
Abstract
Case selection for cone beam computed tomography (CBCT) for dental purposes is primarily based on individual risk-benefit assessment, balancing between the long-term radiation risks of CBCT and its ultimate benefit for each individual patient. Based on the currently available literature, the expected ultimate benefit to the patient, as evaluated by the level of diagnostic efficacy of CBCT in dentistry, is yet unclear, and it is mainly limited to its technical and the diagnostic accuracy efficacies. Even for these levels of efficacy, evidence is incomplete. Therefore, the efficacy of CBCT in supporting the practitioner’s decision making, the treatment planning, and eventually in affecting treatment outcomes is not fully elucidated. On the other hand, the potential radiation risks of CBCT scan are uncertain and are stochastic in nature, thus requiring a preventive clinical approach. Consequently, cautious decision making is warranted when a CBCT scan is considered. This chapter reviews the current literature concerning the benefits of CBCT in dental practice, alongside its risks in this use, and presents a practical case-selection algorithm for the use of CBCT in dentistry.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Keywords
7.1 Introduction
Cone beam computed tomography (CBCT) was introduced in the late 1990s to construct three-dimensional scans of the maxillofacial region at a reduced radiation dose compared to the conventional CT [1–11] and has become a popular diagnostic technique in dentistry [1, 2, 12]. Although the effective radiation dose of CBCT scans is indeed reduced compared to multi-slice computed tomography (MSCT), it is still significantly higher than intraoral radiography or panoramic radiography [12, 13]. In addition, the long-term health risks of CBCT use in dentistry are unclear [2, 14–18]. It is therefore an acceptable practice that every effort should be made to reduce the overall effective radiation dose to the dental patient [2, 4, 12].
In recent years there has been a debate whether CBCT should be used as a standard preoperative imaging modality in dentistry [5–11, 19–23]. For example, it was stated in the American Association of Endodontists (AAE) and the American Academy of Oral and Maxillofacial Radiology (AAOMR) joint position statements from 2010 [2] and from 2015 [1] that CBCT should not be used routinely for endodontic diagnosis or for screening purposes in the absence of clinical signs and symptoms [1, 2]. However, the exact criteria for using CBCT for endodontic purposes are not sufficiently clear [2, 24–27], and the latest published data demonstrate that CBCT is being used also for routine endodontic purposes, such as preoperative evaluation of root canal system anatomy [28, 29], determination of root canal working length [30–33], identification of a healthy periapical tissue, or diagnosing vital teeth with irreversible pulpitis [12, 34, 35]. The increased usage rates of CBCT in dental practices, along with its unknown long-term health risks, present a significant long-term health concern [2, 4, 12, 36–38].
The decision to perform a CBCT scan must be justified on an individual basis by demonstrating that the benefits to the patient outweigh the potential radiation exposure risks [1, 2, 39]. Therefore, the case selection of CBCT is primarily a question of risk-benefit assessment [2, 12, 39]. These potential benefits to the patient should be largely based on the efficacy of the CBCT as a diagnostic imaging modality for each specific dental evaluation [2, 12, 39–41].
Diagnostic efficacy may be defined as “the probability of benefit to individuals from a system or test under ideal conditions of use” [12, 42]. A shallow view of the efficacy of diagnostic imaging would be that it should provide images of sufficient quality for diagnostic purposes that it was intended for [40, 41]. However, a more comprehensive point of view is required in order to evaluate the ultimate benefit of an imaging modality to an efficient and effective treatment of a patient [40, 41].
This comprehensive point of view on the efficacy of an imaging modality involves parameters that are beyond the technical characteristics and the accuracy of the imaging modality [12, 41, 42]. It should include also additional higher levels of efficacy evaluation such as the efficacy of this modality to support the practitioner’s decision making and treatment planning and eventually to improve the treatment outcome [12, 41, 43].
This chapter reviews the current literature concerning the benefits of CBCT in dental practice, alongside its risks in this use, and presents a case-selection algorithm for the use of CBCT in dentistry.
7.2 The Potential Benefits
It has been stated that CBCT should be considered for diagnosis only if a review of the patient’s health and imaging history together with a meticulous clinical examination lead to a conclusion that CBCT may significantly contribute to achieve an accurate and consistent diagnosis [2, 19, 39, 44, 45]. However, the need to achieve an accurate diagnosis is not the only factor that should be considered for adequate case selection – it is prudent that the decision to use CBCT be justified by demonstrating that the ultimate benefits to that particular patient outweigh the potential risks of radiation exposure [2, 12, 39].
The expected ultimate benefits of CBCT to the patient may be evaluated by levels of diagnostic efficacy. The diagnostic efficacy hierarchical model presented by Fryback and Thornbury [41] is a comprehensive tool for appraisal of the literature on efficacy of a diagnostic imaging modality [12]. It is comprised of six levels of imaging efficacy that include not only the technical characteristics of the imaging modality but also the efficacy of this modality to support the practitioner’s decision making and treatment planning and to eventually improve treatment outcome [12, 41, 43].
