral agents against HBV
Antagonistic and synergist interactions between the resistance pathways of different drugs modulate the efficacy and genetic barrier of a combination regimen. Emergence of ETV resistance is accelerated by previous LAM exposure, and among subjects with LAM RAMs starting ETV, 51 % have ETV resistance after 5 years [75]. In LAM-experienced subjects with resistance, use of ADV add-on therapy with continuation of LAM shows superior virological efficacy to the use of ADV alone, in part reflecting the antagonism between the main pathways of LAM (rtM204) and ADV (rtN236T) resistance, which result in enhanced susceptibility to ADV, reduced emergence of ADV RAMs, and virological benefit, at least in subjects with low baseline HBV DNA levels [117–121].
4 Tests to Detect Drug Resistance
HBV drug resistance is assessed in clinical practice by demonstrating the presence in the RT domain of the viral polymerase of RAMs that are known to confer a drug-resistant phenotype. Testing is generally recommended in patients experiencing suboptimal treatment responses, as indicated by serum HBV DNA levels [1]. There have been several reports of the transmission of HBV drug-resistant variants; however the prevalence of transmitted HBV drug resistance is too low to support the cost-effectiveness of routine resistance testing prior to starting antiviral therapy [122, 123].
4.1 Genotypic Tests
HBV genotypic tests available for diagnostic use comprise conventional and deep genome sequencing and reverse hybridization mutation-specific assays (MSAs) (Table 74.4). Conventional population (Sanger) sequencing of DNA products amplified by PCR provides accurate results, is widely available, and is applicable to any region of the HBV genome. The method yields a consensus sequence of the dominant quasispecies present in a patient’s sample and has a sensitivity ranging from 10 to 20 %. Limitations therefore include inability to identify linkage of mutations at the individual genome level and limited sensitivity for low-frequency mutants. Deep sequencing is the process of parallel sequencing of millions of individual DNA molecules in a single assay, with thousands of clonal viral sequences being analysed to yield estimates of the number and proportion of unique variants within a sample. Deep sequencing offers increased sensitivity for low-frequency HBV RAMs, providing significant insights into viral kinetics during therapy [12, 124]. Deep sequencing platforms are becoming increasingly affordable and available for routine diagnostic use, although they continue to require extensive expertise in bioinformatics for the analysis of the large sequencing output. Deep sequencing is also vulnerable to errors at various stages of the process [125]. A 1 % interpretative cut-off is generally recommended to distinguish biologically significant findings from spurious detection [126, 127]. In addition, clinical validation studies are required to determine the clinical significance of any low-frequency RAM detected [125].
Among MSAs, the reverse hybridization line probe assay (INNO-LiPA) is commercially available, reliable, relatively inexpensive, and easy to perform. The assay uses a PCR-amplified product for reverse hybridization with specific oligonucleotide probes immobilized on nitrocellulose strips and shows higher sensitivity for low-frequency mutants than Sanger sequencing, generally ranging between 2 and 10 % of the total viral population. INNO-LiPA however remains less sensitive than deep sequencing, and detection is limited to the selected number of targeted RAMs. The major limitation of hybridization-based methods lies in their single-base discrimination. Specificity can be influenced by the sequences neighbouring a polymorphic site, or by interference from secondary structures, and the assay must be tailored for each targeted codon and across viral genotypes. Furthermore, as new RAMs are identified, the assays must be updated accordingly.
In research setting, clonal and single genome sequencing are labour-intensive and costly methods that apply Sanger sequencing to the analysis of single viral genomes [12, 128]. The methods allow detection of linkage of individual mutations on the same viral genome, and the study of the evolutionary pathways of resistant variants. Provided a large number of sequences are analysed, the methods also allow detection of low-frequency variants. Single genome sequencing offers the advantage over clonal sequencing of reducing errors related to in vitro recombination of PCR products.
Restriction fragment length polymorphism analysis and PCR-based methodologies such as allele-specific PCR have been used for research purposes to improve sensitivity of detection of low-frequency RAMs. The methods are generally labour-intensive, technically difficult, and expensive, and only detect known mutations requiring mutation-specific protocols. Assays undergoing development include nanopore and single-molecule long-read sequencing, technologies based on oligonucleotide microarrays (DNA chip) or mass spectrometry, and the amplification-refractory mutation system [129].
4.2 Phenotypic Tests
Phenotypic testing plays a key role in the research of the evolution and significance of HBV drug resistance. The characterization of novel mutations requires in vitro analysis to confirm the effects of the mutation on the viral phenotype, including both drug susceptibility and replication capacity [21, 128]. The methods employ HBV polymerase enzymatic assays and cell-culture methods. Most systems rely on the transfection of recombinant replication-competent HBV DNA into hepatoma cell lines. Testing may be performed with clinical isolates and site-directed mutants, allowing the analysis of the impact of mutations both individually and in combinations.
5 Definition of Virological Responses to HBV Therapy
Based upon the established close relationship between ongoing virus replication and liver disease progression the goal of CHB therapy is to achieve and maintain optimal suppression of serum HBV DNA load, as a key surrogate marker for clinical efficacy, and prevention of disease progression to cirrhosis, liver failure, or hepatocellular carcinoma [1, 4, 5, 130–132]. Further aims, which are difficult to achieve with currently available NA therapy, are to induce loss of HBeAg and anti-HBe seroconversion among HBeAg-positive subjects, and ideally, loss of HBsAg in all treated patients [1, 2, 116, 133]. Patients receiving antiviral treatment undergo regular monitoring of virological responses with HBV DNA assays that are sensitive and specific, offer a wide dynamic range of quantification, and are calibrated to express results in International Units [1, 5, 19, 21, 134].
An optimal virological response (VR) is defined as a serum HBV DNA level below the lower limit of quantification of validated assays, typically <15 or <30 IU/mL. With the highly potent NAs TDF and ETV, rates of virological suppression are >90 % in adherent patients after 3 years [71, 92, 135–137]. In 2006, the National Institutes of Health proposed a set of standardized, HBV-specific definitions to describe suboptimal responses to antiviral therapy, based upon HBV DNA levels measured at key time points after treatment initiation. These definitions remain in clinical use, although they require adjustments when applied to current treatment strategies [1], to reflect differences in antiviral potency and overall resistance risk relative to earlier compounds (Fig. 74.4).
5.1 Primary Non-response
Primary non-response is defined as the inability of treatment to reduce serum HBV DNA levels by ≥1 log10 IU/mL after 12 weeks of treatment or by ≥2 log10 after 24 weeks. It is uncommon with NAs, although seen more frequently with ADV (~10–20 %) than with other NAs because of suboptimal antiviral efficacy [111]. It is recommended that treatment be reviewed promptly, considering adherence as a key determinant, and addressing any concerns related to the anticipated drug efficacy, for instance, in the context of previous drug exposure and likely drug resistance. Patients on ADV monotherapy should be switched to more active therapy. In primary non-responders receiving TDF or ETV who show no evidence of resistance at week 24, continued therapy after 24 weeks may achieve suppression. One study compared the cumulative probability of obtaining a VR in patients with and without primary non-response after 12 or 24 weeks of ETV as first-line. Median time to VR was significantly shorter in primary responders than in non-responders at 24 weeks, but the cumulative probability of achieving a VR at 54 months was similar in the two groups (96 % vs. 100 %) [138]. Time to achieving VR and the cumulative probability of VR over time did not differ between primary responders and non-responders at 12 weeks. A more cautious approach is required when considering continuation of ETV therapy in patients with previous exposure to l-nucleosides due to the risk of resistance.
5.2 Partial Response
A partial response is defined by an initial response as measured at 12 or 24 weeks of therapy, followed by persistently detectable serum HBV DNA levels during continued therapy. Useful reference points include a HBV DNA >2000 IU/mL at 24 weeks or a detectable HBV DNA after 48 weeks of therapy [1]. Review is indicated, and management strategies take into account adherence and anticipated drug efficacy, together with the pre-treatment HBV DNA load, the kinetics of HBV DNA decay after starting therapy, and the likelihood of drug resistance emerging. Patients receiving LAM, LdT, or ADV should be switched to more potent therapy if the response is suboptimal at 24 weeks [1]. Even on potent NAs, some patients with high pre-treatment viral load may need longer to achieve complete HBV DNA suppression. ETV recipients with HBV DNA <1000 IU/mL after 48 weeks of therapy often achieve viral suppression by continuing ETV through at least 2 years total [139]. ETV recipients with higher HBV DNA levels at 48 weeks should be managed by switching to or adding TDF, whereas increasing ETV dose is not usually effective [140, 141]. Management strategies for slow responders to TDF monotherapy are less well defined. A subset of patients may benefit from a change of therapy or treatment intensification, particularly if the treatment history indicates partial resistance is possible, or where immunological function is impaired [101, 142].
