
Abstract
Robust criteria for outcome assessment of nonsurgical endodontic treatment are essential determinants for any measure of success. Strindberg (1956) established strict criteria for clinical and radiographic evaluation of the endodontically-treated tooth at follow-up examinations. The absence of clinical symptoms, and the presence or absence of periapical radiolucency became the principal outcome measures of endodontic treatment. Subsequent studies have considered additional parameters that influence outcome such as microbiologic status prior to obturation, histopathologic data, and the effects of different techniques and materials. The “periapical index” (PAI) introduced the concept of a “continuum” that exists between success and failure where lesions could be considered as “healing.” The Toronto study introduced a novel outcome category of “functional” for teeth that were asymptomatic regardless of the PAI score. The American Association of Endodontists (AAE) has proposed that endodontically-treated teeth are considered (1) healed, (2) nonhealed, (3) healing, or (4) functional. More recently, technological advances in radiology and the application of high-resolution cone beam computed tomography (CBCT) have increased diagnostic accuracy of radiographic changes in the apical periodontium. However, the use of this technology has been limited in outcome studies. Microbiological studies indicate the importance of disinfection of the root canal system on endodontic outcome. Therefore, the absence of clinical symptoms and presence or absence of radiographic apical periodontitis, as determined by periapical radiography, remain the principal outcome measures of endodontic treatment. The aim of this chapter is to discuss the development of the criterion for outcome for nonsurgical endodontic treatment from the strict view of success and failure while adequately considering newer concepts of healing and functionality.
What’s in a name?
That which we call a rose by any other name would smell as sweet.
William Shakespeare
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others



Keywords
12.1 Introduction
With completion of endodontic treatment and placement of permanent restoration, the professional obligation to our patients does not end. One of the most exciting aspects of endodontics is actually following up the patients and evaluating how the treatment performed affected the end result, i.e., the resolution of patient symptoms, restoration of normal periradicular structures, function, and ultimately tooth retention. Outcome assessment of endodontically treated teeth has been extensively studied. The terminology used to assess outcomes is varied and may be confusing to the practicing dentist. It is the intent of this chapter to clarify some of those terms and to present outcome assessment with the needs of a primary care dentist in mind. The knowledge gained from the outcome studies should be applied to the case assessment before the commencement of endodontic treatment. This information must be part of preoperative discussion, treatment planning, and informed consent.
Methods used to evaluate the outcome of endodontic therapy include clinical observation for resolution of clinical symptoms and signs, radiographic evaluation of periapical status, and histopathologic findings of biopsy specimens. Symptoms include spontaneous pain and/or pain to percussion, palpation, or biting, following endodontic treatment. The signs include swelling or draining sinus tract after endodontic treatment [1–3].
High pretreatment root canal-associated pain prevalence drops moderately within 1 day and substantially to minimal levels by 7 days after root canal treatment [4]. The frequency of persistent all-cause pain 6 months or longer after root canal therapy of permanent teeth is approximately 5 % and may include pain from an adjacent tooth, referred pain from a nonodontogenic structure, or deafferentation pain [5]. This remaining pain may also be an indicator of persistent infection [3]. Histopathologic analysis is not possible for routine nonsurgical endodontic treatment. Therefore, radiographic evaluation of periapical status remains the primary means to assess endodontic treatment outcomes.
A landmark study on endodontic outcome assessment was published in 1956 – a classic study by Strindberg that laid the foundation for conduct of future endodontic outcome studies [6]. The study was a human clinical prospective cohort study of 344 patients, which included 539 teeth and 779 roots, all treated by a single operator. All pertinent medical, dental, and treatment data were systematically collected, recorded, and analyzed. The follow-up period was 6 years, every 6 months for the first 2 years and yearly thereafter. The retention rate of the treated patients (75 %) was remarkably high. The highlights of this study are that it:
-
1.
Established criteria for evaluation of endodontic outcome, commonly referred to as Strindberg’s criteria
-
2.
Presented success rates for orthograde (conventional) endodontic treatment (Table 12.1)
Table 12.1 Therapeutic results at 4-year and final follow-up examinations [6] -
3.
Related the outcome of endodontic treatment to the preoperative periapical diagnosis
-
4.
Defined the duration and frequency of follow-up: every 6 months for the first 2 years and yearly thereafter up to a minimum of 4 years postoperatively
Outcome studies that followed evaluated the result of endodontic treatment using Strindberg’s criteria or its modification [7–10]. Others expanded on the range of variables being investigated, such as microbiologic status prior to obturation [11–13], the effect of intracanal medicaments [14–16], sealers [17], technical aspects of endodontic treatment [8, 9, 18, 19], and the effect of restoration [20–24].
12.2 Strindberg’s Criteria
Following the publication of his landmark study, and to this day, Strindberg’s criteria continue to be widely used to evaluate the outcome of endodontic treatment. The outcome assessment is based on comparative analysis of clinical presentation and radiographic evaluation of the treated tooth at the time of treatment and follow-up examination. Determination of endodontic outcome was expressed as success, failure, or uncertain and was based on the following criteria that became known as Strindberg’s criteria:
-
I.
