
Abstract
T lymphocytes play a central role in immune homeostasis and modulation of intestinal inflammation. Various subsets of CD4+ T cells, including effector and regulatory T cells, are generated locally and function in the intestinal mucosa. Effector T cells, which mediate inflammation, can be classified by unique cytokine expression signatures. Crohn’s disease (CD) has been associated with Th1 and Th17 cytokine secretion, whereas Th2 cytokines have been associated in ulcerative colitis. However, not all T cells are pathogenic; some normally function to suppress immune responses through diverse mechanisms including the secretion of anti-inflammatory cytokines. Naturally occurring regulatory T cells develop in the thymus whereas those that are generated in the periphery or in vitro are called “inducible” regulatory T cells, which can be further categorized by the cytokines they secrete and the specific methods by which they have been generated. In murine models, a qualitative or quantitative defect in regulatory T cells can lead to colitis development, but there does not appear to be an obvious defect in regulatory T cell number or function in inflammatory bowel diseases. Effector and regulatory T cell localization (homing) to mucosal tissues is facilitated by the expression of unique combinations of specific cell surface molecules. Therapies preventing T cell homing to the gut have been found effective for both Crohn’s disease and ulcerative colitis. Understanding how T cells can mediate or prevent intestinal inflammation may lead to more effective treatments, such as those that may enhance regulatory T cell number and/or function.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- CD4+ T cells
- CD8+ T cells
- TCRγδ
- Regulatory T cells
- Effector T cells
- T cell plasticity
- Tr1 cells
- Th3 cells
- Th1 cells
- Th2 cells
- Th17 cells
- iTR35
- Inducible regulatory T cells
- iTregs
- Naturally occurring regulatory T cells
- nTregs
- NK-T cells
- Foxp3
- Scurfy mice
- IPEX
- IL-10
- TGF-β
- IL-35
- IL-5
- IL-13
- IL-17
- CCR9
- α4β7
- Natalizumab
- Vedolizumab
Introduction
The adaptive immune system plays a central role in the pathogenesis of inflammatory bowel disease (IBD). In a healthy state, both CD8+ and CD4+ subsets of T cells are present in the intestines in small numbers; the former are found mostly in the epithelial layer while the latter are located deeper in the lamina propria. In an inflammatory state, however, the number of CD4+ T cells is often vastly magnified. Early research efforts were largely centered on T lymphocytes given evidence that CD4+ T cells from colitic animals and human IBD patients expressed activation markers and produced pro-inflammatory cytokines [1–5] and adoptive transfer of CD4+ T cells from several animal models of colitis into immunodeficient mice could transfer disease [6–8]. While still controversial, it seems likely in most IBD patients that altered T cells are not the critical initiating signal driving inflammation, but rather are an essential mediator and propagator of disease resulting from aberrant innate immune function [1].
T lymphocytes are broadly classified as regulatory or effector T cells. The latter is crucial in the protective immune response against infections. In contrast, the function of regulatory T cells is to maintain mucosal homeostasis by limiting the immune response to pathogens and by disarming any self-reactive effector T cells that escape negative selection in the thymus. Both T cell subsets are present in the gut-associated lymphoid tissue. Thus, inflammation can result from an imbalance of the number and/or function of these two T cell arms of the homeostatic T cell equation. Most studies on the role of T lymphocytes in IBD pathogenesis have centered on the CD4+ T cell subset, which is the main focus of this chapter; however, other T cell subsets are briefly covered at the end of the chapter.
Effector T Cells
In the human gut, immune homeostasis requires exquisitely regulated responses to rare pathogens among a preponderance of seemingly harmless commensal microorganisms. Effector T cells are critical for protecting against intestinal pathogens and are broadly classified into Th1 , Th2 , or Th17 cells based on their cytokine secretion profile. Interferon-(γ)gamma and TNF-(α)alpha are the predominant cytokines produced by Th1 cells whereas Th2 cells produce interleukin (IL)-4, IL-5 , and/or IL-13 . Th17 cells secrete IL-17 , a phenotype that is perpetuated by IL-23. In a physiologic state, Th1 and Th2 cytokines are necessary to restrain pathogens: Th2 cytokines are secreted in response to parasitic infections, whereas Th1 cytokines are secreted in response to the presence of intracellular bacteria and viruses. Th17 cell produced IL-17, on the other hand, plays a role in protection against pathogenic bacteria, viruses, and fungi, namely by recruitment of other immune subsets to mucosal sites [9, 10].
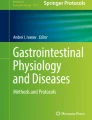
Inappropriately activated effector T cells can lead to pathology. Crohn’s disease was classically considered a Th1-associated disease [3, 5], but more recently, Crohn’s disease has been reclassified as a mixed Th1/17 disease as mucosal tissue from Crohn’s patients have been found to produce IL-17 in addition to TNF-(α)alpha and interferon-(γ)gamma [11]. Ulcerative colitis, on the other hand, has been described by some but not all studies to be a Th2-associated disease with elevated levels of IL-5 and IL-13 (but not the classic Th2 cytokine IL-4) detected in diseased mucosa [4, 11]. More recent studies, however, have reported detection of IL-17 in ulcerative colitis tissues [11]. A relatively new subset of T-helper cells, Th9 cells, defined by their secretion of interleukin-9, has been implicated in the pathogenesis of IBD [12–14]. Patients with active Crohn’s disease or ulcerative colitis have elevated numbers of CD4+PU.1+ and CD4+IRF4+ T cells in the intestinal mucosa compared to control patients [12, 13]. Interestingly, only ulcerative colitis patients showed elevated expression of IL-9 by these cells, and there was an association of IL-9 expression and IL-9+ T cells with the severity of the disease [12, 13]. Ulcerative colitis patients also showed elevated expression of IL-9R in intestinal epithelial cells [12, 13] and it has been proposed that Th9 cell-derived IL9 alters tight junction protein composition in the intestinal epithelium and thereby increases intestinal permeability leading to disease [12, 14]. The association of Crohn’s disease and ulcerative colitis with particular T helper cell subsets is summarized in Fig. 8.1. Please refer to Chaps. 15 and 16 on Th1 /2/17 cells and animal models of IBD, respectively, for further details.