5.3 Virological Rebound or Breakthrough
Virological rebound is defined by a confirmed serum HBV DNA increase of ≥1.0 log10 IU/mL relative to the lowest (nadir) level measured during continued treatment in a previous responder. Although the cut-off of 1 log10 is a useful indicator of a significant virological rebound, any HBV DNA increase above the assay quantification limit after achieving suppression should trigger a review. A confirmed viral load rebound typically signals lapses in adherence and drug resistance testing should be considered [5, 19, 21]. Low-level HBV DNA rebound may also reflect poor immunological function. Among HIV and HBV co-infected patients receiving long-term TDF-containing therapy, intermittent HBV DNA rebound is not uncommon; the risk is related to a history of profound immunocompromise as indicated by a low nadir CD4 cell count, but rebound does not appear to result in the selection of TDF resistance [100].
When considering the relevant HBV DNA load cut-off for defining virological breakthrough, it is also important to appreciate that the impaired fitness of emerging variants may initially limit the magnitude of HBV DNA increase. The addition of compensatory mutations that restore replicative capacity is typically signalled by an increase in serum HBV DNA load and serum aminotransferase levels, and potential for progression of liver disease [13, 38, 41].
6 Prevention and Management of HBV Drug Resistance
Development of HBV drug resistance can be largely avoided by starting therapy with drugs that have high potency and a high genetic barrier to resistance—typically TDF or ETV—and with regular monitoring of treatment responses and ongoing re-enforcement of adherence [1, 5, 19, 111, 143, 144]. In a meta-analysis, TDF and ETV as first-line therapy showed no difference in overall virological efficacy and safety over 48 weeks [145]. Long-term data also support the virological efficacy and safety of both treatment options [1, 71, 89, 91, 103, 116, 131]. TDF monotherapy appears to be sufficient even in patients with high baseline HBV DNA load [146], although the combination of TDF plus FTC appears to be more effective than TDF alone in immunotolerant subjects with normal transaminases and high HBV DNA levels (>1.7 × 107 IU/mL) [147]. Combination therapy with TDF and ETV also appears to have a marginal advantage over ETV monotherapy in patients with high HBV DNA levels (≥108 IU/mL) [148].
Avoiding the use of LAM, LdT, or ADV as single agents is generally recommended due to the risk of resistance [1, 111, 143]. LdT monotherapy may have a role in selected scenarios, including the prevention of mother-to-child transmission [1]. It has also been argued that LAM monotherapy can be safe and cost-effective as first-line treatment in selected patients with a favourable profile (i.e. low HBV DNA levels, absence of significant fibrosis or cirrhosis), or as a maintenance option after achieving serum HBV DNA suppression with more potent first-line treatment [149, 150]. Further studies are required to provide support for these strategies.
There remain a large number of patients that developed HBV drug resistance prior to TDF or ETV becoming available, and from a global perspective many remain at risk due to regionally limited availability of these more costly compounds [151, 152]. Monotherapy with LAM, ADV, or LdT was frequently prescribed in Europe between 2008 and 2010; among treated subjects undergoing resistance testing monotherapy was frequently associated with the detection of drug resistance, especially HBV RAMs of the rtM204 pathway [151]. The adverse consequences of developing NA resistance have been well documented. Patients treated with LAM or ADV who develop virological breakthrough and emergence of drug resistance frequently experience exacerbation and progression of liver disease [19, 106, 153–157]. In a study of cirrhotic patients treated with LAM, disease progression (as measured by a composite end-point of liver-related complications and mortality) occurred in 13 % of patients who developed LAM RAMs compared with 5 % of patients who did not develop resistance [158]. Furthermore, sequential rescue therapy increases the risk of developing hard-to-treat multidrug-resistant (MDR) HBV variants [5, 19, 21, 159].
In patients with LAM resistance, add-on therapy with ADV while continuing LAM is superior to switching to ADV alone, and switching to TDF monotherapy is superior to add-on therapy with LAM plus ADV [108] (Table 74.5). TDF alone is as effective for the treatment of patients with the rtM204I/V ± rtL180M as the combination of TDF plus FTC: in a randomized clinical trial, HBV DNA suppression rates over 96 weeks were 89 % and 86 % with TDF and TDF + FTC, respectively, with no treatment-emergent TDF resistance [105].
TDF is generally less effective for patients with ADV resistance [1, 160]. Patients with the double ADV mutant rtA181T/V + rtN236T may be especially at risk of poor responses [107]. Combination therapy with TDF plus FTC shows superior virological efficacy than TDF monotherapy in this setting [161].
ETV is an alternative treatment option in patients with ADV resistance, with 84 % achieving virological suppression after 24 months, although responses are blunted by previous LAM exposure [79, 162]. Whilst ETV use after prolonged LAM therapy failure is not uncommon in clinical practice, ETV monotherapy in l-nucleoside-experienced subjects is associated with a risk of virological breakthrough and evolution of ETV resistance [151] and is not generally recommended [1].
Combination therapy with ETV and TDF is usually effective in patients with MDR [163]. However combination therapy is not necessarily required in patients with more limited resistance. A multicentre trial investigated patients with ADF RAMs (rtA181V/T and/or rtN236T) randomized to receive TDF monotherapy or TDF plus ETV (1 mg/day) combination therapy [164]. At week 48, the two arms showed similar rates of HBV DNA suppression (62 % vs. 63.5 %; p = 0.88) and a similar mean change in HBV DNA levels from baseline (−3.03 vs. −3.31 log10 IU/mL; p = 0.38). A second multicentre randomized trial investigated patients with ETV RAMs (rtM204V/I and at least one of rtT184A/C/F/G/I/L/S, rtS202G, or rtM250L/V) randomized to receive TDF monotherapy or TDF plus ETV (1 mg/day) combination therapy [165]. At week 48, the two arms showed similar rates of HBV DNA suppression (71 % vs. 73 %; p > 0.99) and a similar mean change in HBV DNA levels from baseline (−3.66 vs. −3.74 log10 IU/mL; p = 0.81). In both trials, no patient developed additional RAMs, and safety profiles were comparable in the two groups.
Development of further treatment options is needed to manage certain subgroups of patients. These may include patients with LAM resistance that experience or are at increased risk of TDF toxicity, typically in the form of reduced renal function. These patients are often managed through TDF dose reductions, raising concerns about both ongoing risk of toxicity and sustained virological suppression. There is hope that the novel compound tenofovir alafenamide (TAF) will retain the high efficacy of TDF against HBV combined with an improved renal and bone safety profile. Besifovir is a new nucleotide analogue that has undergone testing in treatment-naïve patients with CHB. Over 96 weeks, besifovir caused over a 5 log10 IU/mL decline in HBV DNA levels and suppression rates of around 80 % and similar responses were seen in the comparator arm receiving ETV [166]. There was a low overall incidence of virological breakthrough and no development of drug resistance in both arms. CAdAs (4′-C-cyano-2-amino-2′-deoxyadenosine) are novel compounds that offer hope for the management of drug-resistant HBV [167]. Finally, new treatment strategies are also required to improve long-term control of CHB and allow discontinuation of NA therapy after induction [5–7].
7 The Challenge of HIV-HBV Infection in Resource-Limited Settings
In sub-Saharan Africa (SSA), chronic infection with HBV is an important public health issue characterized by high prevalence, frequent co-infection with HIV, and suboptimally applied ascertainment and management strategies [152, 168]. Among people living with HIV, between 6 and 25 % are co-infected with HBV, and co-infection accelerates fibrosis and increases the risk of liver-related morbidity and mortality. In part as a consequence of reduced HIV-related mortality, cirrhosis and hepatocellular carcinoma (HCC) are increasing in the region. For many years, regimens for first-line ART in SSA have been “HBV-blind” and employed LAM plus zidovudine or stavudine in combination with efavirenz or nevirapine. This approach has led to large numbers of HIV and HBV co-infected patients receiving LAM as the sole HBV-active agent across much of SSA, with the resulting associated risk of drug resistance and liver disease progression. In a typical cohort of HIV and HBV co-infected patients in Ghana, after nearly 4 years of standard LAM-containing ART, over half of patients had detectable HBV DNA, one-third had DNA levels >2000 IU/mL, one-third had HBV LAM resistance by Sanger sequencing, and one in eight had advanced liver fibrosis as determined by transient elastography [106]. In this cohort, the introduction of TDF led to substantial improvements in HBV DNA suppression and promising evidence of reversal of liver fibrosis.
