
Abstract
Radiation dose escalation improves prostate cancer outcomes and brachytherapy provides direct radiation dose escalation into the gland whilst minimizing dose to adjacent rectum and bladder. Two types of brachytherapy are commonly used: low dose rate (LDR), involving permanent implantation of radioactive seeds; and high dose rate (HDR), where the dose is delivered from a single radioactive source that moves through temporary implanted catheters. Current studies suggest that brachytherapy, either alone for low risk disease, or combined with external beam radiotherapy, for higher risk disease, results in improved prostate cancer control rates when compared to external beam radiotherapy alone. Improvements in brachytherapy technology have refined dose delivery with the more widespread introduction of HDR after loading devices, more sophisticated computerized treatment planning systems and the incorporation of 3D imaging into the planning process. This chapter provides an overview of the techniques, indications and clinical outcomes for both LDR and HDR prostate brachytherapy.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others
Keywords
- External Beam Radiotherapy
- Clinical Target Volume
- High Dose Rate
- Luteinizing Hormone Release Hormone
- Prostate Brachytherapy
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Brachytherapy (derived from the Greek word brachys meaning ‘short-distance’) is a form of radiation therapy where a sealed radiation source is placed directly into the body. In prostate brachytherapy, the placement of radiation sources in the gland can be permanent or temporary. Both are forms of interstitial brachytherapy, which is defined as the insertion of brachytherapy applicators or sources directly into tissue i.e. the prostate gland.
Permanent interstitial brachytherapy, also known as seed brachytherapy, involves placing small radioactive pellets into the prostate and leaving them permanently to gradually release radiation over time. After all the radiation has decayed the inactive pellets remain in the prostate gland. Permanent brachytherapy uses low dose rate (LDR) sources emitting radiation over weeks and months.
Temporary brachytherapy involves first placing needles or catheters within the prostate and, on confirmation of accurate positioning, temporarily introducing the radioactive source into the prostate. Radiation is delivered using a high dose rate (HDR) machine where actual treatment times are minutes. The radiation dose rate is very similar to that used in external beam radiotherapy. Comparisons of LDR and HDR prostate brachytherapy treatments are listed in Table 1.
Prostate brachytherapy allows safe radiation dose escalation beyond that achieved using external beam radiotherapy alone as it has greater conformity around the prostate, sparing surrounding rectum and bladder. In addition, there are fewer issues with changes in prostate position during treatment delivery. Randomized trials using both techniques demonstrate improved disease control when compared to external beam radiotherapy alone [1, 2].
2 Permanent Prostate Brachytherapy Techniques
The breakthrough in the development of modern brachytherapy was the establishment in the early 1980s of trans-rectal ultrasound (TRUS) combined with the use of a template attached to the TRUS probe to guide trans-perineal needle placement [3]. The procedure was refined by the Seattle group [4] and remains the most commonly used permanent prostate brachytherapy technique.
2.1 Patient Preparation
The procedure is often done as a day-case under general or regional anaesthesia (spinal or caudal blocks). An empty rectum helps optimize TRUS images and the patient should have an enema before the procedure to clear the rectum. Once anaesthetized, the patient is placed in the lithotomy position and a Foley catheter introduced to visualize the urethra. Aerated gel (lubricating gel plus air to make small bubbles) can be used to help visualize the urethra. The scrotum is moved away from the operating field and fixed with an adhesive dressing; the perineum is then cleaned with antiseptic solution.
2.2 TRUS Volume Study
The ultrasound probe placed within the stepper unit (Fig. 1) is inserted into the rectum and positioned under the prostate. The stepping unit can make steps (generally at 5 mm transverse intervals) through the prostate acquiring an image dataset which is then used to contour the prostate volume and adjacent organs at risk (urethra, rectum, bladder neck, neurovascular bundles). Attached to the trans-rectal ultrasound is a perineal template. The coordinates of the template are automatically transposed over the ultrasound images of the prostate.

Trans-rectal ultrasound (TRUS) probe placed within stepper unit allows TRUS image acquisition at 5 mm intervals from prostate base to apex. The trans-perineal template attached to the stepper unit guides accurate needle placement during the implant
The prostate is positioned so that it lies centrally within the template grid with the lower border on the first row and the urethra centred on the middle row (large D). Care should be taken to ensure the prostate is not angled or rotated around its axis. Once the prostate is accurately positioned relative to the template, serial sections are taken from the base to apex at 5 mm intervals. On each section, the prostate capsule is contoured and the information analysed within a planning computer to calculate the exact number and position of seeds required for the implant (Fig. 2).

TRUS prostate image with prostate capsule outlined in red and planned seed positions represented by green dots. The coordinates of the template (letters on x-axis and numerals on y-axis) are superimposed on the TRUS image to guide accurate needle placement. The varying radiation isodose lines are displayed in the key. In I-125 brachytherapy the dose (145 Gy) is prescribed to the 100 % isodose (yellow line) which should encompass the entire prostate with a 3 mm margin apart from posteriorly adjacent to the rectum where no margin is applied (CTV: light blue line)
2.3 Treatment Planning and Implantation
The planning and implantation technique may follow one of the following depending on departmental preferences and experience [5]:
-
1.
Pre-planning: A two-step procedure where there is delayed execution of the treatment plan. The TRUS pre-plan takes place a few weeks before actual implantation.
-
2.
Intraoperative planning: The plan is created in the operating room immediately prior to the procedure.
-
3.
Interactive planning: Stepwise modification of the plan using computerized dose calculations that have been obtained from image-based needle-position feedback.
-
4.
Dynamic dose calculation: Constant updating of the dose distribution using continuous seed position feedback.
