
Abstract
Hemangioblastomas are highly vascular tumors that are typically benign and slow-growing, corresponding to WHO grade I.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Overview
-
Hemangioblastomas are highly vascular tumors that are typically benign and slow-growing, corresponding to WHO grade I.
-
Sporadic occurrence is most common, or they may occur in the context of Von Hippel-Lindau (VHL) syndrome.
-
Historically, they have also been referred to as capillary hemangioblastomas. The stromal cell is clearly the neoplastic component in these tumors, but the underlying cell of origin has yet to be determined.
2 Clinical Features
-
Hemangioblastomas are u ncommon CNS tumors that occur in all age groups, most frequently arising in adults. They often present in children when associated with VHL. No gender predilection is apparent.
-
Clinical signs and symptoms are most often encountered with large tumors and are related to mass effect either from the tumor itself, from expansion of an accompanying cyst, or from peritumoral edema. Intracranial examples may cause ataxia, dysmetria, or hydrocephalus with signs and symptoms of increased intracranial pressure. Spinal tumors often cause radiculopathies, pain, or both.
-
Tumor production of erythropoietin may lead to polycythemia.
-
Spontaneous hemorrhage has occasionally been documented.
3 Neuroimaging
-
Sporadic hemangioblastomas most often arise within the cerebellar hemispheres, whereas those arising within the context of VHL may occur anywhere within the CNS, including the brainstem or cerebellopontine angle, spinal cord, cranial nerves, or nerve roots.
-
Supratentorial localization is uncommon; unusual sites of occurrence include the pineal region, filum terminale, and extraneural locations. Tumor multiplicity may be encountered in VHL patients.
-
Neuroimaging studies typically demonstrate a cystic lesion with a heterogeneously contrast-enhancing mural nodule (Fig. 13.1A).
Fig. 13.1 
Hemangioblastoma. ( A ) An axial T1-weighted post-gadolinium MR image shows a classic posterior fossa loca tion with a cyst bearing an enhancing mural nodule. (B ) A T2-weighted image of same patient shows hyperintense cyst fluid and a solid nodule of heterogeneous intensity with scattered flow voids. (C ) An axial apparent diffusion coefficient (ADC) map shows a high signal corresponding to this tumor
-
Solid portions of tumor are isointense on T1 and hyperintense on T2-weighted MR images (Fig. 13.1B and 13.2A). High signal on apparent diffusion coefficient (ADC) mapping is typical (Fig. 13.1C).
Fig. 13.2 
Hemangioblastoma. (A) Sagittal T2-weighted MR image shows a heterogeneously hyperintense hema ngioblastoma arising in the cervical cord. (B) Angiography confirms an arteriovenous malformation (AVM)–like tangle of vessels within the lesion
-
Flow voids corresponding to large vessels may be encountered, and angiography often shows a tangle of vessels resemblin g an arteriovenous malformation (AVM) (Fig. 13.2B).


4 Pathology
-
Gross pathology
-
◦ Resection specimens are typica lly composed of firm, fleshy to overtly hemorrhagic tissue, often with grossly visible vascular spaces (Fig. 13.3).
Fig. 13.3 
Hemangioblasto ma. (A) Intraoperative view of a cervicomedullary fleshy, red nodule with adjacent cyst and large feeder vessels. (B) Cut surface of a hemangioblastoma surgical specimen from a different patient shows firm, red-brown hemorrhagic tissue with variably sized vascular spaces
-
-
Intraoperative cytologic imprints or smears
-
◦ Intraoperative smears and samples of cystic fluid often contain blood along with abundant stromal cells wit h hyperchromatic nuclei and lacelike vacuolated cytoplasm (Fig. 13.4).
Fig. 13.4 
Cytologic smear pre paration (H&E) showing sheets of cells with abundant, sometimes vacuolated cytoplasm with hyperchromatic nuclei of variable configuration
-
◦ Small vessels, stripped endothelial cells, macrophages, and calcified material may also be present.
-
-
Histology
-
◦ Hemangioblastomas are composed of a combination of stromal cells and a rich vascular network.
-
The stromal cells, representing the neoplastic component of this lesion, vary in their morphologic appearance. They characteristically contain small, bland nuclei and abundant vacuolated, lipid-rich cytoplasm (Fig. 13.5A and B). Occasionally, they may have a more spindled morphology with less obvious cytoplasmic vacuolization and/or more prominent nuclear pleomorphism (Fig. 13.5C and D).
