
Abstract
Primary varicella infection (chickenpox) is typically a mild and self-limited childhood illness presenting with a characteristic rash (pox), fever, malaise, and fatigue. Following primary infection, the varicella zoster virus (VZV) exists in a clinically inactive state in the dorsal root ganglia spinal nerves or sensory ganglia of cranial nerves. The virus can remain latent for years, but has the potential to reactivate as acute herpes zoster (AHZ)—typically seen as a blistering skin rash in the distribution of the affected ganglia. Symptoms are usually self-limited and resolve within several weeks. However, a subset of patients may have persistent pain that can last for months to years. If persistent, this neuropathic pain condition is known as post-herpetic neuralgia (PHN) and is the most common complication from AHZ. Though a 3-month time period for continued pain is typically used as a defining criterion for PHN, time frames in the literature range between 1 and 6 months.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Primary varicella infection
- Acute herpes zoster
- Risk factors
- Symptom control
- Antidepressants
- Anticonvulsants
- Topical applications
- Non-pharmacological treatments
- Zoster vaccine
Introduction
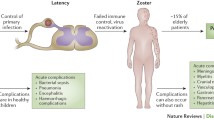
Primary varicella infection (chickenpox) is typically a mild and self-limited childhood illness presenting with a characteristic rash (pox), fever, malaise, and fatigue. Following primary infection, the varicella zoster virus (VZV) exists in a clinically inactive state in the dorsal root ganglia spinal nerves or sensory ganglia of cranial nerves. The virus can remain latent for years, but has the potential to reactivate as acute herpes zoster (AHZ) —typically seen as a blistering skin rash in the distribution of the affected ganglia. Symptoms are usually self-limited and resolve within several weeks. However, a subset of patients may have persistent pain that can last for months to years. If persistent, this neuropathic pain condition is known as post-herpetic neuralgia (PHN) and is the most common complication from AHZ. Though a 3-month time period for continued pain is typically used as a defining criterion for PHN, time frames in the literature range between 1 and 6 months .
Risk Factors
The risk of AHZ increases with advanced age. In the general population, the lifetime risk of AHZ is 25% and escalates to greater than 50% in those older than 80 years. In general, immunocompromised patients are at increased risk for AHZ. Specific examples include advanced age (older than 50), patients with HIV, diabetes, respiratory diseases, and/or cancer, and patients that take medications (e.g., steroids, chemotherapy) that weaken the immune system.
There are several risk factors cited in the literature that increase the chance of developing PHN after AHZ. Like AHZ, the elderly are susceptible—nearly 75% of PHN cases are seen in those 60 years and older. Other named risk factors include: female gender, pain/neurologic symptoms prior to rash (prodrome), uncontrolled acute pain, and rash severity during AHZ.
Pathophysiology
The pain associated with acute herpetic neuralgia is likely due to inflammation and damage to the nerve structures during AHZ. Neural damage is amplified through peripheral and central sensitization mechanisms. Even innocuous afferent input may result in increased spontaneous activity of primary nociceptive and their associated second-order neurons.
Clinical Manifestations
AHZ and PHN most commonly affect thoracic and cervical sensory spinal nerves in addition to one or more divisions of the trigeminal ganglion. Patients present with pain and sensory disturbances along affected nerve distributions. Pain can be spontaneous, paroxysmal, and/or evoked with even innocuous stimuli. Allodynia, hyperesthesia, and dysesthesia are common. Sensory disturbances can include loss of thermal, tactile, and vibration sensations. Persistent pain can affect quality of life, interfere with activities of daily living, and result in chronic fatigue, sleep disorders, depression, and anxiety.
Management
No disease modifying agents currently exist for PHN. Therapy should be geared towards symptom control . Often multiple agents may be necessary to achieve optimal pain control. Topical agents, tricyclic antidepressants (TCAs) , and anticonvulsant s are recommended as first-line agents. Topical applications of lidocaine and capsaicin are generally well-tolerated, have minimal side effects, and may offer efficacious pain relief. Although opiates can also provide analgesia, they should not be offered as an initial option. If prescribed, close monitoring is recommended. Non-pharmacological treatments such as transcutaneous electrical nerve stimulation (TENS), acupuncture, and behavioral therapies should also be considered in patients who have failed first-line pharmacologic treatments. Of note, NMDA receptor antagonists and antiviral medications have not been shown to be effective for treating PHN.
The zoster vaccine is recommended for prevention of AHZ and PHN in patients 50 years old or greater, particularly those with a previous history of AHZ. The vaccine is not recommended in patients who have already received the varicella vaccine (Table 148.1).
Additional Reading
Johnson RW, McElhaney J. Postherpetic neuralgia in the elderly. Int J Clin Pract. 2009;63(9):1386–91.
Johnson RW, Rice ASC. Clinical practice. Postherpetic neuralgia. N Engl J Med. 2014;371(16):1526–33.
Khadem T, Stevens V. Therapeutic options for the treatment of postherpetic neuralgia: a systematic review. J Pain Palliat Care Pharmacother. 2013;27(3):268–83.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Pak, D., Hung, J.C. (2017). Post-Herpetic Neuralgia. In: Yong, R., Nguyen, M., Nelson, E., Urman, R. (eds) Pain Medicine. Springer, Cham. https://doi.org/10.1007/978-3-319-43133-8_148
Download citation
DOI: https://doi.org/10.1007/978-3-319-43133-8_148
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-43131-4
Online ISBN: 978-3-319-43133-8
eBook Packages: MedicineMedicine (R0)