
Abstract
Insomnia in childhood includes difficulty initiating and maintaining sleep and bedtime resistance. These sleep problems are common in childhood and largely result from interactions between the caregivers or parents and their children. However that are other causes and origins of insomnia that can include child temperament, psychopathology, or variation in sleep need that can include decreased need for sleep and atypical circadian regulation. Chronic insomnia symptoms often precipitate a range of functional daytime impairments (e.g., academic impairment, hyperactivity, inattention, irritability, tiredness) which may further undermine subsequent parent–child interactions including the transition to sleep. Evidence-based interventions for childhood insomnia can address these sleep difficulties and family stress. However, dissemination of evidence-based interventions is limited by the dearth of clinicians trained to deliver these interventions, access to sleep disorder centers, and cost. This chapter provides an overview of approaches to diagnosis and management of childhood insomnia.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Cognitive-behavioral therapy (CBT)
- Insomnia
- Evidence-based practice
- Child
- Parent–child relations
- Sleep initiation
- Maintenance
Introduction
The insomnias of childhood include bedtime resistance, sleep initiation sleep, and maintenance problems. These bedtime and sleep problems can place a significant burden on caregivers and parents who may be required to spend significant time attending to a child at the beginning or middle of the night and sometimes early in the morning. The resulting sleep loss can impact parents’ and children’s daytime functioning and increase bedtime-related conflict and influence family dynamics [1]. Even when sleep problems do not meet criteria for a disorder, they are a common cause of stress in parent–child relationships. Childhood sleep problems can be an indicator of poor regulatory capacity in the infant or child, and there is evidence that sleep problems presenting in the first few years of life can be a marker of a diathesis for psychopathology and health problems [2–5]. Even though sleep problems in early childhood are quite common and there are well-established interventions for these problems, little is understood about the etiology pathophysiology of childhood sleep disorders. This chapter reviews common causes of insomnia from infancy through the school-age years that can persist into middle childhood and adolescence. The discussion of pathophysiology will be followed by a detailed practical approach to evaluating and treating insomnias in this age group.
Definitions
While most children have at least minor or transient problems initiating and maintaining sleep, between 15 and 20 % of children have persistent insomnia [6, 7]. The International Classification of Sleep Disorders (ICSD) Third Edition has harmonized with the DSM-5 [8] by consolidating insomnia into chronic and short-term categories, and eliminating prior subtypes. Insomnia may be diagnosed after the age of 6 months at which time the nocturnal sleep of typically developing children has become more consolidated and nighttime feedings are minimal to none. All insomnia subtypes including the behavioral insomnias of childhood (BIC) are no longer independent diagnostic categories but are discussed as descriptors that may have some clinical utility as they suggest etiology. The BIC will be the primary focus of this chapter and treated as a sub-category of insomnia as there is a large evidence-based literature demonstrating the efficacy of insomnia interventions.
The BIC are divided into three diagnostic categories: sleep-onset association type and limit-setting type and a mixed type with features of both sleep-onset association and bedtime resistance difficulties. The specific features of BIC subtypes, as defined in the second edition of the ICSD , are presented in Table 8.1. It is important to note that the criteria for the BIC do not include specific time periods for sleep-onset latency (SOL) and wake time after sleep onset (WASO). However duration criteria differentiate chronic insomnia (3 months or greater with symptoms present three or more times a week) and short-term insomnia (<3 months and may be episodic and occur <3 times a week) [9, 10]. While the primary focus of this chapter is on the BIC subtypes that occur primarily in children 6 years of age and younger, there will also be some discussion of chronic and short-term insomnia. In part because the age range of insomnia has been extended down to 6 months of age, there is a dearth of research on prevalence and treatment. The chapter also focuses on recent advances in the evaluation of cognitive behavior therapy for insomnia (CBTI) in school-age children (6–12 years).
The primary features of BIC subtypes include parent reports of bedtime resistance, involvement of the parent in wake-to-sleep transitions at the beginning and the middle of the night, and sleep/wake schedule conflicts with environmental demands. In children younger than 6 years, it is a parent who typically identifies the sleep problem and brings it to the attention of a pediatrician, mental health provider, or sleep specialist. On occasion, an educator or childcare provider will report changes in daytime functioning including academic impairment, hyperactivity, inattention, and tiredness and has an atypical need for sleep during the day. While even very young children can describe sleep problems, their sleep complaints seldom lead to a referral.
Pathophysiology of BIC
For both children and adults, and perhaps all species of animals, the transition from wake to sleep is a vulnerable period as it requires the letting down of vigilance. While most people currently live in relatively safe and secure environments and have the luxuries of strong locks, lights, and secure homes, this was not the case for most of human history. Bedtime routines and repetitive and familiar behavior sequences facilitate the letting down of vigilance and help to assure that the sleep environment is safe and free of threats. From an evolutionary perspective, these routines allay fears and worries. Across all species, routinized behavior prior to the wake-to-sleep transition is common and typically involves checking the immediate environment for threats and seeking out indicators of safety such as a being in close proximity to one’s clan or pack. Human infants and young children are dependent on their parents for the implementation of routines and maintenance of a safe environment. When individual or environmental factors interfere with routines or cause chronic psychophysiological arousal or hypervigilance at bedtime, wake-to-sleep transitions can be negatively affected.
The origins of BIC and insomnia are often heterogeneous. In some cases it is important to understand the cause as it can maintain the sleep problem. In other cases, the causes are remote and less relevant to intervention. These initial causes, which may occur alone but often co-occur and can sometimes be compounding, can be divided into several categories. The most common cause is parental reinforcement of a child’s attention-seeking behavior, or dependence on the parent’s involvement in wake-to-sleep transitions. Included in this category are feeding problems and poor sleep hygiene. Children who have medical problems (e.g., gastroesophageal reflux or colic) may have an increased risk of developing sleep problems. A sentinel event such as a separation from parents, the birth of a sibling, or an accident can precipitate a subsequent sleep disturbance that then persists. Children with a diathesis for psychopathology, temperamental hyperarousal, or hyperactivity often have increased anxiety and hypervigilance at bedtime. Conflict between environmental demands (e.g., child care or parent work schedules) and the child’s intrinsic circadian phase may result in delayed sleep onset and insufficient sleep during the day. Finally, sleep disorders such as obstructive sleep apnea syndrome and restless leg syndrome can cause insomnia. Further explanation of these categories is warranted as their contributions to the sleep problems may inform the treatment approach.
Parental Reinforcement
Parental reinforcement refers to routines established at wake-to-sleep transitions that involve a child’s bid for attention and a response from the parents that increases the likelihood that the child will repeat their behavior. Over the course of development the wake-to-sleep transition is the first significant period of separation for the child–parent dyad and can lead to heightened arousal and ambivalence on the part of the parent and child. Therefore, an assessment of the child and parent attachment and interactions is critical to understanding the nature of sleep disturbances in young children. Parents’ contributions to the child’s problematic sleep-to-wake transitions and bedtime resistance may occur for a variety of reasons. For example, parents may simply prefer to be present when the child is falling asleep or may learn that their presence results in a faster and easier transition to sleep. When the bedtime routines and the wake-to-sleep transition involve parental presence (e.g., feeding the child, rocking the child, bed sharing, or parental presence in the child’s bedroom), the child may become dependent on this very powerful indicator of safety and security. When the child protests being left alone and the parent repeatedly returns to the child’s room, the parent’s repeated visits reward the child for calling out and reinforce the child’s dependence on the parent. The parent is in turn reinforced by the child’s rapid calming and relatively rapid return to sleep. Ambivalence may be amplified if the child has a history of medical problems and/or if parents who work long hours or more than one job and have limited time with their child due to conflicts in their work schedule.
