
Abstract
The Argus® II epiretinal prosthesis was the first retinal implant to receive commercial approval in Europe and in the United States. To date, it is the most widely used prosthesis worldwide with over 100 implanted patients in several countries, including the United States, United Kingdom, France, Germany, Switzerland, Mexico and Saudi Arabia. The device is used as a treatment for patients with profound vision loss due to end-stage photoreceptor degenerative diseases.
Argus II works by electrical stimulation of the inner retina, retinal ganglion cells and/or bipolar cells that remain partially functional in these patients. The system is an epiretinal prosthesis, meaning that the microelectrode array is surgically implanted on the retinal surface nearest to the nerve fiber layer. Video signals are acquired by a glasses-mounted video camera and transformed into electrical pulses that are finally transmitted via the microelectrode array to the inner retina. The device is capable of eliciting visual perception in a reliable and controllable fashion through video processing and manipulation of stimulation parameters.
Argus II and its predecessor, Argus I, were the first devices tested in humans to pass safety and efficacy assessments. This chapter will summarize the history of device development, initial preclinical studies and results from clinical trials. It will also discuss several future advances needed to improve the device in order to provide a more informative visual perception to blind patients.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
FormalPara Key Points-
The Argus® II epiretinal prosthesis was the first retinal implant to receive commercial approval in Europe and in the United States, and, to date, it is the most widely used visual prosthesis worldwide
-
Argus II works by electrical stimulation of the inner retina, retinal ganglion cells and/or bipolar cells that remain partially functional in patients with end-stage outer retinal degeneration. Video signals are acquired by a glasses-mounted microcamera and transformed into electrical pulses that are finally transmitted via a 60-electrode microarray to the inner retina.
-
The device is capable of eliciting phosphenes in a reliable and controllable fashion through video processing and manipulation of stimulation parameters.
-
Human studies conducted so far have demonstrated the long-term safety of chronic stimulation with Argus® II and the potential benefits provided by the device as a visual aid for patients blinded by outer retinal degeneration.
Principal Idea
The Argus® II epiretinal prosthesis (Second Sight Medical Products, Inc., Sylmar, CA, USA) was the first retinal implant to receive commercial approval from the Conformité Européenne (CE Mark) in 2011 and from the United States Food and Drug Administration (FDA) in 2013. To date, it is the most widely used visual prosthesis worldwide, with over 100 implanted patients in several countries, including the United States, United Kingdom, France, Germany, Switzerland, Mexico and Saudi Arabia [1, 2].
The device is used as a treatment for patients with profound vision loss due to end-stage photoreceptor degenerative diseases [1, 2]. Although pharmacologic agents, stem cell-based and gene therapies have been proposed for the treatment of retinal degeneration, these methods are under development and, therefore, not yet commercially available and not all patients can benefit from them [3–5]. Retinal degenerative diseases, in general, start in the outer retina leaving inner retinal layers undisturbed until very late stages. In fact, post-mortem studies have shown that nearly 80 % of inner nuclear layer cells and approximately 30 % of retinal ganglion cells (RGC) are spared in patients blinded by various forms of Retinitis Pigmentosa (RP) [6, 7]. Additionally, a similar study of patients with advanced neovascular aged-related macular degeneration (AMD) also showed that 93 % of RGCs were spared [8]. Given that the inner retinal elements are relatively spared in the majority of retinal degenerations, the stimulation of inner retinal neurons has been tested and proven to be a feasible method to bypass the loss of photoreceptors and provide the perception of light [9–13].
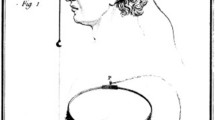
Argus® II works by direct electrical stimulation of the inner retina, RGCs and/or bipolar cells that remain partially functional in these patients. The system is an epiretinal prosthesis, meaning that the microelectrode array is surgically implanted on the retinal surface nearest to the nerve fiber layer (Fig. 5.1). Video signals are acquired by a glasses-mounted video camera and transformed into electrical pulses by a set of custom electronics that are both externally and internally implanted, linked wirelessly, and finally transmitted via the microelectrode array to the RGC and inner retina. Signals elicited from the retinal cells are sent via the optic nerve to the visual cortex, eliciting basic visual percepts called phosphenes. In summary, the device replaces the function (visual phototransduction) of degenerated photoreceptors in a rudimentary fashion, using the remaining natural visual pathway to induce visual responses [14].

