
Abstract
Inflammatory bowel disease (IBD) usually takes a persistent course, and this feature suggests the importance of acquired immunity in the pathogenesis of IBD such as Crohn’s disease (CD) and ulcerative colitis (UC). Helper T (Th) cells differentiated from CD4+ naïve T cells play central roles in the acquired immune system. Th cells are classified as Th1, Th2, Th17, or Treg. In addition, other newly defined Th subsets have also been reported recently. CD was originally thought to be Th1-mediated disease, while UC was thought to be Th2-mediated. However, it has been recently reported that other Th subsets are also involved in the pathogenesis of IBD as well as in multiple animal models. Although Th subsets have become more complexed, it may be helpful for the establishment of future immunologic therapy for IBD.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Inflammatory bowel disease (IBD) may occur only once in a patient’s lifetime, but often it recurs and becomes refractory [1]. This feature suggests “pathogenic memory ” that hints the importance of acquired immunity in the pathogenesis of IBD. Therefore, helper T (Th) cells differentiated from CD4+ naïve T cells play central roles in the acquired immune system. Thus, each Th cell subset secretes various cytokines, which activate other immune cells. Original Th cell subsets only included type 1 (Th1) or type 2 (Th2). Subsequent recognition of regulatory T cells (Treg), which regulates effector T cell functions negatively, and Th17 cells added to the complexity of the system [2].
The effectiveness of monoclonal antibody against TNF-α, which is one of the proinflammatory cytokines secreted by several Th subsets as well as macrophages, for the treatment for both Crohn’s disease (CD) and ulcerative colitis (UC) has changed natural history of IBD pathogenesis [3]. This has encouraged many scientists to develop more effective therapies targeting other T cell activation pathways . Furthermore, Th17 has also been highlighted in the pathogenesis of IBD due to significant association between the genetic polymorphisms in the Th17/IL-23 pathway. In this section, the role of each Th subset in the pathogenesis of IBD is discussed since this will be the fundamental basis for the future development of IBD treatment.
Differentiation of Helper T Cells
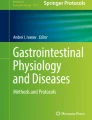
When CD4+ T cells are developed in thymus and migrated to the peripheral tissues, they are called naïve T cells, which secret minimal cytokines and no efficient effector function. However, they are activated when specific antigens are presented to their T cell receptors (TCR) via antigen presenting cells (APC) through MHC class-II with co-stimulatory signaling. Moreover, cytokines in the environment where the antigen presentation occurs determine the polarization of these Th cells. Thus, expression of the specific transcription factors such as T-bet, GATA-3, and retinoic acid receptor-related orphan receptor (ROR-γτ) is induced in these cells. Such an event allows naïve T cells to differentiate into various Th cells that secrete characteristic type of cytokines [4] (Fig. 14.1).

Differentiation of helper CD4+ T cells. When antigens specific for their own TCR are presented to naïve T cells by APC through MHC class-II/TCR signal with co-stimulatory signals, naïve T cells differentiate to helper T cells, which secrete characteristic types of cytokines and express specific transcription factors. Cytokines in the environment where the antigen presentation occurs determine the polarization of these helper T cells. Th1 cells differentiate in the presence of IL-12, and secrete IFN-γ, TNF-α, and IL-2. IL-12 activates STAT4 pathway through IL-12R and promotes T-bet, which is a master regulator for the Th1 differentiation. Th2 cells differentiate in the presence of IL-4, and secrete IL-4, IL-5, and IL-13. IL-4 activates STAT6 pathway through IL-4R and promotes GATA-3, which is a master regulator of the Th2 differentiation. Th17 cells produce L-17A, IL-17F, IL-21, IL-22, and TNF-α. Th17 cells differentiate in the presence of IL-6 and TGF-β, through the expression of ROR-γt, which is a master regulator of Th17. While TGF-β drives Smad signaling, IL-6 activates STAT3 pathway, which promotes the expression of RORγt. IL-21 is an important cytokine for the amplification of Th17, while IL-23 is important for their stabilization. Th9 cells differentiate in the presence of TGF-β and IL-4, and secrete IL-9. IL-9 expression in these cells is regulated by transcription factors such as PU.1, STAT6, Batf, GATA3, and IRF4. Particularly, PU.1, which is induced by TGFβ, is thought to be a master regulator for Th9, and inhibits the development of Th2. Th22 cells differentiate in the presence of IL-6, TNF, and FICZ, and secrete IL-22, but not IL-17. FICZ activates AHR, which is thought to be a master regulator for the Th22 differentiation. Th22 cells are also known to produce IL-13 and FGF. On the other hand, TGF-β is known to suppress Th22. iTreg is derived from naïve T cells in the presence of TGF-β and the absence of IL-6 through the expression of Foxp3. RA and IL-2 promote iTreg differentiation. In addition, IL-2 is an important survival factor for Treg. On the other hand, IL-6 prevents iTreg differentiation and promotes Th17 differentiation
Th1 Differentiation
Classically, helper CD4+ T cells were classified as Th1 or Th2. Th1 cells differentiate in the presence of IL-12 and secrete IFN-γ, TNF-α, and IL-2. Th1 cells play an important role in the cellular immunity against tumors and intracellular viral and/or bacterial infections. IL-12 is secreted by APC such as macrophages and dendritic cells (DC) . IL-12 activates STAT4 pathway through IL-12 receptor (IL-12R) signalin g and T-bet, a transcription factor which promotes specific gene expression profile including IFN-γ. This expression of IFN-γ is also one of the important factors for Th1 differentiation, because such differentiation can be inhibited by IFN-γ neutralization according to in vitro experiments. However, T-bet, a member of the T-box family, is thought to be the master regulator of the Th1 differentiation. While artificial transduction of T-bet in polarized Th2 cells converts them into Th1 cells, its absence causes disorder of Th1 differentiation in vitro and in vivo. T-bet prompts IL-12R expression and activates IFN-γ gene, which results in a positive feedback of Th1 polarization [4, 5].
