
Abstract
Hip fracture is one of the most common conditions in the elderly, particularly in women. Although data are sparse and partially conflicting, it is estimated that hip fractures will occur in 18 % of women and 6 % in men in a lifetime, with an absolute number expected to increase from 1.26 million in 1990 to 4.5 million by the year 2050. Given these huge numbers, and the degree to which it negatively impacts quality and expectancy of life, hip fracture represents an important medical condition. The costs associated with this condition are enormous since it requires a long period of hospitalisation and rehabilitation. Furthermore, hip fracture is associated with higher development of sarcopenia, disability and depression, with additional costs for society.
In this chapter, we discuss the epidemiological data around hip fracture, including known risk factors and conditions that seem pivotal for determining this condition. Moreover, we analyse the costs related to hip fracture. This medical condition seems to be comparable to other common diseases (like cardiovascular conditions) in terms of hospitalisation and rehabilitation, but other social costs (due to onset of new co-morbidities, sarcopenia, poor quality of life, disability and mortality) are probably greater.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
2.1 Introduction
Hip fractures constitute a remarkable public health problem in industrialised countries, since this condition is associated with a higher rate of disability and mortality [1]. Therefore, it is hardly surprising that hip fracture is also associated with enormous social and economic costs. Moreover, since hip fracture incidence linearly increases with advancing age, and it is estimated that older people will represent a substantial proportion of the worldwide population in future, the costs of hip fracture will probably increase.
In this chapter, we aim to summarise the current epidemiological data about this condition, with a special focus on the economic impact.
2.2 Epidemiological Data
2.2.1 Risk Factors for Hip Fracture
The pathogenesis of hip fracture is multifactorial. Although many conditions contribute to the development of hip fracture, the main factors can be summarised in two wide categories: those affecting/decreasing bone mineral density (BMD) and those increasing the rate of falls.
2.2.2 Factors Affecting Bone Mineral Density
The factors negatively affecting BMD are the same as those that increase the risk of osteoporosis. Since another chapter is specifically dedicated to this important issue, we will say only a few words about it.
The conditions negatively affecting BMD could be further categorised as: non-modifiable and modifiable factors [2, 3].
In the first category, we should mention age, female sex, race, family history of osteoporosis and fractures, and low body frame size. In this category, we could insert the long list of the genetic factors and mutations leading to an increased risk of osteoporosis and so of fragility fractures.
Conversely, among the modifiable factors we can consider low calcium intake, reduced exposure to sunlight, inflammatory diseases (particularly if affecting the gastrointestinal system), some drugs (e.g. cortisone), excessive alcohol intake, eating disorders (particularly anorexia nervosa) and body mass index (BMI), which seems to be associated with hip fractures in a U-shaped way [4–6].
2.2.3 Factors Increasing Rate of Falls
Although in the literature it is mentioned that hip fracture can occur without any trauma, this is not the general rule. Older people, in fact, usually have a hip fracture after a trauma, although often it is a minor trauma, such as a fall from standing height. We could say that the interaction between trauma and low BMD typically lead to the hip fracture. This is somewhat different from other osteoporotic fractures, particularly vertebral ones, which do occur without explicit trauma, probably because of the different composition of bone components.
Therefore, knowledge of factors that increase the rate of falls seems to be important for tailoring appropriate preventive interventions. The risk factors for falls can be categorised as intrinsic (i.e. pertaining to the subject) or extrinsic (i.e. pertaining to the settings in which the person lives).
Among the first, we could count:
-
Advanced age;
-
Poor physical performance (including gait and balance problems): it is known that poor physical performance and particularly muscle weakness increased the risk of falls [7];
-
Poor vision and hearing; [8]
-
Orthostatic hypotension; [9]
-
Chronic conditions including osteoarthritis, diabetes, neurological conditions etc.: these conditions are usually associated with a higher risk of falls through anatomical changes in the joints (like osteoarthritis), less sensitivity (diabetes) or higher use of psychoactive medications that could increase the risk of falls (like dementia or Parkinson’s disease).
-
Fear of falling;
The extrinsic factors include those affecting the setting in which the older person lives. These are of particular importance because they are easily modifiable [10]. Some examples are:
-
Lack of stair handrails;
-
Poor stair design;
-
Lack of bathroom grab bars;
-
Dim lighting or glare;
-
Obstacles and tripping hazards;
-
Slippery or uneven surfaces;
-
Improper use of assistive device.