Whilst TDF is now recommended for first-line antiretroviral therapy in all patients with HIV in SSA, availability remains far from universal and much remains to be done to improve the diagnosis and management of CHB in populations with and without HIV. The World Health Organisation [169] has released guidelines for CHB in resource-limited settings that aim to promote the use of simple, non-invasive diagnostic tests to assess the stage of liver disease and eligibility for treatment; prioritize treatment for those with most advanced liver disease and at greatest risk of mortality; and preferential use of NAs with a high barrier to drug resistance (TDF and ETV). These recommendations provide opportunities to improve the clinical outcomes of persons living with CHB in these settings and reduce HBV incidence and transmission. Implementation remains challenging.
References
Martin P, Lau DT, Nguyen MH, Janssen HL, Dieterich DT, Peters MG, Jacobson IM. A Treatment algorithm for the management of chronic hepatitis B virus Infection in the United States: 2015 update. Clin Gastroenterol Hepatol. 2015;13(12):2071–87.e16.
Buti M. HBeAg-positive chronic hepatitis B: why do I treat my patients with nucleos(t)ide analogs? Liver Int. 2014;34 Suppl 1:108–11.
Jordheim LP, Durantel D, Zoulim F, Dumontet C. Advances in the development of nucleoside and nucleotide analogues for cancer and viral diseases. Nat Rev Drug Discov. 2013;12:447–64.
Lampertico P, Liaw YF. New perspectives in the therapy of chronic hepatitis B. Gut. 2012;61 Suppl 1:i18–24.
Zoulim F, Durantel D. Antiviral therapies and prospects for a cure of chronic hepatitis B. Cold Spring Harb Perspect Med. 2015;1:5(4).
Block TM, Rawat S, Brosgart CL. Chronic hepatitis B: A wave of new therapies on the horizon. Antiviral Res. 2015;121:69–81.
Wang XY, Chen HS. Emerging antivirals for the treatment of hepatitis B. World J Gastroenterol. 2014;20:7707–17.
Ghany M, Liang TJ. Drug targets and molecular mechanisms of drug resistance in chronic hepatitis B. Gastroenterology. 2007;132:1574–85.
Nassal M. Hepatitis B viruses: reverse transcription a different way. Virus Res. 2008;134:235–49.
Girones R, Miller RH. Mutation rate of the hepadnavirus genome. Virology. 1989;170:595–7.
Nowak MA, Bonhoeffer S, Hill AM, Boehme R, Thomas HC, McDade H. Viral dynamics in hepatitis B virus infection. Proc Natl Acad Sci U S A. 1996;93:4398–402.
Aoudjane S, Chaponda M, del Castillo AAG, O’Connor J, Noguera M, Beloukas A, Hopkins M, Khoo S, van Oosterhout JJ, Geretti AM. Hepatitis B virus sub-genotype A1 infection Is characterized by high replication levels and rapid emergence of drug resistance in HIV-positive adults receiving first-line antiretroviral therapy in Malawi. Clin Infect Dis. 2014;59:1618–26.
Lok AS, Zoulim F, Locarnini S, Bartholomeusz A, Ghany MG, Pawlotsky JM, Liaw YF, Mizokami M, Kuiken C. Antiviral drug-resistant HBV: standardization of nomenclature and assays and recommendations for management. Hepatology. 2007;46:254–65.
Shaw T, Bartholomeusz A, Locarnini S. HBV drug resistance: mechanisms, detection and interpretation. J Hepatol. 2006;44:593–606.
Geretti AM, Patel M, Sarfo FS, Chadwick D, Verheyen J, Fraune M, Garcia A, Phillips RO. Detection of highly prevalent hepatitis B virus coinfection among HIV-seropositive persons in Ghana. J Clin Microbiol. 2010;48:3223–30.
Lacombe K, Boyd A, Lavocat F, Pichoud C, Gozlan J, Miailhes P, Lascoux-Combe C, Vernet G, Girard PM, Zoulim F. High incidence of treatment-induced and vaccine-escape hepatitis B virus mutants among human immunodeficiency virus/hepatitis B-infected patients. Hepatology. 2013;58:912–22.
Coffin CS, Mulrooney-Cousins PM, Peters MG, van Marle G, Roberts JP, Michalak TI, Terrault NA. Molecular characterization of intrahepatic and extrahepatic hepatitis B virus (HBV) reservoirs in patients on suppressive antiviral therapy. J Viral Hepat. 2011;18:415–23.
Nassal M. HBV cccDNA: viral persistence reservoir and key obstacle for a cure of chronic hepatitis B. Gut. 2015;64(12):1972–84.
Gish R, Jia JD, Locarnini S, Zoulim F. Selection of chronic hepatitis B therapy with high barrier to resistance. Lancet Infect Dis. 2012;12:341–53.
Wong DK, Seto WK, Fung J, Ip P, Huang FY, Lai CL, Yuen MF. Reduction of hepatitis B surface antigen and covalently closed circular DNA by nucleos(t)ide analogues of different potency. Clin Gastroenterol Hepatol. 2013;11:1004–10.
Zoulim F, Locarnini S. Hepatitis B virus resistance to nucleos(t)ide analogues. Gastroenterology. 2009;137:1593–608.
Pan WL, Hu JL, Fang Y, Luo Q, Xu G, Xu L, Jing ZH, Shan XF, Zhu YL, Huang AL. Allele-specific polymerase chain reaction for detection of a mutation in the relax circular DNA and the covalently closed circular DNA of hepatitis B virus. J Virol Methods. 2013;194:277–9.
Stuyver LJ, Locarnini SA, Lok A, Richman DD, Carman WF, Dienstag JL, Schinazi RF. Nomenclature for antiviral-resistant human hepatitis B virus mutations in the polymerase region. Hepatology. 2001;33:751–7.
Kao JH. HBeAg-positive chronic hepatitis B: why do I treat my patients with pegylated interferon? Liver Int. 2014;34 Suppl 1:112–9.
Sadler AJ, Williams BR. Interferon-inducible antiviral effectors. Nat Rev Immunol. 2008;8:559–68.
Lucifora J, Xia Y, Reisinger F, Zhang K, Stadler D, Cheng X, Sprinzl MF, Koppensteiner H, Makowska Z, Volz T, Remouchamps C, Chou WM, Thasler WE, Huser N, Durantel D, Liang TJ, Munk C, Heim MH, Browning JL, Dejardin E, Dandri M, Schindler M, Heikenwalder M, Protzer U. Specific and nonhepatotoxic degradation of nuclear hepatitis B virus cccDNA. Science. 2014;343:1221–8.
Micco L, Peppa D, Loggi E, Schurich A, Jefferson L, Cursaro C, Panno AM, Bernardi M, Brander C, Bihl F, Andreone P, Maini MK. Differential boosting of innate and adaptive antiviral responses during pegylated-interferon-alpha therapy of chronic hepatitis B. J Hepatol. 2013;58:225–33.
Thimme R, Dandri M. Dissecting the divergent effects of interferon-alpha on immune cells: time to rethink combination therapy in chronic hepatitis B? J Hepatol. 2013;58:205–9.
Lin CL, Kao JH. Hepatitis B virus genotypes and variants. Cold Spring Harb Perspect Med. 2015;5:a021436.
Tseng TC, Liu CJ, Kao JH. Implications of hepatitis B virus genomic variations on treatment outcomes. Curr Pharmacogenomics Person Med. 2010;8:280–8.
De Clercq E. Current treatment of hepatitis B virus infections. Rev Med Virol. 2015;25(6):354–65.
De Clercq E. Strategies in the design of antiviral drugs. Nat Rev Drug Discov. 2002;1:13–25.
Wilkins E, Nelson M, Agarwal K, Awoyemi D, Barnes E, Bhagani S, Brook G, Brown A, Castelino S, Cooke G, Fisher M, Geretti AM, James R, Kulasegaram R, Leen C, Mutimer D, Orkin C, Page E, Palfreeman A, Papineni P, Rodger A, Tong CY. British HIV Association guidelines for the management of hepatitis viruses in adults infected with HIV 2013. HIV Med. 2013;14 Suppl 4:1–71.
Domaoal RA, McMahon M, Thio CL, Bailey CM, Tirado-Rives J, Obikhod A, Detorio M, Rapp KL, Siliciano RF, Schinazi RF, Anderson KS. Pre-steady-state kinetic studies establish entecavir 5′-triphosphate as a substrate for HIV-1 reverse transcriptase. J Biol Chem. 2008;283:5452–9.
Menendez-Arias L, Alvarez M, Pacheco B. Nucleoside/nucleotide analog inhibitors of hepatitis B virus polymerase: mechanism of action and resistance. Curr Opin Virol. 2014;8:1–9.
