
Abstract
Vasculitic neuropathy may occur as a part of systemic vasculitis or an isolated vasculitis of the peripheral nervous system. The typical clinical syndrome is mononeuropathia multiplex, but distal-symmetric neuropathy can also be observed. Neurophysiological examination reveals axonal damage in most cases and nerve biopsy shows inflammatory infiltrates together with vessel wall damage. Treatment includes steroids, cyclophosphamide, azathioprine, rituximab and other immunosuppressants. This chapter provides an overview about clinical, laboratory and histopathological diagnostic criteria and the current treatment options for vasculitic neuropathy.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Vasculitic neuropathies are a group of inflammatory neuropathies, characterised by inflammation of the vasa nervorum, mainly the epineural arteries of the nerve. They can occur as non-systemic vasculitis (non-systemic vasculitic neuropathy NSVN, exclusively affecting the peripheral nervous system) or part of a systemic vasculitis including the involvement of other organs (systemic vasculitic neuropathy) (Table 23.1). The differential diagnosis may be difficult, if the neuropathy is the first manifestation of vasculitis. The exact incidence of vasculitic neuropathy has never been investigated in bigger studies. However, the annual incidence of systemic vasculitis is 60–140/million, which includes a part of 30 % secondary systemic vasculitis [1, 2]. In nerve biopsy specimen obtained in neuropathy of unknown reason, about 1 % show vasculitic neuropathy [3, 4]. Some systemic vasculitic diseases are rarely associated with neuropathy, whereas in others, such as Churg-Strauss syndrome , it belongs to the diagnostic criteria (Table 23.2) [5].
2 Classifi cation
In 1990, the American College of Rheumatology presented classification criteria for PAN, CSS, GPA and others. However, this classification was criticized because (1) there was no discrimination between vasculitis from non-vasculitic disease and (2) ANCA testing was not included in the classification. The Chapel Hill consensus conference (CHCC) in 1994 proposed definitions for most vasculitic diseases according to the size and pathology of the involved vessels [6]. In 2007, a new classification incorporating both ACR and CHCC criteria was established and Wegener’s granulomatosis was renamed granulomatosis with polyangiitis [7]. The 2012 second CHCC updated some of the diagnostic criteria for vasculitis. More recently, it has been proposed to divide the vasculitic neuropathies in two groups according to the size of the affected nerve vessels, distinguishing a nerve large arteriole vasculitis from a nerve microvasculitis. The latter involves arterioles <40 μm and endoneurial microvessels and includes the most non-systemic vasculitic neuropathy, Sjögren syndrome and some virus-associated vasculitic neuropathies [8]. Most neurologists also use the classification developed from the Peripheral Nerve Society Task Force. Vasculitic neuropathy is categorized in primary systemic vasculitis, secondary systemic vasculitis or non-systemic/localized vasculitis depending on the disease-associations (Table 23.1) [9].
3 Pathogenesis
Blood supply in the peripheral nervous system is secured by the regional vasa nervorum, which feed an extensive network between the epineurial and the endoneurial vessels. This allows a functionality of the peripheral nerve even under anaerobic conditions and makes the nerve quite resistant to ischemic damage [10]. The underlying etiology of the vasculitic disease may be different, and, in some diseases, not completely understood. However, occlusion of vessels by vascular inflammation leading to ischemic nerve damage is the common final path in vasculitic neuropathy. This ischemic damage occurs diffusely in the whole nerve, but with a maximum effect in the proximal and middle parts of the nerves, which is the most vulnerable zone to ischemia [11]. In cryoglobulinemia, anti-sulfatide antibodies can be found, which may be involved in the pathogenesis [12]. An increased expression of nerve growth factor (NGF) may be involved in the pain development of vasculitic neuropathy [13].
4 Clinical Features and Diagnostic Procedures
The typical clinical presentation of vasculitis is mononeuropathia multiplex . However, about 30–60 % of patients with vasculitis have other clinical types of neuropathy including painful sensorimotor axonal neuropathy or pure sensory neuropathy or asymmetric neuropathy. Pain is a regular symptom in most vasculitic neuropathies. In biopsy-proven vasculitic neuropathy, 10–40 % are distal-symmetric pattern [14–16]. The peroneal and tibial nerves on the lower and the ulnar nerve on the upper limb are most frequently involved in vasculitic neuropathy. However, there is no association of a distinct clinical pattern with a special type of vasculitic disease. The majority of vasculitic neuropathies develop subacute within days to weeks and only in a few cases, a chronic, slowly progressing neuropathy has been observed. About 80 % of neuropathies associated with systemic vasculitis, but also 50 % of patients with non-systemic vasculitic neuropathies have general symptoms (weight loss, fever, myalgia, or fatigue).
The neurophysiological examination shows multifocal axonal neuropathy including reduced CMAP amplitudes with only slightly reduced nerve conduction velocities (NCV) in neurography [14, 17, 18]. However, if the CMAP amplitudes are massively reduced, the NCV can also be reduced because of the loss of thick myelinated fibres. A transient nerve conduction block can be observed early after symptom onset and represents an ongoing Wallerian degeneration, which has not been completed distal of the affected nerve; however, within 1–2 weeks, this phenomenon disappears. Electromyography reveals neurogenic pattern including spontaneous muscle fiber activity, and polyphasic, extended, or high-amplitude motor unit action potentials (MUAP). However, if an additional vasculitic myopathy is also present, myopathic and neurogenic changes can be observed at the same time [9, 19].
Whenever systemic vasculitis or another reason for the neuropathy is not known, a variety of laboratory investigations should be performed. As a first step, routine laboratory investigations should be performed in neuropathies with unknown reason. If an inflammatory neuropathy is suspected, a more detailed laboratory investigation should be performed (Table 23.3). Analysis of the cerebrospinal fluid will not increase the sensitivity to detect vasculitic neuropathy, but can be an important investigation in the differential diagnosis of an as yet unclear neuropathy. Other routine technical diagnostic procedures depend on the suspected diagnosis (Table 23.4).
If a patient develops subacute asymmetrical neuropathy or mononeuropathia multiplex without evidence for systemic vasculitis, nerve biopsy should be performed. In most cases, the sural nerve is used with or without muscle biopsy. The combined biopsy of the superficial peroneal nerve together with the peronaeus brevis muscle is an alternative to the sural nerve biopsy [20]. Although controlled studies are lacking, the combined nerve/muscle biopsy has a slightly higher sensitivity to detect vasculitis and the biopsy of the peronaeus brevis muscle may be more effective than the gastrocnemius muscle. One study used a proximal muscle for biopsy (quadriceps) and showed no increased yield for vasculitic neuropathy compared to nerve biopsy alone, indicating that distal muscles are more suitable for biopsy in suspected vasculitis [14].