2.3 Prevalence and Incidence of Hip Fracture
Prevalence and incidence rates of hip fracture reported in different studies vary significantly around the world and it is suggested that the two major causes of these differences are gender and race. The International Osteoporosis Foundation (IOF) estimates that worldwide hip fractures will occur in 18 % of women and 6 % in men [11].
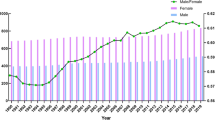
Figure 2.1 shows the age-standardised incidence rates for hip fracture (/100,000) for some representative countries. Considering both genders together, the highest incidence was observed in Denmark (439/100,000), the lowest in Ecuador (55/100,000) [12].

Age-standardised hip fracture incidence rates (/100,000) for some representative countries
Regarding the site usually affected by hip fracture, in the United States, femoral neck and intertrochanteric fractures are very similar in frequency in patients aged more than 65 years, with a higher frequency in white women than in men [13].
2.3.1 Gender Differences
Because women have more bone loss and higher rate of falls than men, the incidence of hip fracture in this sex is about twice that seen in men at any age in the industrialised countries [3].
It is estimated that about one third of women living to age 80 will have a hip fracture [14]. This risk is somewhat comparable to the combined risk of developing any kind of genito-urinary cancer [15]. In women, the lowest annual incidence rate was seen in Nigeria (2/100,000), the highest in Northern Europe countries, like Denmark (574/100,000), Norway (563/100,000) and Sweden (539/100,000) [12].
Regarding men, it is estimated that each year they experience about one third of the total hip fractures affecting a population. However, in this gender, the risk for hip fractures exponentially increases after age 70, and 17 % of men living beyond 80 years of age will report a hip fracture [16]. Although less frequent than in women, hip fractures in men seem to be more dangerous, since one third of men reporting a hip fracture die within 1 year [16].
In this gender, the lowest incidence rate was seen in Ecuador (35/100,000) and the highest in Denmark (290/100,000) [12].
2.3.2 Racial Differences
Whites (particularly if living at higher latitudes) exhibit a higher age and sex-adjusted incidence of hip fractures ranging from 420/100,000 new hip fractures each year in Norway [17] to 195/100,000 in USA [18]. After age 50, white women have an almost doubled risk of hip fracture than men with the highest annual incidence of hip fractures after 80 [1, 12].
Interestingly, people living in the Mediterranean area, although mainly whites, report lower incidence of fractures. This seems to be attributable to several factors, particularly higher serum 25-hydroxy vitamin D (25OHD) levels and healthier lifestyle [19]. Recent research highlights a role also for the Mediterranean diet since it is known that this dietary pattern is associated with lower inflammation levels, lower adiposity and decrease risk of falls, all these factors being important for the development of hip fracture [19, 20].
By contrast, fewer studies have investigated the epidemiology of hip fractures in other races.
Blacks seem to have a decreased risk of hip fracture compared to whites, reporting an age and sex adjusted incidence ranging from 31/100,000 in the Bantu population [21] to 185/100,000 in California [22].
Asians demonstrate a risk of hip fracture intermediate between whites and blacks [23, 24]. Around 30 % of the hip fractures occurring worldwide are thought to arise in Asian populations, most notably in China, making this country of particular importance [25]. The incidence observed among men and women between 1966 and 1985 significantly increased (1.7 fold among men and 2.5 fold among women), however between 1985 and 1995 it remained steady [25]. Regarding other Asiatic countries, the most recent studies from Hong Kong and Singapore suggest that temporal trends may have reached a plateau, but those from Japan suggest significant age-adjusted increases [26, 27].
Finally, Hispanic populations show the lowest incidence of hip fractures among all the races investigated and interestingly the ratio between women and men is reversed [1, 12]. However, annual fracture rates among the Hispanic population increased significantly (4.2 % in men and 4.9 % in women) between 1983 and 2000, in contrast to other races [28].
2.3.3 Time Trends in the Incidence of Hip Fractures
The total number of persons affected by hip fractures may be increasing over time in the next years, mainly due to the progressive ageing of the population. Indeed, the absolute number of hip fractures is expected to increase to 4.5 million by the year 2050 [25]. However, these projections do not take into account several important confounders, such as the increased use of anti-osteoporotic drugs, the use of supplementation with calcium and vitamin D and the strategies adopted by some countries for the early identification of osteoporosis.