Th2 Differentiation
Th2 cells are differentiated in the presence of IL-4 when specific antigens are presented to their TCR by APC, and these cells then start to secrete IL-4, IL-5, and IL-13. Th2 cells play an important role mainly in humoral immunity against parasites and some allergens. IL-4 activates STAT6 pathway through IL-4 receptor (IL-4R) signaling and promotes expression of GATA-3, which is a master regulator of the Th2 differentiation. In the absence of GATA-3, Th2 development is inhibited in vitro and in vivo, while transduction of GATA-3 in the polarized Th1 cells results in IL-4 secretion. GATA-3 induces IL-4 gene expression , which forms a positive feedback of Th2 polarization. IL-12 inhibits Th2 polarization, while IL-4 inhibits Th1 differentiation, which makes these subsets reciprocal [4, 5].
Th17 Differentiation
Th17 cells have been reported to produce L-17A, IL-17F, IL-21, IL-22, and TNF-α, and these cells play an important role in the protective immunity against the extracellular pathogens such as bacteria [6]. Th17 cells are differentiated in the presence of IL-6 and TGF-β at the antigen presentation through the expression of RORγt. While TGF-β drives Smad signaling, IL-6 activates STAT3 pathway , which promotes the expression of RORγt [2]. RORγt, a transcription factor expressed on double positive (DP) T cells in the thymus and type 3 innate lymphoid cells (ILC3) , is thought to be the master regulator of Th17 differentiation. Transduction of RORγt to CD4+ T cells results in significant IL-17A secretion, while depletion in Th17 cells results in decreased IL-17A production. In addition to RORγt, Th17 cells may also express RORα, which is upregulated by STAT3 pathway . RORα deficient mice are still able to produce normal level of IL-17A, while RORγt deficient mice have impaired production of IL-17A. However, IL-17A production in RORγt deficient mice is dependent on the expression of RORα, and thus RORα and RORγt double deficient mice cannot produce any IL-17A [7]. In addition, IL-21 is also important cytokine for the differentiation of Th17. IL-6 promotes the production of IL-21 from Th17 cells independent of RORγt, and subsequently IL-21 upregulates the expression of RORγt through the activation of STAT3 pathway . This process forms a positive feedback in the Th17 differentiation and is thus called “amplification”. Therefore, it is necessary for the amplification of Th17 cells although IL-21 is not essential for h17 polarization. In fact, IL-21 deficient mice show a reduction in the number of Th17 cells [8]. IL-23 is also important for the Th17 pathway. However, IL-23 receptor (IL-23R) is not originally expressed on naïve T cells. TGF-β signal mediates IL-23R expression on Th17 cells, which makes them responsive to IL-23. IL-23 is essential to the maintenance of the Th17 phenotype in long-term cultures. Therefore, the effect of IL-23 on Th17 is defined as “stabilization” [8]. IL-23 is highly expressed in mucosa of human ileum, and there are many Th17 cells in the human GALT. These Th17 cells play an important role for protective immunity against intestinal pathogens. Intestinal microbiota is essential for the development of Th17, since mice in germ-free condition show decreased number of Th17 cells [9].