Regulatory and Effector T cell populations controlling IBD. Various effector T cells (Th1, Th2, Th17, and Th9) are depicted and their cytokine secretion patterns as well as potential IBD disease associations. Regulatory T cells (nTregs and iTregs) can suppress effector T cell function employing diverse mechanisms including anti-inflammatory cytokine secretion (e.g., IL-10 , TGF-β, and IL-35 )
Regulatory T Cells
The proinflammatory capacity of effector cells is kept in balance by regulatory T cells. These cells are classically hypoproliferative, hyporesponsive, and potent in their suppressive capacity to inhibit proliferation and activation of non-regulatory T cell counterparts. Regulatory T cells are classically divided into at least two distinct populations (summarized in Fig. 8.1): naturally occurring regulatory T cells (nTregs) that are generated in the thymus and “induced” regulatory T cells (iTregs) that are generated in peripheral tissues or are generated in vitro in the presence of certain anti-inflammatory cytokines. Both populations are likely essential, with distinct and nonredundant functions in maintaining mucosal homeostasis [14–16].
Naturally Occurring Tregs
Easily detected in the peripheral blood and peripheral immune compartments, such as the spleen, lymph nodes, and the intestines, nTregs express Foxp3 , a member of the fork-head family of transcription factors that is crucial for their development and function. Scurfy mice , that have mutant FOXP3, are devoid of nTregs, die soon after birth from autoimmunity, a phenotype that can be rescued by transfer of regulatory T cells within a few days after birth [15]. Similarly, humans without functional Foxp3 develop immune dysregulation, polyendocrinopathy, enteropathy, X-linked (IPEX) syndrome and also suffer from multiple autoimmune manifestations, including enteropathy [17–19]. In addition to IPEX, other genetic deficiencies including mutations in WASP, CD25, and IL-10 all lead to abnormal Treg cell numbers and/or function, and are associated with increased risk of IBD [20, 21]. In the mouse, Foxp3 is a reliable marker of Tregs. However, in human cells, CD4+ T cells can transiently express low levels of Foxp3 when activated, thus, making Foxp3 an ambiguous marker of nTregs [22]. Some cell surface markers have been described, albeit inconsistently, to be expressed by nTregs, such as GITR, GARP, CD49d, ICOS, CD25, and CTLA-4 [23, 24]. Unfortunately, these cell surface markers are not specific to nTregs and, therefore, leave room for better markers for identification of nTregs. Liu et al. proposed a strategy to identify “pure” FOXP3+ Treg cells, devoid of activated T cells, by inclusion of the IL-7 receptor alpha chain (CD127) in their flow cytometry-based purification protocols. More specifically, low expression of CD127, in conjunction with CD25 expression, provides a useful strategy for the identification of a highly enriched FOXP3+ cells in humans [15, 25, 26].
Despite the fact that they make up only 5–10 % of the total CD4+ cell population, nTregs are critical in maintaining immunologic homeostasis. In the mouse, co-transfer of nTregs with CD45RBhi T cells into immunodeficient mice not only protect against colitis but can also reverse ongoing colitis [27, 28]. Transfer of nTregs into susceptible animals can also ameliorate other autoimmune diseases, such as experimental autoimmune encephalopathy (a model of multiple sclerosis), or nonobese diabetic (NOD) mice (a model of type I diabetes), or systemic lupus erythematosus [29–31]. Along the same line, mice depleted of CD25+ T cells, which consist mainly of nTregs, develop significant autoimmune diseases [32]. In the in vitro setting, nTregs can potently suppress proliferation of cocultured naïve T cells [23, 33].
Naturally occurring Tregs function partly through secretion of a multitude of anti-inflammatory cytokines, including IL-10 , TGFβ , and IL-35 [34]. Tregs deficient in TGFβ or WT Tregs transferred with neutralizing antibodies to TGFβ were not able to suppress disease in an adoptive cell transfer model of colitis [35, 36]. The data regarding IL-10 are not as clear; Tregs deficient in IL-10 or WT Tregs transferred with neutralizing antibodies to IL-10R are defective in colitis protection in some, but not all, settings [6, 37]. Moreover, deletion of IL-10 from Foxp3 + Treg leads to less severe intestinal inflammation compared to deletion in total CD4+ T cells , implicating CD4+ Foxp3− cells as a functional source of IL-10 that contributes to intestinal homeostasis [16, 38]. On the other hand, IL-35 , which is a heterodimer of Epstein-Barr-virus-induced gene 3 (EBI3) and IL-12α, appears crucial to the regulatory function of Tregs, since EBI3-deficient and IL-12α deficient Tregs lose their suppressive properties both in vitro and in vivo in a model of colitis [34, 39]. In addition to cytokine-mediated regulation, Tregs can also modulate antigen presenting cell and effector T cell function by alteration of cellular metabolism by surface expression of enzymes CD39 and CD73 that convert proinflammatory extracellular ATP into the immunosuppressive nucleoside adenosine [40, 41]. Whether or not all these regulatory mechanism are necessary for mucosal homeostasis in a normal mouse is not clear, but collectively they play important roles in the suppressive function of Tregs in different settings [16, 42].
Inducible Tregs
In addition to nTregs that are generated in the thymus, regulatory T cells can be “induced” in vivo outside of the thymus in peripheral lymphoid tissue under tolerogenic conditions. The majority of peripheral Foxp3 + cells in the spleen and lymph nodes are thymically established nTreg cells. In contrast, the inducible Tregs (iTregs) make up a large fraction of T cells in the lamina propria (LP) and gut-associated lymphoid tissue (GALT) of the intestine [15, 16, 43]. Observed by transferring Foxp3− cells from reporter animals into lymphopenic mice and identified by the induced expression of FoxP3, these iTregs were demonstrated to be as suppressive as nTregs in an in vitro suppression assay [44]. In addition, antigen administration at low dose can lead to oral tolerance, a condition of systemic and/or local immunological tolerance, through the generation of iTregs that secrete both TGF-β and IL-10 [45].