Right now, reported trends differ markedly across countries with some studies reporting a significant increase [29–32], some a decrease [33–37], and some others stable rates [38–40]. In studies reporting a lower incidence of age- and sex-specific incidence hip fracture over time, possible explanations seem to be a higher adherence to anti-osteoporotic medications as well as increased use of calcium and vitamin D supplementation, avoidance of smoking and alcohol, and more efficacious strategies for the prevention of falls [41].
In summary, with a few exceptions, age-specific incidence rates of hip fractures significantly rose in Western populations until 1980 with subsequent stability or sometimes a decrease. In Western countries, the trends seem to be more pronounced in women than in men [25]. However, a final word cannot be given regarding this relevant issue and future longitudinal studies (particularly in populations not including whites) are needed, to see in which direction we are moving.
2.4 Social Costs
In contrast to other types of fragility fracture (e.g. vertebral), hip fractures usually need immediate intervention and consequently hospitalisation. Every year about 300,000 subjects are hospitalised with hip fractures in the United States alone [42]. Approximately one-third of fracture patients receive prosthetic replacement. It is therefore hardly surprisingly that in the United States alone, the estimated cost of treatment was approximately 10.3 to 15.2 billion dollars per year in 1990 [43] and 17 billion in 2002 [3].
Hip fractures require a long period of hospitalisation, usually longer than other medical conditions, except for psychiatric diseases [44].
The burden of hip fracture management on both the individual and society is substantial, and includes direct fracture-treatment costs and social costs resulting from functional impairment and increased morbidity [45].
2.4.1 Hospitalisation and Rehabilitation Costs
The data available suggest that hip fracture is a condition associated with a high social cost, particularly for expenses needed for hospitalisation and rehabilitation. Expenditures are rising very quickly and are a source of concern in many countries [3]. In a prospective study lasting 1 year in Belgium, a group of 159 older women totalled a mean cost of the initial hospitalisation of $9,534 and the total direct costs during the year after discharge were $13,470. These costs were almost triple that of a group of age- and sex-matched older subjects without hip fracture [46].
It is estimated that the expenditure needed for hip fracture exceeds that for breast and gynaecological cancers combined, but not those for cardiovascular disease in USA [47]. The comparison of costs between hip fracture and cardiovascular diseases is intriguing. In Switzerland, for example, osteoporotic hip fractures account for more hospital bed days than myocardial infarction and stroke and consequently lead to higher costs [48], while in Italy the costs due to hip fractures are comparable to those of acute myocardial infarction [44].
2.4.2 Hospital Costs
Hospital costs include costs associated with surgery (implant and theatre costs), laboratory and radiological investigations and length of hospitalisation in an acute ward [49].
The mean duration of hospitalisation is highly variable. In the United Kingdom, a study reported that, in people with a mean age over 80 years, the duration of hospitalisation was 23 days, without including the days due to rehabilitation [49]. In Italy, another study in people over 45 years of age found the mean duration of hospitalisation was about 15 days, again not considering rehabilitation [44]. In the United States, on the contrary, during the period from 1990 to 2003, the mean length of stay in the hospital for hip fractures declined by about half, leading to an average hospital stay of 6.5 days [50]. It should be noted that these huge differences probably depend on the different health systems and the relative costs for each day of hospitalisation. In the United States, for example, every day in hospital costs $1,791 in for-profit hospitals, $1,878 in state/local government hospitals and $2,289 in non-profit hospitals [50], while in the United Kingdom 1 day costs $600 [51]. It should be noted that shorter lengths of stay have been associated with higher 30-day mortality in patients experiencing a hip fracture in Sweden [52]. By contrast, a recent study in USA demonstrated that decreased length of stay was associated with reduced rates of early mortality [53]. This difference might be related to the fact that increased time to surgery is associated with longer hospital stay and we know that time to surgery (more than 24/48 h after the fracture) is a key factor in predicting early mortality [54].
2.4.3 Rehabilitation and Nursing Home Costs
Rehabilitation is a mandatory step for people having experienced a hip fracture [55]. However, the advanced age and the co-morbidities affecting hip fracture patients often dictate that the completion of the rehabilitation programme takes place in a long-term care (LTC) facility or in a nursing home [56]. The percentage of people requiring a LTC facility or similar institution is estimated at between 6 and 60 % of people with a hip fracture, with a cost ranging from $19,000 to $66,000 [56]. The costs needed for a LTC seem to be almost double those required by a rehabilitation institute [57].