4.1 Pathology
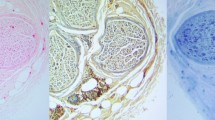
The histopathological diagnosis of vasculitic neuropathy requires different criteria, which have been set up in detail in a guideline of the Peripheral Nerve Society [9]. The definite diagnosis of vasculitis includes both intramural inflammation (Fig. 23.1) and additionally vessel damage (Table 23.5). It can be distinguished between findings in active lesions and chronic lesions. However, not all patients meet the criteria for definite vasculitic neuropathy, although vasculitis is clinically highly suspected. For these cases, criteria for probable vasculitic neuropathy have been established (Table 23.6). The histopathological picture shows mainly axonal damage, and the predominant blood vessels affected are epineurial more than peri- or endoneurial. The cellular infiltrates include mainly T-lymphocytes and macrophages, B-cells are rarely seen. In PAN and CSS eosinophils may also be present. Immune complex deposits consisting of complement proteins, immunoglobulins and fibrinogen may be present [21, 22].

Peripheral nerve vasculitis. Epineurial vessel with lymphocyte infiltration and subtotal stenosis. Lymphocytes stained with anti-LCA (lymphocyte common antigen) antibody (Courtesy of Prof. J. Weis, Aachen)
5 Primary Systemic Vasculitides
Neuropathies associated with primary systemic vasculitides have been classified according to the diameter of the affected blood vessels into three groups: large-vessel-, medium-vessel-, and small-vessel vasculitis. Vasculitic neuropathy can be observed predominantly in the small-vessel- and medium-vessel vasculitides, since the vessel diameters in nerves and muscles are mainly in a range between 50 and 300 μm.
5.1 Large Vessel Vasculitides
The large vessel vasculitides include Takayasu arteritis and giant cell arteritis. Takayasu arteritis is normally not associated with neuropathies, but shows significant central nervous system involvement, mainly strokes. Giant cell arteritis patients often have central nervous system involvement, in some rare cases, neuropathies have been described [23].
5.2 Medium-Sized Vessel Vasculitides
5.2.1 Polyarteritis Nodosa (PAN)
The polyarteritis nodosa is a very rare disease, the annual incidence decreased to 0.1–1.6 cases/million in developed countries after establishment of hepatitis B vaccination [24]. The histopathological features have been revised in the CHCC. PAN is a disease of the small and medium-sized arteries, sparing arterioles, capillaries and venules. The vascular inflammation is segmental, often predominantly seen in branching points with mixed inflammatory infiltrates [25]. In later stages vascular remodelling with intima hyperplasia and diffuse fibrotic changes can be found. PAN can develop as idiopathic form, but also associated with viral infections. Hepatitis B was the main virus inducing PAN, but hepatitis C virus, cytomegalovirus, HIV, parvovirus B19 and even streptococci can also trigger the disease. The clinical symptoms include constitutional symptoms, such as fever, weight loss and arthralgia, but also organ involvement of different organ symptoms, of which skin symptoms and nervous system involvement are the most frequent. In contrast to other primary systemic vasculitides , PAN is a typical monophasic disease with a relapse rate of less than 10 %. Heart and central nervous system involvement determines a poor prognosis. The French vasculitis group proposed a five factor score for estimation of the prognosis of PAN. Neuropathies can be found in about 75 % of PAN patients [26]. The typical manifestation is a painful mononeuropathia multiplex , but distal-symmetric sensorimotor neuropathies and even chronic inflammatory demyelinating polyneuropathy (CIDP) can be observed as peripheral nervous system involvement in PAN [5]. There is no typical laboratory abnormality, blood sedimentation rate and C-reactive protein are often elevated and PAN is not associated with ANCA. The diagnosis can be confirmed by the typical histological features in biopsy and/or the detection of microaneurysms in the intestinal angiography .
5.3 Small Vessel Vasculitides
5.3.1 Churg-Strauss Syndrome (CSS)
This vasculitis type was first described in 1951 by Churg and Strauss. A development over different phases can be observed: (1) a prodromal phase with asthma or rhinitis, which can last for years before the vasculitic symptoms develop, (2) an intermittent phase with eosinophilia and pulmonary eosinophilic infiltrates, and (3) the main vasculitic manifestation including cutaneous, gastrointestinal symptoms, sinusitis, arthralgia and vasculitic neuropathy. PNS involvement is frequent (75–80 % of patients) and neuropathy can be the initial manifestation in a substantial proportion of patients [27]. The main clinical syndrome is mononeuropathia multiplex , some patients may have pure sensory or sensorimotor distal neuropathy [28, 29]. Neurophysiological examination shows typically an axonal damage. Eosinophilia in the peripheral blood can be found regularly and in 40–70 % of patients, pANCA are positive [30]. Eosinophilic infiltrates are present in biopsy specimen of nerve and other tissues [29]. One study suggests two different histopathological types of neuropathy in CSS patients. In this study, ANCA-positive CSS patients have predominantly necrotizing vasculitis in the nerve biopsy, whereas ANCA-negative CSS nerve biopsies show a large number of eosinophilic infiltrates in the epineurium [29].
5.4 Granulomatosis with Polyagiitis (GPA )
GPA is a vasculitic disease, regularly associated with c-ANCA , which are directed against proteinase 3. Mostly, patients have granulomatous involvement of the upper and lower respiratory tract and additional rapid-rapidly progressive glomerulonephritis. Subsequent development of vasculitic disease is common and many patients show the full-generalised form including pulmonary and renal involvement. Interestingly, the c-ANCA seems to be directly involved in the physiopathology by activation and degranulation of granulocytes. The cANCA bind to surface-expressed proteinase-3, which has been translocated from inside the cell by the proinflammatory cytokines TNF-α and IL-1. The degranulation of the granulocytes then induces a necrotizing vasculitis with endothelial damage.
Vasculitic neuropathy can be observed in 20–25 % of GPA patients [31, 32]. Most of them show mononeuritis multiplex , in a few patients, cranial nerve involvement has been described [33]. The neuropathy may be the first symptom of GPA in some patients, which underlines the importance of ANA/ANCA diagnostic tests in patients with newly diagnosed asymmetric neuropathy [27].
5.5 Microscopic Polyangiitis (MPA)
MPA is a systemic, necrotizing vasculitis of the small vessels, mainly in older patients with a slight male predominance. Patients have lung involvement, glomerulonephritis, skin lesions and abdominal pain. In 50–75 % of patients p-ANCA can be found, some patients can have c-ANCA [34]. About 10–50 % of MPA patients develop neuropathy. The most frequent clinical manifestation is mononeuropathia multiplex , mainly affecting the peroneal, median and ulnar nerves [33, 35, 36].
6 IgG4-Related Disease
Immunoglobulin G4-related disease was recently recognized as a common pathophysiology in a heterogeneous group of diseases and can affect a variety of organ systems [37]. One of the first diseases described is the Mikulicz syndrome, an inflammatory disease of the salivary gland, which was already described in the late nineteenth century [38]. The main finding is an infiltration of the affected tissue with IgG4+ plasma cells; the IgG4 level in the serum may be elevated [39]. Single cases of an IgG4-associated neuropathy were reported, but the incidence of IgG4-related neuropathy is unknown yet [40].
