
Abstract
The hypothalamic-pituitary-testicular axis is activated in the third trimester of intrauterine life and during the neonatal period. Fetus testes differentiate by the end of the fifth embryonic week, before the gonadotrophs are functionally active. Therefore, GnRH deficiency does not affect male sexual differentiation.
The 46,XY disorders of sex development (DSD) are characterized by atypical or female external genitalia, caused by incomplete intrauterine masculinization, in the presence or absence of Müllerian structures. 46,XY DSD result from decreased production of testosterone, decreased conversion of testosterone into dihydrotestosterone, or from impairment of their peripheral action. Under histological analysis, testicular tissue in patients with 46,XY DSD can be absent, partially or completely dysgenetic, or almost normal. Taking in account testosterone levels, the etiology of the 46,XY DSD can be classified into two large groups: low testosterone secretion and normal or high testosterone secretion.
Most patients with DSD present with atypical genitalia and their sex assignment may be a complex procedure. The choice of male sex−of rearing in 46,XY babies with atypical genitalia is a challenging situation. The participation of a multidisciplinary team is essential during this process and the immediate identification of a molecular defect causing the disorder might aid in this decision.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Pulsatile secretion of GnRH by neurons of the medium basal hypothalamus region is a crucial element of the reproductive cascade. GnRH binds to its receptor (GnRHR) on the gonadotrophs surface initiating the synthesis release of pituitary gonadotropins. In turn, luteinizing hormone (LH ) and follicle-stimulating hormone (FSH) stimulate testicular hormone secretion that induces pubertal development and gametogenesis [1]. Normal testicular physiology results from the integrated function of the tubular and interstitial compartments.
Fetus testes are differentiated by the end of the fifth embryonic week, before the gonadotrophs are functionally active. The hypothalamic-pituitary-testicular axis is activated in the third trimester of intrauterine life and during the neonatal period. However, GnRH deficiency does not affect male sexual differentiation that occurs in the first trimester of pregnancy because in this phase, the Leydig cell function is regulated by the placental chorionic gonadotropin (hCG). Conversely, during the second half of gestation, fetal LH and FSH become major regulators of testicular physiology [2]. FSH stimulates Sertoli cell proliferation , inhibin B and the anti-Müllerian hormone (AMH) secretion responsible for the regression of the Müllerian ducts during embryonic development. Fetal LH stimulates the production of androgens and insulin-like factor 3 (INSL3) through Leydig cells, leading to penile and scrotum growth and testicular descent [3]. Toward term, a decline in pituitary and testicular hormones is observed. These physiological events explain the occurrence of micropenis and cryptorchidism and lack of genital ambiguity in male newborns with congenital hypogonadotropic hypogonadism.
After birth, gonadotropins, testosterone, and AMH levels are transiently low, then increase and remain high for 3–6 months. Thereafter, gonadotropin levels decrease, resulting in a fall of testicular testosterone secretion to low or undetectable levels during infancy and childhood. Sertoli cells continue to be active, producing AMH and inhibin B during infancy and childhood [3].
Control of Male Gonadotropic Axis Function
GnRH Secretion
Although the hypothalamic secretion of GnRH has been considered the key component in controlling the male hypothalamic-pituitary-testicular axis, a number of other important components in the GnRH neuronal network have been identified. Stimulatory (kisspeptin) and inhibitory (MKRN3) pathways have been described in controlling the GnRH secretion [4, 5].
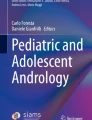
The discovery of the crucial role of kisspeptin in human puberty completely changed the knowledge of the neuroendocrine regulation of human reproduction [6, 7]. Kisspeptin is a modulator that acts upstream of GnRH and is sensitive to sex steroid feedback. This peptide is now recognized as a critical regulator of the onset of puberty, sex hormone-mediated secretion of gonadotropins, and fertility [8]. Kisspeptin is a potent stimulator of the hypothalamic-pituitary-gonadal axis and acts directly with GnRH neurons through its receptor, KISS1R (GPR54) to release GnRH into portal circulation, which in turn stimulates the secretion of LH and FSH (Fig. 3.1). The same neuronal network co-secretes Kisspeptin, neuroKinin B, and dynorphin, a opioid inhibitor. Neurokinin B, via the neurokinin B receptor, stimulates the pulsatile Kisspeptin secretion, whereas dynorphin, acting in its kappa opioid peptide receptor, inhibits kisspeptin secretion [9].

Hormonal control of Male Gonadotropic axis. T = Testosterone; E2 = Estradiol; DHT = Dihydrotestosterone
LH Secretion
It is well known that testosterone, estradiol, and dihydrotestosterone inhibit LH secretion [10] (Fig. 3.1). Santen and Bardin [11] demonstrated that testosterone acts at the hypothalamic level by decreasing GnRH pulse frequency without a change in pulse amplitude in portal blood. However, the action of estradiol appears to be predominantly at the pituitary where it decreases LH pulse amplitude without changing pulse frequency. Additionally, these studies demonstrated that treatment with estradiol lowered LH levels by decreasing LH pulse amplitude without altering GnRH secretory patterns in portal blood [12]. However, administration of anastrozole, a selective aromatase inhibitor, in males caused an increase in LH pulse amplitude and pulse frequency. The authors also found increased testosterone concentrations accompanied by an increase in FSH levels. The investigators concluded that estradiol exerted a negative feedback by acting at the hypothalamus decreasing GnRH pulse frequency and at the pituitary, thereby decreasing the responsiveness to GnRH [13].
It has been shown more recently that Kisspeptin also stimulates the secretion of both LH and FSH in humans. While kisspeptin stimulates LH release 2- to 3-fold in most circumstances, the stimulatory effect on FSH levels is much lower and is less consistent [14]. This differential effect of Kisspeptin on LH and FSH secretion is concordant with studies in rodents [15, 16]. The capacity of kisspeptin to enhance LH pulsatility has also been demonstrated in human reproductive disorders, including male hypogonadism associated with type 2 diabetes [14] and in hypogonadism as a result of neurokinin B signaling defects [17].
FSH Secretion
It is well known that testosterone and estradiol are capable of suppressing FSH levels in males [18]. However, inhibin, a glycoprotein hormone, exerts a specific negative feedback inhibition on FSH secretion at the pituitary level [19]. Two forms of inhibin have been isolated, inhibin A and inhibin B [20]. Both inhibins have the capacity to specifically inhibit FSH secretion through pituitary cells in culture. In contrast, the dimers of the β subunit, termed activins through pituitary cells in culture [21, 22] (Fig. 3.1). Activin, inhibin, and AMH belong to the transforming growth factor (TGF)-β protein superfamily.