However, the roles of these organisations for rehabilitation of older patients are still debated. In a well-known study on this topic, hip fracture patients admitted to rehabilitation hospitals did not differ from patients admitted to nursing homes in their return to the community or in disability rate [58]. Moreover, costs were significantly greater for rehabilitation hospital patients than for nursing home patients and the evidence about the value of these organisations in the elderly is conflicting [58–60].
2.4.4 Other Social Costs Related to Hip Fracture
Hip fracture is associated with several negative outcomes. For example, reports of permanent disability in those surviving initial hospitalisation after a hip fracture ranged from 32 to 80 % [56].
The most common and important consequence of hip fracture is, however, increased mortality. It is estimated that about 20 % of the subjects die within the first 3–6 months of their injury [61]. Moreover, as for cardiovascular diseases, the likelihood of having any subsequent hospital episodes increased by 231 %, any subsequent incident increased future incident episodes by 9.4 %, the total number of hospital days by 21.3 % and the total charges by 16.3 % [62].
Other consequences may be loss of muscle strength, increased postural sway and decline in walking speed that can lead to loss of functional muscle mass, sarcopenia and finally to disability [61]. The impact on disability is striking: 1 year after fracturing a hip, 40 % of patients are still unable to walk independently, 60 % have difficulty with at least one essential activity of daily living, and 80 % are restricted in instrumental activities of daily living, such as driving and grocery shopping [63].
Finally, hip fracture seems to be associated with the onset of other co-morbidities with a high cost for society. Recent research has highlighted that people experiencing a hip fracture have a greater incidence of depression [64] and consequently a higher use of anti-depressant medications [65]. Another field of interest is the possible relationship between hip fracture and the onset of cardiovascular diseases. Hip fracture, in fact, seems to increase the risk of coronary heart disease, particularly during the first year after the event [66]. Since cardiovascular diseases are among the most expensive medical conditions [67], the impact of hip fracture in contributing to a huge increase in medical and social costs is highly relevant.
Conclusions
Hip fracture is a common and debilitating condition, particularly for older persons. Although the age (and gender) specific incidence is decreasing in some countries, the global incidence of hip fracture is rising everywhere, suggesting that more should be done for its prevention, also in view of its impact on social costs and quality of life. Future epidemiological studies are thus needed to better verify the trend in incidence of hip fracture and the strategies effective for its prevention.
References
Maggi S, Kelsey JL, Litvak J, Heyse SP (1991) Incidence of hip fractures in the elderly: a cross-national analysis. Osteoporos Int 1(4):232–241
Seeman E, Allen T (1989) Risk factors for osteoporosis. Aust N Z J Med [Internet]. [cited 2016 Apr 13];19(1):69–75. Available from: http://doi.wiley.com/10.1111/j.1445-5994.1989.tb01682.x
Cummings SRML, Melton LJ (2002) Epidemiology and outcomes of osteoporotic fractures. Lancet 359:1–1761
Veronese N, Solmi M, Rizza W, Manzato E, Sergi G, Santonastaso P, et al (2014) Vitamin D status in anorexia nervosa: a meta-analysis. Int J Eat Disord [Internet]. [cited 2015 Sep 25]; Available from: http://www.ncbi.nlm.nih.gov/pubmed/25445242
Solmi M, Veronese N, Correll CU, Favaro A, Santonastaso P, Caregaro L, et al (2016) Bone mineral density, osteoporosis, and fractures among people with eating disorders: a systematic review and meta-analysis. Acta Psychiatr Scand [Internet]. [cited 2016 Apr 13]; Available from: http://www.ncbi.nlm.nih.gov/pubmed/26763350
De Laet C, Kanis JA, Odén A, Johanson H, Johnell O, Delmas P, et al (2005) Body mass index as a predictor of fracture risk: a meta-analysis. Osteoporos Int [Internet]. 16(11):1330–1338. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15928804