7 Secondary Systemic Vasculitis
Secondary systemic vasculitis is a heterogeneous disease group. Infectious diseases, connective tissue diseases, malignancies and drugs can cause vasculitis including vasculitic neuropathy.
7.1 Systemic Lupus Erythematosus (SLE)
A variety of neurological disturbances can be observed in SLE , including cerebral vasculitis, which often leads to stroke, cerebral venous thrombosis, transverse myelitis, or peripheral neuropathy. The latter can be observed in about 10–20 % of SLE patients [41, 42]. Clinically, the neuropathy in SLE is mainly distal-symmetric sensory or sensorimotor neuropathy and less frequent mononeuropathia multiplex or small fibre [41]. Neurophysiological investigation reveals axonal type in 80–90 % and demyelinating type in 10–20 % of SLE -associated neuropathy. Autonomic disturbances are present in one third of the neuropathy patients, including both sympathetic and parasympathetic nervous system involvement [43].
7.2 Systemic Sclerosis (SSc)
About 30 % of systemic sclerosis patients have neuropathy, predominantly sensory or small-fibre type [44]. Additionally, autonomic dysfunction causes mainly gut motility disturbances in these patients [45]. In some cases of systemic sclerosis, neuropathy can be the initial presentation of the disease.
7.3 Sjögren’s Syndrome
Due to an affection of the exocrine glands, Sjögren’s syndrome is clinically defined by the so-called sicca complex (dry eyes/dry mouth). Anti-SSA and –SSB autoantibodies, a subgroup of ENA can be found regularly in these patients [46]. Interestingly, autoantibodies against the muscarinic M3 receptor seem to have an important pathophysiological role in the sialoadenitis and could also be involved in the nervous system manifestations of these patients [47]. Both central and peripheral nervous system involvement including trigeminal nerve affection has been described [48]. Neuropathies have been found in 2–64 % of the patients. These neuropathies can be symmetric or asymmetric or resemble small fibre neuropathy and only a small part of them are vasculitic [49].
7.4 Rheumatoid Arthritis (RA)
About 15–50 % of RA patients develop neuropathy. However, peripheral nervous system disease in RA can have a variety of origins, such as drug-induced neuropathy or entrapment mononeuropathy. The main form of polyneuropathy is an axonal, distal-symmetric sensorimotor neuropathy [50].
7.5 Paraneoplastic Vasculitic Neuropathy
Until now, every clinical type of neuropathy was found in paraneoplastic (tumor-associated) neuropathy. However, pure sensory neuronopathy (Denny-Brown) is the most classical type of paraneoplastic neuropathy, and this special neuropathy is mainly associated with small cell lung cancer (SCLC) and anti-Hu antibodies can be found (Fig. 23.2). In general, SCLC, breast and ovarian cancer as well as lymphoma are the most frequent tumors found in paraneoplastic neuropathy [51]. Patients with vasculitic paraneoplastic neuropathy have mostly mononeuropathia multiplex or asymmetric neuropathy. Torvik and Berntzen in 1968 and Johnson et al. 1979 described the first patients with vasculitic neuropathy associated with tumors (renal cell carcinoma, SCLC or lymphoma) [52, 53]. Oh described 26 patients with paraneoplastic vasculitic neuropathy, mainly associated with SCLC and lymphoma. Many of them had elevated CSF protein and high ESR [54]. Clinically, mononeuritis multiplex and distal-symmetric sensorimotor neuropathy can be observed. If paraneoplastic vasculitic neuropathy is suspected, antineuronal autoantibodies, as well as antinuclear antibodies (ANA) and ANCA should be examined. In some patients with paraneoplastic neuropathies, both vasculitic and non-vasculitic, only ANA can be found [55]. Non-vasculitic paraneoplastic neuropathies, such as the anti-Hu positive sensory neuronopathy Denny-Brown, do not respond to immunotherapy, whereas vasculitic paraneoplastic neuropathy may respond to immunosuppressants (steroids, cyclophosphamide ) in the majority of patients.

Antineuronal antibody (antu-Hu) from a patient with vasculitic neuropathy and small cell lung cancer. Staining of neuronal nuclei and (to a lesser extent) cytoplasm of cerebellar neurons
7.6 Hepatitis C/Cryoglobulinemia
Cryoglobulinemia can occur essential or in the context of chronic infections or lymphoproliferative diseases. The cryoglobulins are mono- or polyclonal immunoglobulins, that precipitate at cool temperatures and these proteins can induce vascular damage by occlusion of microvessels or induction of immune complex deposits in small vessels [56–58]. Fifty per cent of hepatitis C patients have mixed cryoglobulinemia , but only 15 % of them develop the clinical syndrome of mixed cryoglobulinemic vasculitis (MCV). About 80 % of MCV lacking other reasons are caused by chronic hepatitis C. The clinical symptoms consist of skin lesions (purpura), neuropathy, glomerulonephritis, ulcers, arthritis, and sicca syndrome. Rheumatoid factor can be found in more than 80 % and decreased complement factors C3 and C4 occur in 70 % of MCV patients [56]. The pathophysiological role of anti-sulfatide and anti-ganglioside antibodies , which can be detected in a part of MCV-associated neuropathy, is still not elucidated yet [12].
Neuropathy can be asymmetric, mononeuropathia multiplex or distal-symmetric, the latter often showing a slowly progressive course, whereas the others develop acute or subacute [59, 60]. Pure sensory neuropathy has also been described [50]. Pain occurs in 50 % of MCV-associated neuropathy and predominant small-fibre neuropathies have also been observed [59]. Neurophysiological examination reveals axonal neuropathy and even without clinical symptoms, most patients with MCV show at least neurophysiological abnormalities suggestive of neuropathy [61–63]. Nerve biopsy studies show axonal damage, perivascular infiltration with mononuclear cells predominantly in the epineurium and IgM and complement deposits in the affected vessel walls [59, 63, 64].
7.7 Other Secondary Systemic Vasculitides
Sarcoidosis can be associated with mononeuropathia multiplex , small fibre neuropathy or typical CIDP. The latter shows a good response to intravenous immunoglobulins (IVIg) , the others respond regularly to steroids [65–68].
Behcet’s disease and inflammatory bowel disease both are rarely associated with neuropathy and most of them are non-vasculitic. In both diseases, central nervous system involvement is much more frequent [69, 70].
A vasculitic neuropathy in HIV has been described in association with cytomegalovirus (CMV) or with lymphoma. This disease may be the result of immune complex deposition more than direct HIV infection of the nervous system [71–73]. However, there is an increased risk for HIV patients to develop other secondary vasculitides, including PAN or MPA .
