
Abstract
Atrial fibrillation (AF) is the most frequent sustained arrhythmia in the elderly. AF is often associated with (and aggravates the clinical course of) several age-related disorders, such as chronic heart failure, non-ST-elevation myocardial infarction, cerebrovascular disease, chronic obstructive pulmonary disease, pneumonia, and urinary infections. Older patients can develop the most severe complications of AF, such as stroke and dementia. Despite existing evidence, oral anticoagulation is still underused in the elderly. A rate-control strategy is frequently adopted. In conclusion, AF in elderly patients is common and often represents a marker of multiple comorbidities and frailty. Management should aim at reducing symptoms and improving health-related quality of life and survival.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


12.1 Introduction
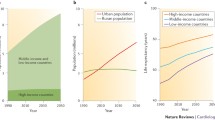
Atrial fibrillation (AF) is the most frequent sustained arrhythmia in the elderly [1, 2] (Fig. 12.1). The Framingham Heart Study, the Cardiovascular Health Study, and the Olmsted County Study all show that the incidence of AF exponentially grows in general population from 60 years of age, reaching 60 cases per 1000 person-years in those age over 80 [4]. The prevalence of arrhythmia follows the same trend. Over 75 and 85 years of age, AF is present in 17 and 23 % of people, respectively [4]. Given the aging population, current projections estimate that by 2060 17.9 million persons will be diagnosed with AF, of these 13.4 million (77.1 %) will be over 75 years of age (Fig. 12.2) [2]. Therefore, AF plays an important role in the elderly due to the associated complications and the resulting disability. In the elderly, the arrhythmia is often silent (up to 27.5 % of cases over 85 years), and optimal prevention strategies may be particularly challenging [5].

Estimated 2010 prevalence of atrial fibrillation in the developed countries participating to the “Global Burden of Disease Study” (Figure drawn by the data reported in Ref. [3])

Estimated numbers of adults with atrial fibrillation in the European Union between 2000 and 2060 (Figure drawn by the data reported in Ref. [2])
12.2 Aging and Changes of Atrial Structure
Aging modifies some characteristics of atrial structure, facilitating the development of AF and increasing the risk of cardio-embolic events. Multi-slice CT imaging studies have shown that the end-systolic diameter of the left atrium progressively increases from 30 mm for ages ≤40 years to 48 mm in those over 80 years (Fig. 12.3) [6]. The thickness of the anterior left atrium also increases from 2 to 3.7 mm. The Framingham Heart Study has recently confirmed, in a longitudinal analysis, that the size of the left atrium increases progressively with age, in both sexes, by approximately 0.6 mm per decade [7]. These modifications can partially be attenuated through the control of some cardiovascular risk factors such as obesity and hypertension [7]. In uncontrolled hypertension, the atrial diameter increases with age by 50 %, at a rate of 0.9 mm per decade [7]. Aging changes both the geometry and structure of the atrial myocardium. In addition, biopsy samples obtained during cardiac surgery have shown an age-related increase of the connective-fibrous tissue, from 10 % of atrial mass in subjects <50 years to 17 % in subjects >70 years [8]. Tissue acetylcholinesterase, a marker of the autonomic nervous system activity, also decreases with age, in association with a decrease in number and extension of nerve fibers [9]. The ostium of the left atrium auricula and the diameter of the pulmonary veins become progressively larger, growing from 12 to 28 mm and from 10 to 24, respectively, between age 30 and 90 years [6].

Left atrium dimensions gradually increase with age. The number of subjects in whom the measure was obtained is reported in brackets (Figure drawn by the data reported in Ref. [6])
In conclusion, the atria seem to encounter a real aging process (“wrinkles in the atrium”) that could justify the increased incident risk of AF in the elderly [10]. Whether age, increase in atrial size, degree of fibrosis, and presence of arrhythmia are causes, effect or epiphenomenon of extra-cardiac alterations still needs to be clarified [10].
12.3 Aging and Risk of Stroke and Systemic Cardio-embolism
Epidemiological studies have shown that, with AF, the incidence of cardio-embolic stroke increases exponentially with age [1, 11]. In a registry study conducted in Dijon, for example, the incidence of cardio-embolic stroke was 28 per 100,000 person-years in men aged 50–60 years and 216 per 100,000 person-years in men >80 years [11]. At advanced ages, the incidence of disease is higher in women [11]. A recent UK community survey showed that the incidence of cardio-embolic stroke was as high as 12.7 per 1000 per year in AF women ≥90 years [12] (Fig. 12.4). About 20 % of all ischemic strokes are AF related [11].

Age-specific rates of a first AF-related incident ischemic stroke and systemic embolism (SE) in the Oxford Vascular Study. The results derive from the experience of about 100 family doctors (nine general UK practices) participating between 2002 and 2012 (M men, W women) (Figure drawn by the data reported in Ref. [12])
Furthermore, the incidence of cryptogenic stroke progressively increases with age, representing, in >75 years patients, the second cause of disease [13]. The use of loop recorders, allowing long EKG monitoring, demonstrated that 25.5 % of all cryptogenic strokes could be attributed to AF [14]. Asymptomatic forms of arrhythmia play an important role in the genesis of silent cerebrovascular disease in type 2 diabetic patients [15].