Success
Clinical
-
No symptoms
Radiographic
-
Contours and width of the periodontal ligament (PDL) are normal (Fig. 12.1).
Fig. 12.1 
Strindberg’s criteria for success: reestablishment of the normal apical periodontal structures. (a) Pretreatment periapical radiograph demonstrating widening of the periodontal ligament space and loss of the adjacent lamina dura around the mesial and distal roots of the mandibular first molar (white arrows). (b) Periapical radiographs made after the completion of endodontic treatment. Trabecular bone around the mesial root apex is slightly radiolucent (white arrow), and the bony contours of the lamina dura are not established around the root apex. Note reduction of radiolucency around the distal root apex. (c) Follow-up periapical radiograph taken at the 1-year recall visit. Trabecular bone around both roots is of normal density. The lamina dura around both root apices is also formed (black arrow) (Images courtesy of Dr. Charles Maupin)
-
PDL contours are widened mainly around excess root filling (Fig. 12.2).
Fig. 12.2 
Strindberg’s criteria for success: altered periodontal ligament space contours around excess endodontic material/root filling. (a) Pretreatment periapical radiograph demonstrating an irregular radiolucency that encompasses almost the entire length of the distal root and the apex of the mesial root (white arrows). Note multiple mesial roots and pulp canals. (b and c) Periapical radiographs made at the completion of endodontic obturation following 4 months of dressing with calcium hydroxide. The radiographs were taken with different horizontal angulations to separate the buccal and lingual pulp canals in the two roots. Note persistence of the radiolucency around the mesial root apex, but considerable resolution with partial osseous healing around the distal root. (d) Follow-up periapical radiograph made at a recall visit, 3.5 years after completion of endodontic therapy. Trabecular bone around both roots is of normal density. The lamina dura around both root apices is also formed. Minimal widening of the periodontal ligament space is seen adjacent to the excess endodontic filling material (black arrow) (Images courtesy of Dr. Charles Maupin)
-
Lamina dura is intact (Figs. 12.3 and 12.4).
Fig. 12.3 
Strindberg’s criteria for success: normal lamina dura. (a) Pretreatment periapical radiograph showing disruption of lamina dura and widening of the periodontal ligament space around the mesial root apex of the mandibular second molar (white arrow) and resorption in the distal root canal. An incidental finding is the proximity of the root apices to the mandibular canal lumen (arrow heads). (b) Periapical radiographs made 1 year after completion of endodontic treatment, following 15 months and two exchanges of calcium hydroxide dressing. Note normal trabecular architecture around the mesial root apex with an intact lamina dura (black arrow). The distal root is shortened, but with normal architecture of the adjacent trabecular bone, suggestive of arrested resorption. As described in Strindberg’s original manuscript, teeth with root resorption but no periradicular pathological changes are categorized as success (Images courtesy of Dr. Nadia Chugal)
Fig. 12.4 
Strindberg’s criteria for success: normal lamina dura. (a) Pretreatment periapical radiograph showing a mandibular molar with three roots. The periodontal ligament space around all roots is discernible. (b and c) Periapical radiographs made immediately following obturation and 1 year after completion of endodontic treatment. Note that there are no interval changes in the periodontal structures (Images courtesy of Dr. Charles Maupin)
-
-
II.
Failure
Clinical
-
Symptoms present
Radiographic
-
Unchanged periradicular rarefaction (Fig. 12.5)
Fig. 12.5 
Strindberg’s criteria for failure: little or no reduction in periradicular rarefaction. (a and b) Pretreatment periapical radiograph showing a periapical radiolucency around the palatal root of the maxillary first molar (white arrow). Note the superimposition of the zygomatic process of the maxilla (black arrow) that can be avoided by changing the vertical angulation as in panel b. (c and d) Follow-up periapical radiographs after completion of endodontic treatment show persistence of the periapical radiolucency (white arrow). Nine months after completion of endodontic treatment, the tooth became symptomatic again. The AAE classification would categorize this radiographic appearance as “nonhealed” (symptomatic). (e and f) Periapical radiographs made 1 year after surgical management of the palatal root of the maxillary first molar. Note complete resolution and osseous healing around the palatal root (black arrow) (Images courtesy of Dr. Alexis Moore and Dr. David Han)
-
Decrease in periradicular rarefaction, but no resolution (Fig. 12.6)
Fig. 12.6 
Strindberg’s criteria for failure: decrease in size but no resolution of periradicular rarefaction. (a) Pretreatment periapical radiograph showing a periapical radiolucency around the mesial root of the mandibular first molar (white arrow). Note external resorption of the mesial root apex. (b through e) Sequential periapical radiographs after completion of endodontic treatment show an increase in the radiodensity of the periapical bone. However, the area of rarefaction is persistent and, in the appropriate clinical context, may be categorized as a treatment failure. The AAE classification would categorize this as “nonhealed” (if symptomatic) or “healing” (if clinically asymptomatic) (Images courtesy of Dr. Nadia Chugal)
-
Appearance of new rarefaction or an increase in the size of initial rarefaction (Fig. 12.7)
Fig. 12.7 
Strindberg’s criteria for failure: increase in the size of the initial rarefaction. (a) Pretreatment periapical radiograph showing disruption of the lamina dura and widening of the periodontal ligament space around the root apices of the mandibular first molar, particularly evident around the mesial root (white arrow). The surrounding trabecular bone is sclerotic, suggestive of a chronic inflammatory process. (b and c) Follow-up periapical radiographs three and a half years after completion of endodontic treatment show persistence and an increase in the size of the periapical radiolucency (white arrow) and, in the appropriate clinical context, (accompanied with increasing clinical symptoms of pain) is categorized as a treatment failure. (d) Periapical radiograph made after completion of endodontic surgery. Note radiolucent bony defect around the mesial root apex (black arrow). (e) Osseous healing and resolution of the periapical radiolucency (black arrow) (Images courtesy of Dr. David Han)
-
Discontinuous or poorly defined lamina dura
-
-
III.