7.8 Drug-Induced Vasculitic Neuropathy
A variety of drugs can induce vasculitis, both ANCA-positive and –negative. These drugs include many of the new biologicals (etanercept , adalimumab , infliximab and others) as well as other medications, such as carbimazole or levamisole. Some drugs have especially been reported to induce vasculitic neuropathy. However, to prove a causal relationship is sometimes difficult, since some of the drugs are given as a treatment of vasculitic diseases. The antibiotic minocycline can induce a non-systemic vasculitic neuropathy [74, 75]. Other drugs, such as naproxen , penicillin or the antiepileptic phenytoin induced systemic vasculitis including neuropathy, and the discontinuation of the drug resulted in an improvement of the vasculitis [76]. Table 23.7 gives an overview about drugs, which can induce vasculitic neuropathy.
8 Non-systemic Vasculitis of the Peripheral Nervous System
If vasculitic neuropathy occurs without detectable systemic involvement, the term non-systemic vasculitic neuropathy (NSVN) is used. About 25 % of all vasculitic neuropathies belong to this group [44]. The course of NSVN is often subacute, but about one third of the patients show progressive disease. The typical clinical picture is an asymmetric, progressive and painful neuropathy with severe paresis [77]. The neurophysiological examination shows axonal sensorimotor or motor neuropathy. Mostly, NSVN remains a localized vasculitis; however, in some cases additional skin manifestations or generalization was observed and the neuropathy tends to relapse, when immunosuppressive treatment is reduced [78, 79]. Nerve biopsy should be performed, if NSVN is suspected and histopathology shows nerve microvasculitis. Recently, the main clinical and histopathological features were published in a guideline of the peripheral nerve society, describing criteria for definite, probable and possible vasculitic neuropathy [9].
Treatment of NSVN includes corticosteroids, cyclophosphamide , methotrexate and azathioprine in the first line and is described in detail in the treatment section. In a recent single-center cohort of 60 patients with histologically proven NSVN, initially all patients improved after iv methylprednisolone. However, after 4 years, 48 % of the patients still had immunosuppressive treatment and an age <64 years was associated with a better prognosis [80].
9 Diabetic and Non-Diabetic Lumbosacral Radiculoplexus Neuropathy (DLRPN/LRPN)
In patients with diabetes, the lumbosacral plexus including roots and peripheral nerves can be affected in a often painful disease, termed diabetic lumbosacral radiculoplexus neuropathy (DLRPN) [81]. The disease starts often with acute, severe neuropathic pain, followed by asymmetric paresis of the lower limbs, which become disabling during the acute stage. DLRPN is a monophasic disease, but half of the patients have walking difficulties or become wheelchair bound in this stage [8]. Autonomic symptoms can be found in 50 % of DLRPN patients. Spontaneous recovery may occur, but most patients have incomplete recovery including weakness and sensory disturbances. Interestingly, it mainly affects patients with mild diabetes mellitus in a stable situation; a non-diabetic form (LRPN) has also been described. Although upper limb nerves can be involved in DLRPN, a separate upper limb variant exists (DCRPN) [82]. Moreover, an overlap with CIDP has been described in some patients [83]. The histopathological picture is a focal nerve ischemia, caused by microvasculitis [84]. Neurophysiological examination shows axonal involvement of the lumbosacral plexus and very often includes paraspinal denervation. The cerebrospinal analysis reveals elevated total protein and a normal cell count in most patients.
10 Treatment
10.1 Treatment of Non-Systemic Vasculitic Neuropathy (NSVN)
There are no randomized controlled studies (RCT) for NSVN yet. However, the Peripheral Nerve Society published recommendations for the treatment of NSVN [9]. It is recommended to treat NSVN patients with corticosteroids (initially prednisolone 1 mg/kg/day) with a slow tapering over months. Initial high-dose prednisolone pulses (500–1000 mg prednisolone for 3–5 days) can be used alternatively, followed by daily treatment with 1 mg/kg. Osteoporosis prophylaxis should be given; it is unclear yet, whether steroid treatment increases the risk of peptic ulcers and whether patients should be treated with proton pump inhibitors prophylactically. In case of rapid progressive neuropathy, cyclophosphamide (CYC) pulse treatment should be considered and long-term immunosuppression with methotrexate or azathioprine is necessary [85]. To reduce the risk of hemorrhagic cystitis, mesna should always be used in CYC pulse therapy and for toxicity reason, CYC should only be given for 6–12 months. There are two cohort studies, which implicate a better efficiency of a combination therapy [16, 79]. Other treatment regimens are poorly investigated. Intravenous immunoglobulins have been used successfully in a few otherwise treatment-resistant vasculitis patients [86]. Plasma exchange seems to have little effect, even in combination treatment [87–89]. Since rituximab treatment shows a good effect also on the neuropathic symptoms in generalized vasculitic diseases, it may also be used for NSVN in otherwise treatment-refractory patients [90]. Since vasculitic neuropathies usually are predominantly axonal, no significant improvement may be seen in the first weeks or even months. However, there is no surrogate marker, by which the treatment efficacy during the treatment can be verified. The first symptom, which may improve under sufficient immunosuppression, is the neuropathic pain.
10.2 Treatment of Non-Viral Systemic Vasculitic Neuropathy (SVN)
The treatment of vasculitic neuropathy associated with systemic vasculitis (SVN) should be performed according to the guidelines of the underlying systemic disease. As in NSVN, corticosteroids are used as initial treatment of SVN in the same dosages. Improvement of SVN may last weeks or months because of the axonal damage of the nerves. Therefore, erythrocyte sedimentation rate or C-reactive protein can be used to control the efficacy of the treatment. Suppiah and colleagues recently reported a rate of 15 % clinical apparent neuropathy in a cohort of ANCA-associated vasculitis and 40 % improved after treatment [33]. In severe SVN cases, cyclophosphamide (CYC) is used either additionally or subsequently to corticosteroid treatment. Daily oral cyclophosphamide shows serious side effects, therefore pulse therapy (0.6–0.75 g/m2 every 2–4 weeks) should be preferred and mesna should be given to avoid hemorrhagic cystitis. Cyclophosphamide treatment should be limited to 6–12 months, since there are a variety of long-term immunosuppressive drugs with less toxic side effects. Methotrexate (20–25 mg weekly) or azathioprine (1–2 mg/kg daily) are the classical long-term immunosuppressants to maintain remission. Leflunomide can be used in the long-term treatment of GPA [91].
Another immunosuppressant in the treatment of vasculitis is mycophenolate mofetil (MMF): However, its effectiveness is not completely clear. One open-label pilot trial showed remission maintenance in 13 out of 17 patients with GPA , in another study relapses were more frequent and earlier in comparison to azathioprine [25, 92]. In lupus treatment, MMF is equally effective to azathioprine but has less side effects [93]. However, no data are available regarding its effect on vasculitic neuropathy.
Rituximab , an anti-CD20 monoclonal antibody, targets mainly B-cells and is established as an effective treatment in MPA and GPA . It has recently been licensed for ANCA-associated vasculitis. In the meantime, rituximab is a first-line therapy of ANCA-associated vasculitis and is as effective as cyclophosphamide [90]. It is also effective in cryoglobulinemic vasculitis and is usually given in a weekly dosage of 375 mg/m2 for four times [94].