The European Community Stroke Project Study, which enrolled 4462 subjects, with a first ischemic stroke, demonstrated that patients with cardio-embolism had a more severe form of disease [16] with a greater incidence of delirium, coma, motor impairment, aphasia, dysphagia, and urinary incontinence [16] and higher in-hospital and short- (3 months, 32.8 vs. 19.9 %, p <0.001) and long-term (2 years, 57 vs. 31 %, p <0.001) mortality [11, 16].
Thus, survivors of AF-related strokes are at increased risk of disability and more frequently need assistance in basic activities of daily living and institutionalization in nursing homes [16]. AF-related disability-adjusted life years progressively increase with age [3]. The higher severity of cardio-embolic stroke can be explained by the more frequent involvement of the anterior portion of the circle of Willis [16]. All these reasons support the fact that age is one of the most important variables linked to AF-related stroke [17].
The incidence of systemic cardio-embolism (SE) was 0.24 per 100 patient-years (11.5 % of all cardio-embolic events), involving lower limbs and renal and mesenteric circulation. SE mortality was 25 %, while 20 % of survivors had some kind of residual disability [18].
12.4 AF and Chronic Kidney Disease
The prevalence of chronic kidney disease increases with age, ranging from 20 % in subjects aged 60–69 years to over 45 % in subjects >70 years. In the Atherosclerosis Risk Communities Study (ARIC), a cohort of 10.328 subjects, after a 10-year follow-up, the risk of developing AF was independently associated with renal function [19]. When compared to those with a normal glomerular filtration rate (GFR), the relative risk of developing new arrhythmic events was 1.57 and 2.84 higher in those with a GFR of 30–59 and 15–29 ml, respectively [19].
The Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study showed that in 11,527 AF patients, followed up from 1996 to 2003, the incidence of cardio-embolism was directly related to the degree of chronic renal impairment, increasing from 1.63 to 4.22 events per 100 person-years for GFR values ranging from ≥60 to <45 ml/min/1.73 m2 [20]. Recently, a large Danish cohort study has further clarified the relationship between AF, chronic kidney disease, and clinical outcomes in 132,732 patients, hospitalized between 1997 and 2008 with a diagnosis of AF [21]. The prevalence of non-end-stage and end-stage kidney failure was 2.7 % and 0.9 %, respectively. During follow-up, the incidence of ischemic stroke and cardio-embolic events was higher with impaired kidney function, with a relative risk of 1.49 and 1.83 in patients with non-end-stage disease and in those requiring dialysis. A similar trend was observed for risk of myocardial infarction and major bleeding [21]. Total mortality was higher in AF patients with impaired kidney function [21].
These evidences led the investigators of ROCKET AF trial to elaborate and validate the R2CHADS2 score, in which two additional points are assigned in subjects with chronic renal failure, defined by a GFR < 60 ml/min [22]. Even if this score presents some limitations (it was derived in a selected trial cohort that excluded patients with severe renal impairment or presenting some risk of stroke) [23], it reflects the awareness that AF patients with chronic renal failure have a higher risk of thromboembolism and major bleeding [23].
12.5 AF and Peripheral Artery Disease
The prevalence of peripheral artery disease is high among AF patients [24], and, in a review of ten observational studies, it was found to be associated with a 1.3–2.5 times greater stroke risk [25].
Less is known about the mechanisms linking the condition to arrhythmia development. In the Framingham Heart Study, the incidence of AF on a median follow-up of 12 years was 13.1 % (N = 698/5331), and it was lower in those with a pulse pressure ≤40 mmHg than in those with a pulse pressure >61 mmHg (5.6 vs. 23.3 %). After multivariate adjustment, pulse pressure, but not mean arterial pressure, was associated with an increased risk of arrhythmia development [26]. The observational “Atrial Fibrillation Registry for Ankle-Brachial Index Prevalence Assessment-Collaborative Italian Study” (ARAPACIS), conducted on 2027 patients, analyzed the relation between peripheral arterial disease and non-valvular AF. The study showed that abnormal ankle-brachial index (ABI) values (≤0.90) are found in 21 % of AF patients and have a direct association with the arrhythmic burden [27]. A higher prevalence of a previous ischemic stroke was observed in patients with a pathologic ABI when compared to those with a normal one (17 vs. 10 %, p < 0.001) [27]. Later, the same study found that an ABI ≤ 0.90 was an independent predictor of vascular events, vascular death, and MI [28]. More recently, arterial stiffness was found to be an independent predictor of left atrium dimensions even after adjustment for interventricular septum thickness [29]. Hence, aortic mechanical characteristics, possibly through inflammation cascade, could play a role in promoting and maintaining AF [29, 30].