Uncertain
Radiographic
-
Ambiguous or technically unsatisfactory radiograph which could not be interpreted with certainty (Fig. 12.8).
Fig. 12.8 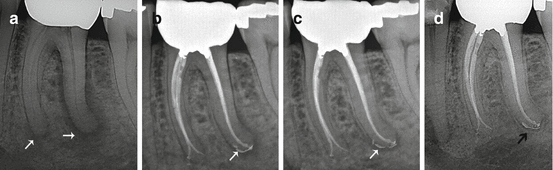
Strindberg’s criteria, uncertain outcome: periapical rarefaction less than 1 mm and with broken lamina dura. (a) Pretreatment periapical radiograph showing periradicular rarefaction around the mesial and distal roots of the mandibular first molar (white arrows). (b) Periapical radiograph made immediately after obturation, following 4 months in calcium hydroxide intracanal dressing. Note reduction in periapical radiolucency during this 4-month period. Slight excess of endodontic filling material is noted at the distal root apex (white arrow). (c) Periapical radiograph made 6 months post-obturation. The periodontal ligament space at the distal root apex is wide (white arrow), with absence of the lamina dura. As an asymptomatic tooth, this radiographic appearance would be categorized as an uncertain endodontic outcome. In contrast, the AAE classification would categorize this as “healing” (clinically asymptomatic). (d) Periapical radiograph made 18 months posttreatment. The periodontal ligament space at the distal root apex is minimally wide. Note presence of an intact lamina dura around the root (black arrow) signifying resolved periapical radiolucency and a successful radiographic outcome. The AAE classification would categorize this as “healed” and “functional” (clinically asymptomatic) (Images courtesy of Dr. Charles Maupin)
-
Periradicular rarefaction less than 1 mm and disrupted lamina dura.
-
The tooth was extracted prior to recall due to reasons not related to endodontic outcome.
-








These criteria were accepted as a standard by which endodontically treated teeth are evaluated. It soon became evident that Strindberg’s criteria were very rigid. For example, only teeth with complete absence of clinical signs and symptoms and normal radiographic presentation are classified as “success” (Figs. 12.1, 12.2 and 12.3). In contrast, an asymptomatic tooth with the appearance of broken or poorly defined lamina dura is classified as uncertain (Fig. 12.8), and clinical judgment is required for its subsequent management.
12.3 Radiographic Evaluations Have Been Inconsistent
Absence of clinical symptoms and absence of periapical radiolucency are currently the principal outcome measures that denote successful endodontic treatment. However, radiographic examination has its limitations. Radiographs provide us with a static image of the degree of mineralization in the tooth and its surrounding periodontal structures. However, for changes in bone to be radiographically apparent, there must be sufficient demineralization (or remineralization) within the lesion. A classic study examined the sensitivity of conventional radiography to detect experimental lesions in bone and showed that periapical lesions confined to the cancellous bone are not predictably detected [25]. Furthermore, radiographic evaluations tend to be subjective and influenced by observer bias [1, 26–29]. Indeed, multiple evaluators that reviewed the same radiographs differed in their scoring/interpretation, with six evaluators agreeing only 47 % of the time [26]. Importantly, radiographic assessment is also not very reproducible – when the same radiographs were evaluated 6–8 months later, the intraexaminer agreement ranged from approximately 72 % to 88 % depending on the radiographic feature being examined [27]. This variability between evaluators, and within the same evaluator, may explain the large variations in the outcome rates among clinical and radiographic studies [30]. These data underscore the need to calibrate evaluators and minimize inconsistencies in radiographic evaluation when designing studies evaluating endodontic treatment outcomes. Importantly, the inherent observer variability in radiographic analyses emphasizes the need to select those radiographic outcome measures that are robust to be used in clinical practice.
12.4 The Periapical Index (PAI) Scoring System
In clinical practice, the principal end points to assess endodontic treatment outcomes are clinical findings and the status of apical periodontal bone as assessed by periapical radiography. These radiographic assessments are based on subjective evaluation of changes in radiodensity of the periapical lesion with osseous healing and with the reestablishment of the apical periodontal structures. Currently used criteria for endodontic outcome assessment are Strindberg’s criteria and the American Association of Endodontic (AAE) classification, and both of these require radiographic assessment as one of the key end points analyzed.