Similarly, iTregs can also be induced ex vivo in the cell culture system when naïve T cells are stimulated through the TCR in the presence of different anti-inflammatory cytokines . For example, Th3 cells can be generated in vivo by exposure to oral antigen at low dose or in vitro by stimulating naïve T cells in the presence of TGF-β, along with other cytokines. Tr1 cells result when naïve T cells are stimulated in the presence of IL-10 either in vitro or in vivo. Th3 cells secrete abundant amounts of TGF-β and have been described to express Foxp3 . Th3 cells can protect against colitis alone but also synergize with nTregs in an adoptive cell transfer model of colitis [46]. Tr1 cells, which secrete large amounts of IL-10 and some TGF-β but do not express Foxp3, also have been shown to prevent a similar model of colitis by adoptive cell transfer [47, 48]. Although Tr1 cells certainly can be generated in vitro from both human and murine naïve T cells [47], they can also be found in the GALT of normal mice [49] and have been detected in humans in the setting of transplantation, autoimmune diseases, and exposure to allergens (reviewed in ref. [50]). Recently Gagliani and colleagues identified the surface markers CD49b and lymphocyte activation gene 3 (LAG-3) as being co-expressed on mouse and human Tr1 cells [51]. The use of these markers makes it possible to track and purify Tr1 cells to explore there immune regulatory potential in cell based therapy.
Another Treg population, iTr35 cells , was identified that are generated in the setting of IL-35 stimulation [52]. Culture of either mouse or human CD4+ T cells with IL-35 leads to iTR35 cells, which are potent secretors of IL-35. These cells are highly effective suppressors of T cell proliferation in vitro and autoimmune diseases in vivo [52], as shown in both experimental models of multiple sclerosis and colitis [52]. Unlike other regulatory T cells, iTR35 cells appear stable and retain suppressive properties in vivo after transfer into recipient mice [52].
A new population of iTreg co-expressing FoxP3 and Rorγ was recently described by several groups in both mice and human [53, 54]. They comprise 40–60 % of colonic Tregs in inbreed mouse strains raised in specific pathogen free conditions; the frequency are much lower in germ-free settings. Microbial colonization of intestinal mucosa induces generation of these CD4+Helios−FoxP3+Rorγ+ Tregs. They also found that these cells protect from colonic inflammation in TNBS-induced colitis model [53].
Plasticity of T Cells
T cell differentiation was once considered linear and irreversible, but recent findings indicate that this process is flexible and committed cells can acquire features of different effector cells upon adequate stimuli [55]. Tregs co-expressing Foxp3 and IL-17 have been described at mucosal sites and Tregs can be induced to express IFN-γ potentially leading to tissue damage by certain microbial infections (reviewed in refs. [56, 57]). In fact, cells that were previously Tregs have been demonstrated to lose their Foxp3 expression, gain a memory T cell phenotype, produce inflammatory cytokines, and lead to diabetes in an adaptive cell transfer model [58]. Moreover, IL17 producing Treg cells were also identified in inflamed intestinal mucosa of patients with Crohn’s disease [59]. Similarly, trans-differentiation of Th17 cells into a regulatory Tr1 cells can occur during an immune response. Conversion of Th17 cells into Tr1 cells are promoted by activation of Ahr signaling in presence of TGF-β1 and contribute to the resolution of inflammation [60]. Previously it has been shown by the same group that anti-CD3 treatment leads to the generation of regulatory Th17 (rTh17) cell in the small intestine. rTh17 cells express high level of anti-inflammatory cytokine IL10 and suppressive capacity of these cells was dependent of the expression of IL10, TGF-β, and CTLA-4 [61]. Collectively, it can be concluded that both Treg and Th17 lymphocytes possess an intrinsic functional plasticity, which must be considered in attempts to target these cells therapeutically.
Less Conventional T Cell Subsets
In addition to CD4+ T cells , other T lymphocyte subsets have potential effector or regulatory properties. In the lamina propria, CD8+ cells possess regulatory function and have been noted to be decreased in IBD tissues compared to controls [62, 63]. Likewise, in the intraepithelial compartment, TCRαα+ CD8+ T cells have been shown to be protective in animal models of colitis using adoptive cell transfer [64, 65] whereas TCRγδ+ cells appear to limit the extent of injury and promote tissue healing in a chemically induced model of colitis [66]. However, others have demonstrated a potential pathogenic role of TCRγδ+ cells given absence of these cells in a transgenic colitis model leads to attenuated disease [67]. These findings may have implications for the pathogenesis of ulcerative colitis given higher frequency of these TCRγδ+ cells has been noted in colonic tissue from UC patients [67]. Another less common subset of T cell is NK-T cells , which express surface markers and possess certain functional properties typical of both NK cells and T cells. In addition to expressing components of the T cell receptor complex, CD3, they express semi-invariant CD1d-restricted αβ TCRs recognizing glycolipid antigens. Some regard these cells as potentially pathogenic in inflammatory bowel disease. In fact, Fuss et al. demonstrated circumstantial evidence for NK-T cells being the source of high IL-13 levels noted in samples from patients with active UC, suggestive of a pathogenic role of these cells [4]. Likewise, in the oxazolone-induced murine model of ulcerative colitis, depletion of NK-T cells led to protection against disease [68]. However, in a chemically induced model of colitis (with dextran sodium sulfate), NK-T cells have been demonstrated to possess a regulatory function [69]. A recent murine study showed that microbial exposure during early life leads to the generation of mucosal invariant (i)-NKT cell tolerance. In absence of such tolerogenic commensal exposure in germ-free mice leads to CXCL16-mediated iNKT cell driven intestinal inflammation in oxazolone-induced colitis model [70]. Although these less conventional T cell subsets typically have reduced frequencies when compared with the more conventional CD4+ T cells, their pathogenic/regulatory properties may contribute, at least in part, to overall mucosal homeostasis [70].
The Role of T Cells in Colitis
T cells have been long recognized to be central to the mucosal inflammatory process and thought early on to even be the instigator of disease given the marked expansion of activated CD4+ T cells in the lamina propria of both inflamed mouse and human intestinal tissues [1, 2, 10]. CD4+ T cells from intestinal samples isolated from Crohn’s disease and ulcerative colitis patients were found to be resistant to apoptosis [71], which may be one mechanism for such seemingly inadequately controlled expansion of T cells. The ability to transfer colitis by adoptively transferring CD4+ T cells from a colitic mouse to an immunodeficient host in many animal models also implicated the colitogenic potential of CD4+ T cells [6–8]. Even transfer of CD4+ T cells depleted of CD25+ regulatory T cells from normal animals could lead to disease in a lymphocyte-deficient host [27], demonstrating the pro-inflammatory nature of effector T cells and its usual tight regulation by regulatory T cells during homeostasis.