This model [40, 41] includes the following efficacy levels (in a hierarchical order, from the lowest to the highest efficacy level):
-
The technical efficacy – the technical quality of the images
-
The diagnostic accuracy efficacy – the diagnostic accuracy associated with interpretation of the images
-
The diagnostic thinking efficacy – the effect of the obtained radiographic information on clinician’s estimate of the probability that a patient suffers from a disease or health condition
-
The therapeutic efficacy – the effects of the radiographic information on the patient’s management plan
-
The patient outcome efficacy – the effect of the obtained radiographic information on patient’s outcomes
-
The societal efficacy – the impact of the imaging modality on society as a whole [12]
-
This model is aimed to draw conclusions regarding the diagnostic efficacy of any imaging modality based on the currently available literature, and it has been used in recent years in dental research to evaluate the diagnostic efficacies of CBCT [12, 20, 21, 23, 40].
Numerous studies have been published on the applications of CBCT in dentistry, and the significant variability in their study designs generated inconsistent and confusing results [4–11, 13, 24, 25, 27–35, 45–47]. Evidence-based dentistry (EBD) is an approach to oral healthcare that integrates the best available clinical evidence to support a practitioner’s clinical expertise for each patient’s treatment needs and preferences [48–50]. Therefore, systematic reviews, which constitute the foundations of EBD, are of utmost importance in the evaluation of the diagnostic efficacy of CBCT in dentistry [48, 50, 51].
A recent systematic review [20] evaluated the evidence for the diagnostic efficacy of 3-D cephalometry in orthodontics and concluded that the current evidence for it is limited. In this systematic review, only six studies met the criteria for a moderate level of evidence, stressing the need for methodologically standardized studies on a 3-D cephalometric analysis [20].
Another study [21] evaluated the available clinical research and diagnostic efficacy studies in the oral and maxillofacial radiology literature and concluded that the current literature consists mostly of case reports, case series, and cross-sectional studies, assessing mostly technical efficacy and diagnostic accuracy [21]. In this review the authors stated that “such studies do not provide strong evidence for clinical decision making nor do they address the impact of diagnostic imaging on patient care” and that “more studies at the higher end of the study design and efficacy hierarchies are needed in order to make wise choices regarding clinical decisions and resource allocations” [21].
Another recently published study [43] evaluated the efficacy of CBCT for assessment of mandibular third molars using the hierarchical model by Fryback and Thornbury [41] and reported that only few high-evidence studies on the efficacy of CBCT for radiographic examination of mandibular third molars currently exist [43]. They stated that “periapical or panoramic examination is sufficient in most cases before removal of mandibular third molars. However, CBCT may be suggested when one or more signs for a close contact between the tooth and the canal are present in the two-dimensional image – if it is believed that CBCT will change the treatment or the treatment outcome for the patient” [43] (Fig. 7.1).

(a–c) Presents three cases of assessment of mandibular third molars that are planned to be extracted. (a) The right mandibular third molar was scheduled for extraction. The initial panoramic radiograph (a1) was not sufficient in order to plan the procedure, and therefore CBCT evaluation was performed (a2, a3). (b) The right mandibular third molar was scheduled for extraction. The initial panoramic radiograph (b1) was not sufficient in order to plan the procedure, and therefore CBCT evaluation was performed (b2, b3). (c) The left (c2) and the right (c1) mandibular third molars were scheduled for extraction. The panoramic radiograph was sufficient in order to plan the procedures. Therefore, CBCT was not performed
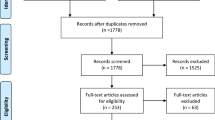
In a recent study [12], a systematic review of the literature was performed to identify and analyze studies evaluating the use of CBCT in endodontics. Initially 485 possible relevant articles were identified. However, following the application of strict inclusion criteria, only 58 articles (12 %) met the inclusion criteria and were analyzed and allocated to levels of efficacy according to the Fryback and Thornbury model [41]. Most eligible articles (n = 52, 90 %) evaluated technical characteristics or the accuracy of CBCT, defined in this model as low levels of efficacy [41]. Only six articles (10 %) proclaimed to evaluate the efficacy of CBCT to support the practitioner’s decision making and treatment planning and ultimately to affect the treatment outcome, defined as higher levels of efficacy. They concluded that the expected ultimate benefit of CBCT to the endodontic patient as evaluated by its level of diagnostic efficacy is yet unclear and is mainly limited to its technical and diagnostic accuracy efficacies. They therefore concluded that a cautious and rational approach is advised when considering CBCT for endodontic purposes [12] (Fig. 7.2).