For widespread application of such criteria, clinicians should be trained to reproducibly identify radiographic features of apical periodontitis. Equally important, research studies that examine endodontic treatment outcomes should use reliable and reproducible criteria to define success and failure. To address this issue, a scoring system for apical periodontitis, as depicted on conventional two-dimensional periapical radiographs was developed [31]. This scale provides clinicians and researchers with a reliable and reproducible tool to assess endodontic outcomes and to reasonably discriminate between subpopulations of success and failure.
The periapical index is a structured scoring system for categorization of radiographic features of apical periodontitis. It is based on a visual scale of periapical periodontitis severity and was built upon a classical study of histological-radiological correlations [32]. It is a five-point ordinal scale as listed below:
-
1.
Normal periapical structures
-
2.
Small changes in bone structure with no demineralization
-
3.
Changes in bone structure with some diffuse demineralization
-
4.
Apical periodontitis with well-defined radiolucent area
-
5.
Severe apical periodontitis, with exacerbating features
The PAI therefore provides more objective criteria for radiographic evaluation of periapical status of teeth that have undergone endodontic treatment. Consequently, it has been used in a number of endodontic outcome studies for the assessment of periapical status [33–46].
Recently, cone beam computed tomography (CBCT) has found considerable applications in endodontic diagnosis and treatment planning [47]. The CBCT-PAI (CBCT periapical index) was developed to apply standardization in approaches to assess the severity of apical periodontitis by CBCT. This index is a six-point scale that includes a score (0–5) plus two variables that assess expansion and destruction of cortical bone. The CBCT-PAI scale is as listed below:
- 0::
-
Intact periapical bone structures
- 1::
-
Diameter of periapical radiolucency 0.5–1 mm
- 2::
-
Diameter of periapical radiolucency 1–2 mm
- 3::
-
Diameter of periapical radiolucency 2–4 mm
- 4::
-
Diameter of periapical radiolucency 4–8 mm
- 5::
-
Diameter of periapical radiolucency 8 mm
- E::
-
Expansion of periapical cortical bone
- D::
-
Destruction of periapical cortical bone
CBCT is more sensitive than conventional periapical radiography for detection of apical radiolucencies. Thus, it can be expected that the CBCT-PAI will likely reduce the number of false-negative diagnoses on periapical radiographs. However, a recent study demonstrated significant variation in the periodontal ligament space morphology of clinically healthy teeth [48]. This underscores the need to better evaluate and clearly define normal and abnormal features on CBCT imaging, before considering systematic application of this new technology to outcome assessment.
12.5 Outcome Definitions Have Been Inconsistent
Over the years, the terms “success” and “failure” came under close scrutiny due to discrepancies in clinical, histologic, and radiographic observations [2]. New modifiers and criteria were added such as “stringent” and “lenient” where strict definition of success is characterized by “clinical and radiographic normalcy” and lenient only by “clinical normalcy” [49, 50]. Additional criteria were defined such as “strict” and “loose” [51, 52]. Strict criteria of success are defined by the absence of clinical signs and symptoms and by conventional radiographic measures of complete healing/presence of a normal periodontal ligament space. In contrast, success based on loose criteria may be defined by absence of signs and symptoms and conventional radiographic measures of complete healing or presence of a normal periodontal ligament space or incomplete healing [51, 52]. This became very confusing for the practicing dentist who had to decipher the terminology and apply it to clinical assessment of endodontic outcome.
Escalating the debate and controversy on endodontic treatment choices was the misleading comparison of endodontic treatment outcomes to the success rate of a single-tooth implant [53–55]. The term “success” was based on entirely different criteria for two treatment modalities. This comparison is also confusing to patients who have to decide whether to elect endodontic treatment or to extract the tooth and replace it with an implant.
A series of papers now known as the Toronto study [37, 39, 40, 43–45] introduced yet another set of terms that were deemed more appropriate to assess endodontic outcomes and differed from the commonly used outcome categorization of “success.” The Toronto study assessment of outcome was based on the periapical index (PAI) and categorized outcomes as “healed” when the PAI score is less than 3 or “disease” for PAI scores greater than or equal to 3. Importantly, the group introduced a novel category “functional” for all teeth that were asymptomatic, regardless of PAI score. Subsequently, it was proposed that that endodontic treatment outcome should be expressed in terms of the healing of disease, and these new terms were proposed: healed, healing, disease, and functional retention [55].
12.6 The American Association of Endodontists Outcome Criteria
Typical radiographic features of periradicular inflammation that are evident on periapical radiographs include disruption of the lamina dura, widening of the periodontal ligament space, periapical radiolucency, and root resorption. With successful endodontic treatment, the periradicular inflammatory changes resolve and the osseous and periodontal structures regenerate around the tooth apex. For these changes to be radiographically apparent, there must be adequate remineralization of the bone. This emphasizes the need to consider the radiographic changes in the context of the tooth’s functional status and clinical symptoms. Recognizing this, the AAE and AAE Foundation (AAEF) took the lead to review the existing criteria used in endodontics and compared these to the outcome measures used by other specialties. The organization subsequently defined new terms for outcome assessment using valid measures that are appropriate for endodontics. The rationale for new definitions was that terms such as “success” and “failure” are too vague. As an alternative to the widely used Strindberg’s criteria, the new definitions were approved by the Foundation’s Board of Trustees in 2004 and by the AAE Board of Directors in 2005 [56].