Typically about 80–100 seeds will be implanted using 25–30 needles, but the precise number will depend on the prostate size/shape and the activity of the seeds. The needles are 20 cm long (18 gauge). A modified peripheral loading pattern is used where the majority of seeds are positioned adjacent to the capsule and a smaller number placed centrally but away from the urethra.
The needles are guided through the perineal skin using the template that provides the X and Y co-ordinates with the depth (Z co-ordinate) confirmed using sagittal ultrasound imaging. Seed positions are referenced to the base plane defined as where the prostate meets the bladder base. Not all needles are inserted as far as the base plane, some are inserted closer to the apex to provide seed coverage more proximally. Stranded or linked seed trains are often used as this reduces seed migration into the peri-prostatic venous circulation. A Mick applicator can be used to insert single or ‘loose’ seeds into gland.
The most frequently used isotope for permanent seed implantation is Iodine-125. It has a mean energy of 25 KeV with a half-life of 59.6 days. The Iodine-125 is absorbed onto a silver rod, which is encased in a titanium case. The overall size of seeds is just under 5 mm long and 1 mm in diameter. In the early years of permanent prostate brachytherapy Palladium-103 was used, citing a theoretical advantage for more rapidly growing tumours as it has a shorter half-life (i.e. higher dose rate) than Iodine-125, but with long-term follow-up no clinical advantage has been demonstrated. The prescribed dose when using Iodine-125 is 145 Gy for monotherapy and 110 Gy when used as a boost treatment with supplemental external beam radiotherapy.
Detailed GEC-ESTRO (Groupe Europeen de Curietherapie -European Society of Therapeutic Radiation Oncology) guidelines on the clinical and technical aspects of permanent prostate brachytherapy are recommended [6, 7]. The clinical target volume (CTV) is defined as the prostate gland plus a 3 mm margin in each direction. This can be constrained to the rectum posteriorly and the bladder neck cranially.
The dose distribution inside a prostate implant is highly non uniform and doses can be considerably higher than the minimum peripheral dose to the CTV. The GEC-ESTRO recommends that the following dosimetric parameters should be aimed for and recorded:
Clinical Target Volume (CTV)
-
V100 CTV (percentage of the CTV that receives the prescription dose) ≥95 %
-
V150 CTV (percentage of the CTV that receives the 150 % prescription dose) ≤50 %
-
D90 CTV (dose that covers 90 % of the CTV) > prescription dose
Rectum
-
D2cc rectum (the minimum dose in the most irradiated 2 cc volume of the rectum) < prescription dose
-
D0.1 cc rectum (the minimum dose in the most irradiated 0.1 cc volume of the rectum) <200 Gy
Urethra
-
D10% urethra (the minimum dose in the most irradiated 10 % of the urethral volume) <150 % of prescription dose
-
D30% urethra (the minimum dose in the most irradiated 30 % of the urethral volume) <130 % of the prescription dose
2.4 Quality Assurance
Practice guidelines to ensure high quality training and quality assurance have been published following errors in US centres, where poor quality implants led adverse patient outcomes [8–10]. It is recommended that all patients undergo post implantation CT based dosimetry to compare the actual dose delivered to the treatment plan. If available, MR-CT fusion is a useful tool to more accurately evaluate seed placement relative to the prostate capsule (Fig. 3). The optimal timing of imaging has not been established and it can be undertaken Day 0, 1 or 2–6 weeks following the implant. Post-implant dosimetry should measure the following parameters: Prostate D90%, V100%, V150% and organ at risk doses (urethra and rectum). Post-implantation results should be reviewed and action, such as re-implantation, undertaken to compensate for sub-optimal treatment in individual patients. The impact on post-implant dosimetry of changes in personnel or implant technique should also be assessed by regular review, as a learning curve for permanent prostate brachytherapy is well described.

Post Implant dosimetry should be undertaken in all seed brachytherapy patients to check actual dose delivered. (a) Pelvic CT scan demonstrating seeds within gland. (b) CT can be fused with MRI to aid prostate capsule identification
2.5 Radiation Protection
The low emission energy of the seeds and the ease of shielding mean that seed loading and implantation can be undertaken without the need for significantly increased radiation protection measures in the operating theatre.
Following implantation, men and their families should be given radiation protection advice both verbally and on an information card. This advice should include this information;
-
Avoid close (<1 m) contact with young children and pregnant women in the first 2 months following implantation.
-
Partners can safely sleep in the same bed.
-
Sex can resume when comfortable after implantation but condoms should be used for the first 5 ejaculations, then flushed away.
-
Should a seed be passed pick it up with a spoon or long handled tweezers and flush away.
-
In the event of death within 20 months of implantation cremation is not allowed.
-
Airport radiation monitors may be triggered up to 6 months after and a wallet sized information card should be carried with information for airport security staff.
3 Indications for Permanent Prostate Brachytherapy
3.1 Monotherapy in Localized Prostate Cancer
Non-metastatic prostate cancer is stratified into risk groups depending on PSA, T stage and Gleason score. In broad terms, low risk is defined as T1/T2a, PSA ≤10 ng/mL and Gleason score 6, intermediate risk as T1/2 and/or PSA 10–20 ng/mL and/or Gleason 7 and high risk as any having one of the following features T3-4, PSA >20 ng/mL or Gleason 8–10. Stratification into these risk categories helps guide treatment choices and predicts long term outcomes.
Patients with low risk localized prostate cancer (T1c-T2a, Gleason 6, <50 % core positive, PSA ≤10 ng/mL) and selected patients with low volume intermediate risk localized prostate cancer (T1c-T2a, Gleason 3 + 4, PSA ≤10 ng/mL, <33 % core positive) are suitable for permanent prostate brachytherapy alone (Table 2).