Veronese N, Bolzetta F, Toffanello ED, Zambon S, De Rui M, Perissinotto E, et al (2014) Association between short physical performance battery and falls in older people: the Pro.V.A study. Rejuvenation Res [Internet]. 1–29. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24387140
Gleeson M, Sherrington C, Keay L (2014) Exercise and physical training improve physical function in older adults with visual impairments but their effect on falls is unclear: a systematic review. J Physiother [Internet]. [cited 2016 Apr 13];60(3):130–135. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25066935
Veronese N, De Rui M, Bolzetta F, Zambon S, Corti MC, Baggio G, et al (2015) Orthostatic changes in blood pressure and mortality in the elderly: the Pro.V.A study. Am J Hypertens [Internet]. [cited 2015 Sep 25];28(10):1248–1256. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25767137
Berg RL, Cassells JS (1992) Falls in older persons: risk factors and prevention. In: Berg RL, Cassells JS (eds) The second fifty years: promoting health and preventing disability [Internet]. National Academies Press, Washington, DC, pp 263–290. [cited 2016 Apr 13]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK235613/
Cooper C, Campion G, Melton LJ (1992) Hip fractures in the elderly: a world-wide projection. Osteoporos Int 2(6):285–289
Kanis JA, Odén A, McCloskey EV, Johansson H, Wahl DA, Cooper C (2012) A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos Int 23(9):2239–2256
Karagas MR, Lu-Yao GL, Barrett JA, Beach ML, Baron JA (1996) Heterogeneity of hip fracture: age, race, sex, and geographic patterns of femoral neck and trochanteric fractures among the US elderly. Am J Epidemiol [Internet]. [cited 2016 Apr 23];143(7):677–682. Available from: http://www.ncbi.nlm.nih.gov/pubmed/8651229
Gallagher JC, Melton LJ, Riggs BL, Bergstrath E (1980) Epidemiology of fractures of the proximal femur in Rochester, Minnesota. PubMed – NCBI [Internet]. [cited 2016 Apr 13]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/7428215
Elffors L (1988) Are osteoporotic fractures due to osteoporosis? Impacts of a frailty pandemic in an aging world. Aging (Milan, Italy) [Internet]. [cited 2016 Apr 23];10(3):191–204. Available from: http://www.ncbi.nlm.nih.gov/pubmed/9801729
Iqbal MM (2000) Osteoporosis: epidemiology, diagnosis, and treatment. South Med J [Internet]. [cited 2016 Apr 13];93(1):2–18. Available from: http://www.ncbi.nlm.nih.gov/pubmed/10653058
Emaus N, Olsen LR, Ahmed LA, Balteskard L, Jacobsen BK, Magnus T, et al (2011) Hip fractures in a city in Northern Norway over 15 years: time trends, seasonal variation and mortality: the Harstad Injury Prevention Study. Osteoporos Int [Internet]. [cited 2016 May 2];22(10):2603–2610. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3169771&tool=pmcentrez&rendertype=abstract
Ettinger B, Black DM, Dawson-Hughes B, Pressman AR, Melton LJ (2010) Updated fracture incidence rates for the US version of FRAX®. Osteoporos Int 21(1):25–33
Haring B, Crandall CJ, Wu C, LeBlanc ES, Shikany JM, Carbone L, et al (2016) Dietary patterns and fractures in postmenopausal women. JAMA Intern Med [Internet]. [cited 2016 Mar 28]; Available from: http://www.ncbi.nlm.nih.gov/pubmed/27019044
Romero Pérez A, Rivas Velasco A (2014) Adherence to Mediterranean diet and bone health. Nutrición hospitalaria [Internet]. [cited 2016 Apr 14];29(5):989–996. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24951976
Solomon L (1968) Osteoporosis and fracture of the femoral neck in the South African Bantu. J Bone Joint Surg Br [Internet]. [cited 2016 Apr 23];50(1):2–13. Available from: http://www.ncbi.nlm.nih.gov/pubmed/5641595
Silverman SL, Madison RE (1988) Decreased incidence of hip fracture in Hispanics, Asians, and blacks: California Hospital Discharge Data. Am J Public Health [Internet]. [cited 2016 Apr 23];78(11):1482–1483. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1350247&tool=pmcentrez&rendertype=abstract
Wong PC (2008) Fracture epidemiology in a mixed southeastern Asian community (Singapore). Clin Orthop Relat Res [Internet]. [cited 2016 Apr 23];45:55–61. Available from: http://www.ncbi.nlm.nih.gov/pubmed/5939474