Treg Differentiation
Regulatory T cells (Treg) play a crucial role in peripheral tolerance to prevent autoimmune disease development and chronic inflammation. Thus, Treg is one of the CD4+ T cell subsets that inhibit other Th cells, and this subset consists of two distinct subpopulations, naturally occurring Treg (nTreg) and induced Treg (iTreg) [10]. While nTreg is generated during T cell development in the thymus, iTreg is differentiated from naïve T cells in the peripheral tissues during an immune response.
In the thymus, nTreg is identified as CD4+CD25+ auto-reactive T cells expressing TCR specific for auto-antigens. Although CD25 (also known as IL-2Rα chain) was previously thought to be an activation marker of effector T cells, it is notably expressed on nTreg in response to auto-antigens. nTreg may also express GITR and CTLA-4, as well as Foxp3 which is thought to be the master regulator of nTreg. Genetic depletion of Foxp3 leads to various autoimmune disease and chronic intestinal inflammation similar to that of IBD. Furthermore, induction of Foxp3 to CD4+ T cells causes inhibition of effector T cells [10].
The other Treg subset, iTreg, may be derived from peripheral naïve T cells in the presence of TGF-β and the absence of IL-6 through the expression of Foxp3. It is believed that retinoic acid (RA) and IL-2 promote iTreg differentiation. IL-2 is especially important for the survival factor of Treg. On the other hand, IL-6 prevents iTreg differentiation and promotes Th17 differentiation instead [4–6, 10]. In this manner, IL-6 may be an important cytokine that regulates the balance between Treg and Th17. However, these findings are according to in vitro assays, and whether they can be applied in vivo is still largely unknown.
Role of Each Th Subset in IBD Models
In the past, CD was originally thought to be a Th1-mediated disease, while UC was Th2-mediated. Accordingly, the pathogenesis of animal models of IBD was understood to be either Th1- or Th2-mediated intestinal inflammation. However, many studies have already demonstrated that both Th1 and Th2 conditions can exist in most of animal models (Table 14.1) as well as IBD patients (Table 14.2). Moreover, recent studies also showed plasticity of Th cells differentiating into other subsets. Also, newly defined Th subsets, such as Th9 and Th22, have been added to the mix (Fig. 14.1).
Th1 in Animal Models
It is known that naïve T cells derived from wild type mice can be differentiated into colitogenic effector T cells after transferring to the recipients such as RAG-deficient and SCID mice. Chronic colitis in this animal model was originally thought to be induced by Th1 inflammation. Thus, it has been reported that naïve T cells from T-bet deficient mice are unable to induce colitis in the recipient RAG-deficient mice , and the overexpression of T-bet in naive T cells results in exacerbation of colitis [11]. In addition, naïve T cells from STAT4 deficient mice cause less severe colitis in the recipients [12]. On the other hand, it is known that the lack of IL10 gene results in spontaneous chronic colitis which was also thought to be Th1-mediated. In fact, administration of antagonistic antibody against IFN-γ abrogates colitis in IL-10 deficient mice as well as T cell-reconstituted RAG-deficient mice [13, 14]. However, naïve T cells from IFN-γ deficient mice may induce colitis [12]. Furthermore, IL-10 and IFN-γ double-deficient mice develop colitis equally as IL-10 deficient mice when they are infected with H. hepaticus [15]. These findings suggest that IFN-γ may not be essential for the development of colitis in these models.
Th2 in Animal Models
While Th1 plays important role in the pathogenesis of most animal models of IBD, there are few IBD models that are thought to be Th2 related [16]. Oxazolone-induced colitis , one of the models induced by haptens, reveals acute inflammation limited to colonic mucosa lasting for 4–5 days [17]. CD4+ T cells in the intestinal mucosa in oxazolone-treated mice produce large amounts of Th2 cytokines such as IL-4 and IL-5. Therefore it is believed that Th2 cells plays an important role in this model [17], while CD4+ T cells in TNBS-induced colitis model, which is also hapten-induced, produce Th1 cytokines such as IL-2 and IFN-γ [18]. Neutralization of IL-4 can attenuate the severity of oxazolone-induced colitis [17]. When mice are exposed to oxazolone prior to the rectal administration, chronic inflammation is induced and production of IL-4 is increased in the early phase followed by IL-13 elevation in the chronic phase [18]. In this chronic model, it is reported that the main sources of IL-13 are not only Th2 cells but also CD1d-restricted invariant NKT cells. In fact, either depletion of NKT cells or inhibition of CD1-restricted antigen presentation suppresses the development of colitis in this model [19, 20].