Fundus photograph of an Argus® II retinal implant placed epiretinally over the macular region, within the retinal vessel arcades. Arrows indicate the microarray and the retinal tack (Reprinted with permission from Second Sight Medical Products, Inc)
The device is capable of eliciting phosphenes in a reliable and controllable fashion through video processing and manipulation of stimulating parameters. Patterns of stimulation in general reflect the surrounding visual scenes. Since the implanted patients have a restricted visual field of 20°, they tend to use a head scanning technique as a way of using the camera to survey an area of interest, identifying the position and the shape of an object. Studies have shown that subjects implanted with Argus® II system were able to perform practical tasks with better results than using their residual vision [1, 14].
Argus® II and its predecessor, Argus I, were the first devices tested in humans to pass safety and efficacy assessments. This chapter will summarize the history of device development and results from clinical trials. It will also discuss several future advances needed to improve the device in order to provide a more informative visual perception to blind patients.
Indication
Argus® II is designed for patients that present a combination of advanced outer retinal degeneration with relative inner retinal preservation. The device requires a significant number of viable RGCs to transmit electrical stimuli to the visual cortex in order to generate phosphene perception [1].
RP is the most common hereditary retinal dystrophy that shows the above characteristics. In fact, RP encompasses a wide range of more than 100 genetic disorders with variable molecular defects that ultimately leads to progressive visual loss due to the degeneration of rod photoreceptors. RP affects approximately 1 in 4,000 live births and more than one million patients worldwide [15]. Clinical manifestations may start at different ages, with patients presenting initial symptoms from early infancy up to adulthood. Initially, patients usually experience peripheral visual impairment in low light conditions, since rods are initially affected, and as the disease progresses the cone photoreceptor cells are also affected, and visual acuity declines. Visual loss can be profound, with 0.5 % of patients achieving no light perception while 25 % have worse than 20/200 vision in both eyes [15, 16].
In addition to RP, diseases of the retinal pigment epithelium and choroid can first affect photoreceptors and leave inner retina uncompromised. Choroideremia is an example of a choroidal vascular disease that leads to photoreceptor loss and blindness [17]. Patients with extensive geographic atrophy from dry AMD may also benefit from this technology and a clinical trial has been recently initiated to study the feasibility and potential benefits for this disease (ClinicalTrials.gov Identifier: NCT02227498).
Argus® II prosthesis is not applicable for the restoration of vision in patients who have lost their vision due to damaged RGCs and axons, which is caused by diseases such as glaucoma and optic nerve trauma. Devices that stimulate more proximal visual relay centers in thalamus (lateral geniculate body) and visual cortex may be better options for such patients.
Technical Description
The Argus® II retinal prosthesis consists of an implantable device and an external part. The latter includes a video microcamera mounted on a pair of glasses, a portable computer named the video processing unit (VPU) and a communication coil that is built into the side arm of the glasses. The coil is responsible for wireless communication through radio frequency (RF) telemetry and induction of power to the internal device. The microcamera captures video and sends it to the VPU, which digitizes the image in real time into electrical pulses, then applies image-processing filters which generate a series of commands that are transmitted via the communication coil on the glasses (Fig. 5.2) [1, 18].

Photograph of the Argus® II retinal prosthesis system showing the glasses-mounted microcamera, the external (inductive) coil and the video processing unit (VPU) (Reprinted with permission from Second Sight Medical Products, Inc.)
The implantable part consists of a second matching coil that receives power and data from the external coil and an internal circuit that converts the commands encoded in the RF signals, sets stimulator output based on these commands, and applies stimulus output (electrical pulses) to the intraocular array. The circuit is sealed in a hermetic casing that is sutured on the scleral surface and connected to the internal microelectrode array via a cable through a 5 mm sclerotomy. All electronic components are attached to an encircling band (scleral buckle) which fits inside the orbit (Fig. 5.3). The epiretinal array includes 60 circular electrodes that are 200 μm in diameter and arranged in a 6 × 10 grid. The array is positioned on the macular area with one retinal tack (Fig. 5.1) [18–20]. The array measures 5.5 mm in width and 6 mm in length and spans approximately 20° in a diagonal visual angle, each microelectrode covers an area equivalent to hundreds of photoreceptors. In order to match the field of view, the image captured by the camera is cropped and down sampled to 60 pixels [1, 18, 20–22].

Photograph of the implanted portion of Argus II prosthesis system showing the electrode microarray (6 × 10 electrodes), encircling band, electronics hermetic case and the internal (receiver) coil (Reprinted with permission from Second Sight Medical Products, Inc)
Argus® II is compatible with magnetic resonance imaging (MRI) up to 3-Tesla field strength, not including the external components (glasses and VPU) that must be removed during the scans. Implanted patients have been safely tested with MRI scans at 1.5 and 3-Tesla without any associated complications, change in implant position or subjective symptoms. The device, however, produces an image artifact of approximately 50 mm × 50 mm in size that obscures orbital structures. Specific instructions for MRI are provided with the Argus II patient manual and these should be followed carefully [23–25].