Bozdayi AM, Uzunalimoglu O, Turkyilmaz AR, Aslan N, Sezgin O, Sahin T, Bozdayi G, Cinar K, Pai SB, Pai R, Bozkaya H, Karayalcin S, Yurdaydin C, Schinazi RF. YSDD: a novel mutation in HBV DNA polymerase confers clinical resistance to lamivudine. J Viral Hepat. 2003;10:256–65.
Das K, Xiong X, Yang H, Westland CE, Gibbs CS, Sarafianos SG, Arnold E. Molecular modeling and biochemical characterization reveal the mechanism of hepatitis B virus polymerase resistance to lamivudine (3TC) and emtricitabine (FTC). J Virol. 2001;75:4771–9.
Delaney WE, Yang H, Westland CE, Das K, Arnold E, Gibbs CS, Miller MD, Xiong S. The hepatitis B virus polymerase mutation rtV173L is selected during lamivudine therapy and enhances viral replication in vitro. J Virol. 2003;77:11833–41.
Jones SA, Murakami E, Delaney W, Furman P, Hu J. Noncompetitive inhibition of hepatitis B virus reverse transcriptase protein priming and DNA synthesis by the nucleoside analog clevudine. Antimicrob Agents Chemother. 2013;57:4181–9.
Kwon SY, Park YK, Ahn SH, Cho ES, Choe WH, Lee CH, Kim BK, Ko SY, Choi HS, Park ES, Shin GC, Kim KH. Identification and characterization of clevudine-resistant mutants of hepatitis B virus isolated from chronic hepatitis B patients. J Virol. 2010;84:4494–503.
Lai CL, Dienstag J, Schiff E, Leung NW, Atkins M, Hunt C, Brown N, Woessner M, Boehme R, Condreay L. Prevalence and clinical correlates of YMDD variants during lamivudine therapy for patients with chronic hepatitis B. Clin Infect Dis. 2003;36:687–96.
Lai CL, Leung N, Teo EK, Tong M, Wong F, Hann HW, Han S, Poynard T, Myers M, Chao G, Lloyd D, Brown NA. A 1-year trial of telbivudine, lamivudine, and the combination in patients with hepatitis B e antigen-positive chronic hepatitis B. Gastroenterology. 2005;129:528–36.
Lim SG, Krastev Z, Ng TM, Mechkov G, Kotzev IA, Chan S, Mondou E, Snow A, Sorbel J, Rousseau F. Randomized, double-blind study of emtricitabine (FTC) plus clevudine versus FTC alone in treatment of chronic hepatitis B. Antimicrob Agents Chemother. 2006;50:1642–8.
Lim SG, Ng TM, Kung N, Krastev Z, Volfova M, Husa P, Lee SS, Chan S, Shiffman ML, Washington MK, Rigney A, Anderson J, Mondou E, Snow A, Sorbel J, Guan R, Rousseau F. A double-blind placebo-controlled study of emtricitabine in chronic hepatitis B. Arch Intern Med. 2006;166:49–56.
Locarnini S. Primary resistance, multidrug resistance, and cross-resistance pathways in HBV as a consequence of treatment failure. Hepatol Int. 2008;2:147–51.
Nakanishi H, Kurosaki M, Asahina Y, Onuki Y, Ueda K, Nishimura Y, Tsuchiya K, Kitamura T, Uchihara M, Miyake S, Enomoto N, Izumi N. Polymerase domain B mutation is associated with hepatitis relapse during long-term lamivudine therapy for chronic hepatitis B. Intervirology. 2005;48:381–8.
Pai SB, Bozdayi AM, Pai RB, Beker T, Sarioglu M, Turkyilmaz AR, Grier J, Yurdaydin C, Schinazi RF. Emergence of a novel mutation in the FLLA region of hepatitis B virus during lamivudine therapy. Antimicrob Agents Chemother. 2005;49:2618–24.
Seifer M, Patty A, Serra I, Li B, Standring DN. Telbivudine, a nucleoside analog inhibitor of HBV polymerase, has a different in vitro cross-resistance profile than the nucleotide analog inhibitors adefovir and tenofovir. Antiviral Res. 2009;81:147–55.
Sun J, Xie Q, Tan D, Ning Q, Niu J, Bai X, Fan R, Chen S, Cheng J, Yu Y, Wang H, Xu M, Shi G, Wan M, Chen X, Tang H, Sheng J, Dou X, Shi J, Ren H, Wang M, Zhang H, Gao Z, Chen C, Ma H, Jia J, Hou J. The 104-week efficacy and safety of telbivudine-based optimization strategy in chronic hepatitis B patients: a randomized, controlled study. Hepatology. 2014;59:1283–92.
Yuen L, Bartholomeusz A, Ayres A, Littlejohn M, Locarnini S. Multidrug resistance and cross-resistance pathways in HBV as a consequence of treatment failure. Hepatology. 2008;2(2):147–51.
Lada O, Benhamou Y, Cahour A, Katlama C, Poynard T, Thibault V. In vitro susceptibility of lamivudine-resistant hepatitis B virus to adefovir and tenofovir. Antivir Ther. 2004;9:353–63.
Karatayli E, Karayalcin S, Karaaslan H, Kayhan H, Turkyilmaz AR, Sahin F, Yurdaydin C, Bozdayi AM. A novel mutation pattern emerging during lamivudine treatment shows cross-resistance to adefovir dipivoxil treatment. Antivir Ther. 2007;12(5):761–8.
Lacombe K, Ollivet A, Gozlan J, Durantel S, Tran N, Girard PM, Zoulim F. A novel hepatitis B virus mutation with resistance to adefovir but not to tenofovir in an HIV-hepatitis B virus-co-infected patient. AIDS. 2006;20:2229–31.
Villet S, Pichoud C, Billioud G, Barraud L, Durantel S, Trepo C, Zoulim F. Impact of hepatitis B virus rtA181V/T mutants on hepatitis B treatment failure. J Hepatol. 2008;48:747–55.
Warner N, Locarnini S. The antiviral drug selected hepatitis B virus rtA181T/sW172* mutant has a dominant negative secretion defect and alters the typical profile of viral rebound. Hepatology. 2008;48:88–98.
Yatsuji H, Noguchi C, Hiraga N, Mori N, Tsuge M, Imamura M, Takahashi S, Iwao E, Fujimoto Y, Ochi H, Abe H, Maekawa T, Tateno C, Yoshizato K, Suzuki F, Kumada H, Chayama K. Emergence of a novel lamivudine-resistant hepatitis B virus variant with a substitution outside the YMDD motif. Antimicrob Agents Chemother. 2006;50:3867–74.
Yeh CT, Chien RN, Chu CM, Liaw YF. Clearance of the original hepatitis B virus YMDD-motif mutants with emergence of distinct lamivudine-resistant mutants during prolonged lamivudine therapy. Hepatology. 2000;31:1318–26.
Liu Y, Xu Z, Wang Y, Li X, Liu L, Chen L, Xin S, Xu D. rtM204Q may serve as a novel lamivudine-resistance-associated mutation of hepatitis B virus. PLoS One. 2014;9:e89015.
Allen MI, Deslauriers M, Andrews CW, Tipples GA, Walters KA, Tyrrell DL, Brown N, Condreay LD. Identification and characterization of mutations in hepatitis B virus resistant to lamivudine. Hepatology. 1998;27:1670–7.
Chong Y, Stuyver L, Otto MJ, Schinazi RF, Chu CK. Mechanism of antiviral activities of 3′-substituted L-nucleosides against 3TC-resistant HBV polymerase: a molecular modelling approach. Antivir Chem Chemother. 2003;14:309–19.
Lee K, Chu CK. Molecular modeling approach to understanding the mode of action of L-nucleosides as antiviral agents. Antimicrob Agents Chemother. 2001;45:138–44.
Hong YB, Choi Y, Jung G. Increased DNA polymerase fidelity of the lamivudine resistant variants of human hepatitis B virus DNA polymerase. J Biochem Mol Biol. 2004;37:167–76.
Lai CL, Gane E, Liaw YF, Hsu CW, Thongsawat S, Wang Y, Chen Y, Heathcote EJ, Rasenack J, Bzowej N, Naoumov NV, Di Bisceglie AM, Zeuzem S, Moon YM, Goodman Z, Chao G, Constance BF, Brown NA. Telbivudine versus lamivudine in patients with chronic hepatitis B. N Engl J Med. 2007;357:2576–88.
Liaw YF, Gane E, Leung N, Zeuzem S, Wang YM, Lai CL, Heathcote EJ, Manns M, Bzowej N, Niu JQ, Han SH, Hwang SG, Cakaloglu Y, Tong MJ, Papatheodoridis G, Chen YG, Brown NA, Albanis E, Galil K, Naoumov NV. 2-Year GLOBE trial results: Telbivudine is superior to lamivudine in patients with chronic hepatitis B. Gastroenterology. 2009;136:486–95.