Finally, a protein called follistatin has the capability to suppress FSH secretion specifically via pituitary cells in culture [23]. This action is a result of the capability of follistatin to bind and neutralize the actions of activin [24].
The inhibin is produced by the Sertoli cell and the predominant form of inhibin secreted by the testis is inhibin B [25]. The levels of inhibin B in males are inversely related to the levels of FSH [26]. It has been demonstrated that FSH predominantly stimulates inhibin α-subunit production and does not alter the β-subunit message [27]. Corroborating this, a clear increase in these glycoproteins under the stimulation of elevated FSH levels has been shown [28].
In men, testosterone at amounts equivalent to or greater than its production rate can suppress both FSH and LH [10], with greater suppression of LH secretion in contrast to the actions of inhibin [18]. The observation of an increase in FSH levels in men treated with a selective aromatase inhibitor raised the possibility that estradiol exerts a negative feedback action on FSH particularly because the treated men experienced a concomitant significant increase in testosterone [13].
There is evidence to suggest that the Sertoli cells, Leydig cells, and peritubular myoid cells can produce activin that exerts local actions within the testis such as the stimulation of spermatogonial mitosis [29]. Moreover, activin A is responsible for the stimulation of Sertoli cell mitosis during the development of the testis in both rats and mice [30, 31]. Additionally, receptors for activin are present on primary spermatocytes, round spermatids, and Sertoli cells [32]. However, our knowledge on activin functions in the male gonadotrophic axis is still emerging.
Follistatin is also produced by the Sertoli cells, spermatogonia, primary spermatocytes and round spermatids in the testis [33]. However, castration does not result in a clear decrease in follistatin levels in the circulation, suggesting that the testis does not contribute significantly to the circulating levels of follistatin [34].
The absence of changes in activin and follistatin levels, whereas the inhibin levels in the circulation decreased to undetectable levels after castration, strongly suggest that the gonadal feedback signal on FSH secretion is inhibin. Furthermore, in several species the infusion or injection of recombinant human inhibin caused a specific fall in FSH secretion 6 h following its administration [35]. Additionally, normal levels of inhibin A in castrate rams, suppressed FSH levels into the normal range in the absence of testosterone [36].
There is substantial evidence that activin and follistatin can exert a paracrine role directly in the pituitary gland. It is therefore likely that the actions of inhibin are predominantly exerted through secretion from the testis and transport via the peripheral circulation whereas the actions of activins and follistatin on FSH secretion occur through paracrine actions at the level of the pituitary gland. Further evidence supporting the stimulation of FSH by activin secretion emerges from the decline in FSH levels in mice with targeted disruption of the activin type II receptor gene [37].
The increase of gonadotropin pulse amplitude and frequency drives pubertal development of the testis. The FSH induces a new Sertoli cell proliferation and the LH re-stimulates the maturation of Leydig cells. The increase of testosterone concentration into the testis incites the maturation of Sertoli cell [38] and down-regulation of AMH levels [39]. It is noteworthy that intratesticular testosterone levels regulate spermatogenesis. Indeed, the administration of exogenous testosterone results in elevated serum testosterone levels, but without reaching intratesticular testosterone concentration to induce spermatogenesis. Moreover, testosterone levels associated with an adequate expression of the androgen receptor in Sertoli cells are necessary for meiosis [40]. Young et al. demonstrated that mean serum AMH levels in men with untreated hypogonadotropic hypogonadism, were significantly higher than in normal men and were similar to those previously reported in prepubertal boys. The hCG treatment in these patients induced an increase of plasma T associated with a dramatic decrease of AMH serum. The similar increase in plasma T levels was obtained in those patients treated with exogenous T, but a lesser decrease of AMH serum. These data suggest that intratesticular testosterone concentration can be estimated by measuring AMH serum [41].
Inhibin B secretion during puberty is regulated by FSH and germ cells [42]. Adult levels of inhibin B are achieved in coincidence with the increase in LH serum and intratesticular testosterone levels.
46,XY Disorders of Sex Development
The term disorders of sex development (DSD ) comprises congenital conditions in which development of chromosomal, gonadal, or anatomic sex is atypical. The 46,XY DSD are characterized by atypical or female external genitalia, caused by incomplete intrauterine masculinization , in the presence or absence of Müllerian structures. Complete absence of virilization results in normal female external genitalia and these patients generally seek medical attention at the pubertal age, because of the absence of breast development and/or primary amenorrhea [43].
Male phenotypic development can be viewed as a two-step process: (1) testis formation from the primitive gonad (sex determination) and (2) internal and external genitalia differentiation resulting from factors secreted by the testis (sex differentiation) [43, 44].
At the start of gestation, embryos of the two sexes differ only by their karyotypes. Specific genes lead to the determination of the bipotential gonad into a testis or an ovary. In turn, the hormonal production of the fetal gonad induces the anatomic and possibly psychological differences, leading to various behaviors that are ultimately influenced by the social environment. This pool of factors will determine the individual sex.
At 6–7 weeks of gestation, the paramesonephric duct (Müllerian duct) develops next to the mesonephric duct (Wolffian duct). If a testis develops, AMH , a glycoprotein secreted by the Sertoli cells, acts on its receptor in the Müllerian ducts to cause their regression. Testosterone secreted by the testicular Leydig cells acts with the androgen receptor in the Wolffian ducts to induce the formation of epidydimis, deferent ducts, and seminal vesicles. Testosterone is further reduced to dihydrotestosterone (DHT), which acts with the androgen receptor of the prostate and external genitalia to cause its masculinization. If the testes do not develop normally, and hormones are absent or insufficient, the mesonephric duct does not grow and eventually degenerates, whereas the paramesonephric duct proliferates and the fallopian tube, uterus, and upper third of the vagina develop [45].
Testosterone mediates three main functions in the male physiology : regulation of the LH secretion from the anterior pituitary, virilization of the Wolffian ducts in the male embryo, and regulation of spermatogenesis. The other androgen action during embryogenesis and intrauterine life is mediated by DHT [46]. Testosterone and DHT act via a single androgen receptor, and DHT binds more tightly to the hormone-binding domain of the receptor as a result of a decreased rate of dissociation of the DHT-receptor complex; the consequence of similar association rates but different dissociation rates is that in the steady state, DHT occupies most receptor sites, even when testosterone is the predominant steroid in the cell [47].