12.7 The AAE-Approved Definitions of Endodontic Outcomes
-
I.
Healed – Functional*, asymptomatic teeth with no or minimal radiographic periradicular pathosis (Figs. 12.1c, 12.3b, 12.4c, 12.5e–f, 12.7e, 12.8d)
-
II.
Nonhealed – Nonfunctional, symptomatic teeth with or without radiographic periradicular pathosis (Figs. 12.2b–c, 12.5c–d, 12.6b–e, 12.7b–c)
-
III.
Healing – Teeth with periradicular pathosis, which are asymptomatic and functional, or teeth with or without radiographic periradicular pathosis, which are symptomatic but whose intended function is not altered (Fig. 12.8c)
-
IV.
FUNCTIONAL* – A treated tooth or root that is serving its intended purpose in the dentition
12.8 Cone Beam Computed Tomography-Based Outcome Assessment
Over the last few years, newer imaging modalities such as cone beam computed tomography (CBCT) have been used increasingly in endodontic diagnosis and treatment planning, with intent to incorporate this technology to better assess treatment decisions and outcomes [57, 58]. The AAE and the American Academy of Oral and Maxillofacial Radiology (AAOMR) jointly developed guidelines for the appropriate use of CBCT imaging in endodontics. These guidelines define clinical scenarios and two-dimensional radiographic appearances that are likely to benefit from CBCT imaging. Notably, CBCT is more sensitive than periapical radiography to detect bone lesions, and thus, its use to evaluate outcomes will undoubtedly be beneficial to identify cases that would be false negatives on periapical radiography. Despite its higher accuracy for detecting periapical disease, the AAE-AAOMR guidelines recommend against using CBCT as a routine diagnostic and outcome assessment tool [59].
The role of CBCT imaging in endodontics is best illustrated by a case presented in Chap. 3, (Fig. 3.8). This case highlights the value of CBCT as a powerful diagnostic tool that alters diagnosis and treatment plans. Note that the decision to proceed with CBCT was made only after clinical examination and two-dimensional radiography. Additional information provided by the CBCT examination was critical in elucidating the cause of endodontic failure by identifying an untreated infected canal. It is important for clinicians to recognize that CBCT imaging does not replace conventional imaging for documentation of case completion and outcome assessment. Whereas CBCT is of value in potentially identifying causes of endodontic treatment failure, the use of CBCT imaging only to monitor treatment outcome for asymptomatic teeth is unjustified (Fig. 12.9).

Monitoring outcomes by radiography. The maxillary second molar was retreated (see details in Chap. 3, Fig. 3.8). (a, b, and c) Periapical radiographs taken at different horizontal angulations to evaluate endodontically treated symptomatic maxillary left second molar. Note the presence of a radiolucency around the mesiobuccal root apex. This represents a treatment failure according to Strindberg’s criteria and nonhealing according to the AAE classification. (d, e, and f) Axial, coronal, and sagittal CBCT sections, respectively, through the maxillary second molar. Note the presence of an untreated second mesiobuccal canal (red arrow) that is not evident on the periapical radiographs. The extent of the lytic changes (yellow arrows) is better visualized on the CBCT sections, compared with the periapical radiographs. (g, h, and i) Periapical radiographs made at completion of endodontic re-treatment and 6-month and 30-month recall visits, respectively. The tooth continued to be clinically asymptomatic. The progressive resolution of apical periodontitis is consistent with a successful outcome (Strindberg’s criteria) and/or healed classification of outcome (AAE). Note that in the absence of symptoms, conventional imaging is adequate to document this successful outcome. Additional imaging with CBCT at these follow-up stages is unnecessary and unjustified (Images courtesy of Dr. Nadia Chugal and Dr. Sotirios Tetradis)
12.9 Outcome Rates for Orthograde Endodontic Treatment
The results of Strindberg’s seminal study on outcomes of endodontic treatment at the end of the 4-year follow-up are presented in Table 12.1. These data demonstrate that success rates for endodontic treatment are significantly lower for necrotic teeth with apical periodontitis than for the teeth with a normal periapex (p < 0.05). The rates for aggregate analysis and stratification on preoperative periapical diagnosis demonstrate the intimate relationship between endodontic diagnosis and outcome of treatment. Therefore, the presence of a preoperative periapical radiolucency, denoting apical periodontitis, represents a powerful prognostic indicator [6]. This finding has been repeatedly demonstrated in a number of outcome studies that followed [8–10, 37, 52, 60, 61].
An outcome study utilized microbiologic sampling prior to obturation and stratified analysis of treatment outcome based on bacteriologic findings [11]. The 4-year outcome was assessed according to Strindberg’s criteria. The results showed that teeth with positive bacteriologic culture prior to obturation, denoting residual infection, had significantly lower rate of success compared with teeth that had negative culture results (Table 12.2).