Fig. 13.5 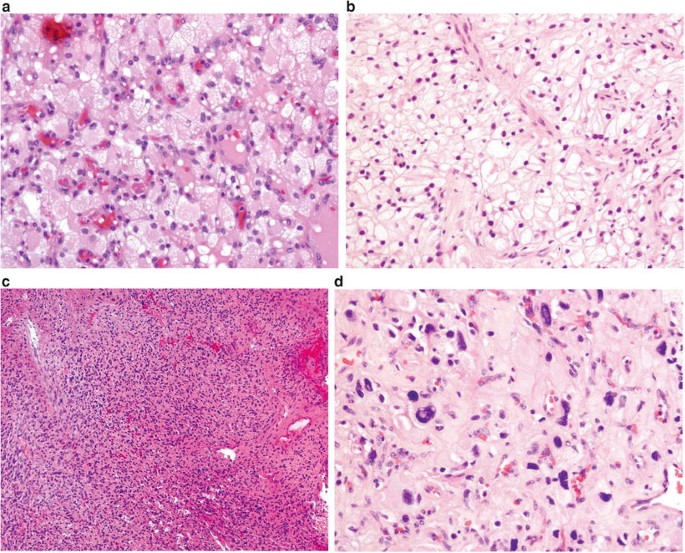
Stromal cells of h emangioblastoma characteristically have small bland nuclei and abundant vacuolated cytoplasm (A); one may also encounter cells resembling clear cell renal cell carcinoma (B), spindle cell morphology (C), or cells with striking nuclear pleomorphism (D)
-
The vascular component consists of numerous capillaries sprinkled throughout the tumor, together with scattered larger feeding (and draining) vessels.
-
Either of these two components may be a predominant feature; abundant vasculature (Fig. 13.6A), intratumoral hemorrhage, or extensive sclerosis may significantly mask the stromal cell component.
Fig. 13.6 
(A) Abundant vasculat ure in this hemangioblastoma effectively masks the diagnostic stromal cells. (B) Hemangioblastomas characteristically harbor a rich reticulin network
-
A reticulin-rich network is invariably present (Fig. 13.6B). It is especially prominent in the highly vascular reticular variant, notable for small, compact nests of stromal cells. In the cellular variant, broad sheets of stromal cells are uninterrupted by reticulin.
-
Mitotic figures are uncommon.
-
Mast cells and extramedullary hematopoiesis are frequently present.
-
These lesions are sharply demarcated with the surrounding brain, often showing a striking surrounding astrogliosis that may mimic a pilocytic astrocytoma, replete with Rosenthal fibers and eosinophilic granular bodies.
-
-




5 Immunohistochemistry
-
The stromal cell and vascula r components show significantly different immunoexpression patterns:
-
◦ Stromal cells are consistently positive for vimentin, alpha inhibin, D2-40, and aquaporin, and variably positive for S-100, NCAM, neuron-specific enolase (NSE), erythropoietin, EGFR, VEGF, alpha-1-antitrypsin, and antichymotrypsin (Fig. 13.7A–C). Progesterone receptor and factor Xllla positivity have also been reported in a high percentage of cases. They may be focally positive for glial fibrillary acidic protein (GFAP), keratin, epithelial membrane antigen (EMA), or desmin. Specific neuronal markers (neurofila ment, synaptophysin, and chromogranin) and endothelial cell markers (CD31, CD34, and VWF) are typically negative.
Fig. 13.7 
Stromal cells of hemangioblastoma are diffusely positive for vimentin (A) and variably positive for S-100 (B) and neu ron-specific enolase (NSE) (C). CD31-positive vessels (D) stand out from the background of nonstaining stromal cells
-
◦ Endothelial cells are consistently positive for CD31, CD34, and VWF (Fig. 13.7D).
-

6 Electron Microscopy
-
At the ultrastructural level, hemangioblastomas contain three cell types: endothelial cells lining fenestrated vascular channels, pericytes ensheathed by basal lamina, and stromal cells. Stromal cells often contain lipid droplets and may contain intracellular caveolae consistent with early capillary lumina, or small Weibel-Palade bodies.
-
Transitional forms of these three cellular constituents may be present.
7 Molecular Pathology
-
Whereas germline mutatio ns of the VHL gene are the norm in familial (VHL disease–associated) hemangioblastoma, loss or inactivation of this gene also occurs in up to 50 % of sporadic cases.
-
Recent studies have indicated that inactivation of the ZAC1 gene (6q24-25) may also play a role in the development of hemangioblastoma, particularly non–VHL-associated cases.
8 Differential Diagnosis
-
Clear cell renal cell carcinoma (RCC) is an important diagnostic consideration, particularly in VHL patients who may have both hemangioblastoma and RCC.
-
◦ Both tumors contain cells with clear, lipid-rich cytoplasm with variable vascular investments, though the cells of RCC tend to have more monotonous nuclear profiles and less reticulin positivity than hemangioblastoma.
-
◦ Definitive diagnosis typically relies upon demonstration of immunopositivity for markers such as D2-40, inhibin, and aquaporin 1 in hemangioblastoma, and for CD10, RCC, EMA, and cytokeratin AE1/AE3 in RCC.
-
◦ More recently, PAX2 and PAX8 (positive in RCC) in conjunction with inhibin (positive in hemangioblastoma) have been shown to be an effective panel in distinguishing these two entities.
-
-
Several meningioma vari ants may mimic hemangioblastoma, especially the microcystic, clear cell, and angiomatous subtypes, as well as those with xanthomatous areas.