Testosterone is the principal androgen synthesized by both fetal and mature testes. Testosterone secretion begins just prior to the onset of virilization of the male embryo and promotes the conversion of the Wolffian ducts into the eipidiymides, vasa deferentia, seminal vesicles, and ejaculatory ducts. DHT, in turn, causes development of the prostate in the urogenital sinus, midline fusion, elongation, and enlargement of the urogenital tubercle and the urogenital folds, eventuating in the development of the scrotum and phallus [46].
46,XY DSD result from decreased production of testosterone, decreased conversion of testosterone into DHT, or from impairment of their peripheral action. At histological analysis, testicular tissue in patients with 46,XY DSD can be absent, partially or completely dysgenetic, or almost normal [45].
Taking into account testosterone levels, the etiology of the 46,XY DSD can be classified into two large groups:
-
1.
Low testosterone secretion
-
(a)
Defects in the formation of the testes
-
(b)
Enzymatic defects in testosterone synthesis
-
(a)
-
2.
Normal or high testosterone secretion
-
(a)
Defects in the conversion of testosterone in DHT
-
5α reductase 2 deficiency
-
-
(b)
Defects in testosterone action
-
Androgen receptor defects
-
-
(a)
46,XY DSD due to Low Testosterone Secretion
Defects in Formation of the Testes
46,XY Gonadal Dysgenesis
46,XY gonadal dysgenesis includes a variety of clinical conditions in which the fetal testes development is abnormal. This group encompasses both complete and a partial forms, embryonic testicular regression syndrome, and testicular agenesis. The complete form is characterized by female external and internal genitalia, lack of secondary sexual characteristics, normal or tall stature without somatic stigmata of Turner syndrome, and the presence of bilateral dysgenetic gonads . On the other hand, the partial form of this syndrome is characterized by impaired testicular development which results in patients with ambiguous external genitalia with or without Müllerian structures [43].
46,XY gonadal dysgenesis is a genetic heterogeneous disorder associated with alterations in a number of genes involved in the male gonad development. SRY and NR5A1/SF1 mutations are the most frequent cause of non syndromic 46,XY gonadal dysgenesis [48]. Considering that molecular diagnosis is established in just 20 % of patients with DSD, aCGH or whole-exome or -genome sequencing evaluation may enable molecular diagnosis involving known genes and novel candidate genes for 46,XY gonadal dysgenesis [45].
Table 3.1 summarizes the genes that determine abnormalities in testis development and may or may not be associated with other syndromic signs.
The dysgenetic testes showed disorganized seminiferous tubules and ovarian stroma with occasional primitive sex cords devoid of germ cells; primordial follicles are sometimes observed in the streak gonad in the first years of life [49].
The laboratorial diagnosis is based on the 46,XY karyotype and high levels of LH and FSH with a predominance of FSH. Basal testosterone levels are within pre-pubertal range and fail to increase after hCG stimulation.
Defects of Testosterone Production
LH/hCG Insensibility : Leydig Cell Hypoplasia
Leydig cell hypoplasia is an autosomal recessive disorder. The inability of Leydig cells to secrete testosterone in 46,XY DSD results in failure of intrauterine and pubertal virilization. Both hCG and LH act by stimulating a common G-protein coupled receptor (LHCGR) and mutations in this gene cause Leydig cell hypoplasia. Patients affected with the complete form have female external genitalia leading to female sex assignment, absence of sexual characteristics at puberty, primary amenorrhea undescended testes slightly smaller than normal with relatively preserved seminiferous tubules and absence of mature Leydig cells, presence of rudimentary epididymis and vas deferens and absence of uterus and fallopian tubes, low testosterone levels despite elevated gonadotrophin levels, with LH levels predominant over FSH levels, testicular unresponsiveness to hCG stimulation, and no abnormal step up in testosterone biosynthesis precursors [50, 51]. Several different mutations in the LH receptor gene were reported in these patients [43, 50, 51].
In contrast to the homogenous phenotype of the complete form of Leydig cell hypoplasia, the partial formof Leydig cell hypoplasia has a broad spectrum [50–53]. Most patients have predominantly male external genitalia with a micropenis and/or hypospadias. Testes are cryptorchidic or topic. During puberty, partial virilization occurs and testicular size is normal or only slightly reduced, while penile growth is significantly impaired. Testosterone response to the hCG test is subnormal without accumulation of testosterone precursors. After puberty, LH levels are elevated and testosterone levels are intermediate between those of children and normal males [43].
46,XY DSD Due to Cholesterol Synthesis Defects
Smith-Lemli-Opitz is a rare syndrome caused by a deficiency of 7-dehydrocholesterol reductase [54]. The first step of testosterone biosynthesis begins with the uptake of cholesterol from the extracellular space and/or the endogenous synthesis of cholesterol by Leydig cells. In both instances, the action of 7-dehydrosterolreductase is necessary for cholesterol synthesis from 7-dehydrocholesterol. The SLOS phenotypic spectrum is broad and variable—from early embryonic non-viability to varying levels of severity postnatally including distinctive facial appearance; growth and mental retardation; autistic behavior; hypotonia; failure to feed; decreased life span; and variable structural anomalies of the heart, lungs, brain, gastrointestinal tract, limbs, genitalia, and kidneys.
Enzymatic Defects in Testosterone Synthesis
Five enzymatic defects that alter the normal synthesis of testosterone from cholesterol have been described (Fig. 3.2). Three of thos defects are associated with defects in cortisol synthesis leading to congenital adrenal hyperplasia associated with 46,XY DSD. All of them are rare and present an autosomal recessive mode of inheritance.

Main biosynthesis pathways of adrenal and gonadal steroids
Congenital adrenal hyperplasia (CAH) is associated with hypoadrenocorticism or a mixture of hypo-and hyper-corticoadrenal steroid secretion. Synthesis of cortisol only or both gluco- and mineralocorticoids is impaired leading to a compensatory increase in adrenocorticotrophic hormone (ACTH) and in renin–angiotensin production. These compensatory mechanisms may return cortisol or aldosterone production to normal or near normal levels, but with an excessive production of other steroids causing undesirable hormonal effects. Defects in P45011A enzyme, also called P450scc, steroidogenic acute regulatory (StAR) protein, 3β-hydroxysteroid dehydrogenase (3β-HSD) type II, and 17α-hydroxylase cause congenital adrenal hyperplasia in patients with 46,XY [43].