Th17 in Animal Models
IL-23 forms a heterodimer made of p19 subunit and p40 subunit, which is also a subunit of IL-12. Therefore it was previously difficult to determine whether IL-12/Th1 or IL-23/Th17 pathway was more critical in the pathogenesis in many animal models since the antibody used in these experiments targeted IL-12p40. In fact, it has been reported the increase of Th17 cells in several colitis models are IL-12 dependent [5]. For example, in both IL-10 deficient mice and T cell-reconstituted RAG deficient mice, both of which have been thought as Th1 models previously, CD4+ T cells producing a large amount of IL-17 are increased as well as IFN-γ producing cells [21, 22]. IL-23p19 transgenic mice develop colitis and systemic autoimmune disease [23]. Administration of recombinant IL-23 exacerbates colitis in RAG deficient mice that has with naïve T cells from IL-10 deficient mice [22]. Genetic depletion or neutralization of IL-23p19 ameliorates colitis in both IL-10 deficient and T cell-transferred RAG deficient mice [22, 24]. IL-21 is important for the amplification of Th17 cell, and IL-21 depletion can ameliorates DSS colitis and TNBS colitis [25]. These observations suggest that Th17/IL-23 is more important than IL-12/Th1 in the pathogenesis in this model.
IL-17, including various subtypes such as IL-17A and IL-17F, is a main effector cytokine of Th17. However, the role of IL-17 in the pathogenesis of IBD is controversial, and there are different arguments that it exacerbates, ameliorates, or does not influence colitis. IL-17A deficient mice developed more severe colitis than wild type mice in the TNBS colitis model, and administration of antibody against IL-17A exacerbates colitis induced by DSS [26]. In addition, although IL-23 is not dispensable for the development of colitis in T cell-reconstituted RAG deficient mice, IL-17 is not essential [21]. IL-17A suppresses DSS colitis, while IL-17F accelerates colitis in this model [27]. Similarly, IL-17A suppresses colitis in T cell-transferred RAG deficient mic e, inhibiting the polarization of Th1 [28]. In summary, effects of IL-17 in colitis differ among the various colitis models or experimental methods such as genetic depletion or neutralization antibodies.
In the oxazolone colitis model, depletion of IRF-4, an important factor for the Th2 differentiation, can suppress colitis [29]. However, IRF-4 is also associated with the Th17 differentiation, and therefore the importance of Th17 rather than Th2 cannot be excluded. In addition, it is known that depletion of IL-6, important factor for the differentiation of Th17, leads to suppression of oxazolone colitis, suggesting that Th17 may be critical in the pathogenesis of this model. Furthermore, recent studies reported that Th17 cells may trans-differentiate into Th1 or Treg [30, 31], and Treg cells may trans-differentiate into Th17 cells [32–34]. Taken together, further investigations are needed on Th17 functions in IBD.
Th9 in Animal Models
The expression of a cytokine IL-9 was originally associated with Th2 phenotype such as the one during infection with Leishmania major. However, Th9, a specialized IL-9-producing T cell subset induced by IL-4 and TGFβ, has been recently reported [35–37]. In this subset, IL-9 expression has been reported to be regulated by transcription factors such as PU.1, STAT6, Batf, GATA3, and IRF4. Particularly, IL-9 transcription is controlled by PU.1, which is induced by TGFβ. Therefore, PU.1 is thought to be a master regulator for Th9 (Fig. 14.1). PU.1, which is encoded by Spi1 gene, is known to inhibit the development of Th2.
The exacerbation of colitis in the T cell-reconstituted RAG deficient mice by co-transfer of IL-10 and IL-9 double positive T cells with naïve T cells has been reported [35]. And recently, it has been reported that Th9 subset is also induced in the oxazolone-induced colitis model. Neutralization of IL-9 with antibodies or deficiency in PU.1 results in amelioration of colitis [38]. IL-9 was found to have epithelial cells with impaired intestinal barrier function and poor mucosal healing.
Th22 in Animal Models
IL-22 is known to be produced by Th17 cells. It is an inhibitory cytokine unlike other Th17 cytokines. IL-22 is also produced by ILC3 including lymphoid inducer cells (LTi) and one of the NK cell subset. Recently it is reported that IL-22 producing RORγt+NKp46+ cells play a critical role in the homeostasis of intestinal mucosal immune system. In addition, a newly defined Th subset called Th22 producing IL-22, but not IL-17, has been recently reported [39, 40]. Th22 cells are differentiated in the presence of IL-6, TNF and the tryptophan metabolite 6-formylindolo [3,2-b] carbazole (FICZ) , and secrete IL-22, but not IL-17. FICZ is known to be a natural ligand for aryl hydrocarbon receptor (AHR) . AHR is a ligand-dependent transcription factor, and thought to be a master regulator for the Th22 differentiation (Fig. 14.1). Th22 cells are also known to produce IL-13 and fibroblast growth factor (FGF ). On the other hand, TGF-β is known to suppress Th22 differentiation.