Chan HLY, Heathcote EJ, Marcellin P, Lai CL, Cho M, Moon YM, Chao YC, Myers RP, Minuk GY, Jeffers L, Sievert W, Bzowej N, Harb G, Kaiser R, Qiao XJ, Brown NA. Treatment of hepatitis B e antigen positive chronic hepatitis with telbivudine or adefovir: a randomized trial. Ann Intern Med. 2007;147:745–54.
Hou J, Yin YK, Xu D, Tan D, Niu J, Zhou X, Wang Y, Zhu L, He Y, Ren H, Wan M, Chen C, Wu S, Chen Y, Xu J, Wang Q, Wei L, Chao G, Constance BF, Harb G, Brown NA, Jia J. Telbivudine versus lamivudine in Chinese patients with chronic hepatitis B: results at 1 year of a randomized, double-blind trial. Hepatology. 2008;47:447–54.
Lui YY, Chan HL. A review of telbivudine for the management of chronic hepatitis B virus infection. Expert Opin Drug Metab Toxicol. 2008;4:1351–61.
Tsai MC, Yu HC, Hung CH, Lee CM, Chiu KW, Lin MT, Tseng PL, Chang KC, Yen YH, Chen CH, Hu TH. Comparing the efficacy and clinical outcome of telbivudine and entecavir naive patients with hepatitis B virus-related compensated cirrhosis. J Gastroenterol Hepatol. 2014;29:568–75.
Yuen MF, Lai CL. Telbivudine: an upcoming agent for chronic hepatitis B. Expert Rev Anti Infect Ther. 2005;3:489–94.
Chang TT, Gish RG, de Man R, Gadano A, Sollano J, Chao YC, Lok AS, Han KH, Goodman Z, Zhu J, Cross A, DeHertogh D, Wilber R, Colonno R, Apelian D. A comparison of entecavir and lamivudine for HBeAg-positive chronic hepatitis B. N Engl J Med. 2006;354:1001–10.
Chang TT, Lai CL, Kew Yoon S, Lee SS, Coelho HS, Carrilho FJ, Poordad F, Halota W, Horsmans Y, Tsai N. Entecavir treatment for up to 5 years in patients with hepatitis B e antigen-positive chronic hepatitis B. Hepatology. 2010;51:422–30.
Colonno RJ, Rose R, Baldick CJ, Levine S, Pokornowski K, Yu CF, Walsh A, Fang J, Hsu M, Mazzucco C, Eggers B, Zhang S, Plym M, Klesczewski K, Tenney DJ. Entecavir resistance is rare in nucleoside naive patients with hepatitis B. Hepatology. 2006;44:1656–65.
Gish RG, Lok AS, Chang TT, Lde Man RA, Gadano A, Sollano J, Han KH, Chao YC, Lee SD, Harris M, Yang J, Colonno R, Brett-Smith H. Entecavir therapy for up to 96 weeks in patients with HBeAg-positive chronic hepatitis B. Gastroenterology. 2007;133:1437–44.
Lai CL, Shouval D, Lok AS, Chang TT, Cheinquer H, Goodman Z, DeHertogh D, Wilber R, Zink RC, Cross A, Colonno R, Fernandes L. Entecavir versus lamivudine for patients with HBeAg-negative chronic hepatitis B. N Engl J Med. 2006;354:1011–20.
Tenney DJ, Rose RE, Baldick CJ, Pokornowski KA, Eggers BJ, Fang J, Wichroski MJ, Xu D, Yang J, Wilber RB, Colonno RJ. Long-term monitoring shows hepatitis B virus resistance to entecavir in nucleoside-naive patients is rare through 5 years of therapy. Hepatology. 2009;49:1503–14.
Villet S, Ollivet A, Pichoud C, Barraud L, Villeneuve JP, Trepo C, Zoulim F. Stepwise process for the development of entecavir resistance in a chronic hepatitis B virus infected patient. J Hepatol. 2007;46:531–8.
Baldick CJ, Tenney DJ, Mazzucco CE, Eggers BJ, Rose RE, Pokornowski KA, Yu CF, Colonno RJ. Comprehensive evaluation of hepatitis B virus reverse transcriptase substitutions associated with entecavir resistance. Hepatology. 2008;47:1473–82.
Hayashi S, Murakami S, Omagari K, Matsui T, Iio E, Isogawa M, Watanabe T, Karino Y, Tanaka Y. Characterization of novel entecavir resistance mutations. J Hepatol. 2015;63:546–53.
Reijnders JGP, Deterding K, Petersen J, Zoulim F, Santantonio T, Buti M, van Bommel F, Hansen BE, Wedemeyer H, Janssen HLA. Antiviral effect of entecavir in chronic hepatitis B: influence of prior exposure to nucleos(t)ide analogues. J Hepatol. 2010;52:493–500.
Sherman M, Yurdaydin C, Sollano J, Silva M, Liaw YF, Cianciara J, Boron-Kaczmarska A, Martin P, Goodman Z, Colonno R, Cross A, Denisky G, Kreter B, Hindes R. Entecavir for treatment of lamivudine-refractory, HBeAg-positive chronic hepatitis B. Gastroenterology. 2006;130:2039–49.
Tenney DJ, Levine SM, Rose RE, Walsh AW, Weinheimer SP, Discotto L, Plym M, Pokornowski K, Yu CF, Angus P, Ayres A, Bartholomeusz A, Sievert W, Thompson G, Warner N, Locarnini S, Colonno RJ. Clinical emergence of entecavir-resistant hepatitis B virus requires additional substitutions in virus already resistant to lamivudine. Antimicrob Agents Chemother. 2004;48:3498–507.
De Clercq E, Holy A. Acyclic nucleoside phosphonates: a key class of antiviral drugs. Nat Rev Drug Discov. 2005;4:928–40.
Marcellin P, Chang TT, Lim SG, Sievert W, Tong M, Arterburn S, Borroto-Esoda K, Frederick D, Rousseau F. Long-term efficacy and safety of adefovir dipivoxil for the treatment of hepatitis B e antigen-positive chronic hepatitis B. Hepatology. 2008;48:750–8.
Marcellin P, Heathcote EJ, Buti M, Gane E, de Man RA, Krastev Z, Germanidis G, Lee SS, Flisiak R, Kaita K, Manns M, Kotzev I, Tchernev K, Buggisch P, Weilert F, Kurdas OO, Shiffman ML, Trinh H, Washington MK, Sorbel J, Anderson J, Snow-Lampart A, Mondou E, Quinn J, Rousseau F. Tenofovir disoproxil fumarate versus adefovir dipivoxil for chronic hepatitis B. N Engl J Med. 2008;359:2442–55.
Angus P, Vaughan R, Xiong S, Yang H, Delaney W, Gibbs C, Brosgart C, Colledge D, Edwards R, Ayres A, Bartholomeusz A, Locarnini S. Resistance to adefovir dipivoxil therapy associated with the selection of a novel mutation in the HBV polymerase. Gastroenterology. 2003;125:292–7.
Qi X, Xiong S, Yang H, Miller M, Delaney WE. In vitro susceptibility of adefovir-associated hepatitis B virus polymerase mutations to other antiviral agents. Antivir Ther. 2007;12:355–62.
Schildgen O, Sirma H, Funk A, Olotu C, Wend UC, Hartmann H, Helm M, Rockstroh JK, Willems WR, Will H, Gerlich WH. Variant of hepatitis B virus with primary resistance to adefovir. N Engl J Med. 2006;354:1807–12.
Yadav V, Chu CK. Molecular mechanisms of adefovir sensitivity and resistance in HBV polymerase mutants: a molecular dynamics study. Bioorg Med Chem Lett. 2004;14:4313–7.
Buti M, Tsai N, Petersen J, Flisiak R, Gurel S, Krastev Z, Schall RA, Flaherty JF, Martins EB, Charuworn P, Kitrinos KM, Subramanian GM, Gane E, Marcellin P. Seven-year efficacy and safety of treatment with tenofovir disoproxil fumarate for chronic hepatitis B virus infection. Dig Dis Sci. 2015;60:1457–64.
Delaney WE, Ray AS, Yang H, Qi X, Xiong S, Zhu Y, Miller MD. Intracellular metabolism and in vitro activity of tenofovir against hepatitis B virus. Antimicrob Agents Chemother. 2006;50:2471–7.
Kitrinos KM, Corsa A, Liu Y, Flaherty J, Snow-Lampart A, Marcellin P, Borroto-Esoda K, Miller MD. No detectable resistance to tenofovir disoproxil fumarate after 6 years of therapy in patients with chronic hepatitis B. Hepatology. 2014;59:434–42.