10.3 Vasculitis Associated with Infections
Neuropathy associated with mixed cryoglobulinemia /HCV infection includes both antiviral and immunosuppressive treatment. Antiviral treatment includes pegylated interferon-α, ribavirin , telaprevir and boceprevir and, more recently, the direct-acting antiviral agents. Interferon- α (IFN- α) alone or in combination with ribavirin may improve neuropathic symptoms in a smaller part of patients [64, 95, 96]. However, IFN- α is also able to induce inflammatory neuropathies and can also exacerbate other symptoms of mixed cryoglobulinemic vasculitis [97, 98]. Therefore, corticosteroids, cyclophosphamide or plasma exchange should be added in patients with severe neuropathy or if neuropathic symptoms do not improve under antiviral treatment. To remove circulating cryoglobulins, plasma exchange is used in MCV, although there are no RCT yet and only a part of MCV patients respond.
Ferri and collegues reported a cohort of MCV patients responding to rituximab , independently of HCV status [99]. In their study, 95 % of the neuropathic symptoms improved and rituximab was considered safe and effective. In HCV-associated MCV, additional rituximab showed a better response than antiviral treatment alone [100].
References
Gonzalez-Gay MA, Garcia-Porrua C (1999) Systemic vasculitis in adults in northwestern Spain, 1988–1997. Clinical and epidemiologic aspects. Medicine 78:292–308
Watts RA, Carruthers DM, Scott DG (1995) Epidemiology of systemic vasculitis: changing incidence or definition? Semin Arthritis Rheum 25:28–34
Davies L (1994) Vasculitic neuropathy. Bailliere’s Clin Neurol 3:193–210
Kissel JT, Slivka AP, Warmolts JR, Mendell JR (1985) The clinical spectrum of necrotizing angiopathy of the peripheral nervous system. Ann Neurol 18:251–257
Basu N, Watts R, Bajema I, Baslund B, Bley T, Boers M et al (2010) EULAR points to consider in the development of classification and diagnostic criteria in systemic vasculitis. Ann Rheum Dis 69:1744–1750
Jennette JC, Falk RJ, Andrassy K, Bacon PA, Churg J, Gross WL et al (1994) Nomenclature of systemic vasculitides. Proposal of an international consensus conference. Arthritis Rheum 37:187–192
Watts R, Lane S, Hanslik T, Hauser T, Hellmich B, Koldingsnes W et al (2007) Development and validation of a consensus methodology for the classification of the ANCA-associated vasculitides and polyarteritis nodosa for epidemiological studies. Ann Rheum Dis 66:222–227
Gwathmey KG, Burns TM, Collins MP, Dyck PJ (2014) Vasculitic neuropathies. Lancet Neurol 13:67–82
Collins MP, Dyck PJ, Gronseth GS, Guillevin L, Hadden RD, Heuss D et al (2010) Peripheral Nerve Society Guideline on the classification, diagnosis, investigation, and immunosuppressive therapy of non-systemic vasculitic neuropathy: executive summary. J Peripher Nerv Syst 15:176–184
Beggs J, Johnson PC, Olafsen A, Watkins CJ, Cleary C (1991) Transperineurial arterioles in human sural nerve. J Neuropathol Exp Neurol 50:704–718
Dyck PJ, Conn DL, Okazaki H (1972) Necrotizing angiopathic neuropathy. Three-dimensional morphology of fiber degeneration related to sites of occluded vessels. Mayo Clin Proc Mayo Clinic 47:461–475
Alpa M, Ferrero B, Cavallo R, Naretto C, Menegatti E, Di Simone D et al (2008) Anti-neuronal antibodies in patients with HCV-related mixed cryoglobulinemia. Autoimmun Rev 8:56–58
Yamamoto M, Ito Y, Mitsuma N, Hattori N, Sobue G (2003) Pain-related differential expression of NGF, GDNF, IL-6, and their receptors in human vasculitic neuropathies. Intern Med 42:1100–1103
Bennett DL, Groves M, Blake J, Holton JL, King RH, Orrell RW et al (2008) The use of nerve and muscle biopsy in the diagnosis of vasculitis: a 5 year retrospective study. J Neurol Neurosurg Psychiatry 79:1376–1381
Claussen GC, Thomas TD, Goyne C, Vazquez LG, Oh SJ (2000) Diagnostic value of nerve and muscle biopsy in suspected vasculitis cases. J Clin Neuromuscul Dis 1:117–123
Davies L, Spies JM, Pollard JD, McLeod JG (1996) Vasculitis confined to peripheral nerves. Brain 119(Pt 5):1441–1448
Cruz Martinez A, Barbado FJ, Ferrer MT, Vazquez JJ, Perez Conde MC, Gil AA (1988) Electrophysiological study in systemic necrotizing vasculitis of the polyarteritis nodosa group. Electromyogr Clin Neurophysiol 28:167–173
Seo JH, Ryan HF, Claussen GC, Thomas TD, Oh SJ (2004) Sensory neuropathy in vasculitis: a clinical, pathologic, and electrophysiologic study. Neurology 63:874–878
Marcaud V, Gauthier C, Maisonobe T, Hogenhuis J, Morizot-Koutlidis R, Degos CF (2002) Vasculitis confined to the peripheral nervous system: atypical clinical presentation. La Revue de medecine interne/fondee par la Societe nationale francaise de medecine interne 23:558–562
Agadi JB, Raghav G, Mahadevan A, Shankar SK (2012) Usefulness of superficial peroneal nerve/peroneus brevis muscle biopsy in the diagnosis of vasculitic neuropathy. J Clin Neurosci 19:1392–1396
Collins MP, Periquet-Collins I, Sahenk Z, Kissel JT (2010) Direct immunofluoresence in vasculitic neuropathy: specificity of vascular immune deposits. Muscle Nerve 42:62–69
Hattori N, Ichimura M, Nagamatsu M, Li M, Yamamoto K, Kumazawa K et al (1999) Clinicopathological features of Churg-Strauss syndrome-associated neuropathy. Brain 122(Pt 3):427–439
Caselli RJ, Daube JR, Hunder GG, Whisnant JP (1988) Peripheral neuropathic syndromes in giant cell (temporal) arteritis. Neurology 38:685–689
Hernandez-Rodriguez J, Alba MA, Prieto-Gonzalez S, Cid MC (2014) Diagnosis and classification of polyarteritis nodosa. J Autoimmun 48–49:84–89
Hiemstra TF, Walsh M, Mahr A, Savage CO, de Groot K, Harper L et al (2010) Mycophenolate mofetil vs azathioprine for remission maintenance in antineutrophil cytoplasmic antibody-associated vasculitis: a randomized controlled trial. JAMA 304:2381–2388