It is a widely accepted assumption that by teaching the child to transition to sleep independently at the beginning of the night, the child generalizes this learning to middle of the night awakenings. If the parent attempts to leave the room when the child is awake, or is not present for any or all of the multiple awakenings that occur during a normal night of sleep, the child may have difficulty returning to sleep if the child has not learned to initiate sleep independently.
Parental reinforcement is the most important root cause of behavioral insomnias of childhood and perhaps an initiating cause of insomnia that then follows an independent course and persists from childhood into adolescence. Parents may quickly modify routines and their children will generally adapt quite quickly. When chronic and more severe bedtime and nighttime conflict between the parent and child is present, these interactions can become part of the learned bedtime ritual and may carry over to parent–child interactions during the day. Over time, the child may become labeled by a caregiver or self-identify as a “poor” or “bad sleeper.” One of the goals of treatment is to break this cycle of conflict and to replace impressions that the child is inherently a poor sleeper with the knowledge that the child can learn to be a “good sleeper.”
Feeding Behavior
An infant and young child’s feeding patterns can contribute to irregular sleep/wake patterns. It is common for a mother to nurse or feed her infant during the wake-to-sleep transition. This association between feeding and sleep onset is quite powerful as it involves both physical closeness and sustenance. In older infants the association between feeding and sleep onset can become problematic when the infant becomes dependent on parental presence. If the infant cannot re-initiate sleep independently when natural awakenings occur throughout the night, sleep is then disrupted for the parent and 24-h feeding patterns become irregular for the infant, causing further problems in biological cycling for both. After 6 months of age most typically developing infants do not need to feed at the beginning or middle of the sleep period. Modifying the feeding pattern prior to a sleep intervention is an important first—and in some cases the only necessary—step in establishing an independent wake-to-sleep transition.
Medical Problems
Various medical problems can contribute to a child’s sleep problems and can shape parents’ patterns of response that can in turn complicate the wake-to-sleep transition. Medical problems associated with pain and physical discomfort, as well as medications and procedures, can result in a child developing negative associations with the crib or bed. Parents’ responses to their child’s illnesses can be quite complex. Parental worry that arises from ongoing illness or that is conditioned based on a prior illness can result in some parents having ambivalent feelings about separating from their child at bedtime. Parental guilt , a common and normal response to a child’s illness, can also result in parents having ambivalent or conflicting feelings about separating from their child at bedtime. For example, a child who has gastroesophageal reflux or colic, and consequently has long bouts of screaming and crying at bedtime that cannot be soothed, can cause both the parents and child to develop a negative association with bedtime. While the well-established behavioral treatments for BIC are effective for children with medical illnesses, it is usually optimal to aggressively treat the underlying illness before implementing a behavioral sleep intervention and to help parents understand their child’s and their own negative associations and aversions.
Sentinel Events
A sentinel event in the child’s or family’s life may cause insomnia symptoms and lead to chronic insomnia. The event may cause increased vigilance and worry or a short-term change in routine could lead to dependence on parental presence, and short- or long-term sleep problems at the wake-to-sleep transition. A short-term positive adaptation in a family that has suffered a trauma might involve the parents taking the child into their own bed during the acute response phase. Once the trauma becomes more remote and the parents attempt to shift the child back to his or her bed, the separation at bedtime may reignite fear in the child, parental guilt, and/or parental ambivalence about co-sleeping or being present when the child transitions to sleep. In these cases, treatment may focus on fears that are related to a past event, parental ambivalence, and a behavioral intervention involving a gradual approach to establishing an independent wake-to-sleep transition. If the trauma is severe, or is associated with sleep or bedtime (e.g., sexual abuse or a home fire), a referral to a pediatric mental health specialist for assessment and treatment of post-traumatic stress disorders would be warranted.
Psychopathology and Temperament
There are now well-established links between child sleep disturbances and anxiety disorders [11] as well as the later emergence of mental health problems [12]. There are also significantly increased rates of sleep problems among children with developmental disorders (e.g., autism) [13–15], attention-deficit hyperactivity disorder (ADHD) [6, 16], and other psychiatric disorders [17]. Therefore, a psychiatric history and assessment of mental status are of particular importance. If a comorbid sleep and psychiatric disorder is suspected, a referral for treatment is in order. However, there is some evidence that an intervention for the child’s sleep problems may improve the psychiatric symptoms [18].
The wake-to-sleep transition is one of the first significant separations that a child experiences in his or her development. The ability of the child to self-sooth in order to regulate his or her internal states during these separations may be mediated by the attachment between child and parent. Attachment, as conceptualized by Bowlby [19], is a biologically based bond between the child and parent that ensures safety and survival of the child and over the course of development has components of both physiological and psychological bonds [20]. Attachment patterns develop through a series of separations and reunions with the child and parent and, over time, lead to a stable and predictable relationship that the child internalizes. This internal model of the parent facilitates increasing self-regulatory capacity and independence over time. During infancy the sleep/wake cycle involves multiple separations and reunions. Thus, the wake-to-sleep transitions represent a critically important phenomenon in the emerging patterns of parent–child interactions [21]. A transactional model of sleep/wake development proposed by Anders [22] illustrates how intrinsic (e.g., biomedical factors, infant temperament) and external contexts (e.g., cultural and social norms, family stress, parental psychopathology, SES) interact bidirectionally. When problems arise in the attachment relationship, they may appear first as BIC symptoms of the child but in some instances may also be understood as a function of problems of the child–parent dyad. For example, over-identification with the child and/or guilt over neglect and abandonment may trigger parental separation anxiety, which subsequently becomes generalized by the child as bedtime resistance from and/or difficulty initiating sleep onset. Therefore the child–parent dyad plays an essential role for establishing and maintaining healthy sleep behaviors early in life, and assessment of the child–parent relationship is essential for understating the complex transactions that occur within the context of a family system.
Some children with stable personality characteristics involving avoidance, hyper-arousal, and hyper-reactivity to environmental stimuli may have increased rates of sleep problems [22]. These children may be overly attentive to cues in their environment that threaten their sense of safety and may have difficulty letting down vigilance. Attachment disorders may also increase the risk for sleep problems in children [23]. For example, children who have been adopted from other countries and have been raised in nurseries may be overly attached to parents or may be unable to accept nurturance and calming offered by parents. Criteria for diagnosing these types of problems can be found in the Zero to Three Diagnostic Manual [24]. In addition, there is some evidence that suggests that children adopted from overseas may experience increased rates of sleep problems [25].
There are also some established links between postpartum depression and mother-infant sleep problems . Specifically, maternal depression may be worsened by inadequate sleep which is common during the infant’s first 6 months of life, and maternal depression may result in irritability, withdrawal, and/or impairment in mother–child bonding [26, 27]. Treatment of postpartum depression and behavioral–educational interventions designed to promote maternal and infant sleep resulted in increased maternal nighttime sleep time and longer infant nighttime sleep periods with fewer infant nighttime awakenings [28].