Men with pre-existing urinary symptoms and/or enlarged prostate glands are at high risk of acute retention of urine after brachytherapy and/or experiencing prolonged urinary symptoms. The patient completed International Prostate Symptom Score (IPSS) can be used to screen for significant pre-existing urinary symptoms with a score <9 being ideal and scores <15 acceptable [11]. A more objective measure of urinary function can be obtained from urinary flow tests. Men with peak urinary flow rates of <10 ml/s have a 30 % risk of post-implant retention and brachytherapy is generally not advised. Those with peak flow rates >20 ml/s have <10 % risk of catheterization and are good candidates for brachytherapy [12].
In patients with enlarged prostate glands (over 50 ml) it can be difficult to achieve good implantation of the gland because the pubic arch may shield the anterior prostate. Neo-adjuvant androgen deprivation for 3–6 months before implantation can be used to downsize the gland with the greatest gland shrinkage achieved using luteinizing hormone releasing hormone (LHRH) agonists rather than anti-androgens [13]. LHRH agonists will often achieve a 30 % reduction in prostate size.
Previous trans-urethral resection of the prostate (TURP) is a relative contra-indication to prostate brachytherapy particularly if there is a large prostate defect. The presence of a significant defect makes it difficult to achieve a satisfactory dose distribution. Patients who have had a TURP a number of years before or those where a more recent narrow channel procedure has been undertaken can be considered for brachytherapy.
3.2 Boost Treatment with External Beam Radiotherapy in Intermediate and High Risk Disease
In patients with intermediate and high risk localized prostate cancer there is a significant risk of microscopic extra-capsular spread that may not be included in the high dose region of a seed implant leading to local treatment failure. In this situation brachytherapy may be combined with external beam radiotherapy to ensure an appropriate target volume is treated. External beam doses in the order of 46 Gy in 23 fractions are delivered to either prostate and seminal vesicles or whole pelvis with a boost of 110 Gy delivered to the prostate using 1–125 permanent prostate brachytherapy [2]. Neo-adjuvant and adjuvant hormone manipulation should also be considered as standard care.
4 Results for Permanent Prostate Brachytherapy
There have been no randomized trials comparing brachytherapy as monotherapy with other curative treatment modalities. Outcome data are available from a number of large cohort studies with mature follow-up [14–22]. The biochemical control for low risk patients has been reported to range from 72 to 98 % with follow-up out to 12 years. Morris et al. [22] reported the population based outcomes from British Colombia, Canada and demonstrated biochemical disease-free survival of 94 % at 10 years in low and selected intermediate risk patients. For all series, outcomes for intermediate risk patients vary from 61 to 96 % which is likely to reflect variation in patient selection.
A significant correlation has been shown between the implanted dose and recurrence rates [23]. Patients receiving a D90 (dose covering 90 % of the prostate volume) of >140 Gy had a significantly higher biochemical control rate (PSA < 1.0 ng/mL) after 4 years than patients who received less than 140 Gy (92 vs. 68 %). There is no benefit in adding neo-adjuvant or adjuvant ADT to LDR monotherapy [14].
Dose-escalated external beam radiotherapy has been compared with external beam radiotherapy followed by a LDR brachytherapy boost in intermediate-risk and high-risk patients in a recently presented randomized trial [2]. The ASCENDE-RT (Androgen Suppression Combined with Elective Nodal and Dose Escalated Radiation Therapy) multi-centre Canadian trial compared external beam (total dose of 78 Gy) to external beam (total dose 46 Gy) followed by LDR brachytherapy boost (prescribed dose 115 Gy). With a median follow-up of 6.5 years, a significant improvement in recurrence-free survival at 7 years was found, increasing from 71 % in the dose escalated external beam alone arm to 86 % in the LDR boost arm. This was associated with a higher rate of late urinary morbidity with a 5-year cumulative Grade 3 toxicity rate of 19 % in the LDR boost arm compared to 5 % in the external beam radiotherapy alone arm [24]. Approximately 50 % of the urinary toxicity was due to urethral strictures and it is recommended that a boost dose of 110 Gy rather than 115 Gy should be used in routine practice. Care should also be taken not to over-treat the membranous urethra distal to the prostate apex when using this technique. In addition, although associated with improved recurrence-free survival, use of LDR boost had a significant negative impact on health related quality of life (HRQoL) for urinary and sexual function, general health and bodily pain [25].
5 Morbidity
5.1 Urinary Morbidity
Immediate post-implantation side effects are predominantly urinary. Irritative and obstructive urinary symptoms are very common in the first 2–3 weeks and are relieved by alpha-blocker drugs. Alpha-blockers should be commenced just before the procedure and may need to be continued for several months afterwards until urinary symptoms resolve. Regular anti-inflammatory use will help with pain and discomfort on passing urine. Acute urinary retention can occur in 10–20 % of patients and is managed by urethral catheterization. This usually resolves within 4–6 weeks but in the few patients with on-going problems intermittent self-catheterization effectively manages this symptom. In 95 % of men, urinary symptoms have resolved by 12 months. It is advisable to avoid TURP in the first 12 months, as this is associated with risks of urethral necrosis and incontinence. A narrow-channel TURP can be undertaken after this if outflow symptoms persist.
5.2 Rectal Morbidity
Rectal side effects are usually mild with a minority experiencing rectal discomfort, proctitis and rectal bleeding, which usually resolves within 12 months of treatment. There is a small risk of rectal ulceration and development of recto-prostatic fistulae (0.1–0.2 %).
5.3 Sexual Dysfunction
Erectile dysfunction develops in about 40 % of the patients after 3–5 years. The risk is less in younger men who are fully potent pre-treatment and greater in older men who may already have reduced potency. Daily sildenafil can be used prophylactically for the first 6 months following treatment to help maintain sexual function [26].