P45011A and StAR protein catalyze the first step in conversion of cholesterol to hormonal steroids known as cholesterol side-chain cleavage to form pregnenolone. This is the most severe form of CAH associated with 46,XY DSD. Affected subjects are, in general, phenotypic females or sometimes present slightly virilized external genitalia with or without cryptorchidism, underdeveloped internal male organs, and an enlarged adrenal cortex, engorged with cholesterol and cholesterol esters. Adrenal steroidogenesis deficiency, when untreated, leads to salt wasting crisis, hyponatraemia, hyperkalaemia, hypovolaemia, acidosis, and death in infancy [55].
The following step in testosterone biosynthesis is the conversion of dehydroepiandrosterone (DHEA) in androstenedione by 3β-HSD type II (Fig. 3.2). Male patients with 3β-HSD type II deficiency present with atypical external genitalia, characterized by microphallus, perineal hypospadias, bifid scrotum, and a blind vaginal pouch. Defects with severe impact in enzymatic activity are associated with salt loss. Gynaecomastia is common during the pubertal stage. Male subjects with 46,XY DSD as a result of 3β-HSD type II deficiency without salt wasting showed clinical features in common with the deficiencies of 17β-HSD 3 and 5α-reductase 2 [43].
The next step in the biosynthesis is conversion of pregnenolone into 17α-hydroxypregnenolone and further down into DHEA by P450c17 (Fig. 3.2). The classical phenotype of 17α-hydroxylase deficiency in male patients described is a female-like or slightly virilized external genitalia with blind vaginal pouch, cryptorchidism, and high blood pressure usually associated with hypokalaemia. Differently from other forms of CAH , these patients do not present signs of glucocorticoid insufficiency resulting from elevated levels of corticosterone, which has a glucocorticoid effect [43].
Treatment of patients with these different forms of CAH consists of glucocorticoid and mineralocorticoid replacement in salt-losing forms and testosterone replacement in male patients.
The two last enzymatic defects in testosterone synthesis are not associated with adrenal insufficiency, the isolated 17,20-lyase deficiency (CYP17 deficiency) and 17β-HSD III deficiency (17-β-HSD 3 deficiency) (Fig. 3.2).
The 17,20 lyase activity is catalyzed by P450c17 which converts 17OH-pregnenolone into DHEA and 17OH-progesterone into androstenediona . This is a very rare form of 46,XY DSD and patients with isolated 17,20 lyase deficiency present with atypical genitalia with microphallus, perineal hypospadias, and cryptorchidism [56].
The last step of biosynthesis of testosterone in the Leydig cell is the conversion of androstenedione to testosterone activated by 17β-HSD III .
17β-Hydroxysteroid Dehydrogenase Type III Deficiency
17β-hydroxysteroid dehydrogenase type III deficiency is the most common disorder of androgen synthesis. There are five steroid 17β-HSD enzymes that catalyze this reaction and 46,XY DSD results from mutations in the gene encoding the 17β-HSD 3 isoenzyme [57] that is almost exclusively expressed into testis. Patients present female-like or with atypical genitalia at birth, with the presence of a blind vaginal pouch, intra-abdominal or inguinal testes, and epididymides, vasa deferentia, seminal vesicles and ejaculatory ducts. Most affected males are raised as females, but important virilization occurs at the time of expected puberty (Fig. 3.3). This late virilization is usually a consequence of the presence of testosterone in the circulation as a result of the conversion of androstenedione to testosterone by some other 17β-HSD isoenzyme in the extragonadal tissue and of the secretion of testosterone by the testes when levels of LH are elevated in patientss with some residual 17β-HSD 3 function. However, the discrepancy between the failure of intrauterine masculinization and the virilization at the time of expected puberty is poorly understood. Most patients with 46,XY are raised as girls during childhood and change to male gender-role behavior during puberty. Hormonal diagnosis is based on elevated basal serum levels of androstenedione and low levels of testosterone. At the time of puberty, serum LH and testosterone levels increase in all affected patients and testosterone levels may stay in the normal adult range [43].

Adult patient with 46,XY DSD due to 17β-hydroxysteroid dehydrogenase type III deficiency
Mutations in the HSD17B3 gene are involved with etiology of this disorder.
Table 3.2 summarizes the characteristics of patients with 17β-HSD 3 deficiency.
46,XY DSD with Normal or High Testosterone Secretion
Defects in the Conversion of Testosterone in Dihydrotestosterone: 5 Alpha Reductase 2 Deficiency
Two different enzymes catalyze 5α-reductase reactions. The 5α-RD2 isoenzyme promotes the conversion of testosterone to DHT, the main active metabolite of testosterone responsible for masculinization of external genitalia in the male fetus. It has been demonstrated that the 5α-reductase 1 activity is normal in these patients [58] and that the disorder is due either to homozygous or compound heterozygous loss-of-function mutations of the steroid 5α-reductase 2 gene [59].
Affected male patients present with ambiguous external genitalia, micropenis, normal internal male genitalia (Fig. 3.4b), prostate hypoplasia,and testes with normal differentiation, usually located in the inguinal region and normal or reduced spermatogenesis. Virilization and deep voice appear at puberty, along with penile enlargement and muscle-mass development without gynecomastia. These patients present scarce facial and body hair and absence of temporal male baldness, acne and prostate enlargement. The majority of the patients are reared in the female social sex because of female-like external genitalia at birth (Fig. 3.4a), but many patients who have not been submitted to orchiectomy during childhood undergo a male social sex change at puberty. In our cohort, all patients were registered in the female social sex except for two cases—one who has an affected uncle and the other who was diagnosed before being registered [43] Fourteen out of 30 patients changed to the male gender role. No correlation was observed between SRD5A2 mutation, testosterone/DHT ratio, and gender-role change in these patients. Three cases adopted children and in two cases in vitro fertilization using the patient’s sperm cells resulted in twin siblings in one family and in a single pregnancy in the other. None of the 10 adult female patients are married but eight of them have satisfactory sexual activity [43]. The main differential diagnosis of 5α-RD2 deficiency is with 17β-HSD3 deficiency and partial androgen insensitivity syndrome although in these two disorders, gynecomastia is generally observed .

(a) Female-like external genitalia at prepubertal age. (b) atypical external genitalia and micropenis at pubertal age
The mode of inheritance for 5α-RD2 deficiency is autosomal recessive, however, the uniparental disomy was described in two unrelated patients [60].