Co-sleeping can also be linked to marital and family relational problems. In a marriage in which there is conflict, sexual, or emotional abuse, or avoidance of sexual relations, a child in the parental bed or a parent co-sleeping in a child’s bed may facilitate avoidance or serve as a buffer against further conflict. These parental psychiatric problems and marital problems can contribute significantly to the maintenance of a child’s sleep problems, and referral to an adult psychiatrist or a family therapist may be a necessary adjunctive approach.
Environmental and Circadian Factors
There are a variety of environmental demands that may have a negative impact on the child’s sleep period. Based on preference, and economic or career demands, some parents enforce a sleep schedule on the infant. For example, parents who have to return to work soon after the birth of their child and initiate childcare when the child is 6 weeks of age may be required to wake their child early or put them to bed late. There is currently no consensus on the impact of sleep training or scheduling. Some infants may take easily to an enforced day and nighttime sleep schedule as a result of their being adaptable and having flexibility in mechanisms regulating their circadian phase. Other infants may have difficulty adapting. If the scheduled sleep periods are in direct conflict with the infant’s homeostatic and circadian drive, then sleep problems may immerge; either the infant has difficulty falling asleep at the required time or extended periods of wakefulness lead to poor regulatory capacity and the infant has difficulty settling. While there is no scientific evidence that children who are overtired and who have had insufficient sleep have more difficulty settling and do not sleep as well, this is accepted in clinical practice as a relatively robust phenomena [29–31].
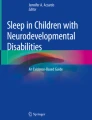
The timing of sleep and nap periods can be difficult to navigate as there are vast individual differences in children’s sleep needs: the timing of their day and nighttime periods of highest sleep propensity, their intrinsic flexibility to tolerate sleeping at different time periods, and their ability to tolerate varying durations of wakefulness between sleep periods during the day. There is a good deal of variability in published normative trends regarding the timing and sleep needs in infants and children (refer to Table 8.2) and no validated or clinically feasible approaches for their evaluation. Actigraphy and sleep logs (see Fig. 8.1) provide the best approximation of key variables (i.e., number and duration of sleep periods, sleep-onset latency, wake time after sleep onset), but interpretation of these data and the development of a treatment plan require consideration of circadian and homeostatic factors as well as assessment of a child’s behavior regulation during the day, and environmental demands.

Two-week visual sleep log
Sleep Disorders
Several sleep disorders can cause symptoms of insomnia and should be evaluated as part of the assessment. These sleep disorders which cause or are associated with inadequate sleep may account for increased irritability and poor regulatory capacity that can delay sleep onset. For example, obstructive sleep apnea syndrome which has a prevalence of 1 and 4 % in children [32] has been associated with behavioral problems and poor sleep regulation [33, 34]. Restless leg syndrome (RLS) has been estimated to occur in as many as 2–6 % of children [35, 36]. RLS involves limb discomfort that tends to occur in the early evening and can delay sleep onset. In some cases parents are called upon to rub the child’s legs to relieve sensations. The child’s overactivity at bedtime may relieve RLS sensations, but parents can misinterpret their child’s activity as oppositional or hyperactive behavior which can result in parent–child conflict. Parasomnias (e.g., confusional arousals and night terrors), while not a cause of insomnia, can be confused for full awakenings. While it can be difficult to differentiate a full from a partial awakening in a very young child or a child with a developmental disability, educating the parent about partial awakenings is an important consideration in developing a treatment plan.
In summary, behavioral sleep problems in young children can present with varying levels of severity, ranging from transient problems with sleep onset to a diagnosable disorder, and their causes are usually multifactorial. While the vast majority of cases are relatively straightforward and can be evaluated and managed by general practice pediatricians or child mental health or behavioral specialists, persistent problems require a comprehensive evaluation and consideration of sleep/wake mechanisms, child-specific factors, developmental and psychiatric status, family function, and environmental demands.
Insomnia Pathophysiology
The literature on the evaluation and treatment of psychophysiological insomnia in adults and BIC is quite large and there are several excellent review articles that summarize this literature [6, 7, 37, 38]. There are a few recent articles on the pathophysiology of adolescent insomnia [39, 40]. However, there are no published reports that describe insomnia symptoms in children aged 6–12, but this is an important area of focus of future research given that pediatric insomnia is included in the most recent edition of the ICSD and in quality metrics for evaluation and treatment of insomnia recently published by the American Academy of Sleep Medicine [41].
We propose that there are three subgroups of patients between 6 and 18 years of age who meet the criteria for chronic and short-term insomnia in the ICSD (Table 8.3) [42]. The first group is composed of children who will have lifelong difficulty initiating and maintaining sleep that supersedes BIC (Table 8.2) and will eventually be diagnosed with chronic insomnia. The second group is composed of children who have temperamental problems and may meet the criteria for a psychiatric disorder and who also have chronic sleep problems that persist even when psychiatric problems remit. The third group is composed of children who have persistent symptoms of insomnia that may be attributed to an initiating cause (e.g., BIC, a medical illness, sentinel event), but their symptoms persist into childhood or adolescence and they are not responsive to established treatment for BIC.
Assessment
Most sleep problems in young children are relatively straightforward to evaluate and treat, and are often addressed by pediatricians who provide general recommendations. Other problems require a comprehensive evaluation and a nuanced interpretation of data derived from sleep logs, actigraphy, and sleep questionnaires. Assessment of sleep problems in primary pediatric practices almost exclusively relies on parental report. When children present to a pediatric sleep specialist, they have typically failed other interventions and require more extensive assessment and an individually tailored treatment plan. This thorough assessment typically takes between 60 and 90 min.
The presenting complaint generally involves a conflict at bedtime or bedtime resistance, disrupted child and parental sleep (multiple middle-of-the-night awakenings and/or early morning awakenings), daytime impairment (e.g., irritability, impaired attention), or general concern that the child’s sleep quality is poor. The first steps in the assessment are refining the presenting complaint and establishing a consensus treatment goal. The specific domains of assessment are provided in detail in Table 8.4. During the interview, observation of parent–child interactions in the examination room can also be useful in understanding the child’s developmental status, regulatory capacity (i.e., their ability to maintain attention or deal with frustration), and their parents’ attentiveness to their needs. When taking a history, some assessment of each of the categories discussed above is optimal. The remainder of the evaluation should focus on the five categories of potential causes and facilitators of sleep problems presented in the section above on pathophysiology.
Sleep logs or diaries and sleep questionnaires are well-established assessment tools that have been used in the vast majority of assessment and treatment studies. Sleep logs used over a 2-week period provide more objective data for sleep patterns and can be used to establish a baseline to evaluate clinical interventions [43]. Diaries are typically kept for 1–2 weeks and provide more detailed information that can be tailored to specific insomnia symptoms [44]. They have been shown to have relatively good reliability with actigraphy [45] and are a necessary complement to actigraphs. Optimally, a family should come to their initial assessment session with a completed 2-week sleep log that documents the timing of sleep periods: time in bed, sleep-onset latency (SOL), wake time after sleep onset (WASO), time out of bed, and schedule and unplanned naps. It is often helpful to compare sleep periods from school schedules to those obtained on weekends, holidays, or vacations. There are several questionnaires and there are two comprehensive reviews of available questionnaires [46]. Two of the most widely used sleep questionnaires, the Sleep Habits Questionnaire [47] and the Pediatric Sleep Questionnaire [48], can be used to identify potential sleep problems in children and adolescents.