Case selection of CBCT for the diagnosis and treatment of teeth with complex anatomy: two comparable cases of an additional third root in mandibular molar teeth scheduled for root canal treatment are presented. In case #1 CBCT was indicated, and in case #2 CBCT was not indicated. Case #1a–1g A lower second mandibular molar with an additional third root was scheduled for endodontic treatment. However, preoperative (1a) and intraoperative (1b) periapical Rx’s, together with a thorough inspection by surgical operation microscope during the treatment did not provide sufficient information to locate the additional root. The patient was referred to CBCT that confirmed the presence and location of the additional third root (1c–1e). This root was endodontically treated (1f, 1g). Case #2a–2c A lower first mandibular molar with an additional third root was scheduled for endodontic treatment. Preoperative (2a) and intraoperative (2b) periapical Rx’s, together with a thorough inspection by surgical operation microscope during the treatment provided sufficient information to locate and endodontically treat the additional root (2c). Therefore, in this case CBCT was not indicated
A comprehensive systematic review of the entire dental literature [40] assessed the risks and benefits of CBCT in dentistry. In that systematic review, it was reported that the understanding of CBCT’s diagnostic efficacy in dentistry was largely limited to the first two lower levels of efficacy (i.e., the technical and diagnostic accuracy efficacies) and that even for these, knowledge is incomplete. In this review only a few publications were identified which addressed higher levels of diagnostic efficacy [40, 41]. The authors concluded [40] that “development of guidelines with high evidence grades was precluded” and that it also “highlights the need for clinical trials which will provide information on higher level efficacies, notably patient outcome efficacy”[40].
It is therefore evident that the current dental literature assessing the efficacy of CBCT as a diagnostic imaging modality is limited to the lower levels of efficacy, specifically to the technical characteristics, or to the accuracy of the imaging modality [40, 41]. These low levels of efficacy may be a prime interest for some clinicians; however, they provide only a partial view of the potential ultimate benefit of CBCT to patients [12, 40, 41]. Since the ultimate goal of medical diagnosis is to treat patients effectively and efficiently, only higher levels of diagnostic efficacies (e.g., therapeutic efficacy, patient outcome efficacy, and societal efficacy, defined as levels 4–6 of efficacies) are capable to provide a comprehensive view of the ultimate benefit of the modality to patients or to the society as a whole [12, 40, 41].
In this context, a high-quality imaging modality such as CBCT may be ineffective in certain instances, while an imaging modality of a lesser quality such as intraoral radiography may be of significant value in certain instances [12, 40, 41]. In addition, in order for an imaging modality to be considered efficacious at a higher level in this hierarchical model of diagnostic efficacy (e.g., therapeutic efficacy and patient outcome efficacy), it must be efficacious at lower levels, but not the other way around. In addition, improvements in the efficacy at a lower level (e.g., technical efficacy) will not guarantee an ensuing improvement at the higher efficacy levels (e.g., patient outcome efficacy) [12, 41, 42].
This asymmetry is often not well understood in dental research reports dealing with diagnostic efficacy levels 1 and 2 (e.g., technical efficacy) [40, 41], in which an improvement in some technical characteristics of CBCT or in its accuracy in a certain clinical scenario may incorrectly lead to a conclusion that these new findings also guarantee an improvement in higher levels of efficacy (e.g., the patient outcome) and in the expected ultimate benefit to the patient. It also highlights the need for additional clinical trials which will provide information on higher level efficacies, especially regarding patient outcome efficacy [12, 40].
Adequate professional standards for performing CBCT imaging in a certain patient should be based on selection criteria derived from the best available evidence [22]. However, the current available dental literature provides a very limited view on the ultimate benefit of CBCT to patients. In conclusion, as recently stated: “in this expanding era of CBCT imaging in dentistry, the apparent urgency of adopting glittering new technology should be balanced with diligent discovery and patience”[22].
7.3 The Potential Risks
In general, CBCT produces a higher radiation dose than traditional intraoral radiography, but less than that produced during a multi-detector CT scan [39]. However, the comparison of radiation doses by itself is too simplistic, as aside from the physical properties of the CBCT machine, estimation of radiation health effects requires an understanding of the nature of the X-ray radiation and its tissue effects and should also take into consideration a variety of other parameters such as the scanning parameters, the patient demographics, and the nature of the exposed tissues and organs [12, 13].
Diagnostic X-ray is an electromagnetic (EM) ionizing radiation with a small wavelength, deep penetration, and high energy transfer capabilities [4, 13, 39, 40, 52] that potentially may cause tissue damage and specifically DNA damage leading to chromosomal mutations and ensuing formation of malignancy [40]. These ionizing effects have no threshold radiation dose and are considered as “chance” (“stochastic”) effects, making the distinction between “harmless” and “dangerous” exposures to radiation impractical [4, 13, 39, 40, 52]. Thus, any exposure to X-rays should not be considered as risk-free [4, 12, 13, 39, 40, 52].