Either genetic depletion or neutralization of IL-22 exacerbates colitis in T cell-reconstituted RAG deficient and DSS-treated mice [41]. IL-22 not only prevents excess activation of immune system but also induces anti-apoptotic molecules in the intestinal epithelial cells to ameliorate epithelial dysfunction in colitis [42].
Each Th Subset in IBD Patients
Th1 had been originally thought to play important roles in the pathogenesis of CD and Th2 in UC. However, it has also been reported that Th17 may be involved in the pathogenesis of CD and UC. In addition, significant associations between genomic regions of Th17/IL-23 pathwa y and IBD have been reported from genome wide association studies (GWAS) [43]. On the other hand, the roles of the newly defined Th9 and Th22 subsets in the pathogenesis of UC have been accumulating (Table 14.2).
CD Patients
A large number of CD4+ T cells that highly express T-bet and STAT-4 have been found in the intestinal mucosa of CD patients [11, 44]. In fact, CD4+ T cells in the intestinal lamina propria of CD patients produce a large amount of IFN-γ and lower amount of IL-4 when compared to that of healthy control [44]. Macrophages in the intestinal lamina propria of CD patients produce a large amount of IL-12 [45]. Lymphocytes in the intestinal lamina propria of CD patients express high levels of IL-12R, and produce a large amount of IFN-γ in response to IL-12 [46]. Although treatment with blocking antibody against IFN-γ has not been effective in CD patient, treatment of monoclonal antibody against IL-12p40 may be effective [47]. These data show that Th1 is also strongly associated with the pathogenesis of CD.
On the other hand, it is reported that IL-17A, IL-17F, IL-21, IL-22, IL-23, RORγt, and IL-23R are highly expressed in the intestinal mucosa of CD patients [4, 48]. Furthermore, a unique macrophage producing IL-23, TNF and IL-6 are found to be increased in the intestinal mucosa of CD patients [49]. IL-17 and IL-23 in CD patients decrease after treatment with steroids or neutralizing antibody against IL-12p40 [50]. As mentioned above, several GWAS proved significant associations between the genomic regions of Th17/IL-23 pathway and IBD [43]. Although Th17 is believed to be an important factor in IBD development, human data are weak, and further studies are still needed.
UC Patients
UC has traditionally been thought of as Th2-mediated, because IFN-γ in the colon of UC patients has always found to be very low. In UC patients, CD4+ T cells in the intestinal lamina propria secretes higher amount of IL-5 and IL-13 compared to that of CD patients or healthy control [44, 51]. On the other hand, IL-4, the predominant Th2 cytokine, level in the intestine of UC is lower than that of CD patients or healthy control [44], and this suggests that UC cannot be defined as merely a Th2-mediated disease. Similarly to the oxazolone-induced colitis model, the main sources of IL-13 in the colonic mucosa of UC patients are CD1d-restricted invariant NKT cells . In fact, there are many NKT cells in the inflamed mucosa of UC patients [51]. However, the role of IL-13 and NKT cells in the pathogenesis of UC is not clear, and further investigations are still needed.
Th17 cytokines, such as IL-17A, IL-17F, IL-21, IL-22, IL-23, RORγt, and IL-23R, are highly expressed in the intestinal mucosa of UC patients [4, 48]. Moreover, Th9 subset expressing the transcription factor PU.1 and IL-9, as well as the epithelial cells expressing IL-9R, has been recently reported in the patients with UC [38]. PU.1 expression is known to be induced by TGF-β signaling. In addition, there is a reduced number of IL-22+ cells in actively inflamed tissue in UC patients despite increase of mono-IL-17-producing cells [40]. It is suggested that such decrease of Th22 cells is associated with increased TGF-β expression. This is consistent with the finding that Th22 population was decreased in lamina propria mononuclear cell culture in vitro by stimulation with recombinant TGF-β, whereas anti-TGF-β antibody increased IL-22 production. Loss of Th22 by increased TGF-β may be associated with alterations of mucosal microbiota in the inflamed colonic tissues of UC.
Treg in Animal Models and IBD Patients
There are several animal models that relates to the importance of regulatory T cells for the homeostasis of intestinal mucosal immune system. Both CTLA4 deficient mice and Foxp3 deficient mice develop colitis, and transferring of Treg suppresses colitis in multiple IBD models [10]. These findings suggest that dysfunction or decrease in Treg may cause IBD.