Children’s Sleep Habits Questionnaire ( CSHQ ; [ 47 ]). The CSHQ is a comprehensive, parent-report measure for assessing children’s sleep with good psychometric properties for both community and sleep-disordered samples for children 4–12 years of age. It yields both a total score and eight subscale scores reflecting key sleep domains that encompass a range of medical and behavioral sleep problems including sleep-disordered breathing, sleep-related anxiety, bedtime refusal, insomnia, parasomnias, and daytime sleepiness. However, it should be noted that the CSHQ does not have established normative values for the total or subscale scores. Items are rated on a three-point scale. The CSHQ has shown adequate internal consistency in both clinical and community samples of children [47]. Two-week test-retest estimates also have been shown to be acceptable (.62 to .79). The CSQH has been primarily used for research to assess sleep at baseline and post-intervention.
The Pediatric Sleep Questionnaire (PSQ ; [ 48 ]). The PSQ is a validated 74-item questionnaire assessing children’s sleeping habits and behaviors in children 2–18 years of age. The PSQ includes a 22-item sleep-related breathing disorder subscale (PSQ-SRBD) that has been shown to predict the risk for PSG-confirmed SDB [49]. In addition, the PSQ includes a four-item Sleepiness Scales (PSQ-SS) that contains items assessing the degree to which sleepiness is a problem rather than perceived sleep propensity in different situations. The PSQ-SS had low-to -moderate validity against an objective measure of sleepiness, the Multiple Sleep Latency Test, which is comparable to what has been observed in the adult literature assessing associations between the Epworth Sleepiness Scale and Multiple Sleep Latency Test [50].
Wrist actigraphy is a cost-effective tool that has a broad array of applications in research and in clinical settings. It estimates sleep by utilizing the difference between reduced activity during a sleep period relative to waking behavior. The actigraph itself is a small battery-operated device (size of a watch) that is worn on the wrist 24 h a day (for up to 2 or more weeks) and records movement sampled several times per second with an accelerometer and stores the sampled data in epochs (typically 1 min). After downloading raw movement data, a computer program applies an algorithm to score sleep/wake periods. Actigraphy has been validated against PSG with agreement rates for minute-by-minute sleep/wake identification of higher than 90 % [51–53]. Actigraphy has been used extensively in clinical and research assessment with children, and there are no risks associated with its use. In addition, actigraphy provides the clinician with the opportunity to collect data from an individual sleeping in her natural sleep environment. Dependent variables derived from actigraphy include total sleep time (TST), sleep efficiency (SE; a ratio of minutes asleep to time in bed), and wake time after sleep onset (WASO). While SOL is also important, actigraphy does not afford reliable measures of this variable.
To aid the assessment of behavioral problems and psychiatric symptoms several of the following validated questionnaires utilizing parent or teacher report may help a clinician characterize behavioral problems and psychiatric symptoms that may be associated with BIC symptoms: (a) general behavioral problems—Child Behavior Checklist (CBCL); (b) depression—Child Depression Inventory (CDI); (c) anxiety—Screen for Child Anxiety-Related Emotional Disorders (SCARED); and (d) ADHD—(Connors). If a co-occurring sleep and psychiatric disorder is suspected, a referral for treatment is in order.
CBCL ([ 54, 55 ]). The CBCL is a 113-item parent-report scale assessing a broad range of behavioral problems and social and academic functioning. The CBCL is one of the most extensively tested rating scales available and possesses excellent psychometrics. The measure yields total, internalizing, and externalizing behavior scales, and eight subscale scores. In addition there are a youth self-report version and teacher report form that have been validated and may be considered to supplement the parental report. The measures take about 10 min to complete and 2 min to score.
SCARED ([ 56, 57 ]). The SCARED is a 42-item measure of childhood anxiety that includes a child and parent form. Birmaher et al. [57] found that the SCARED was able to differentiate between clinically anxious and non-anxious psychiatrically ill youth. Test-retest reliability coefficients and internal consistency coefficients of the subscales were found to be acceptable.
CDI ([ 58 ]). The CDI is the most widely used self-report measure of depressive symptoms in children and is used extensively in pediatric sleep and affective research. The CDI consists of 27 items and yields five factors plus a total score normed according to age and gender. Published reports on the reliability and validity of the CDI are extensive with internal consistency coefficients ranging from .71 to .89 and the test-retest coefficients range from .74 to .83 (time interval 2–3 weeks).
The Connors Rating Scale-Revised (CRS- R ; [ 59 ]). The CRS-R is an 80-item observer (parent or teacher) or self-report questionnaire used to assess attention-deficit/hyperactivity disorder (ADHD) and evaluate problem behavior in children and adolescents. Short versions of the CRS scales are also available. The CRS-R is comprised of seven factors: cognitive problems, oppositional, hyperactivity-impulsivity, anxious-shy, perfectionism, social problems, and psychosomatic. The CRS-R factors have high internal reliability (alphas = .75–.94) but poor-to-adequate 6-week test-retest reliability (rs = .13—parents and .78).
Treatment
There are several interventions that have established efficacy as treatments of the BIC [7, 37, 60, 61], but only a few studies evaluating the efficacy of cognitive behavior therapy for insomnia in school-age children and adolescents (CBT-I) [62, 63]. The interventions for BIC involve simple and graduated extinction techniques, sleep scheduling, positive routines, sleep hygiene training, and parent education. The number of sessions and the order in which these interventions are implemented have not been adequately studied, and the demands of the specific case generally dictate priorities. Based on discussions with pediatric sleep specialists, the most common course of treatment involves a thorough in-person assessment and initial treatment recommendations, and then in-person, telephone, or e-mail follow-up.
Treatment for BIC
Initial recommendations should focus on the treatment of medical problems and feeding schedules. Symptoms of untreated gastroesophageal reflux, and recurrent ear infections and other ailments involving pain and discomfort, can undermine usually efficacious interventions. Special attention may need to be given to parents of children who have had medical problems as they may be, with good reason, hypersensitive to their child’s condition. Children with illnesses involving pain may have developed an aversion to their crib or bed. When this is suspected, and when possible, a change in the bedroom or the type of bed may break this association. Other behavioral techniques such as systematic desensitization or graduated exposure may be most effective.
Ferber [31] recommends addressing feeding schedules prior to implementing a sleep intervention. Common feeding schedules and issues that interfere with an infant’s independent wake-to-sleep transitions can include nursing or bottle feeding the infant. The association between feeding and direct contact with the parents is exceedingly powerful. Middle-of-the-night feedings are equally problematic. While a middle-of-the-night feeding usually results in the infant returning to sleep very rapidly and is rewarding for the overtired parent, it reinforces the child’s dependence on the parent and may disrupt daytime feeding schedules. Specifically, after 6 months of age normally developing infants do not need to feed at night. The one caveat is that an infant whose sole nutrition is mother’s milk may have difficulty going a whole night without a feeding. In this case the introduction of cereal for infants prior to bedtime can help to sustain the infant throughout the night.
