
Abstract
Excision of subareolar ducts (ductal excision) is performed for nipple discharge, for suspicion of intraductal papilloma, or to eradicate a mammary fistula. This chapter discusses indications, essential steps, technical variations, and complications of this common procedure. It provides a template operative dictation.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
Indications
-
Nipple discharge, suspicion of intraductal papilloma
-
Mammary fistula
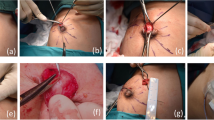
Essential Steps
-
1.
Confirm side of surgery!
-
2.
Cannulate the draining duct with a lacrimal duct probe/0 Prolene.
-
3.
Identify the quadrant to which the probe passes.
-
4.
Circumareolar incision over that quadrant/radially oriented incision including the fistula site.
-
5.
Elevate flaps.
-
6.
Excise the duct distally to termination on the nipple, proximally as far as possible.
-
7.
Orient the specimen.
-
8.
Achieve hemostasis in the cavity.
-
9.
Close the subcutaneous tissue with interrupted 3-0 Vicryl.
-
10.
Close the skin with subcuticular sutures.
Note These Variations
-
Total ductal excision is sometimes needed.
-
When performed for subareolar abscess, use radial incision (including the skin over the fistula site). Leave the tract open if purulence is encountered.
-
If the drainage is scant or difficult to elicit in the clinic, have the patient apply skin glue to the nipple 5 days prior to surgery. This can help to dilate the duct and make it easier to identify intraoperatively. The glue can be carefully peeled off in the operating room.
Complications
-
Hematoma
-
Infection
-
Missed lesion
-
Recurrence
Template Operative Dictation
Preoperative Diagnosis
Right/left nipple discharge
Procedure
Right/left ductal excision
Postoperative Diagnosis
Same
Indications
This ___-year-old female/male with persistent nipple discharge/mammary fistula underwent workup with ultrasound/mammogram/cytology. These showed ___ and ductal excision was recommended for management/diagnosis.
Description of Procedure
The patient was taken to the operating room and placed supine on the operating table and general anesthesia was induced/sedation was given. A time-out was completed verifying correct patient, procedure, site, positioning, and implant(s) and/or special equipment prior to beginning this procedure. The right/left chest and axilla were prepped and draped in the usual sterile fashion. A lacrimal duct probe was used to cannulate the draining duct at the __ o’clock location on the nipple. The relevant quadrant was identified and 1 % lidocaine without epinephrine was used to infiltrate the region. A circumareolar/radially oriented incision was made and flaps were elevated. Using the lacrimal duct probe as a guide, the involved duct was excised sharply from its termination on the nipple with a wedge-shaped portion of the proximal breast tissue. The specimen was oriented and sent to pathology. Additional local anesthesia was infiltrated as needed throughout the case and a total of___ mL of 1 % lidocaine was used.
The wound was irrigated and hemostasis was achieved with electrocautery and suture ligatures of 3-0 Vicryl. The subcutaneous tissue immediately under the skin was approximated with interrupted 3-0 Vicryl sutures. No attempt was made to close the dead space. The breast tissue was approximated with 3-0 Vicryl. The skin was closed with a subcuticular suture of running ___/packed open with ____. A dressing was applied. A debriefing checklist was completed to share information critical to postoperative care of the patient. The patient tolerated the procedure well and was taken to the postanesthesia care unit in stable condition.
Acknowledgment
This chapter was contributed by Carol E.H. Scott-Conner, M.D., in the previous edition.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Splittgerber, B.E., Lizarraga, I. (2017). Excision of Ducts. In: Hoballah, J., Scott-Conner, C., Chong, H. (eds) Operative Dictations in General and Vascular Surgery. Springer, Cham. https://doi.org/10.1007/978-3-319-44797-1_136
Download citation
DOI: https://doi.org/10.1007/978-3-319-44797-1_136
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-44795-7
Online ISBN: 978-3-319-44797-1
eBook Packages: MedicineMedicine (R0)