Surgical Methods
Argus® II can be implanted using common vitreoretinal surgical techniques in a procedure similar to a pars plana vitrectomy with an encircling buckle that takes approximately 2 to 3 h [1, 18, 19].
The procedure starts with a 360° limbal conjunctival peritomy, isolation of the rectus muscles, placement of the encircling band (containing the electronic package) under the muscles and fixed with episcleral sutures and a Watzke® sleeve (Labtician Ophthalmics, Inc., Oakville, Ontario, Canada). The episcleral inductive coil is placed under the lateral rectus muscle while the protective enclosure that contains the electronic circuit is positioned in the superotemporal quadrant [1, 18].
Vitrectomy is then conducted diligently with a posterior vitreous detachment, followed by a 5 mm incision created at 3.5 mm posterior to the limbus for the insertion of the microelectrode array and the cable. The scleral incision is sutured watertight and the array is placed and fixed on the macular region using a single custom retinal tack (Fig. 5.1) (Second Sight Medical Products, Inc., Sylmar, CA, USA). The extraocular portion of the cable is fixed with a scleral suture and the sclerotomies are closed at the end of the procedure. An allograft scleral patch (Tutoplast; IOP, Inc., Costa Mesa, CA, USA) or an alternative material (polytetrafluoroethylene patch or autologous aponeurosis graft) is sutured over the electronic package to reduce the risk of conjunctival irritation and erosion. Finally, tenon’s capsule and conjunctiva are sutured [18]. A prophylactic intravitreal injection of antibiotics is performed at the end of the procedure [1, 18].
Full Clinical Study
Device Development History
It was known for almost a century that electrical stimulation of the visual cortex could elicit the perception of light spots known as phosphenes. In 1956, Australian inventor and radio engineer Graham Tassicker patented a method of implanting a light-sensitive selenium photodiode under the retina to restore light sensation; but this was never translated to a viable device that could provide visual perception to blind patients [14]. Potts and Inoue showed that stimulation of the globe with a corneal electrode could elicit visual signals in patients with RP [26]. Thus, the principle of functional electrical stimulation of the visual pathways was well established by the early 1970s. Since then, different approaches for retinal stimulation have been proposed and initially tested in animal models with the objective of ultimately restoring visual function in blind patients [14, 27].
Animal studies related to the development of Argus I and Argus® II were conducted by Humayun et al. in the early 1990s. The authors first performed electrical stimulation experiments on dissected bullfrogs’ retinas, followed by rabbits with normal retinas and those with outer retinal function abolished by intravenous injection of sodium iodate [28]. These studies demonstrated that platinum electrodes were able to induce electrical evoked potentials through focal retinal electrical stimulation, which elicited phosphenes that were confined to the area of stimulation [28].
A few years later, initial experiments were conducted in humans to study the feasibility of epiretinal stimulation. A group of 5 blind volunteers with bare or no light perception were acutely implanted and tested under local anesthesia. A handheld probe with 2 or more electrodes of different sizes and shapes, was introduced via pars plana to the vitreous cavity and electrical pulses were applied to the macular region. All 5 blind volunteers perceived phosphenes consistent with the application of electrical pulses. They described visual responses of different characteristics, such as shape, size and brightness. One subject was able to distinguish phosphenes with 1.75° center-to-center distance, achieving a theoretical visual acuity of 4/200. They also showed a probable retinotopic localization of retinal responses, an important concept that would then lead to simultaneous stimulation of multiple retinal points to form geometric patterns and pixelated vision [9, 10, 29].
A study with multi-electrode arrays was then conducted with 2 blind patients possessing advanced RP, using electrodes in a 3 × 3 and a 5 × 5 spatial arrangement. Different patterns of stimulation were tested and the subjects were able to perceive corresponding shapes, such as a “box with an empty center”, letter shapes (“H” and “U”), and vertical and horizontal lines when a column or a row of electrodes were activated. These findings corroborated the concept that a multi-electrode array and simultaneous stimulation could be used to elicit forms and visual function in blind patients [10].
Argus I
Argus I epiretinal prosthesis – developed by Second Sight Medical Products, Inc. – was the first epiretinal device to be chronically tested in a clinical trial between 2002 and 2006 (ClinicalTrials.gov Identifier NCT00279500). Safety and efficacy were studied in six blind patients with end-stage RP. The device consisted of 16 electrodes arranged in a 4 × 4 square array with alternating diameters of either 250 or 500 μm, used to evaluate how electrode size affected visual percepts [12, 30].