A thorough evaluation establishes the priorities for interventions and specifically the identification of behaviors that are targets for change. An understanding of the behavioral cues that precede it (antecedents) and the responses or consequences that follow the behavior must be understood as critical components of the behavioral plan to eliminate the problematic behavior. Other considerations, which have been discussed in detail above, involve child-, parent-, and environment-specific factors, and the history and course of the sleep problem.
Extinction
Extinction techniques involve removal of reinforcers that maintain or cue an undesirable behavior. Simple or unmodified extinction involves the immediate removal of reinforcers [64, 65]. For example, parents ignore the child’s bids for attention at bedtime and the middle of the night and over the course of 3–5 days the child learns that crying, call outs, and sometimes more extreme behavior (e.g., throwing toys or other objects and vomiting) do not elicit the desired response from the parent. The child no longer depends on the parents to be present at bedtime because he develops new associations or self-soothing skills, and the attempt to gain the parents’ attention ceases. This approach breaks the chain of interactions between parent and child, and the sleep-onset association (i.e., parental presence) is transferred to an object or a self-soothing behavior that decreases or eliminates the child’s dependence on the parent. Simple extinction has also been called the “cry-it-out” or cold turkey method. This is generally very effective, although not all parents feel comfortable implementing this plan. The child’s crying and call outs can be quite persistent, and it is not uncommon for a child to vomit in their crib as a result of long episodes of crying and upset. If a child vomits during the course of an intervention plan, parents are instructed to clean up immediately, and to provide their child with support but to minimize strong emotional responses (e.g., anger, frustration, physical comforting) that could be reinforcing. Parents who fail to implement simple extinction techniques often inadvertently reinforce longer crying spells and poorer self-regulation.
Graduated extinction (GE) techniques are far easier for parents to tolerate because they involve less crying and more flexibility for parents to regulate the pace of the intervention. The trade-off is that GE can take longer to implement. There are some manualized approaches [65], but most interventions are tailored to the specific needs and preferences of the parent and child. The general principle of a GE intervention is that reinforcement is gradually withdrawn on a set schedule. The variables that are modified over time can include physical contact with the child (e.g., breast feeding, holding, patting), verbal responses, proximity to the child, and frequency and duration of check-ins. Any combination of these variables can be gradually modified. For example, if the parent typically lies in bed with the child until the child falls asleep, the recommendation could involve three nights of sitting next to the child’s bed and holding his or her hand until he falls asleep; followed by three nights of sitting further away from the child and using verbalizations to calm the child; followed by three nights sitting in the room and refusing interactions; followed by three nights of check-ins every 5 min as long as the child stays in bed; followed by three nights of check-ins every 10 min.
There are several types of modifications that can be included in a GE intervention. Fading refers to a gradual decrease in the intensity or quality of parental reinforcement of the child’s behavior. Shaping refers to the parents’ reinforcement of qualitative changes in the child’s behavior. For example, if the child cries for extended periods of time, the parent might only enter the room when there is a pause in the child’s crying, thereby reinforcing calming behavior. Chaining refers to the parent gradually modifying the child’s behavioral response. For example, the parents may tell the child that they will check in with the child as long as the child does not cry, and then the parents may tell the child that they will check in as long as the child does not call out. Thinning refers to a gradual decrease in the frequency of parental reinforcement of child-calming behavior.
Positive Routines
Positive routines involve modification of parent–child interactions and behaviors at bedtime to decrease stress and conflict and to establish a relaxed environment that is conducive to a smooth transition to sleep. Positive routines also establish new wake-to-sleep associations. This may be coupled with a shift in the time to bed so that the child has an increased sleep propensity but is not overtired and hyperaroused. In adjusting time to bed, it is also important to consider that there is a naturally occurring increase in arousal level also called the “danger zone .” When a regular sequence of activities is established, the child knows what to expect and the sequence should involve increasing calm and relaxing behaviors like reading, close time with parents, and quiet singing. Parental warmth and calm, and positive and supportive statements, reinforce the child’s participation in the quiet activities, set the tone, model appropriate behavior, and reinforce and facilitate learning. Once the child learns the routine and transitions to sleep more quickly, the parents can gradually advance the bedtime with the goal of increasing the child’s total sleep time. After about 6 months of age, the introduction of a transitional object (a blanket, a plush toy) can become an important part of the bedtime routine and can take the place of the parent or other sleep-onset associations that are problematic. The choice of an object is important because it will sometimes be with the family for years. It should be washable and made of a non-toxic material and parents may want to purchase a duplicate in the event that the object is lost.
Schedule Modification
Schedule modification is sometimes necessary when the child’s bedtime is exceedingly early or late or when the timing of naps interferes with bedtime. Schedule problems can arise when a child’s optimal sleep time (controlled by their circadian phase) conflicts with parental or other environmental demands. Some young infants have very rigid early morning awakenings that chronically disrupt parents’ sleep. While small shifts in the sleep phase can sometimes be achieved, parents may need help in adjusting their schedule or agreeing on an alternating care plan for their child. Helping parents identify the optimal nap times based on the child’s age and daytime sleep needs can be complicated. A late-afternoon nap for some children over the age of 3 can erode their ability to fall asleep at night while others need a nap. Eliminating a morning nap between 18 and 24 months of age can extend the duration and improve the quality of the afternoon nap.
Sleep Hygiene Training
Sleep hygiene training involves changes in behaviors, sleep-related activities, or the environment that precede sleep and that interfere with sleep or the process of decreasing arousal. Sleep hygiene education is a common component of behavioral interventions used to address adult sleep problems such as insomnia and is routinely included in behavioral interventions targeted in pediatric populations [66–68]. Sleep hygiene education begins with an assessment of daytime and bedtime routines that delay sleep onset (e.g., exercise, use of electronic media, pets in the bedroom) and degrade sleep quality (e.g., caffeine use, environmental factors like light, noise, and temperature). The clinician works with parents and their child to establish guidelines that are feasible and within reference to developmental norms. During the hour leading up to the child’s scheduled bedtime parent and children are instructed to engage in calm and relaxing activities that the child enjoys (e.g., reading). This may require some negotiation between child and parent and activities that have the potential to cause conflict and should be avoided. The timing of bedtime routine activities should be consistent and predictable and the scheduled bedtimes should not deviate significantly (e.g., 30–60 min) from day to day. The bed should only be used for sleeping; therefore, activities other than sleep (e.g., play) should be avoided to strengthen the association between the bed and sleep. Some flexibility can be exercised with calm and focused activities such as reading. It is best practice to keep all electronic devices out of bed and the bedroom. A later bedtime may be warranted especially if a child appears alert and functions well with slightly less sleep. To the extent possible light (e.g., use of a nightlight) and noise should be reduced to promote an optimal sleep environment.
Other Treatment Considerations
Another intervention that can be useful with older children involves the use of a bedtime pass [69, 70]. The child is provided with a token or piece of paper that allows them one opportunity to engage the parent after bedtime. This technique provides the child with more control and helps them to weigh their actual need to see the parent. If passes are not used on successive nights then the child can turn them in for a reward. As part of the intervention, parents should also be informed that following the initial implementation of the intervention, an extinction burst commonly occurs [71]. This phenomenon that occurs in many behavioral interventions involves a temporary return to the undesired behavior. If parents are unaware of the phenomena they may assume that the intervention has failed. They are generally instructed to persist in the treatment plan.
