
Abstract
The umbilicus is a very important component of the abdominal region; therefore, loss of the umbilicus for any reason is a challenging problem. The goal of aesthetically pleasing umbilical reconstruction is to create a neoumbilicus with sufficient depth and good morphology, with natural-looking appearance and minimal scarring.
Various methods for umbilicus reconstruction have been published. Most of these methods are complex, and the surgical outcome is mostly unsatisfactory for the patients. The authors have developed a simple method for umbilicus reconstruction using a bilobed flap.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


1 Introduction
The umbilicus is located at the intersection of the vertical line joining the xiphoid and midpubis and the horizontal line joining the superior iliac crests. It is usually located approximately 9–12 cm above the superior margin of the mons pubis and is an important aesthetic unit of the abdominal wall. The shape is elliptical in vertical direction or T-shaped with the long axis lying vertically in the midline. The umbilical diameter averages 1.5–2 cm [1], with a conical depression whose apex is tethered to the anterior muscular wall.
The umbilicus may be absent because of some congenital anomalies such as gastroschisis, bladder exstrophy, cloacal exstrophy, or omphalocele; inflammatory conditions such as necrotizing fasciitis and umbilical sepsis; and surgical causes such as umbilical herniorrhaphy, skin cancer ablation surgery and also after abdominoplasty, and breast reconstruction using abdominal tissues (Table 20.1). The goal of any reconstructive procedure should be an aesthetically pleasing umbilicus with a natural look and permanent depth [2].
Various methods have been employed in order to reconstruct the umbilicus, including the purse-string method [3], the use of several local flaps [4–10], and the use of an ear conchal cartilage graft [11]. Thomas et al. [12] reported a new technique for reconstruction of the nipple using a local cutaneous flap in the design of an unfolded cylinder. Ozbek and Ozcan [2] modified this method and formed a flap designed as an unfolded horizontal cylinder. We modified these methods and formed a vertical bilobed flap, which is simpler in design. Our method leaves a vertical scar, which is more acceptable, and results in sufficient and permanent depth.
2 Technique
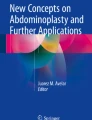
The procedure was performed with the patient under general anesthesia. Before surgical cleaning, the locations of the new umbilicus and the flap were drawn on the abdominal skin (Figs. 20.1, 20.2, and 20.3). A small portion of the skin opposite to the flap pedicle was marked for removal. The pedicle length of the bilobed flap had to be equal to one-third of the vertical flap length. The horizontal length of the flap had to equal the length of the pedicle. The length of the flap pedicle was planned to be 1.5 times the vertical diameter of the neoumbilicus. The flap pedicle would form half of the neoumbilicus circle. The other half would be formed by one of the bilobed flap lobes.

(a) Umbilical bilobed flap design. (b) Bilobed flap x and y elevated. (c) Flap x and y sutured together to create a cylinder formation. Flap x is fixed to the deep fascia to form the bottom of the umbilicus. Lateral side of the flap y forms the umbilical circle. (d) The donor site defect closed by separate sutures

Preoperative patient

Preoperative planning of the flap on the abdominal skin
After surgical cleaning and draping, the edges of the bilobed flap were cut through the subcutaneous adipose layer. The skin flap was elevated enough to permit the formation of a cylinder. After meticulous hemostasis, flaps x and y were sutured together (Fig. 20.1). The base of the cylinder was also sutured. The cylinder then was embedded in its place and fixed to the bottom with 4–0 nonabsorbable sutures. The donor site was closed by separated sutures (Fig. 20.4). The neoumbilicus was filled with a piece of moisture gauze, and the operation site was dressed. After ten days, all sutures were removed. There were no complications such as wound disruption, flap necrosis, hematoma, or infection. After 1 year, sufficient and permanent depth was observed, and the patient was satisfied (Fig. 20.5).