12.6 AF and Dementia
The incident risk of dementia is about twice higher in patients with AF. In a cohort of 6584 subjects, the Rotterdam Study investigators reported that AF prevalence increased with the severity of cognitive impairment, from 2.1 % in normal cognitive status to 6 and 13 % in mild cognitive impairment and dementia [31]. The Olmsted County Study confirmed this association [32].
More recently, the Cardiovascular Health Study evaluated in a longitudinal analysis the changes in cognitive profile of the 5150 participants enrolled between 1989 and 1993. During a mean follow-up of 7 years, cognitive performance test (assessed by a modified version of the Mini-Mental State Examination) decreased progressively with age. The presence of AF was associated with a higher score reduction in those older than 75 years [33] (Fig. 12.5). These data confirm the observations of “The Adult Changes in Thought Study,” where the incidence of dementia had a 38 % risk increase in arrhythmic patients, growing from 25 to 47.9 events per 1000 person-years [34].

Predicted trajectories of the “modified Mini-Mental State Examination” (3MSE) in the Cardiovascular Health Study (CHS) participants. An incident atrial fibrillation determines a steeper decline of cognitive function. The 3MSE score ranges between 0 (worst) and 100 (best performance) (Adapted from Ref. [33]. (License by Wolters Kluwer Health, Inc.))
A meta-analysis of observational studies showed an association between AF and dementia in the subgroup of patients with a previous stroke (OR = 2.4) [35]. In an extensive review of literature, eight out of 11 studies published between 1990 and 2012 (three cross-sectional, two case-control, and three prospective cohorts) were found to report a significant correlation between cognitive decline and the arrhythmia. Among cross-sectional studies, patients with AF had a 1.7 to a 3.3 greater risk of cognitive impairment, and a 2.3-fold increased risk of dementia, compared to those in sinus rhythm [36].
All these findings would suggest that the arrhythmia could produce cognitive changes not only through cardio-embolic events but also through the increased production of beta-amyloid [35]. Evidence shows a possible pathway linking vascular disease to reduced beta-amyloid clearance, which would determine a further worsening of vascular disease. This mechanism, sustained by protein tau hyper-phosphorylation, would result in white and gray matter reduction [37]. Furthermore, variation in the concentration of inflammatory mediators could help to explain the association between the arrhythmia and the risk of dementia. Beside a higher CPR level, AF patients show higher concentrations of pro- (e.g., interferon, interleukin-1, interleukin-6, tumor necrosis factor-α) and anti-inflammatory (e.g., transforming growth factor-β) cytokines. Similar changes can be also observed in dementia [38].
12.7 Anticoagulant Therapy in Elderly AF Patients
Oral anticoagulant therapy (OAT) with vitamin K antagonists proved to be extremely effective in reducing the incidence of cardio-embolism in patients with non-valvular AF. A meta-analysis of the original historical trials demonstrated that OAT, compared to placebo, reduces the risk of stroke by 62 % and all-cause mortality by 26 % [39, 40]. The benefit of OAT is also significantly higher compared to that of aspirin, with a 36 % additional risk reduction [39, 40].
The “Birmingham Atrial Fibrillation Treatment of the Aged Study” (BAFTA) first explored the effects of OAT, compared with aspirin, in the elderly (inclusion criteria, age ≥75 years). After a mean follow-up of 2.7 years, in the 973 patients enrolled (mean age 81.5 years), OAT significantly reduced the combined risk of stroke, cardio-embolism, and intracranial hemorrhage compared to aspirin (1.8 vs. 3.8 % per year, RR = 0.48; p = 0.003) [41].
Subsequently, a sub-analysis of ATRIA study analyzed in 13,559 patients the net clinical benefit (avoided ischemic stroke – provoked hemorrhagic strokes) of OAT by age group. Interestingly, the benefit of anticoagulation increased with age, reaching the statistical significance for those aged 75–84 and ≥85 years [42]. In the “Loire Valley Atrial Fibrillation Project,” which enrolled 4832 patients <75 years and 4130 patients ≥75 years, the benefit of warfarin vs. placebo to prevent stroke, thromboembolism, and mortality was maintained through all age strata, even in subjects older than 85 and 90 years [43] (Fig. 12.6).

The influence of warfarin (W) on all-cause mortality in “The Loire Valley Atrial Fibrillation Project” by age-group (<75 vs. ≥75 years) (upper panel). The benefit of therapy (vitamin K antagonist, VKA) is maintained independently of age even in subjects aged >90 years (lower panel). (HR hazard ratio) (Adapted from Ref. [43]. (License by Wolters Kluwer Health, Inc.))
As shown in a Swedish registry enrolling 182,678 subjects, the risk of cardio-embolism was progressively higher for increasing scores not only of CHA2DS2-VASc but also of the HAS-BLED, the instrument used to assess the bleeding risk [44].
In addition, the results of an Italian prospective multicenter registry enrolling 4093 elderly patients (mean age, 84 years) receiving anticoagulants for AF or deep vein thrombosis showed that bleeding could be minimized (1.87 events per 100 patient.years) by the adoption of tight monitoring protocols [45]. In multivariate analysis, the incidence of hemorrhagic events was associated with the presence of deep vein thrombosis, prior bleeding, an active cancer, and a history of falls [45].