In the interest of managing expectations when discussing interventions for BIC it is important that some caregivers may feel concerned about inducing distress in their child during a critical time in a family transition for infants and their caregivers. These are natural concerns that should be met with empathy and validation. Such concerns provide a clinician with the opportunity that to date there exists no empirical evidence from longitudinal studies indicating long-standing negative behavioral, emotional, psychosocial, or hormonal effects associated with the behavioral strategies to address BIC [72].
CBT-I for School-Age Children
The approach to the assessment of insomnia in school-age children does not differ significantly from that of younger children; however, involving a verbal child in the assessment and treatment plan is likely useful in assuring their understanding and willingness to participate. Cognitive behavioral treatments for insomnia are described elsewhere in this book but a brief overview of the core components of CBT-I with some modifications is provided. CBT-I is a comprehensive, non-pharmacologic, and evidence-based intervention for insomnia that has been developed for adults with well-established short-term and long-term efficacy [73, 74]. CBT-I has been modified to be developmentally appropriate for adolescents [75, 76] and school-age children [63] and includes components intended to promote greater control over sleep, reduce emotional distress, and enhance sleep efficiency.
Following assessment, CBT-I begins with psychoeducation, to provide parents and children with information about the role of sleep, its regulation, and consequences of insufficient sleep framed within a developmentally appropriate context (e.g., school-aged children required 10–11 h of sleep). For some parents it may be helpful to draw on the two-process model of sleep regulation (i.e., homeostatic sleep pressure and circadian rhythm) to provide a framework for sleep regulation [77]. In addition Spielman’s 3P model of insomnia may also be a useful heurist for framing interventions intended to identify and resolve factors perpetuating insomnia [78]. As described above sleep hygiene practices can be included with psychoeducation and used to supplement CBT-I interventions as needed.
The core behavioral components of CBT-I consist of stimulus control therapy and sleep restriction which are well-evaluated interventions used in adults that meet established treatment standards as defined by the American Psychological Association [79] and American Academy of Sleep Medicine [80]. Stimulus control therapy [81] utilizes standardized instructions intended to associate the bed/sleep environment with sleep rather than sleep-incompatible behaviors (e.g., boredom, frustration, or worry at not being able to sleep) and to re-establish a consistent sleep/wake schedule. Sleep restriction therapy aims to increase sleep drive and consolidate sleep by limiting a patient’s time in bed to the total sleep time derived from 1 to 2 weeks of sleep diary [82]. Time in bed is subsequently titrated up or down based on response to intervention and minimum time in bed is generally never less than 7.5 h for school-age children and is applied flexibly based on acceptance and adherence to treatment. Prohibits naps at times other than the assigned time in bed.
Although stimulus control and sleep restriction therapy may be adequate behavioral interventions to address insomnia some older school-age children may also benefit from the inclusion of cognitive strategies aimed at reducing cognitive arousal associated with anxious thoughts or identifying and challenging dysfunctional attitudes and beliefs and misconceptions about sleep that contribute to emotional distress and further sleep problems.
The CBT-I interventions described above may be augmented with relaxation training to introduce strategies aimed at reducing somatic tension or intrusive thoughts at bedtime interfering with sleep. Common techniques include diaphragmatic breathing and progressive muscle relaxation.
Conclusion
Behavioral sleep problems during childhood represent a complex group of problems ranging from short-term delays in sleep onset and parental reinforcement of problematic behavior to chronic problems with sleep initiation and maintenance. Thorough assessment is required to define the causes and clinical course of the problems, especially when they are chronic and disrupt the family and/or the child’s daytime behavior. There is currently no research on the developmental pathophysiology of behavioral sleep problems in childhood, particularly those that are chronic and persist into later childhood and early adolescence. There is a relatively large literature and several good reviews of behavioral treatment strategies for BIC occurring in infants and children under the age of 7. In most cases, parents can implement these interventions independently or with the assistance of a pediatrician or pediatric nurse. However, persistent problems require the expertise of a sleep specialist.
References
Sadeh A, Tikotzky L, Scher A. Parenting and infant sleep. Sleep Med Rev. 2010;14(2):89–96. Epub 2009/07/28.
Wong MM, Nigg JT, Zucker RA, Puttler LI, Fitzgerald HE, Jester JM, et al. Behavioral control and resiliency in the onset of alcohol and illicit drug use: a prospective study from preschool to adolescence. Child Dev. 2006;77(4):1016–33.
Gregory AM, Caspi A, Eley TC, Moffitt TE, Oconnor TG, Poulton R. Prospective longitudinal associations between persistent sleep problems in childhood and anxiety and depression disorders in adulthood. J Abnorm Child Psychol. 2005;33(2):157–63.
Chorney DB, Detweiler MF, Morris TL, Kuhn BR. The interplay of sleep disturbance, anxiety, and depression in children. J Pediatr Psychol. 2008;33(4):339–48. Epub 2007/11/10.
Touchette E, Petit D, Tremblay RE, Boivin M, Falissard B, Genolini C, et al. Associations between sleep duration patterns and overweight/obesity at age 6. Sleep. 2008;31(11):1507–14. Epub 2008/11/19.
Mindell JA, Kuhn B, Lewin DS, Meltzer LJ, Sadeh A, American Academy of Sleep Medicine. Behavioral treatment of bedtime problems and night wakings in infants and young children. Sleep. 2006;29(10):1263–76 [erratum appears in Sleep. 2006 Nov 1;29(11):1380].
Kuhn BR, Elliott AJ. Treatment efficacy in behavioral pediatric sleep medicine. J Psychosom Res. 2003;54:587–97.
American Psychiatric Association. Cautionary statement for forensic use of DSM-5. Diagnostic and statistical manual of mental disorders. 5th ed. Arlington, VA: American Psychiatric Publishing; 2013.
AASM. The international classification of sleep disorders: diagnostic & coding manual, ICSD-2. 2nd ed. Westchester, IL: American Academy of Sleep Medicine; 2005.
American Academy of Sleep Medicine Work Group. International classification of sleep disorders. 3rd ed. Westchester, IL: American Academy of Sleep Medicine; 2014.
Alfano CA, Ginsburg GS, Kingery JN. Sleep-related problems among children and adolescents with anxiety disorders. J Am Acad Child Adolesc Psychiatry. 2007;46(2):224–32.
Gregory AM, Rijsdijk FV, Dahl RE, McGuffin P, Eley TC. Associations between sleep problems, anxiety, and depression in twins at 8 years of age. Pediatrics. 2006;118(3):1124–32.
Dorris L, Scott N, Zuberi S, Gibson N, Espie C. Sleep problems in children with neurological disorders. Dev Neurorehabil. 2008;11(2):95–114.
Liu X, Hubbard JA, Fabes RA, Adam JB. Sleep disturbances and correlates of children with autism spectrum disorders. Child Psychiatry Hum Dev. 2006;37(2):179–91.
Malow BA, Marzec ML, McGrew SG, Wang L, Henderson LM, Stone WL. Characterizing sleep in children with autism spectrum disorders: a multidimensional approach. Sleep. 2006;29(12):1563–71.
Mindell JA, Emslie G, Blumer J, Genel M, Glaze D, Ivanenko A, et al. Pharmacologic management of insomnia in children and adolescents: consensus statement. Pediatrics. 2006;117(6):e1223–32.