Chalmers J, Ho KC (1970) Geographical variations in senile osteoporosis. The association with physical activity. J Bone Joint Surg Br [Internet]. [cited 2016 Apr 23];52(4):667–675. Available from: http://www.ncbi.nlm.nih.gov/pubmed/5487566
Cooper C, Cole ZA, Holroyd CR, Earl SC, Harvey NC, Dennison EM, et al (2011) Secular trends in the incidence of hip and other osteoporotic fractures. Osteoporos Int [Internet]. [cited 2016 Mar 18];22(5):1277–1288. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3546313&tool=pmcentrez&rendertype=abstract
Hagino H, Furukawa K, Fujiwara S, Okano T, Katagiri H, Yamamoto K, et al (2009) Recent trends in the incidence and lifetime risk of hip fracture in Tottori, Japan. Osteoporos Int [Internet]. [cited 2016 May 2];20(4):543–548. Available from: http://www.ncbi.nlm.nih.gov/pubmed/18633667
Koh LK, Saw SM, Lee JJ, Leong KH, Lee J (2001) Hip fracture incidence rates in Singapore 1991–1998. Osteoporos Int [Internet]. [cited 2016 Apr 18];12(4):311–318. Available from: http://www.ncbi.nlm.nih.gov/pubmed/11420781
Zingmond DS, Melton LJ, Silverman SL (2004) Increasing hip fracture incidence in California Hispanics, 1983 to 2000. Osteoporos Int [Internet]. [cited 2016 May 2];15(8):603–610. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15004666
Arakaki H, Owan I, Kudoh H, Horizono H, Arakaki K, Ikema Y, et al (2011) Epidemiology of hip fractures in Okinawa, Japan. J Bone Miner Metab [Internet]. [cited 2016 Apr 23];29(3):309–314. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20814705
Piscitelli P, Tarantino U, Chitano G, Argentiero A, Neglia C, Agnello N, et al (2011) Updated incidence rates of fragility fractures in Italy: extension study 2002–2008. Clin Cases Miner Bone Metab [Internet]. [cited 2016 Apr 23];8(3):54–61. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3279067&tool=pmcentrez&rendertype=abstract
Mann E, Meyer G, Haastert B, Icks A (2010) Comparison of hip fracture incidence and trends between Germany and Austria 1995–2004: an epidemiological study. BMC Public Health [Internet]. [cited 2016 Apr 23];10:46. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2831031&tool=pmcentrez&rendertype=abstract
Tuzun S, Eskiyurt N, Akarirmak U, Saridogan M, Senocak M, Johansson H, et al (2012) Incidence of hip fracture and prevalence of osteoporosis in Turkey: the FRACTURK study. Osteoporos Int [Internet]. [cited 2016 Apr 23];23(3):949–955. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21594756
Langley J, Samaranayaka A, Davie G, Campbell AJ (2011) Age, cohort and period effects on hip fracture incidence: analysis and predictions from New Zealand data 1974–2007. Osteoporos Int [Internet]. [cited 2016 Apr 23];22(1):105–111. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20309526
Nymark T, Lauritsen JM, Ovesen O, Röck ND, Jeune B (2006) Decreasing incidence of hip fracture in the Funen County, Denmark. Acta Orthop [Internet]. [cited 2016 Apr 23];77(1):109–113. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16534709
Leslie WD, O’Donnell S, Jean S, Lagacé C, Walsh P, Bancej C, et al (2009) Trends in hip fracture rates in Canada. JAMA [Internet]. [cited 2016 Apr 15];302(8):883–889. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19706862
Cassell E, Clapperton A (2013) A decreasing trend in fall-related hip fracture incidence in Victoria, Australia. Osteoporos Int [Internet]. [cited 2016 Apr 23];24(1):99–109. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22349962
Adams AL, Shi J, Takayanagi M, Dell RM, Funahashi TT, Jacobsen SJ (2013) Ten-year hip fracture incidence rate trends in a large California population, 1997–2006. Osteoporos Int [Internet]. [cited 2016 Apr 23];24(1):373–376. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22349963
Wu T-Y, Jen M-H, Bottle A, Liaw C-K, Aylin P, Majeed A (2011) Admission rates and in-hospital mortality for hip fractures in England 1998 to 2009: time trends study. J Public Health (Oxford, England) [Internet]. [cited 2016 Apr 23];33(2):284–291. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20926392
