
Abstract
Epidemiological cohort studies have shown that the long-term exposure to PM2.5 is associated with increased mortality from cardiorespiratory diseases and lung cancer. We use an atmospheric chemistry-general circulation model in combination with population data, country-level health statistics and pollution exposure response functions to investigate the link between premature mortality and several emission source categories, combining all aerosol types that contribute to PM2.5. We estimate the global premature mortality by PM2.5 at 3.15 million/year in 2010. We find that high emissions levels mainly from residential energy use have the largest impact on premature mortality in Eastern and Southeastern Asia (almost 70 % of the global), with China and India being the counties with higher mortality levels attributable. For Europe we estimate 375 thousand premature deaths (about 11 % of the global rate), and 274 thousand deaths for the Eastern Mediterranean region in 2010. In this work we assume that all particles are equally toxic.
Access provided by CONRICYT-eBooks. Download conference paper PDF
Similar content being viewed by others
Keywords
- Chronic Obstructive Pulmonary Disease
- Premature Mortality
- Eastern Mediterranean Region
- Acute Lower Respiration Infection
- Exposure Response
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Air pollution is the largest contributor to the burden of disease from the environment. The World Health Organization (WHO) reported that in 2012 outdoor air pollution was responsible for the deaths of 3.7 million people (WHO 2009). The WHO also emphasizes that indoor and outdoor air pollution combined are among the largest health risk worldwide, both being of similar magnitude. Epidemiological studies have linked exposure to PM2.5 pollution with several health problems, including premature mortality from cardiovascular, respiratory diseases and lung cancer, non-fatal heart and lung disorders and acute asthma. Fine particles can cause health impacts even at very low concentrations. Estimates of mortality attributable to outdoor air pollution and the subsequent overall costs to the society are useful to justify air quality control policies and help improve public health.
2 Data and Methodology
For this work we applied model calculated global PM2.5 concentrations, population data, country-level baseline mortality rates and exposure response functions to a health impact function, to estimate premature mortality attributable to long-term exposure to PM2.5. We follow the same methodology as the Global Burden of Disease for 2010 (Lim et al. 2012) applying improved exposure response functions that more realistically account for health effects at very high PM2.5 concentrations.
2.1 Data
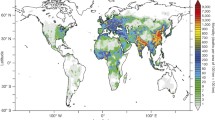
Model and emissions: We used the EMAC global atmospheric chemistry—general circulation model to simulate annual mean PM2.5 concentrations. EMAC comprise sub-models that represent tropospheric and lower stratospheric processes and their interaction with oceans, land and human influences. The model has been extensively validated and the output has been tested against in situ and remote sensing observations (De Meij et al. 2012; Jöckel et al. 2006; Pozzer et al. 2012a, b, 2015; Pringle et al. 2010). We obtained results for the year 2010, applying monthly varying emissions from EDGAR—the Emission Database for Global Atmospheric Research (Pozzer et al. 2012a).
Population data: The population data were obtained from the NASA Socioeconomic Data and Applications Center (SEDAC), hosted by the Columbia University Center for International Earth Science Information Network (CIESIN), available at a resolution of 2.5 × 2.5 arc minutes (about 5 × 5 km2) (http://sedac.ciesin.columbia.edu/), and projections by United Nations Department of Economic and Social Affairs/Population Division (UNDES 2011).
Mortality data: Baseline mortality data describe the number of deaths in a particular year for the population under consideration. These data were obtained from the World Health Organization (WHO) Statistical Information System on the country-level (WHO 2014), based on the International Classification of Diseases 10th Revision (ICD-10) classification system.
2.2 Methodology
We apply the following health impact function to estimate premature mortality related to PM2.5:
where yo is the baseline mortality rate (Giannadaki et al. 2014; Lelieveld et al. 2013, 2015) and Pop is the exposed population. AF is the fraction of the disease burden attributable to the risk factor (here PM2.5). RR is the relative risk of certain health impacts of the population exposed to outdoor PM2.5 air pollution. To estimate the global burden of disease attributable to PM2.5 we applied the integrated health risk function (Eq. 3) from Burnett et al. (2014), also used by Lim et al. (2012) for the GBD in 2010.