Marcellin P, Gane E, Buti M, Gane E, Buti M, Afdhal N, Sievert W, Jacobson IM, Washington MK, Germanidis G, Flaherty JF, Schall RA, Bornstein JD, Kitrinos KM, Subramanian GM, McHutchison JG, Heathcote EJ. Regression of cirrhosis during treatment with tenofovir disoproxil fumarate for chronic hepatitis B: a 5-year open-label follow-up study. Lancet. 2013;381:468–75.
Snow-Lampart A, Chappell B, Curtis M, Zhu Y, Myrick F, Schawalder J, Kitrinos K, Svarovskaia ES, Miller MD, Sorbel J, Heathcote J, Marcellin P, Borroto-Esoda K. No resistance to tenofovir disoproxil fumarate detected after up to 144 weeks of therapy in patients monoinfected with chronic hepatitis B virus. Hepatology. 2011;53:763–73.
van Bommel F, Zollner B, Sarrazin C, Spengler U, Huppe D, Moller B, Feucht HH, Wiedenmann B, Berg T. Tenofovir for patients with lamivudine-resistant hepatitis B virus (HBV) infection and high HBV DNA level during adefovir therapy. Hepatology. 2006;44:318–25.
van Hemert FJ, Berkhout B, Zaaijer HL. Differential binding of tenofovir and adefovir to reverse transcriptase of hepatitis B virus. PLoS One. 2014;9:e106324.
Amini-Bavil-Olyaee S, Herbers U, Sheldon J, Luedde T, Trautwein C, Tacke F. The rtA194T polymerase mutation impacts viral replication and susceptibility to tenofovir in hepatitis B e antigen-positive and hepatitis B e antigen-negative hepatitis B virus strains. Hepatology. 2009;49:1158–65.
Sheldon J, Camino N, Rodes B, Bartholomeusz A, Kuiper M, Tacke F, Nunez M, Mauss S, Lutz T, Klausen G, Locarnini S, Soriano V. Selection of hepatitis B virus polymerase mutations in HIV-coinfected patients treated with tenofovir. Antivir Ther. 2005;10:727–34.
Zhu Y, Curtis M, Borroto-Esoda K. The YMDD and rtA194T mutations result in decreased replication capacity in wild-type HBV as well as in HBV with precore and basal core promoter mutations. Antivir Chem Chemother. 2011;22:13–22.
Qin B, Budeus B, Cao L, Wu C, Wang Y, Zhang X, Rayner S, Hoffmann D, Lu M, Chen X. The amino acid substitutions rtP177G and rtF249A in the reverse transcriptase domain of hepatitis B virus polymerase reduce the susceptibility to tenofovir. Antiviral Res. 2013;97:93–100.
Boyd A, Gozlan J, Maylin S, Delaugerre C, Peytavin G, Girard PM, Zoulim F, Lacombe K. Persistent viremia in human immunodeficiency virus/hepatitis B coinfected patients undergoing long-term tenofovir: virological and clinical implications. Hepatology. 2014;60:497–507.
Childs K, Joshi D, Byrne R, Bruce M, Carey I, Agarwal K, Taylor C. Tenofovir-based combination therapy for HIV/HBV co-infection: factors associated with a partial HBV virological response in patients with undetectable HIV viraemia. AIDS. 2013;27:1443–8.
Matthews GV, Seaberg EC, Avihingsanon A, Bowden S, Dore GJ, Lewin SR, Sasadeusz J, Revill PA, Littlejohn M, Hoy JF, Finlayson R, Ruxrungtham K, Saulynas M, Locarnini S, Thio CL. Patterns and causes of suboptimal response to tenofovir-based therapy in individuals coinfected with HIV and hepatitis B virus. Clin Infect Dis. 2013;56:e87–94.
Corsa AC, Liu Y, Flaherty JF, Marcellin P, Miller M, Kitrinos KM. No detectable resistance to tenofovir disoproxil fumarate (TDF) in HBeAg + and HBeAg- patients with chronic hepatitis B (CHB) after eight years of treatment. 65th Annual Meeting of the American Association for the Study of Liver Diseases. Boston, MA, November 7–11, 2014. Hepatology. 2014;60(Suppl 1):1020A.
Baran B, Soyer OM, Ormeci AC, Gokturk S, Evirgen S, Bozbey HU, Akyuz F, Karaca C, Demir K, Besisik F, Onel D, Gulluoglu M, Badur S, Kaymakoglu S. Efficacy of tenofovir in patients with lamivudine failure is not different from that in nucleoside/nucleotide analogue-naive patients with chronic hepatitis B. Antimicrob Agents Chemother. 2013;57:1790–6.
Fung S, Kwan P, Fabri M, Horban A, Pelemis M, Hann HW, Gurel S, Caruntu FA, Flaherty JF, Massetto B, Dinh P, Corsa A, Subramanian GM, McHutchison JG, Husa P, Gane E. Randomized comparison of tenofovir disoproxil fumarate vs emtricitabine and tenofovir disoproxil fumarate in patients with lamivudine-resistant chronic hepatitis B. Gastroenterology. 2014;146:980–8.
Stockdale AJ, Phillips RO, Beloukas A, Appiah LT, Chadwick D, Bhagani S, Bonnett L, Sarfo FS, Dusheiko G, Geretti AM. Liver fibrosis by transient elastography and virologic outcomes after introduction of tenofovir in lamivudine-experienced adults with HIV and Hepatitis B virus coinfection in Ghana. Clin Infect Dis. 2015;61:883–91.
Patterson SJ, George J, Strasser SI, Lee AU, Sievert W, Nicoll AJ, Desmond PV, Roberts SK, Locarnini S, Bowden S, Angus PW. Tenofovir disoproxil fumarate rescue therapy following failure of both lamivudine and adefovir dipivoxil in chronic hepatitis B. Gut. 2011;60:247–54.
Yang DH, Xie YJ, Zhao NF, Pan HY, Li MW, Huang HJ. Tenofovir disoproxil fumarate is superior to lamivudine plus adefovir in lamivudine-resistant chronic hepatitis B patients. World J Gastroenterol. 2015;21:2746–53.
Svicher V, Cento V, Salpini R, Mercurio F, Fraune M, Beggel B, Han Y, Gori C, Wittkop L, Bertoli A, Micheli V, Gubertini G, Longo R, Romano S, Visca M, Gallinaro V, Marino N, Mazzotta F, De Sanctis GM, Fleury H, Trimoulet P, Angelico M, Cappiello G, Zhang XX, Verheyen J, Ceccherini-Silberstein F, Perno CF. Role of hepatitis B virus genetic barrier in drug-resistance and immune-escape development. Dig Liver Dis. 2011;43:975–83.
Zaaijer HL, Takkenberg RB, Weegink CJ, Rebers SP, Menting S, Reesink HW, Schinkel J, Molenkamp R. Susceptibility of hepatitis B virus to lamivudine restored by resistance to adefovir. J Med Virol. 2009;81:413–6.
EASL—European Association for the Study of Liver. Practice guidelines. 2012. http://www.easl.eu/research/our-contributions/clinical-practice-guidelines. Accessed 20 Aug 2015.
Lazarevic I. Clinical implications of hepatitis B virus mutations: recent advances. World J Gastroenterol. 2014;20:7653–64.
Liaw YF. Impact of YMDD mutations during lamivudine therapy in patients with chronic hepatitis B. Antivir Chem Chemother. 2001;12 Suppl 1:67–71.
Lok AS, Lai CL, Leung N, Yao GB, Cui ZY, Schiff ER, Dienstag JL, Heathcote EJ, Little NR, Griffiths DA, Gardner SD, Castiglia M. Long-term safety of lamivudine treatment in patients with chronic hepatitis B. Gastroenterology. 2003;125:1714–22.
Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, Chang TT, Kitis G, Rizzetto M, Marcellin P, Lik SG, Goodman Z, Ma J, Brosgart CL, Eorroto-Esoda K, Arterburn S, Chuck SL. Long-term therapy with adefovir dipivoxil for HBeAg-negative chronic hepatitis B for up to 5 years. Gastroenterology. 2006;131:1743–51.
Lee HW, Kwon JC, Oh IS, Chang HY, Cha YJ, Choi IS, Kim HJ. Prolonged entecavir therapy is not effective for HBeAg seroconversion in treatment-naive chronic hepatitis B patients with a partial virological response. Antimicrob Agents Chemother. 2015;9:5348–56.
Ijaz S, Arnold C, Dervisevic S, Mechurova J, Tatman N, Tedder RS, Naoumov NV. Dynamics of lamivudine-resistant hepatitis B virus during adefovir monotherapy versus lamivudine plus adefovir combination therapy. J Med Virol. 2008;80:1160–70.