The Argus I electronics were based on cochlear implant technology, as such the protective enclosure for the device was placed subcutaneously in the temporal bone recess. A cable from the enclosure was tunneled along the temporal bone to reach the periorbital space via a lateral canthotomy. The retinal stimulating array was at the end of the cable. Because of this design, the surgical procedure was similar to the approach used with the cochlear implant and required the assistance of an otolaryngology/maxillofacial expert to dissect the temporal region, which resulted in a longer surgical time. The external coil would be held magnetically over the temporal bone, connecting to the internal coil. Argus® II’s design, however, was modified so that the hermetic casing was implanted inside the orbit, simplifying the procedure and reducing surgical time [12].
At the end of the initial 33-month follow-up, no major adverse event was reported, thus supporting the long-term safety of the device. Additionally, electrode thresholds were evaluated within and across patients, showing that many electrodes were able to elicit phosphenes using charge densities within the safety limit [31]. Although there was variability across patients when performing visually-guided tasks (e.g. target localization, object recognition and direction of movement), the majority of tests presented better performance with the device turned ON than OFF, showing encouraging results. Subjects were able to locate and count high contrast objects, distinguish the orientation of the letter “L” on a computer screen, and identify objects such as a plate, a cup and a knife with results better than chance. One patient even managed to indicate the orientation of a high contrast square wave gratings, distinguishing directions (horizontal, vertical, diagonals right and left) better with the device enabled than disabled [12].
The study demonstrated the safety of long-term stimulation and supported the crucial concept that blind subjects were able to use an epiretinal prosthesis combined with patterned electrical stimulation to perform better in visually-guided tasks. Recently, an Argus I subject was evaluated 10 years after implantation and still had measurable perceptual thresholds. These encouraging results motivated the development of the more advanced Argus® II retinal implant [30].
Argus® II
A phase II clinical trial began in 2006 to study the safety and utility of the Argus® II System in providing visual function to blind subjects with severe to profound outer retinal degeneration. Thirty subjects were enrolled in a multicenter, single-arm, prospective and unmasked study (Clinicaltrials.gov, Identifier number NCT00407602) that was sponsored by Second Sight Medical Products, Inc., and conducted at 5 centers in the United States as well as in Mexico, France, United Kingdom, Switzerland and France. Inclusion and exclusion criteria for this study are listed in Table 5.1. Argus® II was implanted monocularly, typically in the eye with the worst vision [1].
Patients
Surgeries were performed from 2007 to 2009 in 30 patients, of which 29 were diagnosed with RP, including one with Leber Congenital Amaurosis, and one with Choroideremia. Vision acuity was bare light perception in both eyes in 29 subjects, while one had no light perception in both eyes. At the time of surgery, patient’s age ranged from 28 to 77 years (mean 57.5 ± 9.9 years); 21 being males and nine being females. All patients completed a follow-up of 3 years and each visit included complete eye examination, intraocular pressure measurement, fundus photography, fluorescein angiography and optical coherence tomography. Safety and visual function were the primary endpoints of this study, while the secondary endpoints included stability, functionality and reliability of the device, orientation and mobility tests, activities of daily living and quality of life [1].
Adverse Events
Device- or surgery-related adverse events were classified, whether or not they required medical/surgical intervention or hospitalization to prevent permanent injury, which was defined as a serious adverse event (SAE). After 3 years of implantation, the device showed an acceptable safety profile, with 11 patients (37 %) experiencing a total of 23 SAEs. Most of the SAEs (61 %) occurred within the first 6 months after surgery and only 5 SAEs (22 %) after month 12. Events were clustered within patients, with three patients (10 %) accounted for over 55 % of SAEs after 3 years of implantation. Two patients underwent an acute revision surgery (within 1 week after implantation) to re-tack the microarray to the retinal surface, and one patient’s device was removed at 1.2 years due to recurrent conjunctival erosions, choroidal efusions associated with hypotony and retinal detachment that demanded multiple repairs. The most common SAEs were hypotony, conjunctival dehiscence or erosion and presumed endophthalmitis (culture negative) and apart from the explanted patient, all cases were treatable with standard ophthalmic approaches without loss of eyes (enucleation). There were three cases of sterile endophthalmitis reported in the first group of 15 surgeries that were treated and resolved with intravitreous injections of antibiotics combined with topical and systemic antibiotics [1].