Affected children show lower DHT levels and elevated testosterone/DHT ratio after hCG stimulation. Post-pubertal affected patients present with normal or elevated testosterone levels, low DHT levels and elevated testosterone/DHT ratio in basal conditions. Low DHT production following exogenous testosterone administration is also capable of identifying 5a-RD2 deficiency. An elevated 5β/5α urinary metabolite ratio is also an accurate method to diagnose 5α-reductase 2 deficiency even at a prepubertal age and in orchiectomized adult patients [61].
To our knowledge, there are more than 50 families with this described disorder worldwide. In a few cases of 46,XY DSD as a result of 5-a RD2 deficiency diagnosed by clinical and hormonal findings, no mutations were identified in the SRD5A2 gene .
Small penis size is the main concern of male patients with a 5-a RD2 deficiency .
Table 3.3 summarizes the characteristics of patients with 5-a RD2 deficiency.
Defects in Testosterone Action: Androgen Receptor Defects
Disorders of androgen action are the most frequent cause of 46,XY DSD. Androgen insensitivity syndrome is classified as the complete form (CAIS) when there is an absolute absence of androgen action, as the partial form (PAIS) when there are variable degrees of androgen action impairment, and the mild form that is reported in healthy men and boys who can present with adolescent gynecomastia or infertility in later life. Therefore, androgen insensitivity syndrome can be defined as a disorder resulting from complete or partial resistance to the biological actions of androgens in an XY subject with normal testis determination and production of age-appropriate androgen concentrations [62].
Prenatal diagnosis of CAIS can be suspected when a 46,XY fetus presents with female genitalia on prenatal ultrasound. At the prepubertal age, an inguinal hernia in girls can indicate the presence of testes. At puberty, complete breast development and primary amenorrhoea associated with reduced or absent pubic and axillary hair suggest CAIS. Adult women who have intact gonads have the endocrine profile of a hormone-resistant state. Serum testosterone concentrations are either within or above the normal range for men and LH concentrations are increased. FSH and inhibin are generally normal. Estradiol serum levels arising from testosterone aromatization are higher than those observed in men. Gonadotropin serum levels increase further after gonadectomy, but are only partly suppressed with estrogen substitution [62].
Gonadectomy should be performed because of the increased risk of testicular tumors, although it has been reported that tumor risk is low in patients with CAIS before and during puberty [63]. On the other hand, some authors advise to postpone gonadectomy until after spontaneous breast development at puberty [64]. We are for prepubertal gonadectomy as soon as a diagnosis is established and then induction of puberty with estrogens at the appropriate age. This approach diminishes the presence of an inguinal mass that is often painful. In addition, a young child can psychologically better handle the surgical procedure than an adolescent girl. In our experience, breast development is similarly obtained with endogenous estrogenization or with pharmacological replacement. Ultimately, the optimal timing for gonadectomy in patients with CAIS is still controversial [43].
Whereas the clinical picture of CAIS is homogeneous, the phenotype of PAIS is quite variable and depends on the responsiveness of the external genitalia to androgens. Atypical genitalia with microphallus, severe hypospadias, bifid scrotum, and palpable gonads is the most frequent phenotype of PAIS. The large phenotype spectrum of patients with PAIS can cause misdiagnosis with several 46,XY DSDs as a result of defects in androgen production [62]. PAIS diagnosis is unequivocally established by the identification of a molecular defect on the AR gene.
The maternal female relatives of the patient are eligible for screening of the mutation identified in the index case. In case of the carrier status, genetic counseling should be performed.
In patients with AIS, final height is intermediate between mean normal male and female, and decreased bone mineral density in the lumbar spine has been demonstrated [66].
Mild AIS is associated with a mutation of the androgen receptor gene and is infrequently reported. It presents in men as infertility but is not associated with genital anomalies [65]. The product of LH serum and testosterone concentrations as an index of possible mild AIS in infertile men could be a useful screening test for the presence of a mutation in the androgen receptor gene [66].
AR mutations were found in the majority of patients with CAIS and in several patients with PAIS [67, 68]. In our experience, selecting patients with normal basal and hCG-stimulated testosterone and steroid precursors levels, gynecomastia at puberty, and a family history suggestive of X-linked inheritance, results in the identification of mutations in 89 % and 77 % of the families with postpubertal patients with CAIS and PAIS, respectively [68].
As of September 2011, more than 800 different AR mutations have been entered in the Cambridge database of androgen receptor genes.
Patients with CAIS were raised as females and maintained a female gender. Most patients with PAIS who were raised as females maintained a female social sex after postpubertal age, despite clitoral growth and partial virilization. In our experience, all cases with PAIS kept the female social sex [68]. This is in distinct contrast to other forms of 46,XY DSD such as 5-reductase 2 deficiency and 17β-hydroxysteroid dehydrogenase III deficiency in which several affected individuals were raised as females and underwent a change to male social sex at puberty [61, 69].
Table 3.4 summarizes the characteristics of patients with PAIS.
Hormonal treatment: High doses of testosterone esters (250–500 mg twice a week) are used to increase DHT levels and consequently penis size and male secondary characteristics. Maximum penis enlargement is obtained after 6 months of high doses and then the normal dosage is reinstated. The use of topical DHT gel is also useful to increase penis size with the advantage of not causing gynecomastia and promoting a faster increase of penis size as it is 50 times more active than testosterone. DHT is not aromatized, allowing the use of higher doses than testosterone during prepubertal age and consequently attaining a higher degree of virilization.
Management of Patients with 46,XY DSD
The treatment of patients with 46,XY DSD requires an appropriately trained multi-disciplinary team. Early diagnosis is important for good patient outcome and should begin with a careful examination of the newborn’s genitalia.
Psychological evaluation is of extreme importance in the treatment of patients with DSD. Every couple who have a child with atypical genitalia must be assessed and counseled by an experienced psychologist, specialized in gender identity, who must act as soon as the diagnosis is suspected.
The physician and psychologist must inform the parents about normal sexual development. A simple, detailed and comprehensive explanation about what to expect regarding integration into social life, sexual activity, requirement of hormonal and surgical treatment, and the possibility of fertility according to the sex of rearing, should also be discussed with the parents, before the attainment of final social sex.
The determination of social sex must take into account the etiological diagnosis, penis size, ethnic traditions, sexual identity, and the acceptance of the assigned social sex by the parents. In the event that the parents and health care providers disagree over the sex of rearing and psychological support was not able to change the parents’ choice, their opinion should always prevail to avoid ambiguous sex of rearing. The affected child and his/her family must be followed throughout life to ascertain the patient’s adjustment to his/her social sex [43].