The number of CD4+CD25+FOXP3+ T cells in the peripheral blood of both CD and UC patients is decreased when compared to that of the healthy control [52, 53]. On the other hand, the number of CD4+CD25+FOXP3+ T cells in intestinal mucosa of both CD and UC patients is increased [53, 54]. Furthermore, these Treg from IBD patients can suppress effector T cells in vitro [54]. These findings of either decrease in the effector site or dysfunction of Treg are not observed in IBD patients, and thus they raise doubts regarding the importance of Tregs in the pathogenesis of IBD. However, as compared with other intestinal inflammatory diseases such as diverticulitis, intestinal Treg in IBD patients is decreased [52, 53], and it is thought that there exists an imbalance between Treg and effector T cells in IBD patients.
IL-10 is one of the regulatory cytokines produced by Treg. It is known that IL-10 deficient mice develop colitis. Administration of recombinant IL-10 or transgenic overexpression of IL-10 suppresses colitis in T cell-reconstituted RAG deficient mice. In human , there is a strong association between polymorphism at IL10 locus and UC [55]. Rare alleles of IL10R locus associated with familial enterocolitis [56] have also been reported.
Conclusion
Previously, anti-inflammatory and/or nonspecific immunosuppression drugs have been used to treat IBD. Recently, anti-TNF therapies including chimeric or humanized monoclonal antibody have advanced and revolutionized the disease management. The traditional Th1/Th2 paradigm is augmented by the discovery of other equally important cells and cytokines such as Treg, Th17, Th9, and Th22. Also, follicular helper T cell subset supporting the differentiation and immunoglobulin secretion of B cells has been recently identified [57]. Definitions of such Th subsets have become more complex. However, understanding the role of each Th subset will accelerate the development of new IBD therapies.
References
Abraham C, Cho JH. Inflammatory bowel disease. N Engl J Med. 2009;361(21):2066–78. Review.
Manel N, Unutmaz D, Littman DR. The differentiation of human T(H)-17 cells requires transforming growth factor-beta and induction of the nuclear receptor RORgammat. Nat Immunol. 2008;9(6):641–9.
Hanauer SB, Feagan BG, Lichtenstein GR, Mayer LF, Schreiber S, Colombel JF, et al. Maintenance infliximab for Crohn’s disease: the ACCENT I randomised trial. Lancet. 2002;359(9317):1541–9.
Zenewicz LA, Antov A, Flavell RA. CD4 T-cell differentiation and inflammatory bowel disease. Trends Mol Med. 2009;15(5):199–207. Review.
Maynard CL, Weaver CT. Intestinal effector T cells in health and disease. Immunity. 2009;31(3):389–400. Review.
Weaver CT, Hatton RD, Mangan PR, Harrington LE. IL-17 family cytokines and the expanding diversity of effector T cell lineages. Annu Rev Immunol. 2007;25:821–52. Review.
Yang XO, Pappu BP, Nurieva R, et al. T helper 17 lineage differentiation is programmed by orphan nuclear receptors ROR alpha and ROR gamma. Immunity. 2008;28(1):29–39.
Abraham C, Cho JH. IL-23 and autoimmunity: new insights into the pathogenesis of inflammatory bowel disease. Annu Rev Med. 2009;60:97–110. Review.
Atarashi K, Nishimura J, Shima T, et al. ATP drives lamina propria T(H)17 cell differentiation. Nature. 2008;455(7214):808–12.
Sakaguchi S, Yamaguchi T, Nomura T, Ono M. Regulatory T cells and immune tolerance. Cell. 2008;133(5):775–87. Review.
Neurath MF, Weigmann B, Finotto S, et al. The transcription factor T-bet regulates mucosal T cell activation in experimental colitis and Crohn’s disease. J Exp Med. 2002;195(9):1129–43.
Simpson SJ, Shah S, Comiskey M, et al. T cell-mediated pathology in two models of experimental colitis depends predominantly on the interleukin 12/Signal transducer and activator of transcription (Stat)-4 pathway, but is not conditional on interferon gamma expression by T cells. J Exp Med. 1998;187(8):1225–34.
Berg DJ, Davidson N, Kühn R, et al. Enterocolitis and colon cancer in interleukin-10-deficient mice are associated with aberrant cytokine production and CD4(+) TH1-like responses. J Clin Invest. 1996;98(4):1010–20.
Powrie F, Leach MW, Mauze S, et al. Inhibition of Th1 responses prevents inflammatory bowel disease in scid mice reconstituted with CD45RBhi CD4+ T cells. Immunity. 1994;1(7):553–62.
Kullberg MC, Rothfuchs AG, Jankovic D, et al. Helicobacter hepaticus-induced colitis in interleukin-10-deficient mice: cytokine requirements for the induction and maintenance of intestinal inflammation. Infect Immun. 2001;69(7):4232–41.