A protocol adjustment was made halfway through the trial to add a prophylactic injection of intravitreal antibiotics after the surgery. After this change, no other case of endophthalmitis was reported. Modifications on the surgical technique and on the design of the device were also implemented, leading to a significant reduction of SAEs [1]. A few years later, another study by Rizzo et al. evaluated the safety outcome of six patients implanted by the same surgeon and reported no case of SAE, corroborating the importance of the refinement of surgical technique and the influence of learning curve [2]. In this study, although one patient presented high intraocular pressure postoperatively and another patient suffered from choroidal detachment, both cases were successfully managed with topical medication [2].
Functional Ouctomes
Visual Function
Considering that standard visual acuity tests, such as Snellen acuity/logMAR or contrast sensitivity could not be assessed, in general, due to the insufficient visual level provided by the prosthesis, visual function was measured by computer-based tests especially developed for low vision. Patients were objectively evaluated for basic visual skills, including target localization, motion detection, navigation, form discrimination and recognition. Since it was a single group study of a rare condition, each patient served as his/her own control, and status and performance of the implanted eye prior to surgery (residual vision) was used as a comparator [1].
In the target localization test called “square localization”, patients were asked to locate and touch a white square that appeared randomly on a black touchscreen monitor. The distance between the center of the square and the patient’s response was measured in centimeters, recorded and averaged after 40 trials. Another test called “direction of motion” assessed the patient’s ability to draw the path of a white line that moved across a black touchscreen monitor. The difference between the patient’s response and the angle of the white line was measured in degrees and averaged over 80 trials [1].
Visual acuity was evaluated using black and white gratings of various widths that were displayed randomly for 5 s on a computer screen in four orientations: horizontal, vertical, diagonal right and diagonal left. Each width corresponded to a visual acuity, on a scale that ranged from 2.9 to 1.6 logMAR (20/15887–20/756 Snellen notation, respectively). This was a 4-alternative forced-choice test, meaning that patients had to provide one of the four above alternatives, even if they could not determine the orientation of the gratings. In general, performance of these tasks increased when the device was turned ON. The results (in percent correct) for specific tasks were as follows: Square Localization (89.3 %, n = 28), Direction of Motion (55.6 %, n = 27) and Grating Visual Acuity (33.3 %, n = 27), with mean visual acuity of 2.5 logMAR [1].
Orientation and Mobilitity Tests
The orientation and mobility tests were aimed to evaluate patients’ performance in more real-world conditions, which included two indoor experiments. First, a simulated door (2.1 high × 1 m wide) made of a black cloth on a white wall was placed across a room and the patient was asked to locate and walk toward it. The “Door Task” was repeated 12 times (six times with the system ON and OFF) and the black cloth was either positioned 3 m to the right or to the left from the center of the wall. At year 3, the overall success of 28 patients in this test using the device was 54.2 ± 6.2 % versus 19.0 ± 4.3 % when the system was turned OFF. In the second test called “Line Task”, a white line (15 cm wide × 6 m long) configured three different paths on a black floor made of rubber interlocking tiles. Patients were asked to walk over the path that could be a straight line or have a 90° turn to the right or to the left. The mean percentage of success of 28 patients was 67.9 ± 6.5 % with the system ON versus 14.3 ± 3.8 % with the system OFF [1].
Activities of Daily Living
Patients were also evaluated using the system in their daily lives after they had been trained to operate the device, approximately 1 month after implantation. A visual rehabilitation expert conducted interviews with patients and assessed their ability to carry out tasks of daily living such as orientation and mobility around their homes and social interactions. The impact of the system on the patients’ quality of life was rated positive, mild positive, prior positive (positive effects in the past that were not present at the time of evaluation), neutral and negative. The overall effect of the device was rated positive or mild positive in 12 out of 15 subjects at year 1 (80 %) and prior positive or neutral in three subjects. At year 3, 65.2 % rated as positive and mild positive and 34.8 % as prior positive and neutral, from a total of 23 subjects [1].
In addition to the clinical trial, an increasing number of investigator sponsored studies are being reported, which provide further information on the capabilities and limitations of the Argus II. A group of 11 European subjects participated in an experiment of shapes recognition. They were asked to identify eight high contrast shapes (square, circle, triangle, rectangle, pentagon, hexagon, cross of half circle) presented in white or gray against a black background on a monitor. Each shape was shown in five different sizes (XL = 22.6, L = 14.3, M = 9, S = 5.6, XS = 3.6 cm) and was either outlined or solid. The mean percentage of success using the device ON was 32.8 ± 15.7 % versus 12.5 ± 6.7 % with the system OFF (p = 0.02) and chance rate of 12.5 %. When outlined shapes were presented, the percentage of success recognition was higher: 41.4 ± 17.7 % (system ON) versus 9.4 ± 7.5 % (system OFF). The study indicated better results when outlined shapes were used, suggesting a possible influence of total illumination on the subjetcs’ performance [32].