The effective dose of CBCT scans, which takes into consideration also the specific radiosensitivity of the evaluated tissues [40], varies among scanners and depends on both clinical parameters such as the region of the jaw being scanned and on acquisition parameters, such as the field-of-view (FOV) dimensions, exposure time, and the tube electric current and potential [13]. A recent meta-analysis of the literature [53] analyzed the reported effective dose estimations of dental CBCT examinations and found large variations: the reported adult-effective doses ranged from 46 to 1073 μSv for large FOVs, between 9 and 560 μSv for medium FOVs, and between 5 and 652 μSv for small FOVs. The reported child-effective doses ranged from 13 to 769 μSv for large or medium FOVs and from 7 to 521 μSv for small FOVs. They concluded that “large exposure ranges make CBCT doses difficult to generalize” [53].
In addition, the radiation damage experienced by an exposed group and its descendants is gender and age dependent [36–38, 40]. At all ages, the reported risks for females are slightly higher than for males [13]. It has been reported that the risk is tripled in children under 10 years old in relation to the risk at age 30 [40]. Children’s cancer risk per unit dose of ionizing radiation is higher than adults, and they have a longer lifetime risk of developing radiation-induced cancers [2, 17, 39]. Therefore, additional strict considerations should be weighted prior to the exposure of children to CBCT scanning [36–38].
Radiation risk management is the assessment of future-associated health risks, including the effect of uncertainty, followed by efforts to minimize the probability and impact of these suspected adverse effects [36–38, 54]. CBCT radiation risk management requires a combination of two principles: justification, defined as “doing more good than harm to the patient,” and optimization based on the “ALARA” principle – as low as reasonably achievable, meaning to obtain the necessary diagnostic information using the lowest radiation dose that can be reasonably achieved [40]. However, the uncertain long-term and stochastic nature of radiation risks requires a preventive clinical approach [2, 13, 39, 54], which may not always be easy to implement [12, 36–38].
The traditional nonpreventive approach to health hazards, late lessons from early warnings [55], is described as delayed learning from historical early worrying events [55]. A historical medical example of this approach is the story of asbestos: in 1898, Lucy Deane, a United Kingdom (UK) industrial inspector, observed and reported about the evil effects of asbestos dust [55]. However, only in 1998 the UK government, followed by the European Union (EU), decided to ban the use of asbestos [55], and current future estimates suggest that the number of asbestos-related fatalities in Western Europe would reach about a quarter of a million over the next 35 years [56]. This devastating outcome is an example to a misuse of the concept of precaution when dealing with a potential health hazard and to the need to adopt a modern preventive approach [55].
In this context, preventing long-term health hazards sometimes requires acting before there is an established proof of harm [55]. The precautionary principle represents a modern preventive approach to health hazards that can be defined as a “better safe than sorry approach suggesting that action should be taken to avoid harm even when it is not certain to occur”[57]. However, this preventive approach may be especially difficult to implement when the impacts of the potential health hazard are far into the future and the immediate perceived benefits from avoiding current preventive measures are significant [12, 55–58].
In the context of CBCT imaging, the potential immediate benefit to the individual patient from the use of CBCT imaging in dental practice may be perceived as substantial [2, 12, 59]. However, the relatively high radiation doses associated with CBCT compared to conventional radiography [13] still raise long-term health concerns especially regarding a potential increase in the risk of malignancy and especially in children [2, 14–18, 26, 36–38, 60]. Furthermore, the adverse effects of the CBCT radiation exposure may not be seen until years after the actual exposure [2, 13–18, 36–38]. Thus, implementing the precautionary principle in the decision making when considering a CBCT scan for dental purposes is prudent [2, 12, 55, 57].
With the growing popularity of CBCT technologies among dental practitioners [2, 13], concerns have also been expressed about the level of training, education, and experience required to interpret the CBCT data [39]. In addition to CBCT data on the region of interest, CBCT scans usually include additional adjacent anatomical structures that are usually not visible in the FOV of routine intraoral radiographs, and the practitioner who performs a CBCT study is obligated to systematically examine the entire CBCT image data and report on any anatomical abnormalities or pathological conditions observed [2, 39, 40, 61]. However, this diagnostic obligation requires a comprehensive radiology knowledge of head and neck anatomy and pathology that may be beyond the dental practitioner qualifications, thus subjecting the patient to risks of undiagnosed or misdiagnosed pathological conditions and the practitioner to an ensuing medicolegal liability risk [54, 61].
7.4 Case Selection Algorithm for the Use of CBCT in Dental Practice: Benefit Versus Risk
The potential benefits to the patient as judged by the imaging diagnostic efficacy of CBCT should be weighed against the potential radiation risks to that particular patient by applying the precautionary principle to eliminate the uncertainty regarding the long-term health concerns of the radiation exposure. This process must be evidence based [12, 48, 51, 54]. Dental practitioners must stay scientifically updated with the ongoing research and development of the CBCT technology, and with the associated potential long-term radiation risks [14–17, 36–38, 40, 55, 60], and apply an evidence-based approach in case selection for performing CBCT [12, 39, 49].