Long-term healing (8–10 years after endodontic treatment) demonstrated 96 % success rate for roots with vital pulps and 98 % success rate for necrotic teeth without preoperative periapical radiolucency [9]. However, only 86 % of roots with pulp necrosis and periapical lesion healed after root canal treatment. Thus, the prognosis for roots without a preoperative periapical radiolucency is significantly more favorable than for those presenting with periapical rarefaction (p < 0.0001). Another study investigated the role of infection on the prognosis of endodontic treatment 5 years postoperatively using Strindberg’s criteria [13]. All teeth were diagnosed with pulp necrosis and apical periodontitis and microbiologic analysis was performed prior to obturation. This study also had an impressive 5-year retention rate of 96 %. The results showed complete healing in 94 % of teeth that exhibited preobturation negative culture and 68 % if the preobturation culture was positive (p < 0.05), (Table 12.3). The Toronto study arrived at the outcome rates based on PAI score. Teeth without preoperative apical periodontitis (PAI score < 3) showed healed rate of 92 %, whereas those with preoperative apical periodontitis (PAI ≥ 3) had a healed rate of 74 % [37].
A systematic review of clinical studies pertaining to success and failure of nonsurgical endodontic treatment reported an overall radiographic success rate of 81.5 % over a period of 5 years [61]. Another systematic review on the outcome of primary endodontic treatment concluded that the success rates have not changed over the last four or five decades [51]. The wide range of reported success rates in individual studies was attributed to the criteria used. When strict criteria are applied to the analysis of outcome, the average success rates ranged between 31 % and 96.2 % with a pooled success rate of 74.7 %. In contrast, when loose criteria were applied to the analysis, success ranged from 60 % to 100 %, with pooled success rate of 85.2 %. These results show that success rates were on the average about 10 % lower when strict criteria were used [51]. Similar rates were obtained in a prospective study where the success rate of endodontic treatment was 83 % when strict criteria were used in the assessment of outcome [52].
It is evident that varied results in outcome studies may be due to many factors, including definition of success, conditions under which radiographs were taken, calibration of evaluators, criteria used, patient pool, case selection, and length of follow-up. However, common to all these studies is a significantly lower success rate for infected teeth with preoperative apical periodontitis. This emphasizes again the strong axis between diagnosis and prognosis. As discussed in Chap. 3, this places responsibility on the treating dentist to be an astute diagnostician and intervene earlier in the disease process in order to optimize treatment outcome.
Conclusion
The criteria to assess outcomes of nonsurgical endodontic treatment were initially proposed by Strindberg as “success,” “failure,” and “uncertain,” based on specific clinical and radiographic presentations. These criteria were widely adopted, and the presence or absence of clinical signs and symptoms and the persistence or resolution of the periapical radiolucency became the principal outcome measures of endodontic treatment. However, Strindberg’s criteria for radiographic categorization of outcome are stringent and standardization among observers is challenging, and thus, its application to clinical practice was limited. Accordingly, a more reproducible index, PAI, was introduced to guide clinicians to evaluate the healing of periapical lesions after root canal treatment, as depicted on conventional periapical radiographs. Interpretation of the PAI index allows for clinical decisions on transitional phases in the healing/failing process.
More recently, in categorizing the endodontic treatment outcome, the concept of a “functional tooth” was introduced. Similarly, “tooth survival” has been adopted and parallels a common outcome measure in the dental implant literature. An important distinction is that while retention of a functional asymptomatic tooth with a persistent radiographically evident periapical lesion can be regarded an important patient-centered outcome, it is also an indicator of the unsuccessful elimination of the infection as shown in histological studies. Functional and survival clinical outcomes do not imply a successful histopathological outcome. In contrast, successful histopathological outcome implies functional or survival outcome. Clinicians must clearly understand this difference, especially when interpreting the outcome literature, and be able to explain these concepts to their patients. Nevertheless, the presence or absence of clinical signs and symptoms and the persistence or resolution of the radiographic periapical lesion still remain the principal outcome measures of endodontic treatment.
References
Bender IB, Seltzer S, Soltanoff W. Endodontic success – a reappraisal of criteria. Part 1. Oral Surg Oral Med Oral Pathol. 1966;22:780–9.
Bender IB, Seltzer S, Soltanoff W. Endodontic success-a reappraisal of criteria. Part II. Oral Surg Oral Med Oral Pathol. 1966;22:790–802.
Lin LM, Pascon E, Skirbner J, Gaengler P, Langeland K. Clinical, radiographic, and histologic study of endodontic treatment failures. Oral Surg Oral Med Oral Pathol. 1991;71:603–11.
Pak JG, White SN. Pain prevalence and severity before, during, and after root canal treatment: a systematic review. J Endod. 2011;37:429–38.
Nixdorf DR, Moana-Filho EJ, Law AS, McGuire LA, Hodges JS, John MT. Frequency of persistent tooth pain after root canal therapy: a systematic review and meta-analysis. J Endod. 2010;36:224–30.