Hormonal Therapy in Patients With DSD with Male Social Sex
Testosterone replacement begins between 10 and 11 years of age, simulating normal puberty according to the child’s psychological evaluation and height. The initial dose of short-acting testosterone esters is 25–50 mg/month intramuscularly. The maintenance dose in adult patients is 200–250 mg every 2 weeks for injectable short-acting testosterone, 1000 mg every 3 months for long-acting testosterone, and 50–60 mg every day for transdermal testosterone.
In those patients with androgen insensitivity, higher doses of testosterone esters (250–500 mg twice a week) are used to increase penis size and male secondary characteristics. Maximum penis enlargement is obtained after 6 months of high doses and then normal dosage is reinstated [61].
The use of topical DHT gel is also useful to increase penis size with the advantage of not causing gynecomastia and promoting faster increase of penis growth as it is 50 times more active than testosterone. Considering that DHT is not aromatized, one would expect it to have no effect on bone maturation, allowing the use of higher doses than testosterone and consequently attaining a higher degree of virilization [43].
Surgical Procedures in Patients With DSD with Male Social Sex
The goals of surgical treatment are to provide an adequate external genitalia and removal of internal structures that are inappropriate for the social sex. Patients must undergo surgical treatment preferably before 2 years of age, which is the time when the child becomes aware of his/her genitals and social sex. Only skilled surgeons with specific training in the surgery of DSD should perform these procedures [43].
Surgery consists of orthophaloplasty, scrotumplasty with resection of vaginal pouch, proximal and distal urethroplasty, and orchidopexy when necessary. Surgeries are performed in two or three steps in patients with perineal hypospadias. The most frequent complication is urethral fistula in the penoscrotal angle and urethral stenosis that can occur several years after surgery. The aesthetical and functional results of surgical correction are good in our and other series [70].
Most of our patients present with satisfactory sexual performance as long as they present with a penis size of at least 6 cm [70]. New approaches, such as the use of donor-grafting tissue to elongate the urethra and penis may help these patients in the future .
Ultimately, patients with 46,XY DSD present a large phenotype spectrum, and the etiological diagnosis sometimes can not be determined through conventional techniques available clinically. The molecular tools have added new possibilities in the investigation of these patients [45]. The majority of patients with DSD present with atypical genitalia and their sex assignment may be a complex procedure. The choice of male sex-of rearing in 46,XY babies with ambiguous genitalia is a challenging situation. The participation of a multidisciplinary team is essential in this process and the fast identification of a molecular defect causative of the disorder might collaborate in this decision [43].
References
Terasawa E, Fernandez DL. Neurobiological mechanisms of the onset of puberty in primates. Endocr Rev. 2001;22(1):111–51.
Petersen C, Soder O. The sertoli cell--a hormonal target and ‘super’ nurse for germ cells that determines testicular size. Horm Res. 2006;66(4):153–61.
Rey RA, Grinspon RP, Gottlieb S, Pasqualini T, Knoblovits P, Aszpis S, et al. Male hypogonadism: an extended classification based on a developmental, endocrine physiology-based approach. Andrology. 2013;1(1):3–16.
Silveira LG, Latronico AC, Seminara SB. Kisspeptin and clinical disorders. Adv Exp Med Biol. 2013;784:187–99.
Abreu AP, Dauber A, Macedo DB, Noel SD, Brito VN, Gill JC, et al. Central precocious puberty caused by mutations in the imprinted gene MKRN3. N Engl J Med. 2013;368(26):2467–75.
Seminara SB, Messager S, Chatzidaki EE, Thresher RR, Acierno Jr JS, Shagoury JK, et al. The GPR54 gene as a regulator of puberty. N Engl J Med. 2003;349(17):1614–27.
de Roux N, Genin E, Carel JC, Matsuda F, Chaussain JL, Milgrom E. Hypogonadotropic hypogonadism due to loss of function of the KiSS1-derived peptide receptor GPR54. Proc Natl Acad Sci U S A. 2003;100(19):10972–6.
Pinilla L, Aguilar E, Dieguez C, Millar RP, Tena-Sempere M. Kisspeptins and reproduction: physiological roles and regulatory mechanisms. Physiol Rev. 2012;92(3):1235–316.
Skorupskaite K, George JT, Anderson RA. The kisspeptin-GnRH pathway in human reproductive health and disease. Hum Reprod Update. 2014;20(4):485–500.
Sherins RJ, Loriaux DL. Studies of the role of sex steroids in the feedback control of FSH concentrations in men. J Clin Endocrinol Metab. 1973;36(5):886–93.
Santen RJ, Bardin CW. Episodic luteinizing hormone secretion in man. Pulse analysis, clinical interpretation, physiologic mechanisms. J Clin Invest. 1973;52(10):2617–28.
Tilbrook AJ, de Kretser DM, Cummins JT, Clarke IJ. The negative feedback effects of testicular steroids are predominantly at the hypothalamus in the ram. Endocrinology. 1991;129(6):3080–92.
Hayes FJ, Seminara SB, Decruz S, Boepple PA, Crowley Jr WF. Aromatase inhibition in the human male reveals a hypothalamic site of estrogen feedback. J Clin Endocrinol Metab. 2000;85(9):3027–35.
George JT, Veldhuis JD, Roseweir AK, Newton CL, Faccenda E, Millar RP, et al. Kisspeptin-10 is a potent stimulator of LH and increases pulse frequency in men. J Clin Endocrinol Metab. 2011;96(8):E1228–36.
Navarro VM, Castellano JM, Fernandez-Fernandez R, Tovar S, Roa J, Mayen A, et al. Effects of KiSS-1 peptide, the natural ligand of GPR54, on follicle-stimulating hormone secretion in the rat. Endocrinology. 2005;146(4):1689–97.
Thompson EL, Patterson M, Murphy KG, Smith KL, Dhillo WS, Todd JF, et al. Central and peripheral administration of kisspeptin-10 stimulates the hypothalamic-pituitary-gonadal axis. J Neuroendocrinol. 2004;16(10):850–8.
Young J, George JT, Tello JA, Francou B, Bouligand J, Guiochon-Mantel A, et al. Kisspeptin restores pulsatile LH secretion in patients with neurokinin B signaling deficiencies: physiological, pathophysiological and therapeutic implications. Neuroendocrinology. 2013;97(2):193–202.