Postoperative

One year postoperative
3 Discussion
Reconstruction of a neoumbilicus is often required after a previous abdominoplasty [8, 11]. The neoumbilicus should have a natural look as well as a sufficient and permanent depth without too many additional scars [8]. The neoumbilicus should be placed 3 cm above the superior iliac spine or at the highest level of the iliac crest [1, 13]. Shinohara [14] described that an umbilicus with a natural appearance consists of a ring, a tubular wall, a sulcus, and a bottom, without any excess skin that would interfere with the aesthetic aspect of the umbilicus. Marconi [6], and later Bartisch and Schwartz [3], described purse-string methods. Although this is a simple method, this technique requires thorough wound care for an extended period, and long-term results have not been described. Borges reported reconstruction by lateral skin excisions and a rotation of two small paramedian flaps [15]. Jamra [4] reconstructed the umbilicus with flaps on a double V-Y pattern. An elliptical skin island with fat excisions underneath and depression created through a purse-string suture was reported by Marconi [6]. Mateu and Hernandez [7] described their technique of depressing three triangular flaps by suturing their vertices to the aponeurotic plane, similar to Kirianoff’s technique, and constructing the inner walls of the neoumbilicus through tightening of a pure-string suture [5].
All the aforementioned techniques may create an umbilicus-like depression, but some have used distant donor sites. Using most of these techniques, the umbilical depth is maintained by the use of a long-term stent. In practice, this is a challenging task for slim patients and pediatric patients. However, with our technique, flap survival is secured, and there is no need for a stent after 2 weeks. The flaps are not under tension if correctly planned. Because the incision lines of the flap lie under minimal tension lines, the final scar also is satisfactory.
In the presented case, there was vertical scar tissue on the midline, which resulted from a previous umbilicus necrosis after abdominoplasty. The bilobed flap was planned laterally to this scar. We believe that removal of some skin portion opposite the flap pedicle helped to centralize the umbilicus. We did not see any lateral displacement after 1 year. We think that for cases in which there is no such vertical or horizontal bad scar, the bilobed flap should be planned with a vertical axis passing from the midline to avoid lateral displacement of the umbilicus. There is no need for a tissue removal.
4 Conclusions
Technically the procedure gives many advantages; being simple and stable, resulting in an acceptable scar, there is no need to use stent. Considering these advantages and the fact that it leads to aesthetically satisfactory results, this technique is widely employed as a useful neoumbilicoplasty technique in patients suffering from an absent or disfigured umbilicus.
References
Dubou R, Ousterout DK. Placement of the umbilicus in an abdominoplasty. Plast Reconstr Surg. 1978;61:291–3.
Ozbek S, Ozcan M. Umbilicus reconstruction with modified unfolded cylinder technique. Br J Plast Surg. 2005;58:500–3.
Bartisch SA, Schwartz MH. Purse-string method for immediate umbilical reconstruction. Plast Reconstr Surg. 2003;112:1652–5.
Jamra FA. Reconstruction of the umbilicus by a double V-Y procedure. Plast Reconstr Surg. 1978;64:106.
Kirianoff TG. Making a neoumbilicus when none exist. Plast Reconstr Surg. 1978;61:603.
Marconi F. Reconstruction of the umbilicus: a simple technique. Plast Reconstr Surg. 1995;95:1115–7.
Mateu LP, Hernandez C. Neoumbilicoplasty through a purse-string suture of three defatted flaps. Aesthetic Plast Surg. 1997;21:349.
Pfulg M, Sijpe KV, Blondeel P. A simple new technique for neoumbilicoplasty. Br J Plast Surg. 2005;58:688–91.
Miller MJ, Balch CM. “Iris” technique for immediate umbilical reconstruction. Plast Reconstr Surg. 1993;92:754–6.
Matsuo K, Kondoh S, Hirose T. A simple technique for reconstruction of the umbilicus, using a conchal cartilage composite graft. Plast Reconstr Surg. 1990;86:149–51.
Friedland JA, Maffi TR. Abdominoplasty. Plast Reconstr Surg. 2008;121:1–11.
Thomas SV, Gellis MB, Pool R. Nipple reconstruction with a new local tissue flap. Plast Reconstr Surg. 1996;97:1053.
Koshy CE, Taams KO. Umbilicoplasty. Plast Reconstr Surg. 1999;104:1203–4.
Shinohara H, Matsuo K, Kikuchi N. Umbilical reconstruction with an inverted C-V flap. Plast Reconstr Surg. 2000;105:703–5.
Borges AF. Reconstruction of the umbilicus. Br J Plast Surg. 1975;28:75–6.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Sevin, A., Keskin, D., Deren, I.O., Sevin, K. (2017). Bilobed Flap for Umbilicus Reconstruction. In: Shiffman, M. (eds) Adult Umbilical Reconstruction. Springer, Cham. https://doi.org/10.1007/978-3-319-43887-0_20
Download citation
DOI: https://doi.org/10.1007/978-3-319-43887-0_20
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-43885-6
Online ISBN: 978-3-319-43887-0
eBook Packages: MedicineMedicine (R0)