
Abstract
Lateral internal sphincterotomy is performed for patients with chronic anal fissure. This chapter describes indications, essential steps, variations, and complications of this procedure. It provides a detailed template operative note for the procedure.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
Indication
-
Chronic anal fissure
Essential Steps
-
1.
Rectal exam.
-
2.
Inject local anesthetic.
-
3.
Anoscopy.
-
4.
Identify the fissure and curet the base.
-
5.
Identify the intersphincteric groove and make an incision.
-
6.
Elevate and divide fibers of the internal sphincter.
-
7.
Achieve hemostasis.
-
8.
Close the wound.
Note These Variations
-
Prone jackknife vs. lithotomy position vs. left lateral decubitus
-
Longitudinal incision into the anal canal (open technique) on occasion used
Complications
-
Bleeding/hematoma formation
-
Incontinence
-
Recurrence
-
Urinary retention
Template Operative Dictation
Preoperative Diagnosis
Chronic anal fissure
Procedure
Lateral internal sphincterotomy
Postoperative Diagnosis
Same
Indications
This ___-year-old male/female had anal fissure of duration refractory to medical management. Lateral internal sphincterotomy was elected for management.
Description of Procedure
The patient was brought to the operating room. Time-outs were performed using both preinduction and pre-incision safety checklists to verify correct patient, procedure, site, and additional critical information prior to beginning the procedure. General/spinal/monitored care anesthesia was induced. The patient was placed in the prone jackknife/lithotomy/left lateral decubitus position. The perineum was prepped and draped in the usual sterile fashion. Local anesthetic was injected as a perianal/pudendal nerve block. The anus was gently dilated and anoscopy performed to identify the fissure. The anoscope was replaced with a Hill-Ferguson retractor and the base of the fissure scraped with a curet.
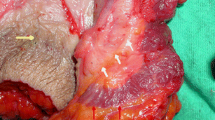
The intersphincteric groove was identified. A short, 4- to 5-mm incision was made directly over the intersphincteric groove on the right/left side. A hemostat was used to dissect the internal sphincter free of anoderm and external sphincter. Fibers were then elevated into the wound using a right-angle clamp and divided with electrocautery/sharp dissection until the hypertrophic sphincter felt relaxed on digital exam. Hemostasis was achieved by holding pressure. The incision was left open to drain. A debriefing checklist was completed to share information critical to postoperative care of the patient.
The patient tolerated the procedure well and was extubated and taken to the postanesthesia care unit in stable condition.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Lorenzo-Rivero, S. (2017). Lateral Internal Sphincterotomy. In: Hoballah, J., Scott-Conner, C., Chong, H. (eds) Operative Dictations in General and Vascular Surgery. Springer, Cham. https://doi.org/10.1007/978-3-319-44797-1_85
Download citation
DOI: https://doi.org/10.1007/978-3-319-44797-1_85
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-44795-7
Online ISBN: 978-3-319-44797-1
eBook Packages: MedicineMedicine (R0)