5.4 Health Related Quality of Life
It is increasingly recognized that patient outcomes measured objectively using validated health related quality of life (HRQoL) questionnaires allow measurement and comparison of how different treatment options impact the individual’s life in a valid and reproducible way. The most robust information about long term HRQoL following treatment for prostate cancer is from randomized trials where groups have balanced baseline characteristics. Attempts to recruit patients into Phase III trials comparing radical prostatectomy versus permanent prostate brachytherapy have been unsuccessful as a significant proportion of informed patients feel unable to commit to a random allocation of treatment. The SPIRIT trial closed early but a comparison of HRQoL at a median of 5.2 years after treatment with either prostatectomy or brachytherapy (no neo-adjuvant hormone use) has been published [27]. This cross-sectional study assessed 168 trial eligible men 3.2–6.5 years after treatment and demonstrated those who had I-125 brachytherapy had better urinary, sexual and patient satisfaction scores than men undergoing radical prostatectomy.
Prospective longitudinal studies comparing non-randomized cohorts of patients undergoing prostatectomy, brachytherapy or external beam radiotherapy without hormone manipulation demonstrate that 3–5 years after treatment brachytherapy patients have less urinary incontinence, bowel effects and sexual dysfunction but more urinary irritative-obstructive symptoms [28–30]. There does appear to be a trend to decreased sexual function with time in brachytherapy patients, which may be related to increasing age and/or a late effect of radiation [28]. Sanda et al. included men who had neo-adjuvant hormone treatment in a multi-centre prospective longitudinal study of brachytherapy, external beam radiotherapy and radical prostatectomy [31]. The use of hormone manipulation in brachytherapy patients was associated with more sexual dysfunction and hormonal symptoms in the first 12 months after treatment but by 2 years function had returned to a level similar to that of the cohort who had brachytherapy alone.
6 Temporary High Dose Rate (HDR) Prostate Brachytherapy Techniques
6.1 Advantages of HDR Prostate Brachytherapy
Although permanent prostate brachytherapy has been the most commonly used prostate brachytherapy technique to date, temporary high dose rate (HDR) brachytherapy techniques using after-loading machines are now increasingly used. HDR is most commonly used as a boost treatment in intermediate and high risk patients combined with external beam radiotherapy.
The principal differences are:
-
Applicators (needles or catheters) are inserted into the prostate ± seminal vesicles and post-implant dosimetry undertaken with no pre-plan required.
-
There is more scope to treat extra-capsular and seminal vesicle disease as applicators can be placed into tissues adjacent to the prostate.
-
There is more flexibility in dosimetry and the technique is less operator dependent.
-
Dose is delivered in large fraction sizes and this may have a biological advantage when treating prostate cancer.
-
HDR brachytherapy is a cost effective option as a single source is repeatedly used for treatments.
-
Use of after-loading means minimal radiation protection issues for staff and patients.
After-loading systems were developed from the 1970s onwards as a way of reducing the radiation exposure to medical and nursing staff. After-loading involves the initial placement of a non-radioactive applicator (metal needles or plastic catheters) into the patient followed by the subsequent insertion of the radioactive isotope. Radiation is then delivered ‘remotely’ with the staff outside the room by computer control of a treatment machine inside the room. With appropriately shielded rooms this technique permits high dose-rate treatments with high activity sources. Modern HDR machines generally use a small iridium-192 source which is stepped through a series of dwell positions in all the treatment needles/catheters in turn, thereby removing the need for several sources or source trains to be present in the machine. Complex 3D dose distributions can be produced from the large combination of dwell times and positions.
6.2 Treatment Planning and Implantation
Patient preparation and positioning are identical to LDR brachytherapy. The patient undergoes general or regional anaesthesia, has a urethral catheter inserted and is placed in the lithotomy position. Trans-rectal ultra-sound is used to guide HDR applicator insertion in the same manner as LDR brachytherapy. Applicators may be hollow blind ending metal needles (re-useable) or plastic catheters (disposable). Applicators are inserted around the periphery of the prostate, generally 1 cm apart, with a small number centrally (Fig. 4). Additional applicators can be inserted into regions of gross tumour to facilitate higher dose delivery in these sub-volumes.

Metal needles used for HDR brachytherapy inserted through trans-perineal template into the prostate gland at approximately 1 cm intervals around the periphery of the gland under trans-rectal ultrasound guidance
Once the applicators are positioned, they are held fixed within the perineal template. If multiple fractions of HDR brachytherapy are planned using the same implant, a means of fixing the perineal template to the perineum will be required. This is usually involves suturing the template to the perineum or use of an adhesive dressing.
After inserting the applicators, 3D imaging is acquired and imported into the computerized treatment planning system so that a treatment plan with dwell positions and timings for the radioactive source can be generated. Imaging with ultrasound, MR and/or CT can all be used to plan HDR treatments. There are two general approaches:
-
1.
Trans-rectal ultrasound obtained whilst the patient remains in the lithotomy position under anaesthetic or sedation, known as real-time US guidance;
-
2.
CT or MR images obtained following recovery from anaesthetic and transfer to the imaging department.
Real-time US imaging in theatre provides good organ definition and allows in-room treatment without the need to change patient positioning. Alternatively, CT or MRI may be used but necessitates moving the patient for imaging and subsequent treatment. In this second situation, quality assurance is essential to ensure that catheters do not move with change in patient positioning. As a minimum, the distal catheter length from the perineal template to the connecting hub should be measured and checked at each step to ensure catheters have not shifted position. If multiple HDR fractions are to be delivered using the same implant a number of hours apart imaging should be re-acquired before each fraction and treatment re-planned or catheters adjusted if clinically relevant changes are found.