Strindberg LZ. The dependence of the results of pulp therapy on certain factors. Acta Odontol Scand. 1956;14:1–175.
Grahnén H, Hansson L. The prognosis of pulp and root canal therapy. A clinical and radiographic follow-up examination. Odontol Revy. 1961;12:146–65.
Kerekes K, Tronstad L. Long-term results of endodontic treatment performed with a standardized technique. J Endod. 1979;5:83–90.
Sjögren U, Hågglund B, Sundqvist G, Wing K. Factors affecting the long-term results of endodontic treatment. J Endod. 1990;16:498–504.
Chugal NM, Clive JM, Spångberg LSW. A prognostic model for assessment of the outcome of endodontic treatment: effect of biologic and diagnostic variables. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;91:342–52.
Engström B, Segerstad LHA, Ramström G, Frostell G. Correlation of positive cultures with the prognosis for root canal treatment. Odontol Revy. 1964;15:257–70.
Engström B, Lundberg M. The correlation between positive culture and the prognosis of root canal therapy after pulpectomy. Odontol Revy. 1965;16:194–203.
Sjögren U, Figdor D, Persson S, Sundqvist G. Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. Int Endod J. 1997;30:297–306.
Bystrom A, Claesson R, Sundqvist G. The antibacterial effect of camphorated paramonochlorophenol, camphorated phenol and calcium hydroxide in the treatment of infected root canals. Endod Dent Traumatol. 1985;1:170–5.
Byström A, Happonen R-P, Sjögren U, Sundqvist G. Healing of periapical lesions of pulpless teeth after endodontic treatment with controlled asepsis. Endod Dent Traumatol. 1987;3:58–63.
Weiger R, Rosendahl R, Lost C. Influence of calcium hydroxide intracanal dressings on the prognosis of teeth with endodontically induced periapical lesions. Int Endod J. 2000;33:219–26.
Friedman S, Löst C, Zarrabian M, Trope M. Evaluation of success and failure after endodontic therapy using a glass ionomer cement sealer. J Endod. 1995;21:384–90.
Kerekes K. Radiographic assessment of an endodontic treatment method. J Endod. 1978;4:210–3.
Chugal N, Clive JM, Spångberg LSW. Endodontic infection: some biologic and treatment factors associated with outcome. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96:81–90.
Safavi KE, Dowden WE, Langeland K. Influence of delayed coronal permanent restoration on endodontic prognosis. Endod Dent Traumatol. 1987;3:187–91.
Kirkevang LL, Ørstavik D, Hörsted-Bindslev P, Wenzel A. Periapical status and quality of root fillings and coronal restorations in a Danish population. Int Endod J. 2000;33:509–15.
Ricucci D, Gröndahl K, Bergenholtz G. Periapical status of root-filled teeth exposed to the oral environment by loss of restoration or caries. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;90:354–9.
Tronstad L, Asbjørnsen K, Døving L, Pedersen I, Eriksen HM. Influence of coronal restorations on the periapical health of endodontically treated teeth. Endod Dent Traumatol. 2000;16:218–21.
Chugal N, Clive JM, Spångberg LSW. Endodontic treatment outcome: effect of the permanent restoration. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104:576–82.
Bender IB, Seltzer S. Roentgenographic and direct observation of experimental lesions in bone: part I. J Am Dent Assoc. 1961;62:152–60.
Goldman M, Pearson AH, Darzenta N. Endodontic success – who’s reading the radiograph? Oral Surg. 1972;33:432–7.
Goldman M, Pearson AH, Darzenta N. Reliability of radiographic interpretations. Oral Surg. 1974;38:287–93.
Gelfand M, Sunderman EJ, Goldman M. Reliability of radiographical interpretations. J Endod. 1983;9:71–5.
Zakariasen KL, Scott DA, Jensen JR. Endodontic recall radiographs: how reliable is our interpretation of endodontic success or failure and what factors affect our reliability? Oral Surg Oral Med Oral Pathol. 1984;7:343–47.
Reit C, Grondahl H. Application of statistical decision theory to radiographic diagnosis of endodontically treated teeth. Scand J Dent Res. 1983;91:213–8.
Ørstavik D, Kerekes K, Eriksen HM. The periapical index: a scoring system for radiographic assessment of apical periodontitis. Endod Dent Traumatol. 1986;2:20–34.
Brynolf I. A histologic and roentgenologic study of the periapical region of human upper incisors. Odontol Revy. 1967;11(Suppl):1–176.
Ørstavik D, Kerekes K, Eriksen HM. Clinical performance of three endodontic sealers. Endod Dent Traumatol. 1987;3:178–86.
Ericksen HM, Ørstavik D, Kerekes K. Healing of apical periodontitis after endodontic treatment using three different root canal sealers. Endod Dent Traumatol. 1988;4:114–7.
Ørstavik D, Horsted-Bindslev P. A comparison of endodontic treatment results at two dental schools. Int Endod J. 1993;26:348–54.
Trope M, Delano EO, Ørstavik D. Endodontic treatment of teeth with apical periodontitis: single vs. multivisit treatment. J Endod. 1999;25:345–50.