Another study with 21 Argus® II patients investigated their ability to read high contrast letters (41.27° in height) presented on a flat LCD screen. Three groups of letters with increasing level of typographical complexity were tested: group A with the simplest form of vertical and horizontal lines (E, F, H, I, J, L T, U); group B with oblique components at the full height of the letter and minor variation on the circle (A, C, D, M, N, O, Q, V, W, Z); and group C, with oblique or curved components at half of the height of the letter (B, G, K, P, R, S, X, Y). Patients were able to correctly identify each letter group with the following mean percentage of success using the system ON versus OFF: group A, 72.3 ± 24.6 % versus 17.7 ± 12.9 %; group B, 55.0 ± 27.4 % versus 11.8 ± 10.7 %; and group C, 51.7 ± 28.9 % versus 15.3 ± 7.4 % (p < 0.001 for all groups). A subgroup of 6 patients who performed well in this first experiment, identifying at least 50 % of the letters of group A under 60 s, also participated in the identification of 2-, 3- and 4-letter words with the device ON and OFF. Four of these patients were able to recognize 7 out of 10 words (mean = 6.8 words) with the device ON and 0 out of 10 (mean = 0.3 words) when the device was turned OFF [33].
Additionally, Luo et al. conducted an experiment with a subset of seven patients in the United Kingdom to investigate recognition of 8 daily life objects that were presented in high contrast, i.e., white or metallic objects against a black background in ambient room light. Patients were allowed 30 s per trial to give a forced-choice answer, and each object was presented twice in random order. Results once again showed a higher percentage of success when patients were using the device, with a mean correct percentage of recognition of 35.7 ± 14.6 % (system enabled) versus 12.5 ± 7.2 % (system disabled), and chance rate of 12.5 % [34, 35].
Human studies conducted so far have demonstrated the long-term safety of chronic stimulation with Argus® II and the potential benefits provided by the device as a visual aid for patients blinded by outer retina degeneration [1, 2, 32–35]. However, further studies are still required to better understand the underlying factors related to pattern electrical stimulation and neural interpretation at the cortical level, which may lead to device enhancements and better visual outcomes.
Future Directions
Software development and image/signal processing represent one of the most promising paths for improvement of Argus® II’s performance. The use of different algorithms to interpret video signals and modulate patterned stimulation has proven to enhance visual perception without making any changes to the existing hardware. One example of this concept is the use of maximized contrast on the edges of images to enhance object recognition and improve orientation and mobility. This adjustment was shown to be beneficial in initial patient tests and later was incorporated as an optional feature in the device [36].
Another image processing software, proposed by Sahel et al. uses magnification and minimization of the acquired image to enable a visual acuity beyond the limit set by theoretical resolution of the implanted array. Although the field of view covered by the array is about 20° diagonally, in this experiment the image was reduced or magnified in a range from 0.4× to 16× using a remote hand-held controller. One Argus® II patient was able to achieve an equivalent visual acuity of 20/200 when using 16× magnification on the gratings visual acuity test, exceeding by far the best nominal acuity achieved with the device, i.e. 20/1260. The same patient managed to read letters of 2.3 cm in height from a notebook at 30 cm, using a magnification of 4× [37].
In another experiment, Stanga et al. applied a facial recognition algorithm that resulted in a visual percept only when a human face was detected by the processor. The facial region would be extracted from the rest of the visual scene and presented by itself in a zoomed-out view. This feature enabled 5 Argus® II patients to locate faces 100 % of the time at 2–3 m distance in a significantly shorter time when using the wider field of view [38].
Apart from software development, hardware improvements have also been proposed for the next generation of epiretinal prosthesis in order to provide a more genuine visual perception. To date, the number of electrodes and the reduced visual field impose limitations to visual acuity and image resolution. An increase in the area of stimulated retina with a larger number of electrodes could potentially enhance visual function. Other approaches involve adding peripheral electrodes to the main array and adjusting the prosthesis curvature to the patient’s retina, considering that electrode-retina distance has been demonstrated to be a critical factor related to perceptual threshold [21].
References
Ho AC, Humayun MS, Dorn JD, da Cruz L, Dagnelie G, Handa J, et al. Long-term results from an epiretinal prosthesis to restore sight to the blind. Ophthalmology. 2015;122(8):1547–54.