Once the 3D image set (either US, CT or MR) is acquired, the following volumes for treatment planning are defined on the planning images (Fig. 5):

Trans-rectal ultrasound images of the prostate with implanted HDR needles imported into computerised treatment planning system. Prostate (red), rectum (green) and urethra contoured. Clinical Target Volume (CTV) generated by expanding prostate contour
-
Clinical target volume (CTV) including the prostate capsule plus any macroscopic extra-capsular disease or seminal vesicle involvement identified on diagnostic images expanded by 3 mm to encompass potential microscopic disease. This is usually constrained posteriorly to the anterior rectal wall and superiorly to the bladder base;
-
Gross tumour volume (GTV) may be defined, if this sub-volume is being boosted, using information from previous diagnostic imaging
-
Rectum defined as outer rectal wall
-
Urethra using the urethral catheter as the landmark on imaging for the urethral contour, which should extend from bladder base to 5–10 mm below the prostatic apex. Contrast such as aerated gel within the catheter will aid visualization on ultrasound
-
Other adjacent organs at risk such as penile bulb, bladder neck and neurovascular bundles may be outlined (optional)
In the treatment planning system through optimization, a balance will be reached between dose to the CTV (± GTV) and the adjacent organs at risk (rectum and urethra). The prescription dose is defined as D90CTV i.e. the dose delivered to 90 % of the CTV. This is individualized for each patient and should be higher than the planning aim, i.e. >100 % (Fig. 6).

HDR Treatment planning system generates the optimal radioactive source dwell times and positions to ensure good coverage of the CTV and minimal dose to the urethra and rectum
The heterogeneity of dose delivered using varying external beam and HDR brachytherapy schedules makes the definition of generalized maximal rectal and urethral doses difficult and the reader should refer to comprehensive guidelines [32].
There are no data available on which recommendations for constraints for penile bulb or neurovascular bundles can currently be made and detailed long term follow-up in cohorts receiving HDR brachytherapy is required.
Once treatment is planned and checked connecting tubes from the HDR treatment machine are attached to each applicator. All staff must leave the HDR treatment room and the patient is observed using remote monitors and CCTV. Treatment delivery times are generally of the order of minutes (Fig. 7).

Patient ready for HDR treatment. Connecting tubes between implanted prostate needles and treatment machine are in place. All staff will leave treatment room during treatment delivery and patient will be monitored remotely
On completion of treatment the applicators, template and urinary catheter are removed.
7 HDR Brachytherapy Indications
7.1 HDR Brachytherapy Boost with External Beam
HDR brachytherapy combined with external beam radiotherapy is a treatment option for patients with intermediate and high risk localized disease, but in addition also an option for those with locally advanced and pelvic node positive prostate cancer. The exclusion criteria are similar to LDR brachytherapy apart from the ability to implant glands up to 60 cm3 and treat patients with higher initial IPS scores (Table 3).
There is no consensus regarding the timing of brachytherapy in relation to external beam radiotherapy and it can be delivered before, during or after. There are also a wide range of external beam volumes and treatment schedules reported in the literature, and it is not possible to recommend one specific prescription. Published schedules include the following:
-
45 Gy in 25 fractions over 5 weeks
-
46 Gy in 23 fractions over 4.5 weeks
-
35.7 Gy in 13 fractions over 2.5 weeks
-
37.5 Gy in 15 fractions over 3 weeks
HDR brachytherapy planning aim doses, defined as a minimum peripheral dose, which have been prescribed with these schedules include:
-
15 Gy in 3 fractions
-
11–22 Gy in 2 fractions
-
12–15 Gy in 1 fraction
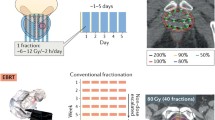
It is not possible to make a firm recommendation on planning aim dose; the randomized trial providing level 1 evidence used 17 Gy in 2 fractions (after 35.7 Gy in 13 fractions external beam) [1]. The need for fractionation and repeated treatments has been a logistical disadvantage for HDR brachytherapy but increasingly, a single dose of 15 Gy is gaining acceptance [35, 36].
There is evidence from a large cohort study that after 45 Gy in 25 fractions external beam a dose response exists up to 22 Gy in 2 fractions [33]. An analysis of the dose prescribed and volume treated in patients in a randomized trial has also shown that biochemical control is higher in with a higher delivered dose and volume covered [34].
7.2 HDR Monotherapy
HDR ‘monotherapy’ is associated with low acute toxicity and high biochemical control rates in the limited series published to date [37–44].
The schedules (planning aim) used include:
-
54 Gy in 9 fractions
-
44 Gy in 6 fractions
-
34 Gy in 4 fractions
-
36–38 Gy in 4 fractions
-
31.5 Gy in 3 fractions
-
26 Gy in 2 fractions
-
19–21 Gy in 1 fraction
Older series have used multiple fractions of HDR but more recent studies are using one or two fractions. Long- term outcome data are not yet available from these cohorts and it is recommended that this treatment is not undertaken outside clinical trials.
7.3 HDR in Recurrence After Previous Radiation
There is limited experience of HDR brachytherapy for locally recurrent prostate cancer after previous irradiation and this is not recommended outside a formal prospective study. Recurrence should be proven by prostate biopsy and patients staged to exclude metastatic disease. Organ at risk constraints are critical in this setting with a significant risk of toxicity due to bladder neck strictures or fistulation. Published schedules (planning aim) include the following:
8 Results
8.1 Results for HDR Prostate Brachytherapy
Multiple single centre series with mature follow-up demonstrate that HDR boost with external beam results in high rates of biochemical control and low toxicity [32, 47]. Biochemical control rates are on average 95 % for low risk, 91 % for intermediate risk and 82 % for high risk disease. Spratt et al. in a single institutional series compared outcomes of contemporaneously treated intermediate risk patients and found that those treated with brachytherapy boost (either LDR or HDR) had improved biochemical disease-free survival and distant metastases-free survival when compared to those treated with dose escalated intensity modulated radiotherapy (IMRT) to a total dose of 86.4 Gy [48]. At a median follow-up of 5.3 years biochemical disease-free survival was 92 % versus 81 %, and distant metastases-free survival 97 % versus 93 % in the brachytherapy boost patients versus IMRT alone patients respectively.