Similar to that seen in a variety of murine models of IBD, CD4+ T cells isolated from patients with Crohn’s disease or ulcerative colitis express large quantities of pro-inflammatory cytokines [3, 5, 11, 72]. Interferon-(γ)gamma , tumor necrosis factor-(α)alpha and IL-2 have been demonstrated repeatedly to be elevated in Crohn’s disease mucosa, whereas IL-5 and IL-13 have been associated with ulcerative colitis. Early studies demonstrating an abundance of Th1 type cytokines in Crohn’s disease suggested IFN-γ+ Th1 cells to be a major mediator of disease, while ulcerative colitis was suggested in some studies to be mediated primarily by excessive Th2 responses. Interestingly, despite an elevated level of IL-5 and IL-13 associated with ulcerative colitis, there is evidence of surprisingly reduced expression of IL4+ Th2 cells [3, 4, 10]. More recent reports demonstrating increased population of IL-5 and IL-13 expressing atypical natural killer T (NKT) cells in ulcerative colitis provided one explanation for this apparent anomaly [4, 10]. More recent studies have shown that tissues from both Crohn’s disease and ulcerative colitis patients have a massive infiltration of Th17 cells and Th17-related cytokines [10, 73, 74]. Apart from activating cellular targets like epithelium, endothelium, monocytes/macrophages, and neutrophils, IL-17 is known to induce proinflammatory cytokines (TNF-α, IL-1B, GM-CSF, G-CSF, IL-6), chemokines (CXCL8, CXCL9, CXCL10), and metalloproteases [74–76]. Interestingly, several signature cytokines involved in Th17 differentiation and expansion, including IL-23R, IL-12B, JAK2, STAT3, CCR6, and TNFSF15, have been identified as susceptibility genes of Crohn’s disease and ulcerative colitis in genome-wide association studies [77–79].
On the basis of the observations that IFNγ, IL-17 , IL-3 may play a key role in the pathogenesis of Crohn’s disease and ulcerative colitis, both in mouse models and in humans, these cytokines have been considered as potential targets for the treatment of IBD. However the outcome in several studies has not been met with much success. Several groups have studied the effect of humanized antibody against IFN-γ, fontolizumab, in patients with Crohn’s disease; however, the efficacy of anti-IFN-γ treatment remains unclear [80–82]. Blockade of IL-17 pathway was also not effective in Crohn’s disease: secukinumab , a fully humanized anti-IL-17A monoclonal antibody, failed to control symptoms and was associated with severe adverse effects [83]. Finally, two anti-IL-13 monoclonal antibodies , tralokinumab [84] and anrunkinzumab [85], recently failed in phase II clinical trials in ulcerative colitis patients [86]. The failure of these agents, which target adaptive immune responses, has led to some rethinking of the central role of these cytokines in the pathogenesis of both Crohn’s disease and ulcerative colitis.
Recent data has suggested that the initial aberrant signal may derive from defects in the innate immune system (such as an epithelial cell, macrophages, dendritic cells, NK cells, etc.). Polymorphisms in genes (e.g., NOD2, ATG16L1, and IRGM) that code for proteins important in recognizing and handling intracellular microbes, processes that occur in innate immune cells, have been recognized to be associated with Crohn’s disease risk in genome-wide association studies [87]. Data from animal studies have also implicated professional antigen presenting cells or epithelial cells in playing a more direct role in colitis induction [37, 88, 89]. Nonetheless, T cells are still thought to be an important mediator of disease, contributing to either the initiation or perpetuation of disease [1]. In this latter context, once activated by soluble factors and/or by cell–cell contact, T cells are able to expand and secrete chemokines and cytokines that recruit and activate, respectively, other immune cell subsets to perpetuate an inflammatory signal.
In order to damage the gut, effector T cells need to adhere and migrate into intestinal mucosa, a process which depends on the recognition between adhesion receptors (CCR9 and α4β7 ) expressed on the T cell surface and their ligands (MAdCAM-1 ) on the gut vascular endothelial surface [90]. CCR9 and α4β7 are the two most well characterized gut-homing receptors on T cells, and blocking the interaction between these receptors and their ligands on endothelial cells prevents T cells from entering the gut. This serves as the basis for the development of biologic therapies for Crohn’s disease such as natalizumab , which is a monoclonal antibody against the integrin α4, and vedolizumab , a monoclonal antibody against α4β7. Both agents interfere with T cell homing to the gut and consequently decrease inflammatory activities leading to clinical efficacy in both Crohn’s disease and ulcerative colitis [91–94]. Additional anti-adhesion molecule strategies including the anti-β7 antibody etrolizumab [95] and anti-MAdCAM-1 antibody targeting the α4β7 ligand [96] are currently being tested in IBD [97]. Moreover, a CCR9 chemokine receptor small-molecule antagonist targeting the CCR9-CCL25 interaction has recently failed in a large [96–98]. Other agents blocking such signals crucial to T cell gut homing are also under development.
One may also hypothesize that T cell suppression is diminished in IBD either from a qualitative or quantitative defect in Treg function. However, a defect in Treg numbers appears not to be a principal cause of IBD, since their proportions are noted to be increased in inflamed IBD tissue when compared to non-inflamed samples from IBD patients or samples from healthy control patients [99]. In fact, during periods of active disease, fewer Tregs are seen in the peripheral blood and more are found in the mucosa, suggesting an increase (through homing) or retention of Treg to sites of inflammation. Moreover, peripheral blood, mesenteric lymph node, and mucosal Tregs when removed from IBD patients retain in vitro suppressive function [99–101]. Thus, Tregs from IBD patients have the capacity for functional activity. However, the increase in Treg proportions in inflamed mucosa from IBD patients appear to be quantitatively less than that seen in non-IBD inflammatory control samples (those with diverticulitis), suggesting the increase in Treg numbers seen in IBD is not as robust as seen in other inflammatory disorders. Nonetheless, despite the presence of regulatory T cells in IBD associated mucosa these cells are not sufficient in situ to control inflammation.