Strober W, Fuss IJ, Blumberg RS. The immunology of mucosal models of inflammation. Annu Rev Immunol. 2002;20:495–549. Review.
Boirivant M, Fuss IJ, Chu A, Strober W. Oxazolone colitis: a murine model of T helper cell type 2 colitis treatable with antibodies to interleukin 4. J Exp Med. 1998;188(10):1929–39.
Neurath MF, Fuss I, Kelsall BL, et al. Antibodies to interleukin 12 abrogate established experimental colitis in mice. J Exp Med. 1995;182(5):1281–90.
Heller F, Fuss IJ, Nieuwenhuis EE, et al. Oxazolone colitis, a Th2 colitis model resembling ulcerative colitis, is mediated by IL-13-producing NK-T cells. Immunity. 2002;17(5):629–38.
Brozovic S, Nagaishi T, Yoshida M, et al. CD1d function is regulated by microsomal triglyceride transfer protein. Nat Med. 2004;10(5):535–9.
Izcue A, Hue S, Buonocore S, et al. Interleukin-23 restrains regulatory T cell activity to drive T cell-dependent colitis. Immunity. 2008;28(4):559–70.
Yen D, Cheung J, Scheerens H, et al. IL-23 is essential for T cell-mediated colitis and promotes inflammation via IL-17 and IL-6. J Clin Invest. 2006;116(5):1310–6.
Wiekowski MT, Leach MW, Evans EW, et al. Ubiquitous transgenic expression of the IL-23 subunit p19 induces multiorgan inflammation, runting, infertility, and premature death. J Immunol. 2001;166(12):7563–70.
Elson CO, Cong Y, Weaver CT, et al. Monoclonal anti-interleukin 23 reverses active colitis in a T cell-mediated model in mice. Gastroenterology. 2007;132(7):2359–70.
Fina D, Sarra M, Fantini MC, et al. Regulation of gut inflammation and th17 cell response by interleukin-21. Gastroenterology. 2008;134(4):1038–48.
Ogawa A, Andoh A, Araki Y, et al. Neutralization of interleukin-17 aggravates dextran sulfate sodium-induced colitis in mice. Clin Immunol. 2004;110(1):55–62.
Yang XO, Chang SH, Park H, et al. Regulation of inflammatory responses by IL-17F. J Exp Med. 2008;205(5):1063–75.
Awasthi A, Kuchroo VK. IL-17A directly inhibits TH1 cells and thereby suppresses development of intestinal inflammation. Nat Immunol. 2009;10(6):568–70.
Mudter J, Amoussina L, Schenk M, et al. The transcription factor IFN regulatory factor-4 controls experimental colitis in mice via T cell-derived IL-6. J Clin Invest. 2008;118(7):2415–26.
Lee YK, Turner H, Maynard CL, et al. Late developmental plasticity in the T helper 17 lineage. Immunity. 2009;30(1):92–107.
Gagliani N, Amezcua-Vesely MC, Iseppon A, et al. Th17 cells transdifferentiate into regulatory T cells during resolution of inflammation. Nature. 2015;253(7559):221–5.
Xu L, Kitani A, Fuss I, Strober W. Regulatory T cells induce CD4+CD25−Foxp3− T cells or are self-induced to become Th17 cells in the absence of exogeneous TGF-beta. J Immunol. 2007;178(11):6725–9.
Zhou L, Lopes JE, Chong MM, et al. TGF-beta-induced Foxp3 inhibits T(H)17 cell differentiation by antagonizing RORgamma function. Nature. 2008;453(7192):236–40.
Hoechst B, Gamrekelashvili J, Manns MP, et al. Plasticity of human Th17 cells and iTregs is orchestrated by different subsets of myeloid cells. Blood. 2011;117(24):6532–41.
Darvalhon V, Awasthi A, Kwon H, et al. IL-4 inhibits TGF-beta-induced Foxp3+ T cells, and together with TGF-beta, generates IL-9+ IL-10+ Foxp3− effector T cells. Nat Immunol. 2008;9(12):1347–55.
Veldhoen M, Uyttenhove C, van Snick J, et al. Transforming growth factor-beta ‘reprograms’ the differentiation of T helper 2 cells and promotes an interleukin 9-producing subset. Nat Immunol. 2008;9(12):1341–6.
Licona-Limon P, Henao-Mejia J, Temann AU, et al. Th9 cells drive host immunity against gastrointestinal worm infection. Immunity. 2013;39(4):744–57.
Gerlach K, Hwang Y, Nikolaev A, et al. Th9 cells that express the transcription factor PU.1 drive T cell-mediated colitis via IL-9 receptor signaling in intestinal epithelial cells. Nat Immunol. 2014;15(7):676–86.