A randomized trial of external beam radiotherapy compared to external beam radiotherapy and HDR brachytherapy boost has been reported [1]. A total of 218 patients with intermediate and high risk prostate cancer were randomized to external beam alone to a dose of 55 Gy in 20 fractions, or external beam to a dose of 35.75 Gy in 13 fractions, followed by HDR brachytherapy to a dose of 17 Gy in two fractions over 24 h. In comparison with external beam alone, the combination showed a significant improvement with 5-, 7- and 10-year estimates of biochemical control at 75, 66 and 46 % for combination treatment compared to 61, 48 and 39 % for external beam alone. No differences in overall survival were noted at a median follow-up time of 85 months. The relatively low total radiation dose in the control arm has been criticized. An on-going trial of the National Cancer Institute of Canada (Clinical Trials. Gov identifier NCT01982786) randomizes patients with intermediate risk disease to either an HDR boost of 15 Gy combined with 37.5 Gy external beam radiotherapy or dose escalated external beam radiotherapy (either 78 Gy in 39 fractions or 60 Gy in 20 fractions) and will provide data on whether dose escalation using HDR boost results in improved disease-free survival when compared to modern dose-escalated radiotherapy.
A systematic review of non-randomized trials has suggested that outcomes with external beam radiotherapy plus HDR brachytherapy are superior to external beam alone or external beam with permanent seed boost [49].
Single centre studies of HDR monotherapy have demonstrated promising results.
Results from the group at California Endocurietherapy, UCLA show 6 and 10-year biochemical control rates of 98 and 97 % in a cohort of 448 low and intermediate risk patients treated over a 13 year period with a median dose of 43.5 Gy in 6 fractions [40]. No significant late rectal toxicity occurred and late (Grade 3+) urinary toxicity occurred in <5 % after a median follow-up of 6.5 years. Yoshioka et al. reported 93 % and 79 % 5-year biochemical control rates for intermediate and high risk patients respectively using a 7- and 9-fraction protocol [38]. Treatment schedules using fewer fractions are also being investigated and have been shown to have acceptable toxicity [37, 43]. Results on biochemical control rates are awaited and monotherapy remains investigational.
9 HDR Brachytherapy Morbidity
9.1 Urinary Morbidity
Urinary symptoms are common in the 2–3 weeks following HDR brachytherapy but have usually resolved by 6 weeks post-implantation. Dysuria may last for a few days following treatment but is less severe than that associated with LDR brachytherapy. Obstructive symptoms can be relieved with the use of alpha-blockers.
Martinez et al. showed a significantly lower rate of acute dysuria (39 % versus 60 %), frequency/urgency (58 % versus 90 %) and acute rectal pain (6.5 % versus 17 %) with HDR monotherapy compared with LDR monotherapy using palladium-103 seeds [50]. Although late grade 3 toxicity was rare with either technique, there was a significantly increased rate of chronic urinary toxicity with LDR, and a comparable rate of late urethral stricture (3 % versus 1.5 %). Urethral dose seems to be predictive of late urinary symptoms and urinary morbidity can probably be decreased with careful technique to minimize the dose to the urethra [51].
The reported rate of late grade 3 urinary toxicity after HDR boost and external beam radiotherapy is around 5 % (range 2–20 %), with the rate of urethral stricture between 0 and 7 % [52].
9.2 Bowel Morbidity
HDR brachytherapy results in low rectal morbidity. In patients undergoing HDR and external beam radiotherapy, bowel symptoms are generally due to the external beam radiotherapy component. Fewer acute gastrointestinal side effects were noted in the randomized trial comparing external beam alone with external beam and HDR brachytherapy [1], although there was no long term differences. Late rectal toxicity is rarely seen with HDR monotherapy.
9.3 Sexual Dysfunction
Erectile dysfunction is reported in 10–47 % of cases. Patients treated with neo-adjuvant and adjuvant hormone manipulation will experience higher rates of erectile dysfunction.
Conclusions
Prostate brachytherapy is a well-established curative treatment option for men with non-metastatic prostate cancer.
LDR monotherapy for low and selected intermediate risk prostate cancer results in durable prostate cancer progression-free survival. Long term sexual dysfunction, bowel symptom and urinary incontinence rates are lower than that seen with the alternative treatment options.
In intermediate and high risk prostate cancer the use of brachytherapy boost, either HDR or LDR, in addition to external beam radiotherapy improves progression-free survival. Additional long term toxicity has been found and there is a need to demonstrate that refinements in brachytherapy techniques can deliver improved patient outcomes both in terms of cancer control rates and toxicity.
References
Hoskin PJ, Rojas AM, Bownes PJ, et al. Randomised trial of external beam radiotherapy alone or combined with high-dose rate brachytherapy boost for localised prostate cancer. Radiother Oncol. 2012;103(2):217–22.
Morris W, et al. LDR brachytherapy is superior to 78 Gy of EBRT for unfavourable risk prostate cancer: the results of a randomized trial. Radiother Oncol. 2015;115:S239.
Holm HH, Juul N, Pedersen JF, et al. Transperineal125 iodine seed implantation in prostatic cancer guided by transrectal ultrasonography. J Urol. 1983;130:283–6.
Blasko JC, Radge H, Schumacher D. Transperineal percutaneous iodine-125 implantation for prostatic carcinoma using transrectal ultrasound and template guidance. Endocurie/Hypertherm Oncol. 1987;3:131–9.
Nag S, et al. Intraoperative planning and evaluation of permanent prostate brachytherapy: report of the American Brachytherapy Society. IJROBP. 2001;51(5):1422–30.