Hernández JL, Olmos JM, Alonso MA, González-Fernández CR, Martínez J, Pajarón M, et al (2006) Trend in hip fracture epidemiology over a 14-year period in a Spanish population. Osteoporos Int [Internet]. [cited 2016 Apr 23];17(3):464–470. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16283063
Rosengren BE, Ahlborg HG, Gärdsell P, Sernbo I, Nilsson J-Å, Daly RM, et al (2012) Forearm bone mineral density and incidence of hip fractures in Swedish urban and rural men 1987–2002. Scand J Public Health [Internet]. [cited 2016 Apr 23];40(1):102–108. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22006168
Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB (2009) Incidence and mortality of hip fractures in the United States. JAMA [Internet] 302(14):1573–1579. Available from: http://jama.jamanetwork.com/article.aspx?doi=10.1001/jama.2009.1462. http://www.ncbi.nlm.nih.gov/pubmed/19826027. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=PMC4410861
Kannus P, Parkkari J, Sievänen H, Heinonen A, Vuori I, Järvinen M (1996) Epidemiology of hip fractures. Bone [Internet]. [cited 2016 Apr 23];18(1 Suppl):57S–63S. Available from: http://www.ncbi.nlm.nih.gov/pubmed/8717549
Cummings SR, Rubin SM, Black D (1990) The future of hip fractures in the United States. Numbers, costs, and potential effects of postmenopausal estrogen. Clin Orthop Relat Res [Internet]. [cited 2016 Apr 23];(252):163–166. Available from: http://www.ncbi.nlm.nih.gov/pubmed/2302881
Piscitelli P, Iolascon G, Gimigliano F, Muratore M, Camboa P, Borgia O et al (2007) Incidence and costs of hip fractures compared to acute myocardial infarction in the Italian population: a 4-year survey. Osteoporos Int 18(2):211–219
Johnell O, Kanis J (2005) Epidemiology of osteoporotic fractures. Osteoporos Int [Internet]. [cited 2016 Apr 4];16(Suppl 2):S3–S7. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15365697
Haentjens P, Autier P, Barette M, Boonen S (2001) The economic cost of hip fractures among elderly women. A one-year, prospective, observational cohort study with matched-pair analysis. Belgian Hip Fracture Study Group. J Bone Joint Surg Am [Internet]. [cited 2016 Apr 25];83-A(4):493–500. Available from: http://www.ncbi.nlm.nih.gov/pubmed/11315777
Hoerger TJ, Downs KE, Lakshmanan MC, Lindrooth RC, Plouffe L, Wendling B, et al (1999) Healthcare use among U.S. women aged 45 and older: total costs and costs for selected postmenopausal health risks. J Womens Health Gender Based Med [Internet]. [cited 2016 Apr 23];8(8):1077–1089. Available from: http://www.ncbi.nlm.nih.gov/pubmed/10565666
Lippuner K, von Overbeck J, Perrelet R, Bosshard H, Jaeger P (1997) Incidence and direct medical costs of hospitalizations due to osteoporotic fractures in Switzerland. Osteoporos Int [Internet]. [cited 2016 Apr 23];7(5):414–425. Available from: http://www.ncbi.nlm.nih.gov/pubmed/9425498
Lawrence TM, White CT, Wenn R, Moran CG (2005) The current hospital costs of treating hip fractures. Injury [Internet]. [cited 2016 Mar 19];36(1):88–91; discussion 92. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15589923
National Hospital Discharge Survey (2010) Health data interactive, health care use and expenditures
Department of Health (2013) National schedule of NHS reference costs 2012–13 – critical care. 57 p
Nordstrom P, Gustafson Y, Michaelsson K, Nordstrom A (2015) Length of hospital stay after hip fracture and short term risk of death after discharge: a total cohort study in Sweden. BMJ [Internet]. [cited 2016 Apr 25];350(feb20 1):h696–h696. Available from: http://www.bmj.com/content/350/bmj.h696
Nikkel LE, Kates SL, Schreck M, Maceroli M, Mahmood B, Elfar JC (2015) Length of hospital stay after hip fracture and risk of early mortality after discharge in New York state: retrospective cohort study. BMJ (Clin Res ed) [Internet]. [cited 2016 May 2];351:h6246. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=4674667&tool=pmcentrez&rendertype=abstract
Maggi S, Siviero P, Wetle T, Besdine RW, Saugo M, Crepaldi G (2010) A multicenter survey on profile of care for hip fracture: predictors of mortality and disability. Osteoporos Int [Internet]. [cited 2016 May 2];21(2):223–231. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19415372