Despite all these findings recommending the adoption of the OAT in elderly AF patients, anticoagulation is still largely underused at older ages. Data from the Euro Heart Survey on Atrial Fibrillation study showed that among 5329 enrolled patients, the use of vitamin K antagonists significantly decreased with age, going from 64 % in the < 65 years group to 56 % in the > 80 years group [46]. These findings were later confirmed by the results of the EURObservational Research Programme-Atrial Fibrillation General Pilot Registry [47]. Moreover, time in the therapeutic range (TTR) was found to be associated with cognitive performance, measured by the Mini-Mental State Examination [48]. Conversely, during follow-up of AF patient with normal cognitive status at baseline, incidence of dementia progressively increases with lower values of TTR [49].
12.8 Non-VKA Oral Anticoagulants
Compared to warfarin, non-VKA oral anticoagulants (NOACs) are characterized by a more foreseeable biological effect, due to their pharmacokinetic and pharmacodynamic characteristics, a reduced interaction with drugs and food, as well as a better safety profile. All randomized controlled trials demonstrated a reduced incidence of intracranial hemorrhage [50–55]. The elderly (age > 75 years) subgroup in the RE-LY study (Randomized Evaluation of Long-Term Anticoagulation Therapy), in the ROCKET AF study (Rivaroxaban Once Daily Oral Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation), in the ARISTOTLE study (Apixaban for Reduction in Stroke and Other Events in Atrial ThromboemboLic Fibrillation) and in the ENGAGE AF-TIMI 48 trial (The Effective Anticoagulation with Factor Xa Next Generation in Atrial Fibrillation-Thrombolysis in Myocardial Infarction 48 trial) were, respectively, 40, 38, 31, and 40 % of all enrolled patients. The subgroup analysis showed no significant age-related differences in the primary efficacy outcome (new cases of stroke and cardio-embolism) compared to warfarin [50–55]. The incidence of major bleeding, with both rivaroxaban and apixaban, did not show any age-related differences [52–54]. Apixaban consistently reduced major bleeding across all age groups [56]. In older patients treated with dabigatran, the incidence of major hemorrhage was not different between dabigatran 110 and 150 mg twice a day, while intracranial hemorrhage was lower in dabigatran 110 mg twice a day, which represent the current recommended dose in the elderly [51, 54].
In a meta-analysis of RE-LY, ROCKET AF, and ARISTOTLE studies, NOACs compared to warfarin were associated with a lower incidence of intracranial hemorrhage (relative risk reduction, RRR −51 %), with similar incidence of systemic major bleeding [57]. Moreover the combined effect of the three molecules, on prevention of all cardio-embolic events, showed RRR of 22 %, compared to warfarin [57]. A meta-analysis of the ten major randomized controlled clinical trials on NOACs, including only over 75 years patients, found that the risk of major or clinically relevant bleeding did not differ between NOACs and conventional therapy (6.4 vs. 6.3 %, OR = 1.02, 95 % CI = 0.73–1.43). Importantly, the incidence of stroke and other thromboembolic events was significantly reduced (3.3 vs. 4.7 %, OR = 0.65, 95 % CI = 0.48–0.87), with a number needed to treat of 71 [58].
The use of NOACs in patients with kidney impairment is a matter of particular importance in elderly patients, considering the high prevalence of the condition [59], and the significantly increased risk associated with both cardio-embolism [20, 21] and hemorrhage [60]. The European Heart Rhythm Association (EHRA) recommendations suggest that NOACs are reasonable choice in patients with mild-to-moderate chronic kidney impairment [61]. Present EHRA guidelines do not recommend dabigatran, which is mainly excreted by kidneys, for GFR lower < 30 ml/min [61]. In ROCKET AF, 20.7 % of patients had a GFR between 30 and 49 ml/min; their mean age was higher (79 vs. 71 years). There was no interaction between degree of kidney impairment, efficacy, and safety of the drug. Fatal bleeding had a lower incidence in rivaroxaban-treated patients (0.28 vs. 0.74 per 100 patient.years; p = 0.047) [52, 62]. A sub-analysis of ARISTOTLE study confirmed that GFR ≤50 ml/min (17 % of the enrolled subjects, mean age 77.6 years) did not affect the efficacy of apixaban. The benefit in terms of major bleeding events was even found to be higher in the presence of kidney impaired function, with an RRR higher than 50 % when compared to the warfarin [53, 63]. Based on these evidences, EHRA therefore recommends the use of rivaroxaban and apixaban, at reduced doses, up to GFR of 15 ml/min [61].