Trifari S, Spits H. IL-22producing CD4+ T cells: middle-men between the immune system and its environment. Eur J Immunol. 2010;40(9):2369–71.
Leuing JM, Davenport M, Wolff MJ, et al. IL-22-producing CD4+ T cells are depleted in actively inflamed colitis tissue. Mucosal Immunol. 2014;7(1):124–33.
Zenewicz LA, Yancopoulos GD, Valenzuela DM, et al. Innate and adaptive interleukin-22 protects mice from inflammatory bowel disease. Immunity. 2008;29(6):947–57.
Luci C, Reynders A, Ivanov II, et al. Influence of the transcription factor RORgammat on the development of NKp46+ cell populations in gut and skin. Nat Immunol. 2009;10(1):75–82.
Duerr RH, Taylor KD, Brant SR, et al. A genome-wide association study identifies IL23R as an inflammatory bowel disease gene. Science. 2006;314:1461–3.
Fuss IJ, Neurath M, Boirivant M, et al. Disparate CD4+ lamina propria (LP) lymphokine secretion profiles in inflammatory bowel disease. Crohn’s disease LP cells manifest increased secretion of IFN-gamma, whereas ulcerative colitis LP cells manifest increased secretion of IL-5. J Immunol. 1996;157(3):1261–70.
Monteleone G, Biancone L, Marasco R, et al. Interleukin 12 is expressed and actively released by Crohn’s disease intestinal lamina propria mononuclear cells. Gastroenterology. 1997;112(4):1169–78.
Okazawa A, Kanai T, Watanabe M, et al. Th1-mediated intestinal inflammation in Crohn’s disease may be induced by activation of lamina propria lymphocytes through synergistic stimulation of interleukin-12 and interleukin-18 without T cell receptor engagement. Am J Gastroenterol. 2002;97(12):3108–17.
Mannon PJ, Fuss IJ, Mayer L, et al. Anti-interleukin-12 antibody for active Crohn’s disease. N Engl J Med. 2004;351(20):2069–79.
Abraham C, Cho J. Interleukin-23/Th17 pathways and inflammatory bowel disease. Inflamm Bowel Dis. 2009;15(7):1090–100. Review.
Kamada N, Hisamatsu T, Okamoto S, et al. Unique CD14 intestinal macrophages contribute to the pathogenesis of Crohn disease via IL-23/IFN-gamma axis. J Clin Invest. 2008;118(6):2269–80.
Fuss IJ, Becker C, Yang Z, et al. Both IL-12p70 and IL-23 are synthesized during active Crohn’s disease and are down-regulated by treatment with anti-IL-12 p40 monoclonal antibody. Inflamm Bowel Dis. 2006;12(1):9–15.
Fuss IJ, Heller F, Boirivant M, et al. Nonclassical CD1d-restricted NK T cells that produce IL-13 characterize an atypical Th2 response in ulcerative colitis. J Clin Invest. 2004;113(10):1490–7.
Maul J, Loddenkemper C, Mundt P, et al. Peripheral and intestinal regulatory CD4+ CD25(high) T cells in inflammatory bowel disease. Gastroenterology. 2005;128(7):1868–78.
Himmel ME, Hardenberg G, Piccirillo CA, et al. The role of T-regulatory cells and Toll-like receptors in the pathogenesis of human inflammatory bowel disease. Immunology. 2008;125(2):145–53. Review.
Makita S, Kanai T, Oshima S, et al. CD4+CD25bright T cells in human intestinal lamina propria as regulatory cells. J Immunol. 2004;173(5):3119–30.
Franke A, Balschun T, Karlsen TH, et al. Sequence variants in IL10, ARPC2 and multiple other loci contribute to ulcerative colitis susceptibility. Nat Genet. 2008;40(11):1319–23.
Glocker EO, Kotlarz D, Boztug K, et al. Inflammatory bowel disease and mutations affecting the interleukin-10 receptor. N Engl J Med. 2009;361(21):2033–45.
Tsuji M, Komatsu N, Kawamoto S, et al. Preferential generation of follicular B helper T cells from Foxp3+ T cells in gut Peyer’s patches. Science. 2009;323(5920):1488–92.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Nagaishi, T., Watanabe, M. (2017). Paradigm of T Cell Differentiation in IBD. In: Baumgart, D. (eds) Crohn's Disease and Ulcerative Colitis. Springer, Cham. https://doi.org/10.1007/978-3-319-33703-6_14
Download citation
DOI: https://doi.org/10.1007/978-3-319-33703-6_14
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-33701-2
Online ISBN: 978-3-319-33703-6
eBook Packages: MedicineMedicine (R0)