Decker MH, Loriaux DL, Cutler Jr GB. A seminiferous tubular factor is not obligatory for regulation of plasma follicle-stimulating hormone in the rat. Endocrinology. 1981;108(3):1035–9.
de Kretser DM, Robertson DM. The isolation and physiology of inhibin and related proteins. Biol Reprod. 1989;40(1):33–47.
Forage RG, Ring JM, Brown RW, McInerney BV, Cobon GS, Gregson RP, et al. Cloning and sequence analysis of cDNA species coding for the two subunits of inhibin from bovine follicular fluid. Proc Natl Acad Sci U S A. 1986;83(10):3091–5.
Ling N, Ying SY, Ueno N, Shimasaki S, Esch F, Hotta M, et al. Pituitary FSH is released by a heterodimer of the beta-subunits from the two forms of inhibin. Nature. 1986;321(6072):779–82.
Vale W, Rivier J, Vaughan J, McClintock R, Corrigan A, Woo W, et al. Purification and characterization of an FSH releasing protein from porcine ovarian follicular fluid. Nature. 1986;321(6072):776–9.
Ueno N, Ling N, Ying SY, Esch F, Shimasaki S, Guillemin R. Isolation and partial characterization of follistatin: a single-chain Mr 35,000 monomeric protein that inhibits the release of follicle-stimulating hormone. Proc Natl Acad Sci U S A. 1987;84(23):8282–6.
Nakamura T, Takio K, Eto Y, Shibai H, Titani K, Sugino H. Activin-binding protein from rat ovary is follistatin. Science. 1990;247(4944):836–8.
Sharpe RM, Turner KJ, McKinnell C, Groome NP, Atanassova N, Millar MR, et al. Inhibin B levels in plasma of the male rat from birth to adulthood: effect of experimental manipulation of Sertoli cell number. J Androl. 1999;20(1):94–101.
Anderson RA, Wallace EM, Groome NP, Bellis AJ, Wu FC. Physiological relationships between inhibin B, follicle stimulating hormone secretion and spermatogenesis in normal men and response to gonadotrophin suppression by exogenous testosterone. Hum Reprod. 1997;12(4):746–51.
Krummen LA, Toppari J, Kim WH, Morelos BS, Ahmad N, Swerdloff RS, et al. Regulation of testicular inhibin subunit messenger ribonucleic acid levels in vivo: effects of hypophysectomy and selective follicle-stimulating hormone replacement. Endocrinology. 1989;125(3):1630–7.
Wallace EM, Groome NP, Riley SC, Parker AC, Wu FC. Effects of chemotherapy-induced testicular damage on inhibin, gonadotropin, and testosterone secretion: a prospective longitudinal study. J Clin Endocrinol Metab. 1997;82(9):3111–5.
Mather JP, Attie KM, Woodruff TK, Rice GC, Phillips DM. Activin stimulates spermatogonial proliferation in germ-Sertoli cell cocultures from immature rat testis. Endocrinology. 1990;127(6):3206–14.
Archambeault DR, Yao HH. Activin A, a product of fetal Leydig cells, is a unique paracrine regulator of Sertoli cell proliferation and fetal testis cord expansion. Proc Natl Acad Sci U S A. 2010;107(23):10526–31.
Mendis SH, Meachem SJ, Sarraj MA, Loveland KL. Activin A balances Sertoli and germ cell proliferation in the fetal mouse testis. Biol Reprod. 2011;84(2):379–91.
de Winter JP, Themmen AP, Hoogerbrugge JW, Klaij IA, Grootegoed JA, de Jong FH. Activin receptor mRNA expression in rat testicular cell types. Mol Cell Endocrinol. 1992;83(1):R1–8.
Meinhardt A, O’Bryan MK, McFarlane JR, Loveland KL, Mallidis C, Foulds LM, et al. Localization of follistatin in the rat testis. J Reprod Fertil. 1998;112(2):233–41.
Tilbrook AJ, de Kretser DM, Dunshea FR, Klein R, Robertson DM, Clarke IJ, et al. The testis is not the major source of circulating follistatin in the ram. J Endocrinol. 1996;149(1):55–63.
Ramaswamy S, Pohl CR, McNeilly AS, Winters SJ, Plant TM. The time course of follicle-stimulating hormone suppression by recombinant human inhibin A in the adult male rhesus monkey (Macaca mulatta). Endocrinology. 1998;139(8):3409–15.
Tilbrook AJ, De Kretser DM, Clarke IJ. Human recombinant inhibin A suppresses plasma follicle-stimulating hormone to intact levels but has no effect on luteinizing hormone in castrated rams. Biol Reprod. 1993;49(4):779–88.
Matzuk MM, Kumar TR, Bradley A. Different phenotypes for mice deficient in either activins or activin receptor type II. Nature. 1995;374(6520):356–60.
Chemes HE, Dym M, Raj HG. Hormonal regulation of Sertoli cell differentiation. Biol Reprod. 1979;21(1):251–62.
Josso N, Picard JY, Rey R, di Clemente N. Testicular anti-Mullerian hormone: history, genetics, regulation and clinical applications. Pediatr Endocrinol Rev. 2006;3(4):347–58.
Rey RA, Musse M, Venara M, Chemes HE. Ontogeny of the androgen receptor expression in the fetal and postnatal testis: its relevance on Sertoli cell maturation and the onset of adult spermatogenesis. Microsc Res Tech. 2009;72(11):787–95.
Young J, Rey R, Couzinet B, Chanson P, Josso N, Schaison G. Antimullerian hormone in patients with hypogonadotropic hypogonadism. J Clin Endocrinol Metab. 1999;84(8):2696–9.
Jensen TK, Andersson AM, Hjollund NH, Scheike T, Kolstad H, Giwercman A, et al. Inhibin B as a serum marker of spermatogenesis: correlation to differences in sperm concentration and follicle-stimulating hormone levels. A study of 349 Danish men. J Clin Endocrinol Metab. 1997;82(12):4059–63.
Mendonca BB, Domenice S, Arnhold IJ, Costa EM. 46,XY disorders of sex development (DSD). Clin Endocrinol (Oxf). 2009;70(2):173–87.
MacLaughlin DT, Donahoe PK. Sex determination and differentiation. N Engl J Med. 2004;350(4):367–78.
Achermann JC, Domenice S, Bachega TA, Nishi MY, Mendonca BB. Disorders of sex development: effect of molecular diagnostics. Nat Rev Endocrinol. 2015;11(8):478–88.