Regulatory T Cells as Potential Therapy for IBD
Given the potent suppressive properties of regulatory T cells, one potential therapeutic option for IBD is quantitative enhancement of Treg numbers and/or functional capacity [21]. One theoretical approach is to isolate Tregs from a patient’s peripheral blood, followed by augmentation of cell function/numbers in vitro, and subsequent infusion of these cells into the patient. However, this idea has been hindered by difficulty in Treg expansion given their tendency for hypoproliferation, poorly defined surface markers, and uncertain stability and longevity in vivo. One potential way of overcoming these difficulties is to generate and expand inducible Tregs in vitro from naïve T cells, such as iTr35 cells , Tr1 cells , or regulatory CD8+ cells [47, 52, 63]. Even then, it is difficult to purify some of these populations due to the lack of specific cell surface markers. In addition, this technique will still require peripheral blood cell isolation; immediate processing or cryopreservation; in vitro culture and stimulation; vigorous testing for function, purity, and viability; and reinfusion of newly induced Tregs, posing technical challenges to avoid infection and maintain quality control. Recently Canavan and colleague have shown that Tregs can be expanded from the blood of patients with Crohn’s disease. They demonstrated that the expanded cells were epigenetically stable and home to human small bowel in a C.B-17 severe combined immune deficiency (SCID) xenotransplant model [102]. In a phase 1/2a study 40 % of the patients showed a clinical response after a single injection of ovalbumin-specific Treg cells in 20 Crohn’s disease patients [97, 103]. In this study autologous Treg cells were expanded in vitro, cloned by limiting dilution, and selected for IL-10 production in response to ovalbumin before transfer [15, 103]. An alternative option is to pharmacologically expand the already existing pool of Tregs or induction of an iTreg population. The latter could be done with an agent such as oral anti-CD3 antibody, which has been shown to expand a particular type of Tregs and has been shown to suppress EAE, SLE, and diabetes in mice [104, 105]. In another study Koreth et al. showed that daily administration of low-dose interleukin-2 in patients with active chronic GVHD that was refractory to glucocorticoid therapy was associated with preferential sustained Treg cell expansion in vivo and amelioration of the manifestations of chronic GVHD in a substantial proportion of patients [106]. Phase 1 studies investigating the role of oral OKT3 (anti-CD3) and low-dose IL2 have been initiated for ulcerative colitis (ClinicalTrials.gov: NCT02200445; ClinicalTrials.gov: NCT01287195). Taken together therapies targeting the immunomodulatory potential of Treg cells seem to be a promising approach for treatments of IBD.
Summary
T cells have been clearly implicated as a mediator and propagator of disease in many animal models of IBD. In patient samples, T cells secrete an abundance of pro-inflammatory cytokines suggesting a central role of T cells in the pathogenesis of disease. Despite the large body of knowledge regarding the role of T cells in mucosal homeostasis, much still remains to be understood with regard to how these T cell subsets interact with each other and with other immune cell subsets to lead to IBD and how these interactions can be repaired to restore intestinal homeostasis.
References
Maynard CL, Weaver CT. Intestinal effector T cells in health and disease. Immunity. 2009;31:389–400.
Elson CO, Cong Y, McCracken VJ, Dimmitt RA, Lorenz RG, Weaver CT. Experimental models of inflammatory bowel disease reveal innate, adaptive, and regulatory mechanisms of host dialogue with the microbiota. Immunol Rev. 2005;206:260–76.
Fuss IJ et al. Disparate CD4+ lamina propria (LP) lymphokine secretion profiles in inflammatory bowel disease. Crohn’s disease LP cells manifest increased secretion of IFN-gamma, whereas ulcerative colitis LP cells manifest increased secretion of IL-5. J Immunol. 1996;157:1261–70.
Fuss IJ et al. Nonclassical CD1d-restricted NK T cells that produce IL-13 characterize an atypical Th2 response in ulcerative colitis. J Clin Invest. 2004;113:1490–7. doi:10.1172/JCI19836.
MacDonald TT, Hutchings P, Choy MY, Murch S, Cooke A. Tumour necrosis factor-alpha and interferon-gamma production measured at the single cell level in normal and inflamed human intestine. Clin Exp Immunol. 1990;81:301–5.
Asseman C, Read S, Powrie F. Colitogenic Th1 cells are present in the antigen-experienced T cell pool in normal mice: control by CD4+ regulatory T cells and IL-10. J Immunol. 2003;171:971–8.
Wirtz S et al. Cutting edge: chronic intestinal inflammation in STAT-4 transgenic mice: characterization of disease and adoptive transfer by TNF- plus IFN-gamma-producing CD4+ T cells that respond to bacterial antigens. J Immunol. 1999;162:1884–8.
Nguyen DD et al. Lymphocyte-dependent and Th2 cytokine-associated colitis in mice deficient in Wiskott-Aldrich syndrome protein. Gastroenterology. 2007;133:1188–97. doi:S0016-5085(07)01311-X [pii].
Khader SA, Gaffen SL, Kolls JK. Th17 cells at the crossroads of innate and adaptive immunity against infectious diseases at the mucosa. Mucosal Immunol. 2009;2:403–11.
Shale M, Schiering C, Powrie F. CD4(+) T-cell subsets in intestinal inflammation. Immunol Rev. 2013;252:164–82. doi:10.1111/imr.12039.
Fujino S et al. Increased expression of interleukin 17 in inflammatory bowel disease. Gut. 2003;52:65–70.
Gerlach K et al. TH9 cells that express the transcription factor PU.1 drive T cell-mediated colitis via IL-9 receptor signaling in intestinal epithelial cells. Nat Immunol. 2014;15:676–86. doi:10.1038/ni.2920.
Nalleweg N et al. IL-9 and its receptor are predominantly involved in the pathogenesis of UC. Gut. 2015;64:743–55. doi:10.1136/gutjnl-2013-305947.
Kaplan MH, Hufford MM, Olson MR. The development and in vivo function of T helper 9 cells. Nat Rev Immunol. 2015;15:295–307. doi:10.1038/nri3824.
Mayne CG, Williams CB. Induced and natural regulatory T cells in the development of inflammatory bowel disease. Inflamm Bowel Dis. 2013;19:1772–88. doi:10.1097/MIB.0b013e318281f5a3.