Ivanenko A, Johnson K. Sleep disturbances in children with psychiatric disorders. Semin Pediatr Neurol. 2008;15(2):70–8.
Insomnia therapy may help improve depression treatment. Using cognitive behavioral therapy in insomnia therapy (CBT-I) also may help make depression treatment more effective. Duke Med Health News. 2014;20(2):5. Epub 2014/03/22.
Bowlby J. A secure base: parent–child attachment and healthy human development. New York: Basic Books; 1988. p. xii. 205 pp.
Gabbard GO. Psychodynamic psychiatry in clinical practice. 4th ed. Washington, DC: American Psychiatric Pub; 2005. p. xiv. 629 pp.
Anders TF. Infant sleep, nighttime relationships, and attachment. Psychiatry. 1994;57(1):11–21.
Anders TF, Halpern LF, Hua J. Sleeping through the night: a developmental perspective. Pediatrics. 1992;90(4):554–60.
Poehlmann J. Representations of attachment relationships in children of incarcerated mothers. Child Dev. 2005;76(3):679–96.
Zero to Three. Diagnostic classification: 0–3: diagnostic classification of mental health and developmental disorders of infancy and early childhood. Washington, DC: Zero to Three: National Center for Infants, Toddlers and Families; 1999. 134 p.
Rettig MA, McCarthy-Rettig K. A survey of the health, sleep, and development of children adopted from China. Health Soc Work. 2006;31(3):201–7.
Dawson G, Hessl D, Frey K. Social influences of early developing biological and behavioral systems related to risk for affective disorder. Dev Psychopathol. 1994;6(4):759–79.
Hiscock H, Wake M. Randomised controlled trial of behavioural infant sleep intervention to improve infant sleep and maternal mood. BMJ. 2002;324(7345):1062–5.
Stremler R, Hodnett E, Lee K, MacMillan S, Mill C, Ongcangco L, et al. A behavioral-educational intervention to promote maternal and infant sleep: a pilot randomized, controlled trial. Sleep. 2006;29(12):1609–15.
Mindell JA, Owens JA. A clinical guide to pediatric sleep: diagnosis and management of sleep problems. New York: Lippincott Williams and Wilkins; 2003.
Mindel J. Sleeping through the night. New York: Harper Collins; 1997.
Ferber R. Solve your child’s sleep problems. New York: Simon & Schuster; 1985.
Lumeng JC, Chervin RD. Epidemiology of pediatric obstructive sleep apnea. Proc Am Thorac Soc. 2008;5(2):242–52. Epub 2008/02/06.
Owens J, Spirito A, Marcotte A, McGuinn M, Berkelhammer L. Neuropsychological and behavioral correlates of obstructive sleep apnea syndrome in children: a preliminary study. Sleep Breath. 2000;4(2):67–78.
Lewin DS, Huntley ED, Eisner M, editors. Neurobehavioral assessment of the effects of sleep restriction on children with obstructive sleep apnea OSA and a healthy comparison group. 18th Annual Meeting of the Associated Professional Sleep Societies (APSS). Philadelphia, PA: American Academy of Sleep Medicine; 2004.
Picchietti D, Allen RP, Walters AS, Davidson JE, Myers A, Ferini-Strambi L. Restless legs syndrome: prevalence and impact in children and adolescents—the Peds REST study. Pediatrics. 2007;120(2):253–66. Epub 2007/08/03.
Picchietti DL, Bruni O, de Weerd A, Durmer JS, Kotagal S, Owens JA, et al. Pediatric restless legs syndrome diagnostic criteria: an update by the International Restless Legs Syndrome Study Group. Sleep Med. 2013;14(12):1253–9. Epub 2013/11/05.
Mindell JA. Empirically supported treatments in pediatric psychology: bedtime refusal and night wakings in young children. J Pediatr Psychol. 1999;24(6):465–81.
Harvey AG. A cognitive model of insomnia. Behav Res Ther. 2002;40(8):869–93. Epub 2002/08/21.
Dohnt H, Gradisar M, Short MA. Insomnia and its symptoms in adolescents: comparing DSM-IV and ICSD-II diagnostic criteria. J Clin Sleep Med. 2012;8(3):295–9. Epub 2012/06/16.
Richardson CE, Gradisar M, Barbero SC. Are cognitive “insomnia” processes involved in the development and maintenance of delayed sleep wake phase disorder? Sleep Med Rev. 2015;26:1–8. Epub 2015/07/05.
Edinger JD, Buysse DJ, Deriy L, Germain A, Lewin DS, Ong JC, et al. Quality measures for the care of patients with insomnia. J Clin Sleep Med. 2015;11(3):311–34. Epub 2015/02/24.
Medicine AAoS. International classification of sleep disorders. Sateia M, editor. 3rd ed. Darien, IL: American Academy of Sleep Medicine; 2014.
Owens JA, Babcook D, Blumer J, Chervin RD, Ferber R, Goetting M, et al. The use of pharmacotherapy in the treatment of pediatric insomnia in primary care: rational approaches. A consensus meeting summary. J Clin Sleep Med. 2005;1(1):49–59.
Carney CE, Buysse DJ, Ancoli-Israel S, Edinger JD, Krystal AD, Lichstein KL, et al. The consensus sleep diary: standardizing prospective sleep self-monitoring. Sleep. 2012;35(2):287–302. Epub 2012/02/02.
Werner H, Molinari L, Guyer C, Jenni OG. Agreement rates between actigraphy, diary, and questionnaire for children’s sleep patterns. Arch Pediatr Adolesc Med. 2008;162(4):350–8.
Spruyt K, Gozal D. Development of pediatric sleep questionnaires as diagnostic or epidemiological tools: a brief review of dos and don’ts. Sleep Med Rev. 2011;15(1):7–17. Epub 2010/10/19.
Owens JA, Spirito A, McGuinn M. The Children’s Sleep Habits Questionnaire (CSHQ): psychometric properties of a survey instrument for school-aged children. Sleep. 2000;23(8):1043–51.
Chervin RD, Hedger K, Dillon JE, Pituch KJ. Pediatric sleep questionnaire (PSQ): validity and reliability of scales for sleep-disordered breathing, snoring, sleepiness, and behavioral problems. Sleep Med. 2000;1(1):21–32.
Chervin RD, Weatherly RA, Garetz SL, Ruzicka DL, Giordani BJ, Hodges EK, et al. Pediatric sleep questionnaire: prediction of sleep apnea and outcomes. Arch Otolaryngol Head Neck Surg. 2007;133(3):216–22.
Chervin RD, Ruzicka DL, Giordani BJ, Weatherly RA, Dillon JE, Hodges EK, et al. Sleep-disordered breathing, behavior, and cognition in children before and after adenotonsillectomy. Pediatrics. 2006;117(4):e769–78.
Ancoli-Isreal S. Actigraphy. In: Kryger MH, Roth T, Dement WC, editors. Principles and practice of sleep medicine. Philadelphia, PA: Elsevier/Saunders; 2005. p. xxxiii. 1517 p.
Sadeh A, Acebo C. The role of actigraphy in sleep medicine. Sleep Med Rev. 2002;6(2):113–24.
Sadeh A, Alster J, Urbach P. Actigraphically based sleep-wake scoring. J Ambulat Monit. 1989;2:209–16.