De Rui M, Veronese N, Manzato E, Sergi G, De Rui Marina, Veronese N, et al (2013) Role of comprehensive geriatric assessment in the management of osteoporotic hip fracture in the elderly: an overview. Disabil Rehabil [Internet] 35(9):758–765. Available from: http://eutils.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&id=22877311&retmode=ref&cmd=prlinks\npapers3://publication/doi/10.3109/09638288.2012.707747. http://www.ncbi.nlm.nih.gov/pubmed/22877311. http://informahealthcare.com/doi/abs/10.3109/09
Braithwaite RS, Col NF, Wong JB (2003) Estimating hip fracture morbidity, mortality and costs. J Am Geriatr Soc 51(3):364–370
Hektoen L, Lund J (2014) Costs of treatment, care, and rehabilitation after hip fractures – a case study from Norway: Liv Faksvag Hektoen. Eur J Public Health [Internet]. [cited 2016 Apr 25];24(Suppl 2):cku166.126. Available from: http://eurpub.oxfordjournals.org/content/24/suppl_2/cku166.126
Kramer AM, Steiner JF, Schlenker RE, Eilertsen TB, Hrincevich CA, Tropea DA, et al (1997) Outcomes and costs after hip fracture and stroke. A comparison of rehabilitation settings. JAMA [Internet]. [cited 2016 Apr 27];277(5):396–404. Available from: http://www.ncbi.nlm.nih.gov/pubmed/9010172
Ward D, Severs M, Dean T, Brooks N (2003) Care home versus hospital and own home environments for rehabilitation of older people (Cochrane Review). Cochrane Database Syst Rev [Internet]. Issue 3(4):Art. No.: CD003164. Available from: doi: 10.1002/14651858.CD003164
Huusko TM (2000) Randomised, clinically controlled trial of intensive geriatric rehabilitation in patients with hip fracture: subgroup analysis of patients with dementia. BMJ [Internet]. [cited 2016 Apr 26];321(7269):1107–1111. Available from: http://www.bmj.com/content/321/7269/1107.short
Marks R, Allegrante JP, Ronald MacKenzie C, Lane JM (2003) Hip fractures among the elderly: causes, consequences and control. Ageing Res Rev [Internet] 2(1):57–93. Available from: http://www.sciencedirect.com/science/article/pii/S1568163702000454
Wolinsky FD, Fitzgerald JF, Stump TE (1997) The effect of hip fracture on mortality, hospitalization, and functional status: a prospective study. Am J Public Health [Internet]. [cited 2016 Apr 26];87(3):398–403. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1381011&tool=pmcentrez&rendertype=abstract
Cooper C (1997) The crippling consequences of fractures and their impact on quality of life. Am J Med [Internet] 103(2):S12–S19. Available from: http://linkinghub.elsevier.com/retrieve/pii/S000293439790022X
Cristancho P, Lenze EJ, Avidan MS, Rawson KS (2016) Trajectories of depressive symptoms after hip fracture. Psychol Med [Internet] 46(07):1413–1425. Available from: http://www.journals.cambridge.org/abstract_S0033291715002974
Iaboni A, Seitz DP, Fischer HD, Diong CC, Rochon PA, Flint AJ (2015) Initiation of antidepressant medication after hip fracture in community-dwelling older adults. Am J Geriatr Psychiatry [Internet]. [cited 2016 Apr 26];23(10):1007–1015. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25488107
Tsai C-H, Lin C-L, Hsu H-C, Chung W-S (2015) Increased risk of coronary heart disease in patients with hip fracture: a nationwide cohort study. Osteoporos Int [Internet] 26(6):1849–1855. Available from: http://springerlink.bibliotecabuap.elogim.com/10.1007/s00198-015-3097-y
Patricoski CT, Steiner G (1999) Cost of medications for patients with ischemic heart disease in a rural family practice center. J Am Board Fam Pract [Internet]. [cited 2016 Apr 26];12(3):200–205. Available from: http://www.ncbi.nlm.nih.gov/pubmed/10395416
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Veronese, N., Maggi, S. (2017). Epidemiology of Hip Fracture and Social Costs. In: Falaschi, P., Marsh, D. (eds) Orthogeriatrics. Practical Issues in Geriatrics. Springer, Cham. https://doi.org/10.1007/978-3-319-43249-6_2
Download citation
DOI: https://doi.org/10.1007/978-3-319-43249-6_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-43248-9
Online ISBN: 978-3-319-43249-6
eBook Packages: MedicineMedicine (R0)