Guillevin L, Pagnoux C, Seror R, Mahr A, Mouthon L, Le Toumelin P (2011) The Five-Factor Score revisited: assessment of prognoses of systemic necrotizing vasculitides based on the French Vasculitis Study Group (FVSG) cohort. Medicine 90:19–27
Wolf J, Schmitt V, Palm F, Grau AJ, Bergner R (2013) Peripheral neuropathy as initial manifestation of primary systemic vasculitides. J Neurol 260:1061–1070
Moosig F, Bremer JP, Hellmich B, Holle JU, Holl-Ulrich K, Laudien M et al (2013) A vasculitis centre based management strategy leads to improved outcome in eosinophilic granulomatosis and polyangiitis (Churg-Strauss, EGPA): monocentric experiences in 150 patients. Ann Rheum Dis 72:1011–1017
Oka N, Kawasaki T, Matsui M, Shigematsu K, Unuma T, Sugiyama H (2011) Two subtypes of Churg-Strauss syndrome with neuropathy: the roles of eosinophils and ANCA. Mod Rheumatol 21:290–295
Sable-Fourtassou R, Cohen P, Mahr A, Pagnoux C, Mouthon L, Jayne D et al (2005) Antineutrophil cytoplasmic antibodies and the Churg-Strauss syndrome. Ann Intern Med 143:632–638
Cattaneo L, Chierici E, Pavone L, Grasselli C, Manganelli P, Buzio C et al (2007) Peripheral neuropathy in Wegener’s granulomatosis, Churg-Strauss syndrome and microscopic polyangiitis. J Neurol Neurosurg Psychiatry 78:1119–1123
Cisternas M, Soto L, Jacobelli S, Marinovic MA, Vargas A, Sobarzo E et al (2005) Clinical features of Wegener granulomatosis and microscopic polyangiitis in Chilean patients. Rev Med Chil 133:273–278
Suppiah R, Hadden RD, Batra R, Arden NK, Collins MP, Guillevin L et al (2011) Peripheral neuropathy in ANCA-associated vasculitis: outcomes from the European Vasculitis Study Group trials. Rheumatology (Oxford) 50:2214–2222
Schonermarck U, Lamprecht P, Csernok E, Gross WL (2001) Prevalence and spectrum of rheumatic diseases associated with proteinase 3-antineutrophil cytoplasmic antibodies (ANCA) and myeloperoxidase-ANCA. Rheumatology (Oxford) 40:178–184
Agard C, Mouthon L, Mahr A, Guillevin L (2003) Microscopic polyangiitis and polyarteritis nodosa: how and when do they start? Arthritis Rheum 49:709–715
Ribi C, Cohen P, Pagnoux C, Mahr A, Arene JP, Puechal X et al (2010) Treatment of polyarteritis nodosa and microscopic polyangiitis without poor-prognosis factors: a prospective randomized study of one hundred twenty-four patients. Arthritis Rheum 62:1186–1197
Beyer G, Schwaiger T, Lerch MM, Mayerle J (2014) IgG4-related disease: a new kid on the block or an old aquaintance? United Eur Gastroenterol J 2:165–172
Pieringer H, Parzer I, Wohrer A, Reis P, Oppl B, Zwerina J (2014) IgG4- related disease: an orphan disease with many faces. Orphanet J Rare Dis 9:110
Perez Alamino R, Martinez C, Espinoza LR (2013) IgG4-associated vasculitis. Curr Rheumatol Rep 15:348
Ohyama K, Koike H, Takahashi M, Kawagashira Y, Iijima M, Watanabe H et al (2015) Immunoglobulin G4-related pathologic features in inflammatory neuropathies. Neurology 85:1400–1407
Jasmin R, Sockalingam S, Ramanaidu LP, Goh KJ (2015) Clinical and electrophysiological characteristics of symmetric polyneuropathy in a cohort of systemic lupus erythematosus patients. Lupus 24:248–255
Oomatia A, Fang H, Petri M, Birnbaum J (2014) Peripheral neuropathies in systemic lupus erythematosus: clinical features, disease associations, and immunologic characteristics evaluated over a twenty-five-year study period. Arthritis Rheumatol 66:1000–1009
Tekatas A, Koca SS, Tekatas DD, Aksu F, Dogru Y, Pamuk ON (2014) R-R interval variation and sympathetic skin response in systemic lupus erythematosus. Clin Rheumatol 33:65–70
Collins MP, Periquet MI (2008) Isolated vasculitis of the peripheral nervous system. Clin Exp Rheumatol 26:S118–S130
Di Ciaula A, Covelli M, Berardino M, Wang DQ, Lapadula G, Palasciano G et al (2008) Gastrointestinal symptoms and motility disorders in patients with systemic scleroderma. BMC Gastroenterol 8:7
Kyriakidis NC, Kapsogeorgou EK, Tzioufas AG (2014) A comprehensive review of autoantibodies in primary Sjogren’s syndrome: clinical phenotypes and regulatory mechanisms. J Autoimmun 51:67–74
Sumida T, Tsuboi H, Iizuka M, Hirota T, Asashima H, Matsumoto I (2014) The role of M3 muscarinic acetylcholine receptor reactive T cells in Sjogren’s syndrome: a critical review. J Autoimmun 51:44–50
Morgen K, McFarland HF, Pillemer SR (2004) Central nervous system disease in primary Sjogrens syndrome: the role of magnetic resonance imaging. Semin Arthritis Rheum 34:623–630
Birnbaum J (2010) Peripheral nervous system manifestations of Sjogren syndrome: clinical patterns, diagnostic paradigms, etiopathogenesis, and therapeutic strategies. Neurologist 16:287–297
Schaublin GA, Michet CJ Jr, Dyck PJ, Burns TM (2005) An update on the classification and treatment of vasculitic neuropathy. Lancet Neurol 4:853–865
Blaes F (2012) Paraneoplastic neurological syndromes–diagnosis and management. Curr Pharm Des 18:4518–4525
Johnson PC, Rolak LA, Hamilton RH, Laguna JF (1979) Paraneoplastic vasculitis of nerve: a remote effect of cancer. Ann Neurol 5:437–444
Torvik A, Berntzen AE (1968) Necrotizing vasculitis without visceral involvement. Postmortem examination of three cases with affection of skeletal muscles and peripheral nerves. Acta Med Scand 184:69–77
Oh SJ (1997) Paraneoplastic vasculitis of the peripheral nervous system. Neurol Clin 15:849–863
Tschernatsch M, Stolz E, Strittmatter M, Kaps M, Blaes F (2005) Antinuclear antibodies define a subgroup of paraneoplastic neuropathies: clinical and immunological data. J Neurol Neurosurg Psychiatry 76:1702–1706
De Vita S, Soldano F, Isola M, Monti G, Gabrielli A, Tzioufas A et al (2011) Preliminary classification criteria for the cryoglobulinaemic vasculitis. Ann Rheum Dis 70:1183–1190