Kurashige N, Hiramatsu N, Ohkawa K, Yakushijin T, Kiso S, Kanto T, Takehara T, Kasahara A, Doi Y, Yamada A, Oshita M, Mita E, Hagiwara H, Nagase T, Yoshihara H, Hayashi E, Imai Y, Kato M, Kashihara T, Hayashi N. Factors contributing to antiviral effect of adefovir dipivoxil therapy added to ongoing lamivudine treatment in patients with lamivudine-resistant chronic hepatitis B. J Gastroenterol. 2009;44:601–7.
Sung JJ, Lai JY, Zeuzem S, Chow WC, Heathcote EJ, Perrillo RP, Brosgart CL, Woessner MA, Scott SA, Gray DF, Gardner SD. Lamivudine compared with lamivudine and adefovir dipivoxil for the treatment of HBeAg-positive chronic hepatitis B. J Hepatol. 2008;48:728–35.
Vassiliadis TG, Giouleme O, Koumerkeridis G, Koumaras H, Tziomalos K, Patsiaoura K, Grammatikos N, Mpoumponaris A, Gkisakis D, Theodoropoulos K, Panderi A, Katsinelos P, Eugenidis N. Adefovir plus lamivudine are more effective than adefovir alone in lamivudine-resistant HBeAg- chronic hepatitis B patients: a 4-year study. J Gastroenterol Hepatol. 2010;25:54–60.
Yuen MF, Lai CL. Treatment of chronic hepatitis B: evolution over two decades. J Gastroenterol Hepatol. 2011;26 Suppl 1:138–43.
Gomes-Gouvea MS, Ferreira AC, Teixeira R, Andrade JR, Ferreira AS, Barros LM, Rezende RE, Nastri AC, Leite AG, Piccoli LZ, Galvan J, Conde SR, Soares MC, Kliemann DA, Bertolini DA, Kunyoshi AS, Lyra AC, Oikawa MK, de Araujo LV, Carrilho FJ, Mendes-Correa MC, Pinho JR. HBV carrying drug-resistance mutations in chronically infected treatment-naive patients. Antivir Ther. 2015;20:387–95.
Vutien P, Trinh HN, Garcia RT, Nguyen HA, Levitt BS, Nguyen K, da Silveira E, Daugherty T, Ahmed A, Garcia G, Lutchman GA, Nguyen MH. Mutations in HBV DNA polymerase associated with nucleos(t)ide resistance are rare in treatment-naive patients. Clin Gastroenterol Hepatol. 2014;12:1363–70.
Bayliss J, Nguyen T, Lesmana CRA, Bowden S, Revill P. Advances in the molecular diagnosis of hepatitis B infection: providing insight into the next generation of disease. Semin Liver Dis. 2013;33:113–21.
Geretti AM, Paredes R, Kozal MJ. Transmission of HIV drug resistance: lessons from sensitive screening assays. Curr Opin Infect Dis. 2015;28:23–30.
Beloukas A, King S, Childs K, Papadimitropoulos A, Hopkins M, Atkins M, Agarwal K, Nelson M, Geretti A. Detection of the NS3 Q80K polymorphism by Sanger and deep sequencing in hepatitis C virus (HCV) genotype 1a strains in the United Kingdom. Clin Microbiol Infect. 2015;21(11):1033–9.
Gianella S, Delport W, Pacold ME, Young JA, Choi JY, Little SJ, Richman DD, Kosakovsky Pond SL, Smith DM. Detection of minority resistance during early HIV-1 infection: natural variation and spurious detection rather than transmission and evolution of multiple viral variants. J Virol. 2011;85:8359–67.
Zoulim F. In vitro models for studying hepatitis B virus drug resistance. Semin Liver Dis. 2006;26:171–80.
Ntziora F, Paraskevis D, Haida C, Manesis E, Papatheodoridis G, Manolakopoulos S, Elefsiniotis I, Karamitros T, Vassilakis A, Hatzakis A. Ultrasensitive amplification refractory mutation system real-time PCR (ARMS RT-PCR) assay for detection of minority hepatitis B virus-resistant strains in the era of personalized medicine. J Clin Microbiol. 2013;51:2893–900.
Chen CJ, Iloeje UH, Yang HI. Long-term outcomes in hepatitis B: the REVEAL-HBV study. Clin Liver Dis. 2007;11:797–816.
Hosaka T, Suzuki F, Kobayashi M, Seko Y, Kawamura Y, Sezaki H, Akuta N, Suzuki Y, Saitoh S, Arase Y, Ikeda K, Kobayashi M, Kumada H. Long-term entecavir treatment reduces hepatocellular carcinoma incidence in patients with hepatitis B virus infection. Hepatology. 2013;58:98–107.
Lai CL, Yuen MF. Prevention of hepatitis B virus-related hepatocellular carcinoma with antiviral therapy. Hepatology. 2013;57:399–408.
Seto WK, Liu K, Wong DK, Fung J, Huang FY, Hung IF, Lai CL, Yuen MF. Patterns of hepatitis B surface antigen decline and HBV DNA suppression in Asian treatment-experienced chronic hepatitis B patients after three years of tenofovir treatment. J Hepatol. 2013;59:709–16.
Pawlotsky JM, Dusheiko G, Hatzakis A, Lau D, Lau G, Liang TJ, Locarnini S, Martin P, Richman DD, Zoulim F. Virologic monitoring of hepatitis B virus therapy in clinical trials and practice: recommendations for a standardized approach. Gastroenterology. 2008;134:405–15.
Heathcote EJ, Marcellin P, Buti M, Gane E, De Man RA, Krastev Z, Germanidis G, Lee SS, Flisiak R, Kaita K, Manns M, Kotzev I, Tchernev K, Buggisch P, Weilert F, Kurdas OO, Shiffman ML, Trinh H, Gurel S, Snow-Lampart A, Borroto-Esoda K, Mondou E, Anderson J, Sorbel J, Rousseau F. Three-year efficacy and safety of tenofovir disoproxil fumarate treatment for chronic hepatitis B. Gastroenterology. 2011;140:132–43.
Ono A, Suzuki F, Kawamura Y, Sezaki H, Hosaka T, Akuta N, Kobayashi M, Suzuki Y, Saitou S, Arase Y, Ikeda K, Kobayashi M, Watahiki S, Mineta R, Kumada H. Long-term continuous entecavir therapy in nucleos(t)ide-naïve chronic hepatitis B patients. J Hepatol. 2012;57:508–14.
Yuen MF, Seto WK, Fung J, Wong DK, Yuen JC, Lai CL. Three years of continuous entecavir therapy in treatment-naïve chronic hepatitis B patients: VIRAL suppression, viral resistance, and clinical safety. Am J Gastroenterol. 2011;106:1264–71.
Yang YJ, Shim JH, Kim KM, Lim YS, Lee HC. Assessment of current criteria for primary nonresponse in chronic hepatitis B patients receiving entecavir therapy. Hepatology. 2014;59:1303–10.
Zoutendijk R, Reijnders JG, Brown A, Zoulim F, Mutimer D, Deterding K, Petersen J, Hofmann WP, Buti M, Santantonio T, van Bömmel F, Pradat P, Oo Y, Luetgehetmann M, Berg T, Hansen BE, Wedemeyer H, Janssen HL. Entecavir treatment for chronic hepatitis B: adaptation is not needed for the majority of naïve patients with a partial virological response. Hepatology. 2011;54:443–51.
Ha NB, Ha NB, Trinh HN, Nguyen HA, Nguyen KK, Nguyen MH. Response to higher dose of entecavir 1.0 mg daily in patients with partial response to entecavir 0.5 mg daily. J Clin Gastroenterol. 2013;47:461–5.
Lu L, Yip B, Trinh H, Pan CQ, Han SH, Wong CC, Li J, Chan S, Krishnan G, Wong CC, Nguyen MH. Tenofovir-based alternate therapies for chronic hepatitis B patients with partial virological response to entecavir. J Viral Hepat. 2015;22:675–81.
Ratcliffe L, Beadsworth MB, Pennell A, Phillips M, Vilar FJ. Managing hepatitis B/HIV co-infected: adding entecavir to truvada (tenofovir disoproxil/emtricitabine) experienced patients. AIDS. 2011;25:1051–6.
AASLD—American Association for the Study of Liver Disease. Practice guidelines. 2009. http://www.aasld.org/publications/practice-guidelines-0. Accessed 30 Aug 2015.
Pol S, Lampertico P. First-line treatment of chronic hepatitis B with entecavir or tenofovir in ‘real-life’ settings: from clinical trials to clinical practice. J Viral Hepat. 2012;19:377–86.