When the decision whether to use CBCT is not based on solid systematic evidence-based foundations, it may lead to misuse or overuse of CBCT, exposing the patient to unnecessary radiation risks without any clinical justification [13, 39]. As an example, it became acceptable and common to use CBCT for the diagnosis of vertical root fractures (VRF), a complex endodontic condition [62], assuming that CBCT is clinically effective for this purpose and that it possesses superior efficacy over conventional radiography [26, 46, 63–76]. Nevertheless, recent published data, including a recent meta-analysis of the literature [25], raises a concern regarding the alleged superiority of CBCT over conventional intraoral radiography for the detection of VRF [24, 25, 27], especially in the presence of metal posts [27]. The exact extent of CBCT scans performed for the diagnosis of VRF is unknown, but is clearly extensive [26]. However, the limited evidence raises a significant concern regarding its clinical effectiveness for the diagnosis of VRFs [12, 13, 24, 25, 27, 39], regarding its superiority over alternative lower-dose conventional dental radiography modalities [13, 24, 25, 27, 39], and regarding its potential ultimate benefit to the patient compared to its potential radiation risks [2, 14–18, 26, 60].
A number of position statements [1, 2, 39] suggested several clinical scenarios when CBCT may be indicated. However, according to the currently available scientific literature on the diagnostic efficacy of CBCT in dentistry, these recommendations are not well supported by a high level of efficacy evaluation [40]. In addition, the caution that is required due to the associated radiation risks of CBCT is commonly presented without a thorough explanation and without adequate implementation of the precautionary principle in light of the uncertainty regarding its possible unknown long-term health risks [12]. Therefore, it is recommended that the selection of patients to be referred to CBCT should be based on an assessment of the need for additional imaging, the benefit of CBCT in that clinical scenario, and the risks of performing CBCT to that particular patient as follows:
-
Need Assessment: Assessment whether the patient’s anamnesis, clinical examination, and lower-dose conventional dental radiography are sufficient or not for the specific diagnostic process
-
Benefit Assessment: Assessment whether the diagnostic efficacy of CBCT is scientifically established, not only for the technical characteristics of the CBCT but also for the efficacy of CBCT to improve the practitioner’s decision making and treatment planning and ultimately the treatment outcomes
-
Benefit Versus Risk Assessment: Assessment whether the potential ultimate benefit to the patient of using CBCT outweighs the potential radiation risks to the particular patient, assessed with the precautionary principle regarding the long-term health concerns of exposure to radiation
The application of these criteria in the case selection for CBCT will ensure the efficient and cautious use of CBCT in dentistry (Fig. 7.3).

Case selection algorithm for CBCT scan in dentistry.1 The diagnostic efficacy of CBCT for the specific clinical situation is scientifically supported not only for the technical characteristics of the CBCT but also for the efficacy of CBCT to support the practitioner’s decision making, the treatment planning, and ultimately the treatment outcome, in that particular clinical scenario.2 The potential radiation risks to the particular patient should be assessed by applying the precautionary principle, considering the uncertainty regarding the long-term health concerns of exposure to radiation
Conclusions
The selection of cases requiring CBCT in dentistry is primarily based on a risk-benefit assessment. The expected ultimate benefit to the patient, as evaluated by the level of diagnostic efficacy of CBCT in dentistry, is not fully elucidated, and it is mainly limited to its technical and the diagnostic accuracy efficacies. Even for these levels of efficacy, evidence is incomplete. On the other hand, the potential radiation risks of CBCT scan are uncertain and stochastic in nature, thus requiring the implementation of the precautionary principle by a preventive clinical approach. Based on these principles, a practical algorithm for the use of CBCT in dentistry is proposed (Fig. 7.3).
References
AAE and AAOMR Joint Position Statement: use of cone beam computed tomography in endodontics. Update 2015.
AAE and AAOMR Joint Position Statement – use of cone-beam-computed tomography in endodontics. 2010.
Pinsky HM, Dyda S, Pinsky RW, Misch KA, Sarment DP. Accuracy of three-dimensional measurements using cone-beam CT. Dentomaxillofac Radiol. 2006;35(6):410–6.
Patel S. New dimensions in endodontic imaging: part 2. Cone beam computed tomography. Int Endod J. 2009;42(6):463–75.
Shah N, Bansal N, Logani A. Recent advances in imaging technologies in dentistry. World J Radiol. 2014;6(10):794–807.
Venskutonis T, Plotino G, Juodzbalys G, Mickeviciene L. The importance of cone-beam computed tomography in the management of endodontic problems: a review of the literature. J Endod. 2014;40:1895–901.