Ferri C (2008) Mixed cryoglobulinemia. Orphanet J Rare Dis 3:25
Ramos-Casals M, Stone JH, Cid MC, Bosch X (2012) The cryoglobulinaemias. Lancet 379:348–360
Gemignani F, Brindani F, Alfieri S, Giuberti T, Allegri I, Ferrari C et al (2005) Clinical spectrum of cryoglobulinaemic neuropathy. J Neurol Neurosurg Psychiatry 76:1410–1414
Taieb G, Maisonobe T, Musset L, Cacoub P, Leger JM, Bouche P (2010) Cryoglobulinemic peripheral neuropathy in hepatitis C virus infection: clinical and anatomical correlations of 22 cases. Rev Neurol 166:509–514
Ammendola A, Sampaolo S, Ambrosone L, Ammendola E, Ciccone G, Migliaresi S et al (2005) Peripheral neuropathy in hepatitis-related mixed cryoglobulinemia: electrophysiologic follow-up study. Muscle Nerve 31:382–385
Ciompi ML, Marini D, Siciliano G, Melchiorre D, Bazzichi L, Sartucci F et al (1996) Cryoglobulinemic peripheral neuropathy: neurophysiologic evaluation in twenty-two patients. Biomed Pharmacother 50:329–336
Valli G, De Vecchi A, Gaddi L, Nobile-Orazio E, Tarantino A, Barbieri S (1989) Peripheral nervous system involvement in essential cryoglobulinemia and nephropathy. Clin Exp Rheumatol 7:479–483
Cacoub P, Maisonobe T, Thibault V, Gatel A, Servan J, Musset L et al (2001) Systemic vasculitis in patients with hepatitis C. J Rheumatol 28:109–118
Marques IB, Giovannoni G, Marta M (2014) Mononeuritis multiplex as the first presentation of refractory sarcoidosis responsive to etanercept. BMC Neurol 14:237
Saito H, Yamaguchi T, Adachi Y, Yamashita T, Wakai Y, Saito K et al (2015) Neurological symptoms of Sarcoidosis-induced small fiber neuropathy effectively relieved with high-dose steroid pulse therapy. Intern Med 54:1281–1286
Singhal NS, Irodenko VS, Margeta M, Layzer RB (2015) Sarcoid polyneuropathy masquerading as chronic inflammatory demyelinating polyneuropathy. Muscle Nerve 52:664–668
Vital A, Lagueny A, Ferrer X, Louiset P, Canron MH, Vital C (2008) Sarcoid neuropathy: clinico-pathological study of 4 new cases and review of the literature. Clin Neuropathol 27:96–105
Kararizou E, Davaki P, Speggos K, Stamboulis E (2012) Rare association of polyneuropathy and Crohn’s disease: a clinicopathological study of 4 cases. Pol J path 63:261–266
Noel N, Drier A, Wechsler B, Piette JC, De Paz R, Dormont D et al (2014) Neurological manifestations of Behcet’s disease. La Revue de medecine interne/fondee par la Societe nationale francaise de medecine interne 35:112–120
Johnson RM, Barbarini G, Barbaro G (2003) Kawasaki-like syndromes and other vasculitic syndromes in HIV-infected patients. AIDS 17(Suppl 1):S77–S82
Roullet E, Assuerus V, Gozlan J, Ropert A, Said G, Baudrimont M et al (1994) Cytomegalovirus multifocal neuropathy in AIDS: analysis of 15 consecutive cases. Neurology 44:2174–2182
Said G, Lacroix C (2005) Primary and secondary vasculitic neuropathy. J Neurol 252:633–641
Baratta JM, Dyck PJ, Brand P, Thaisetthawatkul P, Dyck PJ, Engelstad JK et al (2016) Vasculitic neuropathy following exposure to minocycline. Neurol Neuroimmunol Neuroinflamm 3:e180
Thaisetthawatkul P, Sundell R, Robertson CE, Dyck PJ (2011) Vasculitic neuropathy associated with minocycline use. J Clin Neuromuscul Dis 12:231–234
Schapira D, Balbir-Gurman A, Nahir AM (2000) Naproxen-induced leukocytoclastic vasculitis. Clin Rheumatol 19:242–244
Vrancken AF, Said G (2013) Vasculitic neuropathy. Handb Clin Neurol 115:463–483
Cassereau J, Baguenier-Desormeaux C, Letournel F, Lavigne C, Leclech C, Dubas F et al (2012) Necrotizing vasculitis revealed in a case of multiple mononeuropathy after a 14-year course of spontaneous remissions and relapses. Clin Neurol Neurosurg 114:290–293
Collins MP, Periquet MI, Mendell JR, Sahenk Z, Nagaraja HN, Kissel JT (2003) Nonsystemic vasculitic neuropathy: insights from a clinical cohort. Neurology 61:623–630
Uceyler N, Geng A, Reiners K, Toyka KV, Sommer C (2015) Non-systemic vasculitic neuropathy: single-center follow-up of 60 patients. J Neurol 262:2092–2100
Collins MP (2012) The vasculitic neuropathies: an update. Curr Opin Neurol 25:573–585
Massie R, Mauermann ML, Staff NP, Amrami KK, Mandrekar JN, Dyck PJ et al (2012) Diabetic cervical radiculoplexus neuropathy: a distinct syndrome expanding the spectrum of diabetic radiculoplexus neuropathies. Brain 135:3074–3088
Garces-Sanchez M, Laughlin RS, Dyck PJ, Engelstad JK, Norell JE, Dyck PJ (2011) Painless diabetic motor neuropathy: a variant of diabetic lumbosacral radiculoplexus Neuropathy? Ann Neurol 69:1043–1054
Dyck PJ, Norell JE, Dyck PJ (1999) Microvasculitis and ischemia in diabetic lumbosacral radiculoplexus neuropathy. Neurology 53:2113–2121
Blaes F (2015) Diagnosis and therapeutic options for peripheral vasculitic neuropathy. Ther Adv Musculoskelet Dis 7:45–55
Levy Y, Uziel Y, Zandman GG, Amital H, Sherer Y, Langevitz P et al (2003) Intravenous immunoglobulins in peripheral neuropathy associated with vasculitis. Ann Rheum Dis 62:1221–1223
Geltner D (1981) The place of plasmapheresis in immune complex disease. Harefuah 101:77–78
Geltner D, Kohn RW, Gorevic P, Franklin EC (1981) The effect of combination therapy (steroids, immunosuppressives, and plasmapheresis) on 5 mixed cryoglobulinemia patients with renal, neurologic, and vascular involvement. Arthritis Rheum 24:1121–1127
Monti G, Saccardo F (2007) Emergency in cryoglobulinemic syndrome: what to do? Dig Liver Dis 39(Suppl 1):S112–S115
Stone JH, Merkel PA, Spiera R, Seo P, Langford CA, Hoffman GS et al (2010) Rituximab versus cyclophosphamide for ANCA-associated vasculitis. N Engl J Med 363:221–232
Metzler C, Miehle N, Manger K, Iking-Konert C, de Groot K, Hellmich B et al (2007) Elevated relapse rate under oral methotrexate versus leflunomide for maintenance of remission in Wegener’s granulomatosis. Rheumatology (Oxford) 46:1087–1091