Harrison OJ, Powrie FM. Regulatory T cells and immune tolerance in the intestine. Cold Spring Harb Perspect Biol. 2013;5. doi:10.1101/cshperspect.a018341.
Bennett CL et al. The immune dysregulation, polyendocrinopathy, enteropathy, X-linked syndrome (IPEX) is caused by mutations of FOXP3. Nat Genet. 2001;27:20–1. doi:10.1038/83713.
Wildin RS et al. X-linked neonatal diabetes mellitus, enteropathy and endocrinopathy syndrome is the human equivalent of mouse scurfy. Nat Genet. 2001;27:18–20. doi:10.1038/83707.
Wildin RS, Smyk-Pearson S, Filipovich AH. Clinical and molecular features of the immunodysregulation, polyendocrinopathy, enteropathy, X linked (IPEX) syndrome. J Med Genet. 2002;39:537–45.
Maillard MH et al. The Wiskott-Aldrich syndrome protein is required for the function of CD4(+)CD25(+)Foxp3(+) regulatory T cells. J Exp Med. 2007;204:381–91. doi:10.1084/jem.20061338.
Boden EK, Snapper SB. Regulatory T cells in inflammatory bowel disease. Curr Opin Gastroenterol. 2008;24:733–41.
Gavin MA et al. Single-cell analysis of normal and FOXP3-mutant human T cells: FOXP3 expression without regulatory T cell development. Proc Natl Acad Sci U S A. 2006;103:6659–64.
Takahashi T et al. Immunologic self-tolerance maintained by CD25(+)CD4(+) regulatory T cells constitutively expressing cytotoxic T lymphocyte-associated antigen 4. J Exp Med. 2000;192:303–10.
Shimizu J, Yamazaki S, Takahashi T, Ishida Y, Sakaguchi S. Stimulation of CD25(+)CD4(+) regulatory T cells through GITR breaks immunological self-tolerance. Nat Immunol. 2002;3:135–42.
Liu W et al. CD127 expression inversely correlates with FoxP3 and suppressive function of human CD4+ T reg cells. J Exp Med. 2006;203:1701–11. doi:10.1084/jem.20060772.
Seddiki N et al. Expression of interleukin (IL)-2 and IL-7 receptors discriminates between human regulatory and activated T cells. J Exp Med. 2006;203:1693–700. doi:10.1084/jem.20060468.
Powrie F, Leach MW, Mauze S, Caddle LB, Coffman RL. Phenotypically distinct subsets of CD4+ T cells induce or protect from chronic intestinal inflammation in C. B-17 scid mice. Int Immunol. 1993;5:1461–71.
Mottet C, Uhlig HH, Powrie F. Cutting edge: cure of colitis by CD4+CD25+ regulatory T cells. J Immunol. 2003;170:3939–43.
Tang Q et al. In vitro-expanded antigen-specific regulatory T cells suppress autoimmune diabetes. J Exp Med. 2004;199:1455–65.
Kohm AP, Carpentier PA, Anger HA, Miller SD. Cutting edge: CD4+CD25+ regulatory T cells suppress antigen-specific autoreactive immune responses and central nervous system inflammation during active experimental autoimmune encephalomyelitis. J Immunol. 2002;169:4712–6.
Scalapino KJ, Tang Q, Bluestone JA, Bonyhadi ML, Daikh DI. Suppression of disease in New Zealand Black/New Zealand White lupus-prone mice by adoptive transfer of ex vivo expanded regulatory T cells. J Immunol. 2006;177:1451–9.
Asano M, Toda M, Sakaguchi N, Sakaguchi S. Autoimmune disease as a consequence of developmental abnormality of a T cell subpopulation. J Exp Med. 1996;184:387–96.
Thornton AM, Shevach EM. Suppressor effector function of CD4+CD25+ immunoregulatory T cells is antigen nonspecific. J Immunol. 2000;164:183–90.
Collison LW et al. The inhibitory cytokine IL-35 contributes to regulatory T-cell function. Nature. 2007;450:566–9.
Li MO, Wan YY, Flavell RA. T cell-produced transforming growth factor-beta1 controls T cell tolerance and regulates Th1- and Th17-cell differentiation. Immunity. 2007;26:579–91.
Asseman C, Mauze S, Leach MW, Coffman RL, Powrie F. An essential role for interleukin 10 in the function of regulatory T cells that inhibit intestinal inflammation. J Exp Med. 1999;190:995–1004.
Murai M et al. Interleukin 10 acts on regulatory T cells to maintain expression of the transcription factor Foxp3 and suppressive function in mice with colitis. Nat Immunol. 2009;10:1178–84.
Rubtsov YP et al. Regulatory T cell-derived interleukin-10 limits inflammation at environmental interfaces. Immunity. 2008;28:546–58. doi:10.1016/j.immuni.2008.02.017.
Liu JQ et al. Increased Th17 and regulatory T cell responses in EBV-induced gene 3-deficient mice lead to marginally enhanced development of autoimmune encephalomyelitis. J Immunol. 2012;188:3099–106. doi:10.4049/jimmunol.1100106.
Borsellino G et al. Expression of ectonucleotidase CD39 by Foxp3+ Treg cells: hydrolysis of extracellular ATP and immune suppression. Blood. 2007;110:1225–32. doi:10.1182/blood-2006-12-064527.
Deaglio S et al. Adenosine generation catalyzed by CD39 and CD73 expressed on regulatory T cells mediates immune suppression. J Exp Med. 2007;204:1257–65. doi:10.1084/jem.20062512.
Bettini M, Vignali DA. Regulatory T cells and inhibitory cytokines in autoimmunity. Curr Opin Immunol. 2009;21:612–8.
Bilate AB, Lafaille JJ. It takes two to tango. Immunity. 2011;35:6–8. doi:10.1016/j.immuni.2011.07.003.
Haribhai D et al. A central role for induced regulatory T cells in tolerance induction in experimental colitis. J Immunol. 2009;182:3461–8.
Chen Y et al. Oral tolerance in myelin basic protein T-cell receptor transgenic mice: suppression of autoimmune encephalomyelitis and dose-dependent induction of regulatory cells. Proc Natl Acad Sci U S A. 1996;93:388–91.
Fantini MC et al. Transforming growth factor beta induced FoxP3+ regulatory T cells suppress Th1 mediated experimental colitis. Gut. 2006;55:671–80.