Rizzo S, Belting C, Cinelli L, Allegrini L, Genovesi-Ebert F, Barca F, et al. The Argus II Retinal Prosthesis: 12-month outcomes from a single-study center. Am J Ophthalmol. 2014;157(6):1282–90.
Nazari H, Zhang L, Zhu D, Chader GJ, Falabella P, Stefanini F, et al. Stem cell based therapies for age-related macular degeneration: the promises and the challenges. Prog Retin Eye Res. 2015;48:1–39.
Bainbridge JW, Mehat MS, Sundaram V, Robbie SJ, Barker SE, Ripamonti C, et al. Long-term effect of gene therapy on Leber’s congenital amaurosis. N Engl J Med. 2015;372(20):1887–97.
Sahni JN, Angi M, Irigoyen C, Semeraro F, Romano MR, Parmeggiani F. Therapeutic challenges to retinitis pigmentosa: from neuroprotection to gene therapy. Curr Genomics. 2011;12(4):276–84.
Santos A, Humayun MS, de Juan E, Jr Greenburg RJ, Marsh MJ, Klock IB. Preservation of the inner retina in retinitis pigmentosa. A morphometric analysis. Arch Ophthalmol. 1997;115(4):511–5.
Stone JL, Barlow WE, Humayun MS, de Juan E, Jr Milam AH. Morphometric analysis of macular photoreceptors and ganglion cells in retinas with retinitis pigmentosa. Arch Ophthalmol. 1992;110(11):1634–9.
Kim SY, Sadda S, Pearlman J, Humayun MS, de Juan E, Jr Melia BM, et al. Morphometric analysis of the macula in eyes with disciform age-related macular degeneration. Retina. 2002;22(4):471–7.
Humayun MS, de Juan E, Jr Dagnelie G, Greenberg RJ, Propst RH, Phillips DH. Visual perception elicited by electrical stimulation of retina in blind humans. Arch Ophthalmol. 1996;114(1):40–6.
Humayun MS, de Juan E, Jr Weiland JD, Dagnelie G, Katona S, Greenberg R, et al. Pattern electrical stimulation of the human retina. Vision Res. 1999;39(15):2569–76.
Rizzo 3rd JF, Wyatt J, Loewenstein J, Kelly S, Shire D. Methods and perceptual thresholds for short-term electrical stimulation of human retina with microelectrode arrays. Invest Ophthalmol Vis Sci. 2003;44(12):5355–61.
Humayun MS, Weiland JD, Fujii GY, Greenberg R, Williamson R, Little J, et al. Visual perception in a blind subject with a chronic microelectronic retinal prosthesis. Vision Res. 2003;43(24):2573–81.
Yanai D, Weiland JD, Mahadevappa M, Greenberg RJ, Fine I, Humayun MS. Visual performance using a retinal prosthesis in three subjects with retinitis pigmentosa. Am J Ophthalmol. 2007;143(5):820–7.
Luo YH, da Cruz L. The Argus II retinal prosthesis system. Prog Retin Eye Res. 2016;50:89–107.
Hartong DT, Berson EL, Dryja TP. Retinitis pigmentosa. Lancet. 2006;368(9549):1795–809.
Grover S, Fishman GA, Anderson RJ, Tozatti MS, Heckenlively JR, Weleber RG, et al. Visual acuity impairment in patients with retinitis pigmentosa at age 45 years or older. Ophthalmology. 1999;106(9):1780–5.
Coussa RG, Traboulsi EI. Choroideremia: a review of general findings and pathogenesis. Ophthalmic Genet. 2012;33(2):57–65.
Humayun MS, Dorn JD, da Cruz L, Dagnelie G, Sahel JA, Stanga PE, et al. Interim results from the international trial of Second Sight’s visual prosthesis. Ophthalmology. 2012;119(4):779–88.
Luo YH, da Cruz L. A review and update on the current status of retinal prostheses (bionic eye). Br Med Bull. 2014;109:31–44.
Dorn JD, Ahuja AK, Caspi A, da Cruz L, Dagnelie G, Sahel JA, et al. The detection of motion by blind subjects with the epiretinal 60-electrode (Argus II) retinal prosthesis. JAMA Ophthalmol. 2013;131(2):183–9.
Ahuja AK, Yeoh J, Dorn JD, Caspi A, Wuyyuru V, McMahon MJ, et al. Factors affecting perceptual threshold in Argus II retinal prosthesis subjects. Transl Vis Sci Technol. 2013;2(4):1.