Aljehani YA. Diagnostic applications of cone-beam CT for periodontal diseases. Int J Dent. 2014;2014:865079.
Jaju PP, Jaju SP. Clinical utility of dental cone-beam computed tomography: current perspectives. Clin Cosmet Investig Dent. 2014;6:29–43.
Bornstein MM, Scarfe WC, Vaughn VM, Jacobs R. Cone beam computed tomography in implant dentistry: a systematic review focusing on guidelines, indications, and radiation dose risks. Int J Oral Maxillofac Implants. 2014;29(Suppl):55–77.
Gupta J, Ali SP. Cone beam computed tomography in oral implants. Natl J Maxillofac Surg. 2013;4(1):2–6.
Agrawal JM, Agrawal MS, Nanjannawar LG, Parushetti AD. CBCT in orthodontics: the wave of future. J Contemp Dent Pract. 2013;14(1):153–7.
Rosen E, Taschieri S, Del-Fabbro M, Beitlitum I, Tsesis I. The diagnostic efficacy of cone-beam computed tomography in endodontics: a systematic review and analysis by a hierarchical model of efficacy. J Endod. 2015;41:1008–14.
Patel S, Durack C, Abella F, Shemesh H, Roig M, Lemberg K. Cone beam computed tomography in endodontics- a review. Int Endod J. 2015; 48(1):3–15.
Berrington de Gonzalez A, Mahesh M, Kim KP, Bhargavan M, Lewis R, Mettler F, et al. Projected cancer risks from computed tomographic scans performed in the United States in 2007. Arch Intern Med. 2009;169(22):2071–7.
Brenner D, Elliston C, Hall E, Berdon W. Estimated risks of radiation-induced fatal cancer from pediatric CT. AJR Am J Roentgenol. 2001;176(2):289–96.
Brenner DJ, Hall EJ. Computed tomography--an increasing source of radiation exposure. N Engl J Med. 2007;357(22):2277–84.
Pearce MS, Salotti JA, Little MP, McHugh K, Lee C, Kim KP, et al. Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: a retrospective cohort study. Lancet. 2012;380(9840):499–505.
Rehani MM, Berry M. Radiation doses in computed tomography. The increasing doses of radiation need to be controlled. BMJ. 2000;320(7235):593–4.
Ee J, Fayad MI, Johnson BR. Comparison of endodontic diagnosis and treatment planning decisions using cone-beam volumetric tomography versus periapical radiography. J Endod. 2014;40(7):910–6.
Pittayapat P, Limchaichana-Bolstad N, Willems G, Jacobs R. Three-dimensional cephalometric analysis in orthodontics: a systematic review. Orthod Craniofac Res. 2014;17(2):69–91.
Kim IH, Patel MJ, Hirt SL, Kantor ML. Clinical research and diagnostic efficacy studies in the oral and maxillofacial radiology literature: 1996–2005. Dentomaxillofac Radiol. 2011;40(5):274–81.
Scarfe WC. “All that glitters is not gold”: standards for cone-beam computerized tomographic imaging. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;111(4):402–8.
Kaeppler G, Cornelius CP, Ehrenfeld M, Mast G. Diagnostic efficacy of cone-beam computed tomography for mandibular fractures. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;116(1):98–104.
Chavda R, Mannocci F, Andiappan M, Patel S. Comparing the in vivo diagnostic accuracy of digital periapical radiography with cone-beam computed tomography for the detection of vertical root fracture. J Endod. 2014;40:1524–9.
Corbella S, Del Fabbro M, Tamse A, Rosen E, Tsesis I, Taschieri S. Cone beam computed tomography for the diagnosis of vertical root fractures: a systematic review of the literature and meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol. 2014;118:593–602.
Dailey B, Mines P, Anderson A, M. S. The use of cone beam computer tomography in endodontics: results of a questionnaire. AAE Annual Session abstract presentation; 2010.
Neves FS, Freitas DQ, Campos PS, Ekestubbe A, Lofthag-Hansen S. Evaluation of cone-beam computed tomography in the diagnosis of vertical root fractures: the influence of imaging modes and root canal materials. J Endod. 2014;40:1530–6.
Azim AA, Azim KA, Deutsch AS, Huang GT. Acquisition of anatomic parameters concerning molar pulp chamber landmarks using cone-beam computed tomography. J Endod. 2014;40(9):1298–302.
Matherne RP, Angelopoulos C, Kulild JC, Tira D. Use of cone-beam computed tomography to identify root canal systems in vitro. J Endod. 2008;34(1):87–9.
Metska ME, Liem VM, Parsa A, Koolstra JH, Wesselink PR, Ozok AR. Cone-beam computed tomographic scans in comparison with periapical radiographs for root canal length measurement: an in situ study. J Endod. 2014;40(8):1206–9.