Groux H et al. A CD4+ T-cell subset inhibits antigen-specific T-cell responses and prevents colitis. Nature. 1997;389:737–42.
Faria AM, Weiner HL. Oral tolerance. Immunol Rev. 2005;206:232–59.
Kamanaka M et al. Expression of interleukin-10 in intestinal lymphocytes detected by an interleukin-10 reporter knockin tiger mouse. Immunity. 2006;25:941–52. doi:10.1016/j.immuni.2006.09.013.
Battaglia M, Gregori S, Bacchetta R, Roncarolo MG. Tr1 cells: from discovery to their clinical application. Semin Immunol. 2006;18:120–7.
Gagliani N et al. Coexpression of CD49b and LAG-3 identifies human and mouse T regulatory type 1 cells. Nat Med. 2013;19:739–46. doi:10.1038/nm.3179.
Collison LW et al. IL-35-mediated induction of a potent regulatory T cell population. Nat Immunol. 2010;11:1093–101.
Sefik E et al. Individual intestinal symbionts induce a distinct population of RORgamma + regulatory T cells. Science. 2015;349:993–7. doi:10.1126/science.aaa9420.
Ohnmacht C et al. The microbiota regulates type 2 immunity through RORgammat + T cells. Science. 2015;349:989–93. doi:10.1126/science.aac4263.
Cosmi L, Maggi L, Santarlasci V, Liotta F, Annunziato F. T helper cells plasticity in inflammation. Cytometry A. 2014;85:36–42. doi:10.1002/cyto.a.22348.
Wohlfert E, Belkaid Y. Plasticity of Treg at infected sites. Mucosal Immunol. 2010;3:213–5.
Lee YK, Mukasa R, Hatton RD, Weaver CT. Developmental plasticity of Th17 and Treg cells. Curr Opin Immunol. 2009;21:274–80.
Zhou X et al. Instability of the transcription factor Foxp3 leads to the generation of pathogenic memory T cells in vivo. Nat Immunol. 2009;10:1000–7. doi:10.1038/ni.1774.
Hovhannisyan Z, Treatman J, Littman DR, Mayer L. Characterization of interleukin-17-producing regulatory T cells in inflamed intestinal mucosa from patients with inflammatory bowel diseases. Gastroenterology. 2011;140:957–65. doi:10.1053/j.gastro.2010.12.002.
Gagliani N et al. Th17 cells transdifferentiate into regulatory T cells during resolution of inflammation. Nature. 2015;523:221–5. doi:10.1038/nature14452.
Esplugues E et al. Control of TH17 cells occurs in the small intestine. Nature. 2011;475:514–8. doi:10.1038/nature10228.
Brimnes J et al. Defects in CD8+ regulatory T cells in the lamina propria of patients with inflammatory bowel disease. J Immunol. 2005;174:5814–22.
Allez M, Brimnes J, Dotan I, Mayer L. Expansion of CD8+ T cells with regulatory function after interaction with intestinal epithelial cells. Gastroenterology. 2002;123:1516–26.
Poussier P, Ning T, Banerjee D, Julius M. A unique subset of self-specific intraintestinal T cells maintains gut integrity. J Exp Med. 2002;195:1491–7.
Das G et al. An important regulatory role for CD4+CD8 alpha alpha T cells in the intestinal epithelial layer in the prevention of inflammatory bowel disease. Proc Natl Acad Sci U S A. 2003;100:5324–9.
Chen Y, Chou K, Fuchs E, Havran WL, Boismenu R. Protection of the intestinal mucosa by intraepithelial gamma delta T cells. Proc Natl Acad Sci U S A. 2002;99:14338–43.
Nanno M et al. Exacerbating role of gammadelta T cells in chronic colitis of T-cell receptor alpha mutant mice. Gastroenterology. 2008;134:481–90.
Heller F, Fuss IJ, Nieuwenhuis EE, Blumberg RS, Strober W. Oxazolone colitis, a Th2 colitis model resembling ulcerative colitis, is mediated by IL-13-producing NK-T cells. Immunity. 2002;17:629–38.
Saubermann LJ et al. Activation of natural killer T cells by alpha-galactosylceramide in the presence of CD1d provides protection against colitis in mice. Gastroenterology. 2000;119:119–28.
Olszak T et al. Microbial exposure during early life has persistent effects on natural killer T cell function. Science (New York, NY). 2012;336(6080):489–93. doi:10.1126/science.1219328.
Matsuura T, West GA, Youngman KR, Klein JS, Fiocchi C. Immune activation genes in inflammatory bowel disease. Gastroenterology. 1993;104:448–58.
Boirivant M et al. Lamina propria T cells in Crohn’s disease and other gastrointestinal inflammation show defective CD2 pathway-induced apoptosis. Gastroenterology. 1999;116:557–65.
Galvez J. Role of Th17 cells in the pathogenesis of human IBD. ISRN Inflamm. 2014;2014:928461. doi:10.1155/2014/928461.
Wallace KL, Zheng LB, Kanazawa Y, Shih DQ. Immunopathology of inflammatory bowel disease. World J Gastroenterol. 2014;20:6–21. doi:10.3748/wjg.v20.i1.6.
Awane M, Andres PG, Li DJ, Reinecker HC. NF-kappa B-inducing kinase is a common mediator of IL-17-, TNF-alpha-, and IL-1 beta-induced chemokine promoter activation in intestinal epithelial cells. J Immunol. 1999;162:5337–44.
Witowski J et al. IL-17 stimulates intraperitoneal neutrophil infiltration through the release of GRO alpha chemokine from mesothelial cells. J Immunol. 2000;165:5814–21.
Franke A et al. Genome-wide meta-analysis increases to 71 the number of confirmed Crohn’s disease susceptibility loci. Nat Genet. 2010;42:1118–25. doi:10.1038/ng.717.
Franke A et al. Genome-wide association study for ulcerative colitis identifies risk loci at 7q22 and 22q13 (IL17REL). Nat Genet. 2010;42:292–4. doi:10.1038/ng.553.
McGovern DP et al. Genome-wide association identifies multiple ulcerative colitis susceptibility loci. Nat Genet. 2010;42:332–7. doi:10.1038/ng.549.
