
Abstract
Anatomy: 33 normal vertebra with 24 presacral segments: 7 cervical, 12 thoracic rib-bearing and 5 lumbar non-rib-bearing. Approximately 5 % of population with variant transitional anatomy with lumbarization of S1 or sacralization of L5 due to partial fusion of transverse process with sacrum, which may predispose to Bertolotti’s syndrome, which can be a source of back pain caused by the transitional lumbosacral anatomy (Fig. 29.1).
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others



Keywords
Anatomy: 33 normal vertebra with 24 presacral segments: 7 cervical, 12 thoracic rib-bearing and 5 lumbar non-rib-bearing. Approximately 5 % of population with variant transitional anatomy with lumbarization of S1 or sacralization of L5 due to partial fusion of transverse process with sacrum, which may predispose to Bertolotti’s syndrome, which can be a source of back pain caused by the transitional lumbosacral anatomy (Fig. 29.1).

Frontal radiograph of the lumbar spine shows transitional lumbosacral anatomy with prominent left transverse process of the L5 vertebral body which is partially articulating with the left hemisacrum with resultant sclerosis (oval circle) as can be seen with Bertolotti’s syndrome. Note that 5 non-rib bearing vertebral bodies are presumed with a right-sided small rib denoted at the T12 level (solid black arrow)
X-Ray Imaging
Indications
-
Trauma to evaluate for fracture/dislocation s;
-
Instability to evaluate for spondylolisthesis and spondylolysis ;
-
Low back pain with “red flags” as per American College of Radiology Appropriateness Criteria, including osteoporosis, focal/progressive neurological deficit; >6 weeks symptom duration; age >70; suspected cancer, infection or immunosupression; pain with radiculopathy and surgical or interventional candidate; prior lumbar surgery; cauda equina syndrome.
Technique
-
Standard images include anteroposterior (AP), lateral, and coned-down lateral projections of lumbosacral junction.
-
Bilateral oblique (“Scotty dog”) views helpful to evaluate for facet arthropathy and for pars interarticularis defects and spondylolysis .
-
Lateral views with patient in flexion and extension helpful for evaluating instability and spondylolisthesis (Fig. 29.2).
Fig. 29.2 
(a) Lateral flexion view of the lumbar spine shows anterior translation of the L3 vertebral body (dashed black arrow) over the L4 vertebral body (solid black arrow), by less than 25 % of the vertebral body width, or grade 1 anterolisthesis (anterior spondylolisthesis), as measured by the differences between the posterior cortices. (b) Lateral extension view of the lumbar spine shows minimal interval decrease in the degree of anterior translation of the L3 vertebral body (dashed black arrow) over the L4 vertebral body (solid black arrow). The differences in anterolisthesis between flexion and extension views can be used to evaluate for the degree in dynamic instability

Evaluation
-
Designate number of lumbar vertebra for proper anatomy, evaluate for transitional anatomy;
-
Assess bony mineralization and vertebral body heights, evaluate for osteoporosis and fracture ;
-
Assess vertebral body alignment for spondylolisthesis as measured by incongruence of the posterior cortices:
-
True spondylolisthesis results from a pars interarticularis fracture and spondylolysis (Fig. 29.3);
-
Pseudospondylolisthesis , or degenerative spondylolisthesis, results from degenerative disc disease and facet arthropathy without spondylolysis;
Fig. 29.3 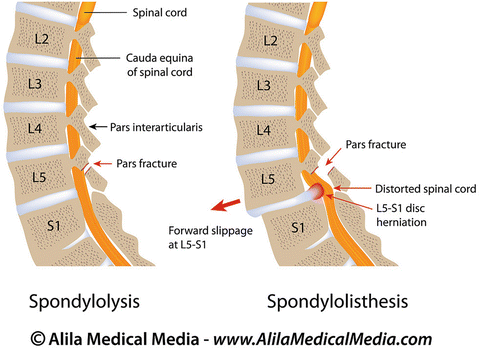
Sagittal schematic images of the lumbar spine show the difference between spondylolysis , which alone is defined as a bony defect or fracture of the pars interarticularis (also known as a pars fracture), versus “true” spondylolisthesis, which is malalignment and incongruence of the posterior cortices of the vertebrae with anterior translation secondary to a pars fracture. In contrast, pseudospondylolisthesis (not shown) is translation in the absence of a pars fracture, usually the result of degenerative disc disease or facet arthropathy. (Used with permission from Alila Medical Media)
-
-
Spondylolisthesis and instability based on measurable changes of horizontal displacements or translation and angular changes between adjacent vertebral bodies between flexion and extension;
-
Curvature for normal lumbar lordosis (on lateral view) and degree of scoliosis (on frontal view);
-
Intervertebral disc space heights for disc space narrowing and degenerative disc disease and the vertebral endplates for osteophytes and subchondral sclerosis;
-
Facet joints to evaluate for osteophytes, subchondral sclerosis, and joint space narrowing in facet arthropathy

CT Imaging
-
Provides greater sensitivity with superior bony detailed evaluation of the trabecular and cortical bone as compared to X-rays, particularly in evaluation of fracture healing and characterization of bone tumors;
-
Multiplanar reformations allow cross-sectional imaging in coronal, sagittal, and axial planes for evaluation of fractures, spondylolysis , pseudoarthrosis, and spinal canal and neural foraminal bony stenosis, particularly in pre-operative evaluation (Fig. 29.4);
-
In the setting of multiple trauma , routine multidetector CT with sagittal and coronal reconstructions is supplanting the role of radiographs;
-
Less useful for soft tissue pathologies such as spinal cord or nerve pathology;
-
IV contrast can be useful for soft tissue pathology
-
Useful if MRI is contraindicated or unavailable;
-
-
Used in conjunction with fluoroscopic-guided myelography for evaluation of disc herniations
-
Helpful in evaluation of postoperative bony graft healing and hardware complications
-
Static acquisition in supine or prone positioning precludes dynamic or weight-bearing evaluation of lumbar spine.
Fig. 29.4 
(a) Sagittal-reformatted CT image of the lumbar spine shows a minimally displaced comminuted fracture of the L2 vertebral body (solid white arrow) extending to the inferior endplate (dashed white arrow) which was occult on radiography (not shown). Compared with radiographs, CT demonstrates superior bony detailed evaluation of the cortex and trabeculae due to the lack of overlapping densities from soft tissue structures and abdominal contents. (b) Axial CT image of the lumbar spine again shows a minimally displaced comminuted fracture of the L2 vertebral body (dotted white arrow) which however, does not show extension to the pedicles or posterior elements. The posterior cortex is intact and no retropulsed bony fragments are seen encroaching on the spinal canal (solid white arrow)

Suggested Reading
Davis PC, Wippold 2nd FJ, Brunberg JA, et al. ACR appropriateness criteria on low back pain. J Am Coll Radiol. 2009;6(6):401–7.
Leone A, Guglielmi G, Cassar-Pullicino VN, et al. Lumbar intervertebral instability: a review. Radiology. 2007;245(1):62–77.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Gaviola, G.C., Shah, N.A. (2017). Lumbar Spine Imaging: X-Ray and CT. In: Yong, R., Nguyen, M., Nelson, E., Urman, R. (eds) Pain Medicine. Springer, Cham. https://doi.org/10.1007/978-3-319-43133-8_29
Download citation
DOI: https://doi.org/10.1007/978-3-319-43133-8_29
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-43131-4
Online ISBN: 978-3-319-43133-8
eBook Packages: MedicineMedicine (R0)