Silva F, Specks U, Kalra S, Hogan MC, Leung N, Sethi S et al (2010) Mycophenolate mofetil for induction and maintenance of remission in microscopic polyangiitis with mild to moderate renal involvement–a prospective, open-label pilot trial. Clin J Am Soc Nephrol 5:445–453
Maneiro JR, Lopez-Canoa N, Salgado E, Gomez-Reino JJ (2014) Maintenance therapy of lupus nephritis with mycophenolate or azathioprine: systematic review and meta-analysis. Rheumatology (Oxford) 53:834–838
De Vita S, Quartuccio L, Isola M, Mazzaro C, Scaini P, Lenzi M et al (2012) A randomized controlled trial of rituximab for the treatment of severe cryoglobulinemic vasculitis. Arthritis Rheum 64:843–853
Ferri C, Marzo E, Longombardo G, Lombardini F, La Civita L, Vanacore R et al (1993) Interferon-alpha in mixed cryoglobulinemia patients: a randomized, crossover-controlled trial. Blood 81:1132–1136
Rieu V, Cohen P, Andre MH, Mouthon L, Godmer P, Jarrousse B et al (2002) Characteristics and outcome of 49 patients with symptomatic cryoglobulinaemia. Rheumatology (Oxford) 41:290–300
Boonyapisit K, Katirji B (2002) Severe exacerbation of hepatitis C-associated vasculitic neuropathy following treatment with interferon alpha: a case report and literature review. Muscle Nerve 25:909–913
Stubgen JP (2009) Interferon alpha and neuromuscular disorders. J Neuroimmunol 207:3–17
Ferri C, Cacoub P, Mazzaro C, Roccatello D, Scaini P, Sebastiani M et al (2011) Treatment with rituximab in patients with mixed cryoglobulinemia syndrome: results of multicenter cohort study and review of the literature. Autoimmun Rev 11:48–55
Dammacco F, Tucci FA, Lauletta G, Gatti P, De Re V, Conteduca V et al (2010) Pegylated interferon-alpha, ribavirin, and rituximab combined therapy of hepatitis C virus-related mixed cryoglobulinemia: a long-term study. Blood 116:343–353
Chia L, Fernandez A, Lacroix C, Adams D, Plante V, Said G (1996) Contribution of nerve biopsy findings to the diagnosis of disabling neuropathy in the elderly. A retrospective review of 100 consecutive patients. Brain 119(Pt 4):1091–1098
Koike H, Sobue G (2013) Clinicopathological features of neuropathy in anti-neutrophil cytoplasmic antibody-associated vasculitis. Clin Exp Nephrol 17:683–685
Ohyama K, Koike H, Masuda M, Sone J, Hashimoto R, Tomita M et al (2013) Autonomic manifestations in acute sensory ataxic neuropathy: a case report. Auton Neurosci 179:155–158
de Souza FH, Radu Halpern AS, Valente Barbas CS, Shinjo SK (2010) Wegener’s granulomatosis: experience from a Brazilian tertiary center. Clin Rheumatol 29:855–860
Cacoub P, Saadoun D (2008) Hepatitis C virus infection induced vasculitis. Clin Rev Allergy Immunol 35:30–39
Servioli L, Perez C, Consani S, Suarez A, Sehabiaga G, Collazo C et al (2007) Prevalence and characteristics of immunomediated neuropathies in a group of patients with autoimmune diseases. J Clin Neuromuscul Dis 9:285–290
Agarwal V, Singh R, Wiclaf CS, Tahlan A, Ahuja CK et al (2008) A clinical, electrophysiological, and pathological study of neuropathy in rheumatoid arthritis. Clin Rheumatol 27:841–844
Voskuyl AE, Hazes JM, Zwinderman AH, Paleolog EM, van der Meer FJ, Daha MR et al (2003) Diagnostic strategy for the assessment of rheumatoid vasculitis. Ann Rheum Dis 62:407–413
Delalande S, de Seze J, Fauchais AL, Hachulla E, Stojkovic T, Ferriby D et al (2004) Neurologic manifestations in primary Sjogren syndrome: a study of 82 patients. Medicine 83:280–291
Terrier B, Lacroix C, Guillevin L, Hatron PY, Dhote R, Maillot F et al (2007) Diagnostic and prognostic relevance of neuromuscular biopsy in primary Sjogren’s syndrome-related neuropathy. Arthritis Rheum 57:1520–1529
Dyck PJ, Hunder GG, Dyck PJ (1997) A case-control and nerve biopsy study of CREST multiple mononeuropathy. Neurology 49:1641–1645
Oh SJ, Slaughter R, Harrell L (1991) Paraneoplastic vasculitic neuropathy: a treatable neuropathy. Muscle Nerve 14:152–156
Kermani TA, Ham EK, Camilleri MJ, Warrington KJ (2012) Polyarteritis nodosa-like vasculitis in association with minocycline use: a single-center case series. Semin Arthritis Rheum 42:213–221
Ogawa N, Kawai H, Yamakawa I, Sanada M, Sugimoto T, Maeda K (2010) Case of minocycline-induced vasculitic neuropathy. Rinsho Shinkeigaku 50:301–305
Pary LF, Henszel A, Kelkar P (2004) Vasculitic mononeuritis multiplex induced by valacyclovir. Neurology 62:1906–1907
Manousakis G, Koch J, Sommerville RB, El-Dokla A, Harms MB, Al-Lozi MT et al (2013) Multifocal radiculoneuropathy during ipilimumab treatment of melanoma. Muscle Nerve 48:440–444
Mauermann ML, Blumenreich MS, Dispenzieri A, Staff NP (2012) A case of peripheral nerve microvasculitis associated with multiple myeloma and bortezomib treatment. Muscle Nerve 46:970–977
Mauermann ML, Ryan ML, Moon JS, Klein CJ (2007) Case of mononeuritis multiplex onset with rituximab therapy for Waldenstrom’s macroglobulinemia. J Neurol Sci 260:240–243
Frigui M, Kechaou M, Haddouk S, Masmoudi A, Kaddour N, Masmoudi H et al (2008) Benzylthiouracil induced ANCA-positive vasculitis: study of three cases and review of the literature. Ann Endocrinol (Paris) 69:517–522
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Blaes, F. (2016). Diagnosis and Therapy for Peripheral Vasculitic Neuropathy. In: Dammacco, F., Ribatti, D., Vacca, A. (eds) Systemic Vasculitides: Current Status and Perspectives. Springer, Cham. https://doi.org/10.1007/978-3-319-40136-2_23
Download citation
DOI: https://doi.org/10.1007/978-3-319-40136-2_23
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-40134-8
Online ISBN: 978-3-319-40136-2
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)