Liang YH, Jiang L, Chen C, Gao XJ, Wesselink PR, Wu MK, et al. The validity of cone-beam computed tomography in measuring root canal length using a gold standard. J Endod. 2013;39(12):1607–10.
Jeger FB, Janner SF, Bornstein MM, Lussi A. Endodontic working length measurement with preexisting cone-beam computed tomography scanning: a prospective, controlled clinical study. J Endod. 2012;38(7):884–8.
Janner SF, Jeger FB, Lussi A, Bornstein MM. Precision of endodontic working length measurements: a pilot investigation comparing cone-beam computed tomography scanning with standard measurement techniques. J Endod. 2011;37(8):1046–51.
Abella F, Patel S, Duran-Sindreu F, Mercade M, Bueno R, Roig M. Evaluating the periapical status of teeth with irreversible pulpitis by using cone-beam computed tomography scanning and periapical radiographs. J Endod. 2012;38(12):1588–91.
Pope O, Sathorn C, Parashos P. A comparative investigation of cone-beam computed tomography and periapical radiography in the diagnosis of a healthy periapex. J Endod. 2014;40(3):360–5.
Pauwels R, Cockmartin L, Ivanauskaite D, Urboniene A, Gavala S, Donta C, et al. Estimating cancer risk from dental cone-beam CT exposures based on skin dosimetry. Phys Med Biol. 2014;59(14):3877–91.
Petersen LB, Olsen KR, Matzen LH, Vaeth M, Wenzel A. Economic and health implications of routine CBCT examination before surgical removal of the mandibular third molar in the Danish population. Dentomaxillofac Radiol. 2015;44(6):20140406.
Wu TH, Lin WC, Chen WK, Chang YC, Hwang JJ. Predicting cancer risks from dental computed tomography. J Dent Res. 2015;94(1):27–35.
ADA, editor The use of cone-beam computed tomography in dentistry. An advisory statement from the American Dental Association Council on Scientific Affairs. Chicago: The American Dental Association Council on Scientific Affairs; 2012.
European-Commission. Radiation protection No 172 Cone beam CT for dental and maxillofacial radiology - Evidence-based guidelines. A report prepared by the SEDENTEXCT project (www.sedentexct.eu.). Luxembourg; 2012.
Fryback DG, Thornbury JR. The efficacy of diagnostic imaging. Med Decis Making. 1991;11(2):88–94.
Krupinski EA, Jiang Y. Anniversary paper: evaluation of medical imaging systems. Med Phys. 2008;35(2):645–59.
Matzen LH, Wenzel A. Efficacy of cone beam computed tomography for assessment of impacted mandibular third molars: a review based on a hierarchical model of evidence. Dentomaxillofac Radiol. 2015;44:20140189.
Carrotte P. Endodontics: part 2 diagnosis and treatment planning. Br Dent J. 2004;197(5):231–8.
Mota de Almeida F, Knutsson K, Flygare L. The impact of cone beam computed tomography (CBCT) on the choice of endodontic diagnosis. Int Endod J. 2015;48:564–72.
Bernardes RA, de Moraes IG, Hungaro Duarte MA, Azevedo BC, de Azevedo JR, Bramante CM. Use of cone-beam volumetric tomography in the diagnosis of root fractures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108(2):270–7.
de Paula-Silva FW, Wu MK, Leonardo MR, da Silva LA, Wesselink PR. Accuracy of periapical radiography and cone-beam computed tomography scans in diagnosing apical periodontitis using histopathological findings as a gold standard. J Endod. 2009;35(7):1009–12.
Gutmann JL. Evidence-based/guest editorial. J Endod. 2009;35:1093.
Mileman PA, van den Hout WB. Evidence-based diagnosis and clinical decision making. Dentomaxillofac Radiol. 2009;38(1):1–10.
Rosenberg W, Donald A. Evidence based medicine: an approach to clinical problem-solving. BMJ. 1995;310(6987):1122–6.
Sutherland SE, Matthews DC. Conducting systematic reviews and creating clinical practice guidelines in dentistry: lessons learned. J Am Dent Assoc. 2004;135(6):747–53.
Patel S, Dawood A, Whaites E, Pitt FT. New dimensions in endodontic imaging: part 1. Conventional and alternative radiographic systems. Int Endod J. 2009;42(6):447–62.
Ludlow JB, Timothy R, Walker C, Hunter R, Benavides E, Samuelson DB, et al. Effective dose of dental CBCT-a meta analysis of published data and additional data for nine CBCT units. Dentomaxillofac Radiol. 2015;44(1):20140197.
Givol N, Rosen E, Taicher S, Tsesis I. Risk management in endodontics. J Endod. 2010;36(6):982–4.
European-Environment-Agency, editor. Late lessons from early warnings: the precautionary principle 1896–2000. Environmental issue report No 22; 2001. Copenhagen: Office for Official Publications of the European Communities; 2001.