In a real-world scenario, in 134,414 Medicare patients, dabigatran, when compared to warfarin, was associated with a reduction of stroke incidence (HR = 0.80, 95 % CI = 0.67–0.96), intracranial hemorrhages (HR = 0.34, 95 % CI = 0.26–0.46), and hence mortality (HR = 0.86, 95 % CI = 0.77–0.96). Only gastrointestinal bleeding had a higher incidence in women ≥75 years and in men >84 years [64]. Recent data seem to demonstrate that older patients treated with NOACs have greater psychological satisfaction, lower therapy-related burden, higher awareness of benefits, and lower psychological stress [65].
12.9 Rhythm and Rate Control of AF in Elderly Patients
Real-world data from the EURObservational Research Programme-Atrial Fibrillation General Pilot Registry show that the use of rate-control strategy was more frequently adopted in the elderly, with lower proportions of electrical cardioversion, transcatheter ablation, and prescription of antiarrhythmic drugs. Among rate-control agents, while beta- blockers were prescribed regardless of age, digoxin and nondihydropyridine calcium channel blockers were more often used in older patients [47]. These findings are partially motivated by the results of a sub-analysis of the “Atrial Fibrillation Follow-Up Investigation of Rhythm Management Study” (AFFIRM) which, in patients between 70 and 80 years of age, showed that rate control, compared to rhythm control of AF, was associated with lower mortality and hospitalization rates [66]. However, the evidence is conflicting. In a sub-analysis, the AFFIRM investigators found that, in the follow-up, the presence of sinus rhythm was associated with a lower risk of death, as was warfarin use. Conversely, the use of antiarrhythmic drugs was linked to increased mortality [67].
The incidence of adverse events related to antiarrhythmic drug therapy constitutes an important clinical issue. Patients treated with amiodarone, the most effective agent to prevent AF recurrences, present more complications compared to those receiving propafenone or sotalol (18 vs. 11 %, p = 0.06) [68]. Recent findings from the ARISTOTLE study showed that, in warfarin treated subjects, amiodarone lowers TTR [69]. A meta-analysis demonstrated that the number needed to harm ranges between 9 for quinidine and 27 for amiodarone, propafenone, and sotalol [70].
Nevertheless, also drugs used for the rate-control strategy were found to be not surely effective. A wide AF cohort showed that the risk of mortality was lower for patients receiving β-blockers or calcium channel blockers, with β-blockers determining the largest risk reduction, whereas digoxin use was associated with greater mortality [71]. However, in a meta-analysis of ten studies evaluating the influence of beta-blockers in heart failure patients, there were no benefits in terms of survival and hospitalization in the presence of AF [72]. In a population study, the use of digoxin in elderly patients with AF increased mortality independently from heart failure [73]. Findings from a sub-analysis of the “Dutch Rate Control Efficacy in Permanent AF: A Comparison Between Lenient Versus Strict Rate Control II trial” showed that digoxin therapy did not increase morbidity, hospitalization rates, and mortality [74].
Regarding invasive procedures, some observations seem to demonstrate that AF ablation could be also suitable over 75 years in appropriately selected patients. After a mean follow-up of 3 years, compared to those receiving medical therapy, ablated subjects were more often in sinus rhythm (83 vs. 22 %, p < 0.001) and had lower incidence of stroke and bleeding and higher life expectancy at 1 and 5 years [75]. Furthermore, AF ablation was associated with improved functional status and health-related quality of life [76].
Conclusions
In elderly patients, AF represents an important clinical issue. The coexistence of anatomic changes and comorbidities greatly increases the prevalence of the arrhythmia, which, especially in older individuals, more often determines stroke and dementia. AF frequently worsens the course of common conditions in the elderly, such as chronic heart failure, pneumonia, non-ST-elevation myocardial infarction, and urinary infections [77, 78]. Thus, in aged patients a comprehensive management of the arrhythmia should aim not at the simple control of rhythm or rate but at reducing morbidity and at improving health-related quality of life and survival.
References
Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics-2016 update: a report from the American Heart Association. Circulation. 2016;133:e38–360.
Krijthe BP, Kunst A, Benjamin EJ, et al. Projections on the number of individuals with atrial fibrillation in the European Union, from 2000 to 2060. Eur Heart J. 2013;34:2746–51.
Chugh SS, Havmoeller R, Narayanan K, et al. Worldwide epidemiology of atrial fibrillation: a Global Burden of Disease 2010 Study. Circulation. 2014;129:837–47.
Miyasaka Y, Barnes ME, Gersh BJ, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 2006;114:119–25.
Collerton J, Davies K, Jagger C, et al. Health and disease in 85 year olds: baseline findings from the Newcastle 85+ cohort study. BMJ. 2009;339:b4904. doi:10.1136/bmj.b4904.:b4904.
Pan NH, Tsao HM, Chang NC, Chen YJ, Chen SA. Aging dilates atrium and pulmonary veins: implications for the genesis of atrial fibrillation. Chest. 2008;133:190–6.
McManus DD, Xanthakis V, Sullivan LM, et al. Longitudinal tracking of left atrial diameter over the adult life course: clinical correlates in the community. Circulation. 2010;121:667–74.
Gramley F, Lorenzen J, Knackstedt C, et al. Age-related atrial fibrosis. Age (Dordr). 2009;31:27–38.