We refer to Burnett et al. (2014), Giannadaki et al. (2014) and Lelieveld et al. (2015) for details on the exposure response models and uncertainties. X is the annual mean PM2.5 concentration in 2010 and Xo is the background concentration below which no impact is assumed. We used mortality data from the World Health Organization (WHO 2014) for ischemic heart disease (IHD), cerebrovascular disease (CEV), chronic obstructive pulmonary disease (COPD), and lung cancer (LC) for the population above 30 year, and for acute lower respiration infection (ALRI) for children below 5 year.
3 Results
We apply the exposure response model (Eq. 1–3), to estimate the global, regional and country level premature mortality related to the long-term exposure to PM2.5. We consider six regions worldwide, as defined by the WHO (WHO member states by region and mortality stratum, http://www.who.int/choice/demography/mortality_strata/en/).
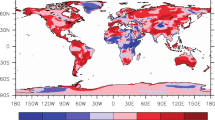
We estimated the global burden of PM2.5 related mortality at 3.15 million per year in 2010. The countries with the highest number of deaths are China (1.33 million), India (575 thousand) and Pakistan (105 thousand). In total counties in Eastern and Southeastern Asia contribute about 70 % to the global level. For Europe we estimated 375 thousand premature deaths (about 12 % of the global level) with Russia ranking first with 67 thousand, followed by Ukraine with 51 thousand. For European Union we estimated 173 thousand premature deaths, which contribute about 5 % to the global level, and 46 to the European toll. Apart from the most evident regions of East and Southeast Asia, where large populations are exposed to high levels of air pollution, Eastern Mediterranean, a region strongly affected from air pollution transport from surrounding areas, is considered a hot spot with high risk to health due to increasing levels of ambient PM2.5. We estimate for Eastern Mediterranean region 274 thousand premature deaths related to PM2.5 (about 9 % of the global). For the above estimations we assume that all particles from different sources and different composition are equally toxic. Figures 1 and 2 highlight the hot spot locations in red with high rates of premature mortality due to PM2.5 in Europe and Eastern Mediterranean respectively in 2010. Table 1 summarizes the mortality attributable to long-term exposure to PM2.5 for the six WHO regions.

PM2.5 related mortality (in deaths/area of 100 × 100 km2) in Europe in 2010

PM2.5 related mortality (in deaths/area of 100 × 100 km2) in Eastern Mediterranean in 2010
4 Conclusions
We estimated the global PM2.5 related premature mortality in 2010 at 3.15 million with China having the higher burden, followed by India and Pakistan. In Europe the toll of premature deaths is estimated at 375 thousand, and 173 thousand in the European Union. In the sensitive region of Eastern Mediterranean our estimates give a toll of 274 thousand deaths. Our results show the urgent need to reduce air pollution levels though strict emission controls, to improve air quality and public health. This effort requires a better understanding of the relative toxicity of particles from various emissions sources. In addition, there is a strong need for developing better emission inventories and monitoring systems, especially in regions with high air pollution burden.