Ke W, Liu L, Zhang C, Ye X, Gao Y, Zhou S, Yang Y. Comparison of efficacy and safety of tenofovir and entecavir in chronic hepatitis B virus infection: a systematic review and meta-analysis. PLoS One. 2014;9:e98865.
Gordon SC, Krastev Z, Horban A, Petersen J, Sperl J, Dinh P, Martins EB, Yee LJ, Flaherty JF, Kitrinos KM, Rustgi VK, Marcellin P. Efficacy of tenofovir disoproxil fumarate at 240 weeks in patients with chronic hepatitis B with high baseline viral load. Hepatology. 2013;58:505–13.
Chan HL, Chan CK, Hui AJ, Chan S, Poordad F, Chang TT, Mathurin P, Flaherty JF, Lin L, Corsa A, Gaggar A, Subramanian GM, McHutchison JG, Lau G, Lee S, Gane EJ. Effects of tenofovir disoproxil fumarate in hepatitis B e antigen-positive patients with normal levels of alanine aminotransferase and high levels of hepatitis B virus DNA. Gastroenterology. 2014;146:1240–8.
Lok AS, Trinh H, Carosi G, Akarca US, Gadano A, Habersetzer F, Sievert W, Wong D, Lovegren M, Cohen D, Llamoso C. Efficacy of entecavir with or without tenofovir disoproxil fumarate for nucleos(t)ide-naïve patients with chronic hepatitis B. Gastroenterology. 2012;143:619–28.
Lui YY, Tsoi KK, Wong VW, Kao JH, Hou JL, Teo EK, Mohamed R, Piratvisuth T, Han KH, Mihm U, Wong GL, Chan HL. Cost-effectiveness analysis of roadmap models in chronic hepatitis B using tenofovir as the rescue therapy. Antivir Ther. 2010;15:145–55.
Soriano V, McMahon B. Strategic use of lamivudine in the management of chronic hepatitis B. Antiviral Res. 2013;100:435–8.
Hermans L, Svicher V, Diepstraten Pas S, Salpini R, Alvarez M, Ben Ari Z, Boland G, Bruzzone B, Coppola N, Seguin-Devaux C, Dyda T, Garcia F, Kaiser R, Köse S, Krarup H, Lazarevic I, Lunar M, Maylin S, Micheli V, Mor O, Paraschiv S, Paraskevis D, Poljak M, Puchhammer-Stöckl E, Simon F, Stanojevic M, Stene-Johansen K, Tihic N, Trimoulet P, Verheyen J, Vince A, Weis N, Yalcinkaya T, Zidovec Lepej S, Perno C, Boucher C, Wensing AMJ. Combined analysis of the prevalence of drug-resistant hepatitis B virus in antiviral therapy-experienced patients in Europe. J Infect Dis. 2016;213(1):39–48.
Stockdale AJ, Geretti AM. Chronic hepatitis B infection in sub-Saharan Africa: a grave challenge and a great hope. Trans R Soc Trop Med Hyg. 2015;109:421–2.
Di Marco V, Marzano A, Lampertico P, Andreone P, Santantonio T, Almasio PL, Rizzetto M, Craxi A. Clinical outcome of HBeAg-negative chronic hepatitis B in relation to virological response to lamivudine. Hepatology. 2004;40:883–91.
Hadziyannis SJ, Papatheodoridis GV, Dimou E, Laras A, Papaioannou C. Efficacy of long-term lamivudine monotherapy in patients with hepatitis B e antigen-negative chronic hepatitis B. Hepatology. 2000;32:847–51.
Liaw YF, Chien RN, Yeh CT, Tsai SL, Chu CM. Acute exacerbation and hepatitis B virus clearance after emergence of YMDD motif mutation during lamivudine therapy. Hepatology. 1999;30:567–72.
Papatheodoridis GV, Dimou E, Laras A, Papadimitropoulos V, Hadziyannis SJ. Course of virologic breakthroughs under long-term lamivudine in HBeAg-negative precore mutant HBV liver disease. Hepatology. 2002;36:219–26.
Rizzetto M, Tassopoulos NC, Goldin RD, Esteban R, Santantonio T, Heathcote EJ, Lagget M, Taak NK, Woessner MA, Gardner SD. Extended lamivudine treatment in patients with HBeAg-negative chronic hepatitis B. J Hepatol. 2005;42:173–9.
Liaw YF, Sung JJ, Chow WC, Farrell G, Lee CZ, Yuen H, Tanwandee T, Tao QM, Shue K, Keene ON, Dixon JS, Gray DF, Sabbat J. Lamivudine for patients with chronic hepatitis B and advanced liver disease. N Engl J Med. 2004;351:1521–31.
Bartholomeusz A, Locarnini SA. Antiviral drug resistance: clinical consequences and molecular aspects. Semin Liver Dis. 2006;26:162–70.
Van Bömmel F, de Man RA, Wedemeyer H, Deterding K, Petersen J, Buggisch P, Erhardt A, Hüppe D, Stein K, Trojan J, Sarrazin C, Böcher WO, Spengler U, Wasmuth HE, Reinders JG, Möller B, Rhode P, Feucht HH, Wiedenmann B, Berg T. Long-term efficacy of tenofovir monotherapy for hepatitis B virus monoinfected patients after failure of nucleoside/nucleotide analogues. Hepatology. 2010;51:73–80.
Tan J, Degertekin B, Wong SN, Husain M, Oberhelman K, Lok AS. Tenofovir monotherapy is effective in hepatitis B patients with antiviral treatment failure to adefovir in the absence of adefovir-resistant mutations. J Hepatol. 2008;48:391–8.
Nguyen NH, Trinh HN, Nguyen TT, Do ST, Tran P, Nguyen HA, Nguyen KK, Garcia RT, Lutchman GA, Nguyen MH. Safety and efficacy of entecavir in adefovir-experienced patients. J Gastroenterol Hepatol. 2015;30:43–50.
Lee YB, Lee JH, Lee DH, Cho H, Ahn H, Choi WM, Cho YY, Lee M, Yoo JJ, Cho Y, Cho EJ, Yu SJ, Kim YJ, Yoon JH, Kim CY, Lee HS. Efficacy of entecavir-tenofovir combination therapy for chronic hepatitis B patients with multidrug-resistant strains. Antimicrob Agents Chemother. 2014;58:6710–6.
Lim YS, Yoo BC, Byun KS, Kwon SY, Kim YJ, An J, Lee HC, Lee YS. Tenofovir monotherapy versus tenofovir and entecavir combination therapy in adefovir-resistant chronic hepatitis B patients with multiple drug failure: results of a randomised trial. Gut. 2016;65(6):1042–51.
Lim YS, Byun KS, Yoo BC, Kwon SY, Kim YJ, An J, Lee HC, Lee YS. Tenofovir monotherapy versus tenofovir and entecavir combination therapy in patients with entecavir-resistant chronic hepatitis B with multiple drug failure: results of a randomised trial. Gut. 2016;65(5):852–60.
Yuen MF, Ahn SH, Lee KS, Um SH, Cho M, Yoon SK, Lee JW, Park NH, Kweon YO, Sohn JH, Lee J, Kim JA, Lai CL, Han KH. Two-year treatment outcome of chronic hepatitis B infection treated with besifovir vs. entecavir: results from a multicentre study. J Hepatol. 2015;62:526–32.
Takamatsu Y, Tanaka Y, Kohgo S, Murakami S, Singh K, Das D, Venzon DJ, Amano M, Kuwata N, Aoki M, Delino NS, Hayashi S, Takahashi S, Sukenaga Y, Haraguchi K, Sarafianos SG, Maeda K, Mitsuya H. 4′-modified nucleoside analogs: potent inhibitors active against entecavir-resistant hepatitis B virus. Hepatology. 2015;62(4):1024–36.
Matthews PC, Geretti AM, Goulder PJ, Klenerman P. Epidemiology and impact of HIV coinfection with hepatitis B and hepatitis C viruses in Sub-Saharan Africa. J Clin Virol. 2014;61:20–33.
WHO—World Health Organisation. Guidelines for the prevention, care and treatment of persons with chronic hepatitis B infection. 2015. http://www.who.int/hiv/pub/hepatitis/hepatitis-b-guidelines/en/. Accessed 30 Aug 2015.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Beloukas, A., Geretti, A.M. (2017). Hepatitis B Virus Drug Resistance. In: Mayers, D., Sobel, J., Ouellette, M., Kaye, K., Marchaim, D. (eds) Antimicrobial Drug Resistance. Springer, Cham. https://doi.org/10.1007/978-3-319-47266-9_26
Download citation
DOI: https://doi.org/10.1007/978-3-319-47266-9_26
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-47264-5
Online ISBN: 978-3-319-47266-9
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)