Ash D, Flynn A, Batterman J, et al. ESTRA/EAU Urological Brachytherapy Group; EORTC Radiotherapy Group. ESTRO/EAU/EORTC recommendations on permanent seed implantation for localized prostate cancer. Radiother Oncol. 2000;57(3):315–21.
Salembier C, Lavagnini P, Nickers P, et al. GEC ESTRO PROBATE Group. Tumour and target volumes in permanent prostate brachytherapy: a supplement to the ESTRO/EAU/EORTC recommendations on prostate brachytherapy. Radiother Oncol. 2007;83(1):3–10.
Department of veterans affairs office of inspector general health inspection: review of brachytherapy treatment of prostate cancer, Philadelphia, Pennsylvania and Other VA Medical Centers Report No. 09-02815-143. Washington, DC: VA Office of Inspector General. 2010.
Davis BJ, Horwitz EM, Lee W, et al. American Brachytherapy Society consensus guidelines for transrectal ultra-sound guided permanent prostate brachytherapy. Brachytherapy. 2012;11(1):6–19.
The Royal College of Radiologists. Quality assurance practice guidelines for transperineal LDR permanent seed brachytherapy of prostate cancer. London: The Royal College of Radiologists; 2012.
Gelblum DY, Potters L, Ashley R, et al. Urinary morbidity following ultra-sound guided transperineal prostate seed implantation. IJROBP. 1999;45:59–67.
Martens C, et al. Relationship of the international prostate symptom score with urinary flow studies and catheterization rates following I-125 prostate brachytherapy. Brachytherapy. 2006;5:9–13.
Lee WR. The role of androgen deprivation therapy combined with prostate brachytherapy. Urology. 2002;37:565–9.
Sylvester JE, Grimm PD, Wong J, Galbreath RW, Merrick G, Blasko JC. Fifteen-year biochemical relapse-free survival, cause-specific survival, and overall survival following I(125) prostate brachytherapy in clinically localized prostate cancer: Seattle experience. Int J Radiat Oncol Biol Phys. 2011;81(2):376–81.
Potters L, Morgenstern C, Calugaru E, et al. 12-year outcomes following permanent prostate brachytherapy in patients with clinically localized prostate cancer. J Urol. 2005;173(5):1562–6.
Stone NN, Stone MM, Rosenstein BS, et al. Influence of pretreatment and treatment factors on intermediate to long-term outcome after prostate brachytherapy. J Urol. 2011;185:494–500.
Zelefsky MJ, Chou JF, Pei X, et al. Predicting biocehmical control after brachytherapy for clinically localized prostate cancer: the Memorial Sloan-Kettering Cancer Centre experience. Brachytherapy. 2012;11:245–9.
Lawton CA, DeSilvio M, Lee WR, et al. Results of a phase II trial of transrectal ultrasound-guided permanent radioactive implantation of the prostate for definitive management of localized adenocarcinoma of the prostate (RTOG 98–05). Int J Radiat Oncol Biol Phys. 2007;67(1):39–47.
Henry AM, Al-Qaisieh B, Gould K, et al. Outcomes following iodine-125 monotherapy for localized prostate cancer: the results of Leeds 10-year single-center brachytherapy experience. Int J Radiat Oncol Biol Phys. 2010;76:50–6.
Hinnen KA, Battermann JJ, van Roermond JGH, et al. Long term biochemical and survival outcome of 921 patients treated with I-125 permanent prostate brachytherapy. Int J Radiat Oncol Biol Phys. 2010;76:1433–8.
Grimm PD, Billiet I, Bostwick D, et al. Comparative analysis of prostate specific antigen free survival outcomes for patients with low, intermediate and high risk prostate cancer treatment by radical therapy. Results from the Prostate Cancer Results Study Group. BJU Int. 2012;109(Suppl1):22–9.
Morris WJ, Keyes M, Spadinger I, et al. Population-based 10-year oncologic outcomes after low-dose-rate brachytherapy for low-risk and intermediate-risk prostate cancer. Cancer. 2013;119(8):1537–46.
Stock RG, Stone NN. Importance of post-implant dosimetry in permanent brachytherapy. Eur Urol. 2002;41(4):434–9.
Rodda SL, Tyldesley S, Morris WJ. Toxicity outcomes in ASCENDE-RT: a multicenter randomized trial of dose-escalation trial for prostate cancer. IJROBP. 2015;93(3):S121.
Rodda SL, Duncan G, Hamm J, Morris WJ. Quality of life outcomes: ASCENDE-RT a multicentre randomized trial of radiation therapy for prostate cancer. IJROBP. 2015;93(3):S2.
Zelefsky MJ, Shasha D, Branco RD, et al. Prophylactic sildenafil citrate for improvement of erectile function in men treated by radiotherapy for prostate cancer. J Urol. 2014;192(3):868–74.
Crook JM, Gomez-Iturriaga A, Wallace K, et al. Comparison of health-related quality of life 5 years after SPIRIT: surgical prostatectomy versus interstitial radiation intervention trial. JCO. 2011;29:362–8.
Pardo Y, Guedea F, Aguilo F, et al. Quality of life impacts of primary treatments for localized prostate cancer in patients without hormonal treatment. JCO. 2010;28:4687–96.
Chen RC, Clark JA, Talcott JA. Individualizing quality-of-life outcomes reporting: how localized prostate cancer treatments affect patients with different levels of baseline urinary, bowel and sexual function. JCO. 2009;27:3916–22.
Ferrer M, et al. Quality of life impact of treatments for localized prostate cancer: cohort study with a 5-year follow-up. Radiother Oncol. 2013;108(2):306–13.
Sanda MG, Dunn RL, Michalski J, et al. Quality of life and satisfaction with outcomes among prostate-cancer survivors. New Engl J Med. 2008;358:1250–61.