References
Burnett RT, Pope CA III, Ezzati M, Olives C, Lim SM, Mentha S, Shin HH, Singh G, Hubbell B, Brauer M, Anderson HR, Smith KR, Kan H, Laden F, Prüss-Ustün A, Turner MC, Thun M, Cohen A (2014) An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ Health Perspect 122:397–403. doi:10.1289/ehp.1307049
CIESIN (Columbia University Center for International Earth Science Information Network) (2012) NASA socioeconomic data and applications center (SEDAC). http://sedac.ciesin.columbia.edu/
De Meij A, Pozzer A, Pringle KJ, Tost H, Lelieveld J (2012) EMAC model evaluation and analysis of atmospheric aerosol properties and distribution. Atmos Res 114–115:38–69
Giannadaki D, Pozzer A, Lelieveld J (2014) Modeled global effects of airborne desert dust on air quality and premature mortality. Atmos Chem Phys 14:957–968
Jöckel P, Tost H, Pozzer A, Brühl Ch, Buchholz J, Ganzeveld L, Hoor P, Kerkweg A, Lawrence MG, Sander R, Steil B, Stiller G, Tanarhte M, Taraborelli D, van Aardenne J, Lelieveld J (2006) The atmospheric chemistry general circulation model ECHAM5/MESSy: consistent simulation of ozone from the surface to the mesosphere. Atmos Chem Phys 6:5067–5104
Lelieveld J, Barlas C, Giannadaki D, Pozzer A (2013) Model calculated global, regional and megacity premature mortality due to air pollution by ozone and fine particulate matter. Atmos Chem Phys 13:7023–7037
Lelieveld J, Evans JS, Fnais M, Giannadaki D, Pozzer A (2015) The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature 525:367–371
Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K et al (2012) A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the global burden of disease study 2010. Lancet 380:2224–2260
Pozzer A, de Meij A, Pringle KJ, Tost H, Doering UM, van Aardenne J, Lelieveld J (2012a) Distributions and regional budgets of aerosols and their precursors simulated with the EMAC chemistry-climate model. Atmos Chem Phys 12:961–987. doi:10.5194/acp-12-961-2012
Pozzer A, Zimmermann P, Doering UM, van Aardenne J, Tost H, Dentener F, Janssens-Maenhout G, Lelieveld J (2012b) Effects of business-as-usual anthropogenic emissions on air quality. Atmos Chem Phys 12:6915–6937. doi:10.5194/acp-12-6915-2012
Pozzer A, de Meij A, Yoon J, Tost H, Georgoulias AK, Astitha M (2015) AOD trends during 2001–2010 from observations and model simulations. Atmos Chem Phys 15:5521–5535. doi:10.5194/acp-15-5521-2015
Pringle KJ, Tost H, Message S, Steil B, Giannadaki D, Nenes A, Fountoukis C, Stier P, Vignati E, Lelieveld J (2010) Description and evaluation of GMXe: a new aerosol submodel for global simulations (v1). Geosci Model Dev 3:391–412
United Nations Department of Economic and Social Affairs (UNDES) (2011) Population division: world population prospects: the 2010 revision, (Population data files of the UNDES. We accessed the 28 June 2011 update in November 2012, available at: http://esa.un.org/unpd/wpp)
WHO (Word Health Organization) (2009) Global health risks: mortality and burden of disease attributable to selected major risks. WHO, Geneva
WHO (World Health Organization) (2014) World health organization statistical information system (WHOSIS), detailed data files of the WHO mortality database. http://www.who.int/whosis/mort/download/en/index.html
Acknowledgments
We are grateful to J.S. Evans from the Department of Environmental Health—Harvard Chan School of Public Health for his valuable help for this work. The research leading to these results has received funding from the European Research Council under the European Union’s Seventh Framework Programme (FP7/2007-2013)/ERC grant agreement No. 226 144.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this paper
Cite this paper
Giannadaki, D., Lelieveld, J., Pozzer, A. (2017). The Impact of Fine Particulate Outdoor Air Pollution to Premature Mortality. In: Karacostas, T., Bais, A., Nastos, P. (eds) Perspectives on Atmospheric Sciences. Springer Atmospheric Sciences. Springer, Cham. https://doi.org/10.1007/978-3-319-35095-0_146
Download citation
DOI: https://doi.org/10.1007/978-3-319-35095-0_146
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-35094-3
Online ISBN: 978-3-319-35095-0
eBook Packages: Earth and Environmental ScienceEarth and Environmental Science (R0)