Peto J, Decarli A, La Vecchia C, Levi F, Negri E. The European mesothelioma epidemic. Br J Cancer. 1999;79(3–4):666–72.
KHEIFETS LI, HESTER GL, BANERJEE GL. The precautionary principle and EMF: implementation and evaluation. J Risk Res. 2001;4(2):113–25.
Ashton J. “Man has lost the capacity to foresee and to forestall, he will end by destroying the world.” (Albert Schweitzer). J Epidemiol Community Health. 2003;57(5):314.
Berman LH, Hartwell GR. Diagnosis. In: Cohen S, Hargreaves KM, editors. Pathways of the pulp. 9th ed. St. Louis: Mosby; 2006. p. 2–39.
Parker L. Computed tomography scanning in children: radiation risks. Pediatr Hematol Oncol. 2001;18(5):307–8.
Friedland B. Medicolegal issues related to cone beam CT. Semin Orthod. 2009;15:77–84.
Tsesis I, Rosen E, Tamse A, Taschieri S, Kfir A. Diagnosis of vertical root fractures in endodontically treated teeth based on clinical and radiographic indices: a systematic review. J Endod. 2010;36(9):1455–8.
da Silveira PF, Vizzotto MB, Liedke GS, da Silveira HL, Montagner F, da Silveira HE. Detection of vertical root fractures by conventional radiographic examination and cone beam computed tomography – an in vitro analysis. Dent Traumatol. 2013;29:41–6.
Edlund M, Nair MK, Nair UP. Detection of vertical root fractures by using cone-beam computed tomography: a clinical study. J Endod. 2011;37(6):768–72.
Fayad MI, Ashkenaz PJ, Johnson BR. Different representations of vertical root fractures detected by cone-beam volumetric tomography: a case series report. J Endod. 2012;38(10):1435–42.
Ferreira RI, Bahrami G, Isidor F, Wenzel A, Haiter-Neto F, Groppo FC. Detection of vertical root fractures by cone-beam computerized tomography in endodontically treated teeth with fiber-resin and titanium posts: an in vitro study. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;115:e49–57.
Fuss Z, Lustig J, Katz A, Tamse A. An evaluation of endodontically treated vertical root fractured teeth: impact of operative procedures. J Endod. 2001;27(1):46–8.
Hassan B, Metska ME, Ozok AR, van der Stelt P, Wesselink PR. Detection of vertical root fractures in endodontically treated teeth by a cone beam computed tomography scan. J Endod. 2009;35(5):719–22.
Hassan B, Metska ME, Ozok AR, van der Stelt P, Wesselink PR. Comparison of five cone beam computed tomography systems for the detection of vertical root fractures. J Endod. 2010;36(1):126–9.
Kambungton J, Janhom A, Prapayasatok S, Pongsiriwet S. Assessment of vertical root fractures using three imaging modalities: cone beam CT, intraoral digital radiography and film. Dentomaxillofac Radiol. 2012;41(2):91–5.
Metska ME, Aartman IH, Wesselink PR, Ozok AR. Detection of vertical root fractures in vivo in endodontically treated teeth by cone-beam computed tomography scans. J Endod. 2012;38(10):1344–7.
Ozer SY. Detection of vertical root fractures of different thicknesses in endodontically enlarged teeth by cone beam computed tomography versus digital radiography. J Endod. 2010;36(7):1245–9.
Ozer SY. Detection of vertical root fractures by using cone beam computed tomography with variable voxel sizes in an in vitro model. J Endod. 2011;37(1):75–9.
Varshosaz M, Tavakoli MA, Mostafavi M, Baghban AA. Comparison of conventional radiography with cone beam computed tomography for detection of vertical root fractures: an in vitro study. J Oral Sci. 2010;52(4):593–7.
Wang P, He W, Sun H, Lu Q, Ni L. Detection of vertical root fractures in non-endodontically treated molars using cone-beam computed tomography: a report of four representative cases. Dent Traumatol. 2012;28(4):329–33.
Zou X, Liu D, Yue L, Wu M. The ability of cone-beam computerized tomography to detect vertical root fractures in endodontically treated and nonendodontically treated teeth: a report of 3 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;111(6):797–801.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Rosen, E., Allareddy, V., Tsesis, I. (2017). Case Selection for the Use of Cone Beam Computed Tomography in Dentistry Based on Diagnostic Efficacy and Risk Assessment. In: Rosen, E., Nemcovsky, C., Tsesis, I. (eds) Evidence-Based Decision Making in Dentistry. Springer, Cham. https://doi.org/10.1007/978-3-319-45733-8_7
Download citation
DOI: https://doi.org/10.1007/978-3-319-45733-8_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-45731-4
Online ISBN: 978-3-319-45733-8
eBook Packages: MedicineMedicine (R0)