-
◦ Unlike hemangioblastoma, all of these meningiomas are expected to show diffuse EMA and claudin positivity and should lack expression of the multiple markers of hemangioblastoma listed above.
-
◦ A negative brachyury (positive in hemangioblastoma) may also be useful in differentiating clear cell meningioma from hemangioblastoma.
-
-
Hemangioblastoma may mimic intraparenchymal vascular lesions, especially capillary hemangioma; the latter will lack vacuolated stromal cells.
-
Macrophages may closely resemble the bubbly stromal cells of hemangioblastoma; CD68 will confirm the identity of the macrophages.
9 Prognosis
-
Surgical resection is the treatment of choice and affords excellent recurrence-free and overall survival outcomes.
-
Management of hemangioblastoma in VHL patients is more difficult, given the tendency of these patients to develop multiple lesions.
-
Lifelong follow-up is required, with treatment indicated for symptomatic lesions and also for those asymptomatic tumors exhibiting radiographic progression.
-
Fractionated external beam radiotherapy may be helpful in those patients with extensive intracranial and/or spinal disease, and in treating residual or recurrent lesions.
-
Tumor emboliza tion in select cases may facilitate complete resection with reduced blood loss.
Suggested Reading
Barresi V, Vitarelli E, Branca V, Antonelli M, Giangaspero F, Barresi G. Expression of brachyury in hemangioblastoma: potential use in differential diagnosis. Am J Surg Pathol. 2012;36:1052–7.
Carney E, Banerjee P, Ellis C, Albadine R, Sharma E, Chaux A, et al. PAX2(−)/PAX8(−)/Inhibin A(+) immunoprofile in hemangioblastoma: a helpful combination in the differential diagnosis with metastatic clear cell renal cell carcinoma to the central nervous system. Am J Surg Pathol. 2011;35:262–7.
Chaudhry AP, Montes M, Cohn GA. Ultrastructure of cerebellar hemangioblastoma. Cancer. 1978;42:1834–50.
Conway JE, Chou D, Clatterbuck RE, Brem H, Long DM, Rigamonti D. Hemangioblastomas of the central nervous system in von Hippel-Lindau syndrome and sporadic disease. Neurosurgery. 2001;48:55–62.
Glasker S. Central nervous system manifestations in VHL: genetics, pathology and clinical phenotypic features. Fam Cancer. 2005;4:37–42.
Jagannathan J, Lonser RR, Smith R, DeVroom HL, Oldfield EH. Surgical management of cerebellar hemangioblastomas in patients with von Hippel-Lindau disease. J Neurosurg. 2008;108:210–22.
Koh ES, Nichol A, Millar BA, Menard C, Pond G, Laperriere NJ. Role of fractionated external beam radiotherapy in hemangioblastoma of the central nervous system. Int J Radiat Oncol Biol Phys. 2007;69:1521–6.
Lach B, Gregor A, Rippstein P, Omulecka A. Angiogenic histogenesis of stromal cells in hemangioblastoma: ultrastructural and immunohistochemical study. Ultrastruct Pathol. 1999;23:299–310.
Lallu S, Naran S, Palmer D, Bethwaite P. Cyst fluid cytology of cerebellar hemangioblastoma: a case report. Diagn Cytopathol. 2008;36:341–3.
Lemeta S, Jarmalaite S, Pylkkanen L, Bohling T, Husgafvel-Pursiainen K. Preferential loss of the nonimprinted allele of ZAC1 tumor suppressor gene in human capillary hemangioblastoma. J Neuropathol Exp Neurol. 2007;66:860–7.
Rodesch G, Gaillard S, Loiseau H, Brotchi J. Embolization of intradural vascular spinal cord tumors: report of five cases and review of the literature. Neuroradiology. 2008;50:145–51.
Roy S, Chu A, Trojanowski JQ, Zhang PJ. D2-40, a novel monoclonal antibody against the M2A antigen as a marker to distinguish hemangioblastomas from renal cell carcinomas. Acta Neuropathol (Berl). 2005;109:497–502.
Weinbreck N, Marie B, Bressenot A, Montagne K, Joud A, Baumann C, et al. Immunohistochemical markers to distinguish between hemangioblastoma and metastatic clear-cell renal cell carcinoma in the brain: Utility of aquaporin1 combined with cytokeratin AE1/AE3 immunostaining. Am J Surg Pathol. 2008;32:1051–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing AG
About this chapter
Cite this chapter
Richard, H.T., Fuller, C.E. (2016). Hemangioblastoma. In: Adesina, A., Tihan, T., Fuller, C., Poussaint, T. (eds) Atlas of Pediatric Brain Tumors. Springer, Cham. https://doi.org/10.1007/978-3-319-33432-5_13
Download citation
DOI: https://doi.org/10.1007/978-3-319-33432-5_13
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-33430-1
Online ISBN: 978-3-319-33432-5
eBook Packages: MedicineMedicine (R0)