Cui D, Huang G, Yang D, Huang B, An B. Efficacy and safety of interferon-gamma-targeted therapy in Crohn’s disease: a systematic review and meta-analysis of randomized controlled trials. Clin Res Hepatol Gastroenterol. 2013;37:507–13. doi:10.1016/j.clinre.2012.12.004.
Reinisch W et al. Fontolizumab in moderate to severe Crohn’s disease: a phase 2, randomized, double-blind, placebo-controlled, multiple-dose study. Inflamm Bowel Dis. 2010;16:233–42. doi:10.1002/ibd.21038.
Reinisch W et al. A dose escalating, placebo controlled, double blind, single dose and multidose, safety and tolerability study of fontolizumab, a humanised anti-interferon gamma antibody, in patients with moderate to severe Crohn’s disease. Gut. 2006;55:1138–44. doi:10.1136/gut.2005.079434.
Hueber W et al. Secukinumab, a human anti-IL-17A monoclonal antibody, for moderate to severe Crohn’s disease: unexpected results of a randomised, double-blind placebo-controlled trial. Gut. 2012;61:1693–700. doi:10.1136/gutjnl-2011-301668.
Danese S et al. Tralokinumab for moderate-to-severe UC: a randomised, double-blind, placebo-controlled, phase IIa study. Gut. 2015;64:243–9. doi:10.1136/gutjnl-2014-308004.
Reinisch W et al. Anrukinzumab, an anti-interleukin 13 monoclonal antibody, in active UC: efficacy and safety from a phase IIa randomised multicentre study. Gut. 2015;64:894–900. doi:10.1136/gutjnl-2014-308337.
Amiot A, Peyrin-Biroulet L. Current, new and future biological agents on the horizon for the treatment of inflammatory bowel diseases. Therap Adv Gastroenterol. 2015;8:66–82. doi:10.1177/1756283X14558193.
Abraham C, Cho JH. Inflammatory bowel disease. N Engl J Med. 2009;361:2066–78.
Abe K et al. Conventional dendritic cells regulate the outcome of colonic inflammation independently of T cells. Proc Natl Acad Sci U S A. 2007;104:17022–7. doi:0708469104 [pii].
Shouval DS et al. Interleukin-10 receptor signaling in innate immune cells regulates mucosal immune tolerance and anti-inflammatory macrophage function. Immunity. 2014;40:706–19. doi:10.1016/j.immuni.2014.03.011.
Podolsky DK. Selective adhesion-molecule therapy and inflammatory bowel disease—a tale of Janus? N Engl J Med. 2005;353:1965–8. doi:10.1056/NEJMe058212.
Feagan BG et al. Treatment of active Crohn’s disease with MLN0002, a humanized antibody to the alpha4beta7 integrin. Clin Gastroenterol Hepatol. 2008;6:1370–7.
Sandborn WJ et al. Natalizumab induction and maintenance therapy for Crohn’s disease. N Engl J Med. 2005;353:1912–25. doi:10.1056/NEJMoa043335.
Feagan BG et al. Treatment of ulcerative colitis with a humanized antibody to the alpha4beta7 integrin. N Engl J Med. 2005;352:2499–507.
Sandborn WJ et al. Vedolizumab as induction and maintenance therapy for Crohn’s disease. N Engl J Med. 2013;369:711–21. doi:10.1056/NEJMoa1215739.
Rutgeerts PJ et al. A randomised phase I study of etrolizumab (rhuMAb beta7) in moderate to severe ulcerative colitis. Gut. 2013;62:1122–30. doi:10.1136/gutjnl-2011-301769.
Thomas S, Baumgart DC. Targeting leukocyte migration and adhesion in Crohn’s disease and ulcerative colitis. Inflammopharmacology. 2012;20:1–18. doi:10.1007/s10787-011-0104-6.
Neurath MF. New targets for mucosal healing and therapy in inflammatory bowel diseases. Mucosal Immunol. 2014;7:6–19. doi:10.1038/mi.2013.73.
Papadakis KA et al. CC chemokine receptor 9 expression defines a subset of peripheral blood lymphocytes with mucosal T cell phenotype and Th1 or T-regulatory 1 cytokine profile. J Immunol. 2003;171:159–65.
Maul J et al. Peripheral and intestinal regulatory CD4+ CD25(high) T cells in inflammatory bowel disease. Gastroenterology. 2005;128:1868–78.
Yu QT et al. Expression and functional characterization of FOXP3+ CD4+ regulatory T cells in ulcerative colitis. Inflamm Bowel Dis. 2007;13:191–9.
Kelsen J et al. FoxP3(+)CD4(+)CD25(+) T cells with regulatory properties can be cultured from colonic mucosa of patients with Crohn’s disease. Clin Exp Immunol. 2005;141:549–57.
Canavan JB et al. Developing in vitro expanded CD45RA+ regulatory T cells as an adoptive cell therapy for Crohn’s disease. Gut. 2015;65:584–94. doi:10.1136/gutjnl-2014-306919.
Desreumaux P et al. Safety and efficacy of antigen-specific regulatory T-cell therapy for patients with refractory Crohn’s disease. Gastroenterology. 2012;143:1207–17. doi:10.1053/j.gastro.2012.07.116. e1201–2.
Ochi H et al. Oral CD3-specific antibody suppresses autoimmune encephalomyelitis by inducing CD4+ CD25− LAP+ T cells. Nat Med. 2006;12:627–35.
Ishikawa H et al. Inhibition of autoimmune diabetes by oral administration of anti-CD3 monoclonal antibody. Diabetes. 2007;56:2103–9.
Koreth J et al. Interleukin-2 and regulatory T cells in graft-versus-host disease. N Engl J Med. 2011;365:2055–66. doi:10.1056/NEJMoa1108188.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Snapper, S., Nguyen, D., Biswas, A. (2017). Immunobiology of T-Cells in Inflammatory Bowel Disease. In: Baumgart, D. (eds) Crohn's Disease and Ulcerative Colitis. Springer, Cham. https://doi.org/10.1007/978-3-319-33703-6_8
Download citation
DOI: https://doi.org/10.1007/978-3-319-33703-6_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-33701-2
Online ISBN: 978-3-319-33703-6
eBook Packages: MedicineMedicine (R0)