Burkauskiene A, Mackiewicz Z, Virtanen I, Konttinen YT. Age-related changes in myocardial nerve and collagen networks of the auricle of the right atrium. Acta Cardiol. 2006;61:513–8.
Asirvatham SJ, Gard JJ. Wrinkles in the atrium: age, atrial fibrillation, or something else. J Am Coll Cardiol. 2011;58:2233–5.
Bejot Y, Ben Salem D, Osseby GV, et al. Epidemiology of ischemic stroke from atrial fibrillation in Dijon, France, from 1985 to 2006. Neurology. 2009;72:346–53.
Yiin GS, Howard DP, Paul NL, et al. Age-specific incidence, outcome, cost, and projected future burden of atrial fibrillation-related embolic vascular events: a population-based study. Circulation. 2014;130:1236–44.
Leyden JM, Kleinig TJ, Newbury J, et al. Adelaide stroke incidence study: declining stroke rates but many preventable cardioembolic strokes. Stroke. 2013;44:1226–31.
Cotter PE, Martin PJ, Ring L, Warburton EA, Belham M, Pugh PJ. Incidence of atrial fibrillation detected by implantable loop recorders in unexplained stroke. Neurology. 2013;80:1546–50.
Marfella R, Sasso FC, Siniscalchi M, et al. Brief episodes of silent atrial fibrillation predict clinical vascular brain disease in type 2 diabetic patients. J Am Coll Cardiol. 2013;62:525–30.
Lamassa M, Di Carlo A, Pracucci G, et al. Characteristics, outcome, and care of stroke associated with atrial fibrillation in Europe: data from a multicenter multinational hospital-based registry (The European Community Stroke Project). Stroke. 2001;32:392–8.
Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010;137:263–72.
Bekwelem W, Connolly SJ, Halperin JL, et al. Extracranial systemic embolic events in patients with nonvalvular atrial fibrillation: incidence, risk factors, and outcomes. Circulation. 2015;132:796–803.
Alonso A, Lopez FL, Matsushita K, et al. Chronic kidney disease is associated with the incidence of atrial fibrillation: the Atherosclerosis Risk in Communities (ARIC) study. Circulation. 2011;123:2946–53.
Go AS, Fang MC, Udaltsova N, et al. Impact of proteinuria and glomerular filtration rate on risk of thromboembolism in atrial fibrillation: the anticoagulation and risk factors in atrial fibrillation (ATRIA) study. Circulation. 2009;119:1363–9.
Olesen JB, Lip GY, Kamper AL, et al. Stroke and bleeding in atrial fibrillation with chronic kidney disease. N Engl J Med. 2012;367:625–35.
Piccini JP, Stevens SR, Chang Y, et al. Renal dysfunction as a predictor of stroke and systemic embolism in patients with nonvalvular atrial fibrillation: validation of the R(2)CHADS(2) index in the ROCKET AF (Rivaroxaban Once-daily, oral, direct factor Xa inhibition Compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation) and ATRIA (AnTicoagulation and Risk factors In Atrial fibrillation) study cohorts. Circulation. 2013;127:224–32.
Boriani G, Savelieva I, Dan GA, et al. Chronic kidney disease in patients with cardiac rhythm disturbances or implantable electrical devices: clinical significance and implications for decision making-a position paper of the European Heart Rhythm Association endorsed by the Heart Rhythm Society and the Asia Pacific Heart Rhythm Society. Europace. 2015;17:1169–96.
Jover E, Marin F, Roldan V, Montoro-Garcia S, Valdes M, Lip GY. Atherosclerosis and thromboembolic risk in atrial fibrillation: focus on peripheral vascular disease. Ann Med. 2013;45:274–90.
Anandasundaram B, Lane DA, Apostolakis S, Lip GY. The impact of atherosclerotic vascular disease in predicting a stroke, thromboembolism and mortality in atrial fibrillation patients: a systematic review. J Thromb Haemost. 2013;11:975–87.
Mitchell GF, Vasan RS, Keyes MJ, et al. Pulse pressure and risk of new-onset atrial fibrillation. JAMA. 2007;297:709–15.
Violi F, Davi G, Hiatt W, et al. Prevalence of peripheral artery disease by abnormal ankle-brachial index in atrial fibrillation: implications for risk and therapy. J Am Coll Cardiol. 2013;62:2255–6.
Violi F, Davi G, Proietti M, et al. Ankle-Brachial Index and cardiovascular events in atrial fibrillation. The ARAPACIS Study. Thromb Haemost. 2016;115:856–63.
Fumagalli S, Gabbai D, Nreu B, et al. Age, left atrial dimension and arterial stiffness after external cardioversion of atrial fibrillation. A vascular component in arrhythmia maintenance? Results from a preliminary study. Aging Clin Exp Res. 2014;26:327–30.
Paulus WJ, Tschope C. A novel paradigm for heart failure with preserved ejection fraction: comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J Am Coll Cardiol. 2013;62:263–71.