Friedman S, Abitbol S, Lawrence HP. Treatment outcome in endodontics: the Toronto study. Phase 1: initial treatment. J Endod. 2003;29:787–93.
Huumonen S, Lenander-Lumikari M, Sigurdsson A, Ørstavik D. Healing of apical periodontitis after endodontic treatment: a comparison between a silicone-based and a zinc oxide-eugenol-based sealer. Int Endod J. 2003;36:296–301.
Farzaneh M, Abitbol S, Lawrence HP, Friedman S, the Toronto Study. Treatment outcome in endodontics-the Toronto study. Phase II: initial treatment. J Endod. 2004;30:302–9.
Farzaneh M, Abitbol S, Friedman S. Treatment outcome in endodontics: the Toronto study. Phases I and II: orthograde retreatment. J Endod. 2004;30:627–33.
Quesnell BT, Alves M, Hawkinson Jr RW, Johnson BR, Wenckus CS, BeGole EA. The effect of human immunodeficiency virus on endodontic treatment outcome. J Endod. 2005;31:633–6.
Waltimo T, Trope M, Haapasalo M, Ørstavik D. Clinical efficacy of treatment procedures in endodontic infection control and one year follow-up of periapical healing. J Endod. 2005;31:863–6.
Marquis VL, Dao T, Farzaneh M, Abitbol S, Friedman S. Treatment outcome in endodontics: the Toronto study. Phase III: initial treatment. J Endod. 2006;32:299–306.
de Chevigny C, Dao TT, Basrani BR, Marquis V, Farzaneh M, Abitbol S, Friedman S. Treatment outcome in endodontics: the Toronto study – phases 3 and 4: orthograde retreatment. J Endod. 2008;34:131–7.
de Chevigny C, Dao TT, Basrani BR, Marquis V, Farzaneh M, Abitbol S, Friedman S. Treatment outcome in endodontics: the Toronto study – phase 4: initial treatment. J Endod. 2008;34:258–63.
Kirkevang LL, Vaeth M, Wenzel A. Ten-year follow-up of root filled teeth: a radiographic study of a Danish population. Int Endod J. 2014;47:980–8.
Estrela C, Bueno MR, Azevedo BC, Azevedo JR, Pécora JD. A new periapical index based on cone beam computed tomography. J Endod. 2008;34:1325–31.
Pope O, Sathorn C, Parashos P. A comparative investigation of cone-beam computed tomography and periapical radiography in the diagnosis of a healthy periapex. J Endod. 2014;40:360–5.
Friedman S. Treatment outcome and prognosis of endodontic therapy. Essential endodontology: prevention and treatment of apical periodontitis. Oxford: Blackwell Science; 1998. p. 367–91.
Friedman S. Prognosis of initial endodontic therapy. Endod Top. 2002;2:59–88.
Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature – part 1. Effects of study characteristics on probability of success. Int Endod J. 2007;40:921–39.
Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of non-surgical root canal treatment: part 2: tooth survival. Int Endod J. 2011;44:610–25.
Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria of success. Int J Oral Maxillofac Implants. 1986;1:11–25.
Roos J, Sennerby L, Lekholm U, Jemt T, Gröndahl K, Albrektsson T. A qualitative and quantitative method for evaluating implant success: a 5-year retrospective analysis of the Brånemark implant. Int J Oral Maxillofac Implants. 1997;12:504–14.
Friedman S, Mor C. The success of endodontic therapy-healing and functionality. J Calif Dent Assoc. 2004;32:493–503.
The American Association of Endodontists Communiqué. AAE and Foundation approve definition of Endodontic Outcomes. XXIX, August/September 2005:3
Wu M-K, Shemesh H, Wesselink PR. Limitations of previously published systematic reviews evaluating the outcome of endodontic treatment. Int Endod J. 2009;42:656–66.
Patel S, Mannocci F, Shemesh H, Wu M-K, Wesselink P, Lambrecht P. Editorial. Int Endod J. 2011;44:887–8.
American Association of Endodontists and American Academy of Oral and Maxillofacial Radiology Position Statement, 2015. http://c.ymcdn.com/sites/www.aaomr.org/resource/resmgr/Docs/AAOMR-AAE_postition_paper_CB.pdf
Matsumoto T, Nagai T, Ida K, Ito M, Kawai Y, Horiba N, Sato R, Nakamura H. Factors affecting successful prognosis of root canal treatment. J Endod. 1987;13:239–42.
Torabinejad M, Kutsenko D, Machnick TK, Ismail A, Newton CW. Levels of evidence for the outcome of nonsurgical endodontic treatment. J Endod. 2005;31:637–46.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Chugal, N., Mallya, S.M., Kahler, B. (2017). Criteria for Outcome Assessment of Nonsurgical Endodontic Treatment. In: Chugal, N., Lin, L. (eds) Endodontic Prognosis. Springer, Cham. https://doi.org/10.1007/978-3-319-42412-5_12
Download citation
DOI: https://doi.org/10.1007/978-3-319-42412-5_12
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-42410-1
Online ISBN: 978-3-319-42412-5
eBook Packages: MedicineMedicine (R0)