New MI, Lekarev O, Parsa A, Yuen TT, O’Malley BW, Hammer GD. Genetic steroid disorders, vol. xiii. Amsterdam: Elsevier; 2014. 392 pages.
Grino PB, Griffin JE, Wilson JD. Testosterone at high concentrations interacts with the human androgen receptor similarly to dihydrotestosterone. Endocrinology. 1990;126(2):1165–72.
Ostrer H. Disorders of sex development (DSDs): an update. J Clin Endocrinol Metab. 2014;99(5):1503–9.
Berkovitz GD, Fechner PY, Zacur HW, Rock JA, Snyder 3rd HM, Migeon CJ, et al. Clinical and pathologic spectrum of 46,XY gonadal dysgenesis: its relevance to the understanding of sex differentiation. Medicine (Baltimore). 1991;70(6):375–83.
Arnhold IJ, de Mendonca BB, Toledo SP, Madureira G, Nicolau W, Bisi H, et al. Leydig cell hypoplasia causing male pseudohermaphroditism: case report and review of the literature. Rev Hosp Clin Fac Med Sao Paulo. 1987;42(5):227–32.
Arnhold IJ, Mendonca BB, Bloise W, Toledo SP. Male pseudohermaphroditism resulting from Leydig cell hypoplasia. J Pediatr. 1985;106(6):1057.
Latronico AC, Anasti J, Arnhold IJ, Rapaport R, Mendonca BB, Bloise W, et al. Brief report: testicular and ovarian resistance to luteinizing hormone caused by inactivating mutations of the luteinizing hormone-receptor gene. N Engl J Med. 1996;334(8):507–12.
Toledo SP, Arnhold IJ, Luthold W, Russo EM, Saldanha PH. Leydig cell hypoplasia determining familial hypergonadotropic hypogonadism. Prog Clin Biol Res. 1985;200:311–4.
Tint GS, Irons M, Elias ER, Batta AK, Frieden R, Chen TS, et al. Defective cholesterol biosynthesis associated with the Smith-Lemli-Opitz syndrome. N Engl J Med. 1994;330(2):107–13.
Miller WL. Molecular biology of steroid hormone synthesis. Endocr Rev. 1988;9(3):295–318.
Geller DH, Auchus RJ, Miller WL. P450c17 mutations R347H and R358Q selectively disrupt 17,20-lyase activity by disrupting interactions with P450 oxidoreductase and cytochrome b5. Mol Endocrinol. 1999;13(1):167–75.
Andersson S, Moghrabi N. Physiology and molecular genetics of 17 beta-hydroxysteroid dehydrogenases. Steroids. 1997;62(1):143–7.
Jenkins EP, Andersson S, Imperato-McGinley J, Wilson JD, Russell DW. Genetic and pharmacological evidence for more than one human steroid 5 alpha-reductase. J Clin Invest. 1992;89(1):293–300.
Thigpen AE, Davis DL, Milatovich A, Mendonca BB, Imperato-McGinley J, Griffin JE, et al. Molecular genetics of steroid 5 alpha-reductase 2 deficiency. J Clin Invest. 1992;90(3):799–809.
Chavez B, Valdez E, Vilchis F. Uniparental disomy in steroid 5alpha-reductase 2 deficiency. J Clin Endocrinol Metab. 2000;85(9):3147–50.
Mendonca BB, Inacio M, Costa EM, Arnhold IJ, Silva FA, Nicolau W, et al. Male pseudohermaphroditism due to steroid 5alpha-reductase 2 deficiency. Diagnosis, psychological evaluation, and management. Medicine (Baltimore). 1996;75(2):64–76.
Hughes IA, Davies JD, Bunch TI, Pasterski V, Mastroyannopoulou K, MacDougall J. Androgen insensitivity syndrome. Lancet. 2012;380(9851):1419–28.
Hannema SE, Scott IS, Rajpert-De Meyts E, Skakkebaek NE, Coleman N, Hughes IA. Testicular development in the complete androgen insensitivity syndrome. J Pathol. 2006;208(4):518–27.
Cools M, van Aerde K, Kersemaekers AM, Boter M, Drop SL, Wolffenbuttel KP, et al. Morphological and immunohistochemical differences between gonadal maturation delay and early germ cell neoplasia in patients with undervirilization syndromes. J Clin Endocrinol Metab. 2005;90(9):5295–303.
Zuccarello D, Ferlin A, Vinanzi C, Prana E, Garolla A, Callewaert L, et al. Detailed functional studies on androgen receptor mild mutations demonstrate their association with male infertility. Clin Endocrinol (Oxf). 2008;68(4):580–8.
Wang RS, Yeh S, Tzeng CR, Chang C. Androgen receptor roles in spermatogenesis and fertility: lessons from testicular cell-specific androgen receptor knockout mice. Endocr Rev. 2009;30(2):119–32.
Ahmed SF, Cheng A, Dovey L, Hawkins JR, Martin H, Rowland J, et al. Phenotypic features, androgen receptor binding, and mutational analysis in 278 clinical cases reported as androgen insensitivity syndrome. J Clin Endocrinol Metab. 2000;85(2):658–65.
Melo KF, Mendonca BB, Billerbeck AE, Costa EM, Inacio M, Silva FA, et al. Clinical, hormonal, behavioral, and genetic characteristics of androgen insensitivity syndrome in a Brazilian cohort: five novel mutations in the androgen receptor gene. J Clin Endocrinol Metab. 2003;88(7):3241–50.
Mendonca BB, Inacio M, Arnhold IJ, Costa EM, Bloise W, Martin RM, et al. Male pseudohermaphroditism due to 17 beta-hydroxysteroid dehydrogenase 3 deficiency. Diagnosis, psychological evaluation, and management. Medicine (Baltimore). 2000;79(5):299–309.
Sircili MH, e Silva FA, Costa EM, Brito VN, Arnhold IJ, Denes FT, et al. Long-term surgical outcome of masculinizing genitoplasty in large cohort of patients with disorders of sex development. J Urol. 2010;184(3):1122–7.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
de Mendonca, B.B., Costa, E.M.F. (2017). Physiology of Male Gonadotropic Axis and Disorders of Sex Development. In: Hohl, A. (eds) Testosterone. Springer, Cham. https://doi.org/10.1007/978-3-319-46086-4_3
Download citation
DOI: https://doi.org/10.1007/978-3-319-46086-4_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-46084-0
Online ISBN: 978-3-319-46086-4
eBook Packages: MedicineMedicine (R0)