Ott A, Breteler MM, de Bruyne MC, van Harskamp F, Grobbee DE, Hofman A. Atrial fibrillation and dementia in a population-based study. The Rotterdam Study. Stroke. 1997;28:316–21.
Miyasaka Y, Barnes ME, Petersen RC, et al. Risk of dementia in stroke-free patients diagnosed with atrial fibrillation: data from a community-based cohort. Eur Heart J. 2007;28:1962–7.
Thacker EL, McKnight B, Psaty BM, et al. Atrial fibrillation and cognitive decline: a longitudinal cohort study. Neurology. 2013;81:119–25.
Dublin S, Anderson ML, Haneuse SJ, et al. Atrial fibrillation and risk of dementia: a prospective cohort study. J Am Geriatr Soc. 2011;59:1369–75.
Kwok CS, Loke YK, Hale R, Potter JF, Myint PK. Atrial fibrillation and incidence of dementia: a systematic review and meta-analysis. Neurology. 2011;76:914–22.
Udompanich S, Lip GY, Apostolakis S, Lane DA. Atrial fibrillation as a risk factor for cognitive impairment: a semi-systematic review. QJM. 2013;106:795–802.
Swardfager W, Black SE. Coronary artery calcification: a canary in the cognitive coalmine. J Am Coll Cardiol. 2016;67:1023–6.
Leonard BE. Inflammation, depression and dementia: are they connected? Neurochem Res. 2007;32:1749–56.
Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146:857–67.
Sellers MB, Newby LK. Atrial fibrillation, anticoagulation, fall risk, and outcomes in elderly patients. Am Heart J. 2011;161:241–6.
Mant J, Hobbs FD, Fletcher K, et al. Warfarin versus aspirin for stroke prevention in an elderly community population with atrial fibrillation (the Birmingham Atrial Fibrillation Treatment of the Aged Study, BAFTA): a randomised controlled trial. Lancet. 2007;370:493–503.
Singer DE, Chang Y, Fang MC, et al. The net clinical benefit of warfarin anticoagulation in atrial fibrillation. Ann Intern Med. 2009;151:297–305.
Lip GY, Clementy N, Pericart L, Banerjee A, Fauchier L. Stroke and major bleeding risk in elderly patients aged >/=75 years with atrial fibrillation: the Loire Valley atrial fibrillation project. Stroke. 2015;46:143–50.
Friberg L, Rosenqvist M, Lip GY. Net clinical benefit of warfarin in patients with atrial fibrillation: a report from the Swedish atrial fibrillation cohort study. Circulation. 2012;125:2298–307.
Poli D, Antonucci E, Testa S, Tosetto A, Ageno W, Palareti G. Bleeding risk in very old patients on vitamin K antagonist treatment: results of a prospective collaborative study on elderly patients followed by Italian Centres for Anticoagulation. Circulation. 2011;124:824–9.
Fumagalli S, Nieuwlaat R, Tarantini F, et al. Characteristics, management and prognosis of elderly patients in the Euro Heart Survey on atrial fibrillation. Aging Clin Exp Res. 2012;24:517–23.
Fumagalli S, Said S, Laroche C, et al. Age-related differences in presentation, treatment, and outcome of patients with atrial fibrillation in Europe: The EORP-AF general pilot registry (EUR Observational Research Programme-Atrial Fibrillation). JACC Clin Electrophysiol. 2015;1:326–34.
Flaker GC, Pogue J, Yusuf S, et al. Cognitive function and anticoagulation control in patients with atrial fibrillation. Circ Cardiovasc Qual Outcomes. 2010;3:277–83.
Jacobs V, Woller SC, Stevens S, et al. Time outside of therapeutic range in atrial fibrillation patients is associated with long-term risk of dementia. Heart Rhythm. 2014;11:2206–13.
Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361:1139–51.
Eikelboom JW, Wallentin L, Connolly SJ, et al. Risk of bleeding with 2 doses of dabigatran compared with warfarin in older and younger patients with atrial fibrillation: an analysis of the randomized evaluation of long-term anticoagulant therapy (RE-LY) trial. Circulation. 2011;123:2363–72.
Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365:883–91.
Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365:981–92.
Deedwania PC. New oral anticoagulants in elderly patients with atrial fibrillation. Am J Med. 2013;126:289–96.
Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013;369:2093–104.
Halvorsen S, Atar D, Yang H, et al. Efficacy and safety of apixaban compared with warfarin according to age for stroke prevention in atrial fibrillation: observations from the ARISTOTLE trial. Eur Heart J. 2014;35:1864–72.
Miller CS, Grandi SM, Shimony A, Filion KB, Eisenberg MJ. Meta-analysis of efficacy and safety of new oral anticoagulants (dabigatran, rivaroxaban, apixaban) versus warfarin in patients with atrial fibrillation. Am J Cardiol. 2012;110:453–60.
Sardar P, Chatterjee S, Chaudhari S, Lip GY. New oral anticoagulants in elderly adults: evidence from a meta-analysis of randomized trials. J Am Geriatr Soc. 2014;62:857–64.