Achenbach TM. Manual for the child behavior checklist/4–18. Burlington, VT: Department of Psychiatry, University of Vermont; 1991.
Achenbach TM. Manual for the child behavior checklist/2–3 and 1992 profile. Burlington, VT: Department of Psychiatry, University of Vermont; 1992. p. xi. 210 pp.
Birmaher B, Brent DA, Chiappetta L, Bridge J, Monga S, Baugher M. Psychometric properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED): a replication study. J Am Acad Child Adolesc Psychiatry. 1999;38(10):1230–6.
Birmaher B, Khetarpal S, Brent D, Cully M, Balach L, Kaufman J, et al. The Screen for Child Anxiety Related Emotional Disorders (SCARED): scale construction and psychometric characteristics. J Am Acad Child Adolesc Psychiatry. 1997;36(4):545–53.
Kovacs M. The children’s depression, inventory (CDI). Psychopharmacol Bull. 1985;21(4):995–8.
Conners CK, Sitarenios G, Parker JD, Epstein JN. The revised Conners’ Parent Rating Scale (CPRS-R): factor structure, reliability, and criterion validity. J Abnorm Child Psychol. 1998;26(4):257–68.
Minde K, Faucon A, Falkner S. Sleep problems in toddlers: effects of treatment on their daytime behavior. J Am Acad Child Adolesc Psychiatry. 1994;33(8):1114–21.
Mindell J, Kuhn B, Lewin D, Meltzer L, Sadeh A. Behavioral treatment of bedtime problems and night wakings in infants and young children. Sleep. 2006;29(10):1263–76.
Clarke G, McGlinchey EL, Hein K, Gullion CM, Dickerson JF, Leo MC, et al. Cognitive-behavioral treatment of insomnia and depression in adolescents: a pilot randomized trial. Behav Res Ther. 2015;69:111–8. Epub 2015/04/29.
Paine S, Gradisar M. A randomised controlled trial of cognitive-behaviour therapy for behavioural insomnia of childhood in school-aged children. Behav Res Ther. 2011;49(6–7):379–88. Epub 2011/05/10.
France KG. Behavior characteristics and security in sleep-disturbed infants treated with extinction. J Pediatr Psychol. 1992;17(4):467–75.
Adams LA, Rickert VI. Reducing bedtime tantrums: comparison between positive routines and graduated extinction. Pediatrics. 1989;84(5):756–61.
Bootzin RR, Stevens SJ. Adolescents, substance abuse, and the treatment of insomnia and daytime sleepiness. Clin Psychol Rev. 2005;25(5):629–44.
Degotardi PJ, Klass ES, Rosenberg BS, Fox DG, Gallelli KA, Gottlieb BS. Development and evaluation of a cognitive-behavioral intervention for juvenile fibromyalgia. J Pediatr Psychol. 2006;31(7):714–23.
Weiss MD, Wasdell MB, Bomben MM, Rea KJ, Freeman RD. Sleep hygiene and melatonin treatment for children and adolescents with ADHD and initial insomnia. J Am Acad Child Adolesc Psychiatry. 2006;45(5):512–9.
Moore BA, Friman PC, Fruzzetti AE, MacAleese K. Brief report: evaluating the Bedtime Pass Program for child resistance to bedtime—a randomized, controlled trial. J Pediatr Psychol. 2007;32(3):283–7.
Freeman KA. Treating bed time resistance with the bed time pass: a systematic replication and component analysis with 3-year-olds. J Appl Behav Anal. 2006;39(4):423–8.
France KG, Blampied NM, Wilkinson P. Treatment of infant sleep disturbance by trimeprazine in combination with extinction. J Dev Behav Pediatr. 1991;12(5):308–14.
Price AM, Wake M, Ukoumunne OC, Hiscock H. Five-year follow-up of harms and benefits of behavioral infant sleep intervention: randomized trial. Pediatrics. 2012;130(4):643–51. Epub 2012/09/12.
Irwin MR, Cole JC, Nicassio PM. Comparative meta-analysis of behavioral interventions for insomnia and their efficacy in middle-aged adults and in older adults 55+ years of age. Health Psychol. 2006;25(1):3–14. Epub 2006/02/02.
Morin CM, Bootzin RR, Buysse DJ, Edinger JD, Espie CA, Lichstein KL. Psychological and behavioral treatment of insomnia: update of the recent evidence (1998–2004). Sleep. 2006;29(11):1398–414. Epub 2006/12/14.
de Bruin EJ, Bogels SM, Oort FJ, Meijer AM. Efficacy of cognitive behavioral therapy for insomnia in adolescents: a randomized controlled trial with internet therapy, group therapy and a waiting list condition. Sleep. 2015;38:1913–26. Epub 2015/07/15.
de Bruin EJ, Oort FJ, Bogels SM, Meijer AM. Efficacy of internet and group-administered cognitive behavioral therapy for insomnia in adolescents: a pilot study. Behav Sleep Med. 2014;12(3):235–54. Epub 2013/06/19.
Borbély AA, Achermann P. Sleep homeostasis and models of sleep regulation. In: Kryger MH, Roth T, Dement WC, editors. Principles and practices of sleep medicine. Philadelphia: Elsevier Saunders; 2005. p. 405–17.
Spielman AJ. Assessment of insomnia. Clin Psychol Rev. 1986;6(1):11–25.
Miller CB, Espie CA, Epstein DR, Friedman L, Morin CM, Pigeon WR, et al. The evidence base of sleep restriction therapy for treating insomnia disorder. Sleep Med Rev. 2014;18(5):415–24. Epub 2014/03/19.
Morgenthaler T, Kramer M, Alessi C, Friedman L, Boehlecke B, Brown T, et al. Practice parameters for the psychological and behavioral treatment of insomnia: an update. An American academy of sleep medicine report. Sleep. 2006;29(11):1415–9. Epub 2006/12/14.
Bootzin RR, editor. Stimulus control treatment for insomnia. 80th Annual Convention of the American Psychological Association. Washington, DC: American Psychological Association; 1972.
Spielman AJ, Saskin P, Thorpy MJ. Treatment of chronic insomnia by restriction of time in bed. Sleep. 1987;10(1):45–56. Epub 1987/02/01.
Health NIo. How much sleep is enough? National Heart Lung and Blood Institute; 2012. https://www.nhlbi.nih.gov/health/health-topics/topics/sdd/howmuch.
Iglowstein I, Jenni OG, Molinari L, Largo RH. Sleep duration from infancy to adolescence: reference values and generational trends. Pediatrics. 2003;111(2):302–7 [see comment].
National Sleep Foundation. National Sleep Foundation: Sleep in America Poll. Sleep and children. Washington, DC: National Sleep Foundation; 2004.
National Sleep Foundation. National Sleep Foundation: Sleep in America Poll. Sleepy Teens. Washington, DC: National Sleep Foundation; 2006.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Lewin, D.S., Huntley, E. (2017). Insomnias of Childhood: Assessment and Treatment. In: Attarian, H. (eds) Clinical Handbook of Insomnia. Current Clinical Neurology. Springer, Cham. https://doi.org/10.1007/978-3-319-41400-3_8
Download citation
DOI: https://doi.org/10.1007/978-3-319-41400-3_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-41398-3
Online ISBN: 978-3-319-41400-3
eBook Packages: MedicineMedicine (R0)