Hoskin PJ, Colombo A, Henry A, et al. GEC/ESTRO recommendations on high dose rate afterloading brachytherapy for localised prostate cancer: an update. Radiother Oncol. 2013;107(3):325–32.
Martinez AA, Gonzalez J, Ye H, et al. Dose escalation improves cancer related events at 10 years for intermediate and high risk prostate cancer patients treated with hypofractionated high-dose-rate boost and external beam radiotherapy. IJROBP. 2011;79(2):363–70.
Hoskin P, Rojas A, Ostler P, et al. Dosimetric predictors of biochemical control of prostate cancer in patients randomised to EBRT with a boost of HDR. RO. 2014;110:110–3.
Morton G, Loblaw DA, Sankreacha A, et al. Single-fraction high dose rate brachytherapy and hypofractionated external beam radiotherapy for men with intermediate risk prostate cancer: an analysis of short and medium term toxicity and quality of life. Int J Radiat Oncol Biol Phys. 2010;77:811–7.
Morton G, Loblaw A, Cheung P, Szumacher E, Chahal M, Danjoux C, Chung HT, Deabreu Mamedov A, Zhang L, Sankreacha R, Vigneault E, Springer C. Is single fraction 15 Gy the preferred high dose-rate brachytherapy boost dose for prostate cancer? Radiother Oncol. 2011;100:463–7.
Ghilezan M, Martinez A, Gustason G, Krauss D, Antonucci JV, Chen P, et al. High-dose-rate brachytherapy as monotherapy delivered in two fractions within one day for favorable/intermediate-risk prostate cancer: preliminary toxicity data. Int J Radiat Oncol Biol Phys. 2012;83(3):927–32.
Yoshioka Y, Konishi K, Sumida I, Takahashi Y, Isohashi F, Ogata T, et al. Monotherapeutic high-dose-rate brachytherapy for prostate cancer: five-year results of an extreme hypofractionation regimen with 54 Gy in nine fractions. Int J Radiat Oncol Biol Phys. 2011;80(2):469–75.
Barkati M, Williams SG, Foroudi F, Tai KH, Chander S, van Dyk S, et al. High-dose-rate brachytherapy as a monotherapy for favorable-risk prostate cancer: a Phase II trial. Int J Radiat Oncol Biol Phys. 2012;82(5):1889–96.
Hauswald H, Kamrava MR, Fallon JM, et al. High-dose-rate monotherapy for localized prostate cancer: 10 -year results. Int J Radiat Oncol Biol Phys. 2016;94(4):667–74.
Prada PJ, Jimenez I, Gonzalez-Suarez H, Fernandez J, Cuervo-Arango C, Mendez L. High-dose-rate interstitial brachytherapy as monotherapy in one fraction and transperineal hyaluronic acid injection into the perirectal fat for the treatment of favorable stage prostate cancer: treatment description and preliminary results. Brachytherapy. 2012;11(2):105–10.
Roger CL, Alders AS, Rogers RL, et al. High dose rate brachytherapy as monotherapy for intermediate risk prostate cancer. J Urol 2012;187:109–16.
Hoskin P, Rojas A, Ostler P, et al. HDR brachytherapy alone given as two or one fraction to patients for locally advanced prostate cancer: acute toxicity. RO. 2014;110:268–71.
Zamboglou N, Tselis N, Baltas D, Buhleier T, Martin T, Milickovic N, et al. High-dose-rate interstitial brachytherapy as monotherapy for clinically localized prostate cancer: treatment evolution and mature results. Int J Radiat Oncol Biol Phys. 2013;85:672–8.
Chen CP, Weinberg V, Shinohara K, et al. Salvage HDR brachytherapy for recurrent prostate cancer after previous definitive radiation therapy: 5-year outcomes. IJROBP. 2013;86:324–9.
Tharp M, Hardacre M, Bennett R, et al. Prostate high-dose-rate brachytherapy as salvage treatment of local failure after previous external or permanent seed irradiation for prostate cancer. Brachytherapy. 2008;7:231–6.
Morton GC. High-dose-rate brachytherapy boost for prostate cancer: rationale and technique. J Contemp Brachytherapy. 2014;6(3):323–30.
Spratt DE, Zumsteg ZS, Ghadjar P, et al. Comparison of high-dose (86.4Gy) IMRT vs. combined brachytherapy plus IMRT for intermediate-risk prostate cancer. BJU Int. 2014;114:360–7.
Pieters BR, de Back DZ, Koning CCE, Zwinderman AH. Comparison of three radiotherapy modalities on biochemical control and overall survival for the treatment of prostate cancer: a systematic review. Radiother Oncol. 2009;93(2):168–73.
Martinez AA, Demanes J, Vargas C, et al. High-dose-rate prostate brachytherapy: an excellent accelerated-hypofractionated treatment for favorable prostate cancer. Am J Clin Oncol. 2010;33:481–8.
Morton GC, Loblaw DA, Chung H, et al. Health-related quality of life after single-fraction high-dose-rate brachytherapy and hypofractionated external beam radiotherapy for prostate cancer. Int J Radiat Oncol Biol Phys. 2011;80:1299–305.
Challapalli A, Jones E, Harvey C, Hellawell GO, Mangar SA. High dose rate prostate brachytherapy: an overview of the rationale, experience and emerging applications in the treatment of prostate cancer. Br J Radiol. 2012;85:S18–27.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Henry, A. (2017). Permanent and High Dose Rate Brachytherapy (Technique, Indications, Results, Morbidity). In: Bolla, M., van Poppel, H. (eds) Management of Prostate Cancer. Springer, Cham. https://doi.org/10.1007/978-3-319-42769-0_13
Download citation
DOI: https://doi.org/10.1007/978-3-319-42769-0_13
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-42768-3
Online ISBN: 978-3-319-42769-0
eBook Packages: MedicineMedicine (R0)