Coresh J, Selvin E, Stevens LA, et al. Prevalence of chronic kidney disease in the United States. JAMA. 2007;298:2038–47.
Pisters R, Lane DA, Nieuwlaat R, de Vos CB, Crijns HJ, Lip GY. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey. Chest. 2010;138:1093–100.
Heidbuchel H, Verhamme P, Alings M, et al. Updated European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist anticoagulants in patients with non-valvular atrial fibrillation. Europace. 2015;17:1467–507.
Fox KA, Piccini JP, Wojdyla D, et al. Prevention of stroke and systemic embolism with rivaroxaban compared with warfarin in patients with non-valvular atrial fibrillation and moderate renal impairment. Eur Heart J. 2011;32:2387–94.
Hohnloser SH, Hijazi Z, Thomas L, et al. Efficacy of apixaban when compared with warfarin in relation to renal function in patients with atrial fibrillation: insights from the ARISTOTLE trial. Eur Heart J. 2012;33:2821–30.
Graham DJ, Reichman ME, Wernecke M, et al. Cardiovascular, bleeding, and mortality risks in elderly Medicare patients treated with dabigatran or warfarin for nonvalvular atrial fibrillation. Circulation. 2015;131:157–64.
Fumagalli S, Cardini F, Roberts AT, et al. Psychological effects of treatment with new oral anticoagulants in elderly patients with atrial fibrillation: a preliminary report. Aging Clin Exp Res. 2015;27:99–102.
Shariff N, Desai RV, Patel K, et al. Rate-control versus rhythm-control strategies and outcomes in septuagenarians with atrial fibrillation. Am J Med. 2013;126:887–93.
Corley SD, Epstein AE, DiMarco JP, et al. Relationships between sinus rhythm, treatment, and survival in the Atrial Fibrillation Follow-Up Investigation of Rhythm Management (AFFIRM) Study. Circulation. 2004;109:1509–13.
Roy D, Talajic M, Dorian P, et al. Amiodarone to prevent recurrence of atrial fibrillation. Canadian Trial of Atrial Fibrillation Investigators. N Engl J Med. 2000;342:913–20.
Flaker G, Lopes RD, Hylek E, et al. Amiodarone, anticoagulation, and clinical events in patients with atrial fibrillation: insights from the ARISTOTLE trial. J Am Coll Cardiol. 2014;64:1541–50.
Lafuente-Lafuente C, Mouly S, Longas-Tejero MA, Mahe I, Bergmann JF. Antiarrhythmic drugs for maintaining sinus rhythm after cardioversion of atrial fibrillation: a systematic review of randomized controlled trials. Arch Intern Med. 2006;166:719–28.
Chao TF, Liu CJ, Tuan TC, et al. Rate-control treatment and mortality in atrial fibrillation. Circulation. 2015;132:1604–12.
Kotecha D, Holmes J, Krum H, et al. Efficacy of beta blockers in patients with heart failure plus atrial fibrillation: an individual-patient data meta-analysis. Lancet. 2014;384:2235–43.
Shah M, Avgil TM, Jackevicius CA, Essebag V, Behlouli H, Pilote L. Relation of digoxin use in atrial fibrillation and the risk of all-cause mortality in patients >/=65 years of age with versus without heart failure. Am J Cardiol. 2014;114:401–6.
Mulder BA, Van Veldhuisen DJ, Crijns HJ, et al. Digoxin in patients with permanent atrial fibrillation: data from the RACE II study. Heart Rhythm. 2014;11:1543–50.
Nademanee K, Amnueypol M, Lee F, et al. Benefits and risks of catheter ablation in elderly patients with atrial fibrillation. Heart Rhythm. 2015;12:44–51.
Fiala M, Wichterle D, Bulkova V, et al. A prospective evaluation of haemodynamics, functional status, and quality of life after radiofrequency catheter ablation of long-standing persistent atrial fibrillation. Europace. 2014;16:15–25.
Fumagalli S, Tarantini F, Guarducci L, et al. Atrial fibrillation is a possible marker of frailty in hospitalized patients: results of the GIFA Study. Aging Clin Exp Res. 2010;22:129–33.
Coyne KS, Paramore C, Grandy S, Mercader M, Reynolds M, Zimetbaum P. Assessing the direct costs of treating nonvalvular atrial fibrillation in the United States. Value Health. 2006;9:348–56.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Fumagalli, S., Gabbai, D., Padeletti, L., Crijns, H.J., Lip, G.Y.H. (2017). Atrial Fibrillation in the Elderly. In: Ungar, A., Marchionni, N. (eds) Cardiac Management in the Frail Elderly Patient and the Oldest Old. Springer, Cham. https://doi.org/10.1007/978-3-319-43468-1_12
Download citation
DOI: https://doi.org/10.1007/978-3-319-43468-1_12
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-43466-7
Online ISBN: 978-3-319-43468-1
eBook Packages: MedicineMedicine (R0)