Roessler G, Laube T, Brockmann C, Kirschkamp T, Mazinani B, Goertz M, et al. Implantation and explantation of a wireless epiretinal retina implant device: observations during the EPIRET3 prospective clinical trial. Invest Ophthalmol Vis Sci. 2009;50(6):3003–8.
Cunningham S, Tjan B, Bao P, Falabella P, Weiland J. Tactile-evoked V1 responses in Argus II retinal prosthesis patients assessed with fMRI: a case study. J Vis. 2015;15(12):359.
Luo YH, Davagnanam I, dacCuz L. MRI brain scans in two patients with the argus II retinal prosthesis. Ophthalmology. 2013;120(8):1711. e8
Cunningham SI, Shi Y, Weiland JD, Falabella P, Olmos de Koo LC, Zacks DN, et al. Feasibility of structural and functional MRI acquisition with unpowered implants in Argus II retinal prosthesis patients: a case study. Transl Vis Sci Technol. 2015;4(6):6.
Potts AM, Inoue J. The electrically evoked response (EER) of the visual system. II. Effect of adaptation and retinitis pigmentosa. Invest Ophthalmol. 1969;8(6):605–12.
Brindley GS, Lewin WS. The sensations produced by electrical stimulation of the visual cortex. J Physiol. 1968;196(2):479–93.
Humayun M, Propst R, de Juan E, Jr McCormick K, Hickingbotham D. Bipolar surface electrical stimulation of the vertebrate retina. Arch Ophthalmol. 1994;112(1):110–6.
Greenberg RJ, Velte TJ, Humayun MS, Scarlatis GN, Jr de Juan E. A computational model of electrical stimulation of the retinal ganglion cell. IEEE Trans Biomed Eng. 1999;46(5):505–14.
Yue L, Falabella P, Christopher P, Wuyyuru V, Dorn J, Schor P, et al. Ten-Year follow-up of a blind patient chronically implanted with epiretinal prosthesis argus I. Ophthalmology. 2015;122(12):2545–52. e1.
Brummer SB, Turner MJ. Electrochemical considerations for safe electrical stimulation of the nervous system with platinum electrodes. IEEE Trans Biomed Eng. 1977;24(1):59–63.
Arsiero M, Cruz LD, Merlini F, Sahel JA, Stanga PE, Hafezi F, et al. Subjects blinded by outer retinal dystrophies are able to recognize shapes using the Argus II retinal prosthesis system. Invest Ophthalmol Vis Sci. 2011;52(14):4951.
da Cruz L, Coley BF, Dorn J, Merlini F, Filley E, Christopher P, et al. The Argus II epiretinal prosthesis system allows letter and word reading and long-term function in patients with profound vision loss. Br J Ophthalmol. 2013;97(5):632–6.
Luo YH, Zhong JJ, da Cruz L. The use of Argus(R) II retinal prosthesis by blind subjects to achieve localisation and prehension of objects in 3-dimensional space. Graefes Arch Clin Exp Ophthalmol. 2015;253(11):1907–14.
Luo YHL, Zhong J, Merlini F, Anaflous F, Arsiero M, Stanga PE, et al. The use of Argus® II retinal prosthesis to identify common objects in blind subjects with outer retinal dystrophies. Invest Ophthalmol Vis Sci. 2014;55(13):1834.
Humayun MS, Dorn JD, Ahuja AK, Caspi A, Filley E, Dagnelie G, et al. Preliminary 6 month results from the Argus II epiretinal prosthesis feasibility study. Conf Proc: Ann Int Conf IEEE Eng Med Biol Soc IEEE Eng Med Biol Soc Ann Conf. 2009;2009:4566–8.
Sahel J, Mohand-Said S, Stanga P, Caspi A, Greenberg R. Acuboost™: enhancing the maximum acuity of the Argus II Retinal Prosthesis System. Invest Ophthalmol Vis Sci. 2013;54(15):1389.
Stanga P, Sahel J, Mohand-Said S, da Cruz L, Caspi A, Merlini F, et al. Face detection using the Argus® II retinal prosthesis system. Invest Ophthalmol Vis Sci. 2013;54(15):1766.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Falabella, P., Nazari, H., Schor, P., Weiland, J.D., Humayun, M.S. (2017). Argus® II Retinal Prosthesis System. In: Gabel, V. (eds) Artificial Vision. Springer, Cham. https://doi.org/10.1007/978-3-319-41876-6_5
Download citation
DOI: https://doi.org/10.1007/978-3-319-41876-6_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-41874-2
Online ISBN: 978-3-319-41876-6
eBook Packages: MedicineMedicine (R0)