
Abstract
Alphaviruses are geographically restricted enveloped, single-strand, message-sense RNA viruses. Alphaviruses are maintained in natural cycles between vertebrate and invertebrate hosts and are transmitted to vertebrates through the bite of an infected mosquito. Eastern equine encephalitis, western equine encephalitis, and Venezuelan equine encephalitis viruses are the neurotropic alphaviruses of greatest importance as causes of human encephalomyelitis and were initially recognized for their ability to cause disease in horses. Alphaviruses primarily associated with rash and arthritis can also cause neurologic disease. Infection with Chikungunya virus has caused encephalitis in humans and Semliki Forest virus and Sindbis virus provide important mouse models for alphavirus encephalomyelitis. Brain and spinal cord neurons are the primary target cells and infection induces a mononuclear inflammatory response. Clearance of infectious virus is rapid and noncytolytic through the actions of antibody and interferon-γ, but viral RNA and proteins are cleared slowly. Diagnosis is usually made by detection of viral RNA or antiviral IgM. No licensed vaccines or treatments are available.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Eastern equine encephalitis virus
- Western equine encephalitis virus
- Chikungunya virus
- Sindbis virus
- Viral encephalomyelitis
- Virus clearance
- Neuronal infection
Introduction
Alphaviruses are members of the Togaviridae family of icosahedral, enveloped, single-strand, message-sense RNA viruses. Eastern equine encephalitis (EEE), western equine encephalitis (WEE), and Venezuelan equine encephalitis (VEE; “Venezuelan Equine Encephalitis” chapter) viruses are the neurotropic alphaviruses of greatest importance as causes of human encephalomyelitis and were initially recognized for their ability to cause disease in horses. Alphaviruses primarily associated with rash and arthritis can also cause neurologic disease. Infection with Chikungunya virus (CHIKV) has caused encephalitis in humans and Semliki Forest virus and Sindbis virus (SINV) provide important mouse models for alphavirus encephalomyelitis. This chapter will cover infection with EEEV , WEEV, CHIKV, and SINV.
EEEV was first isolated in 1933 from the brains of horses during an epizootic of equine encephalitis in Virginia and New Jersey and was demonstrated to cause human encephalitis in 1938 (Ten Broeck and Merrill 1933; Webster and Wright 1938). In the summer of 1930 a similar equine epizootic occurred in the San Joaquin Valley of California and WEEV was isolated from the brains of affected horses, followed in 1938 by recovery of the same virus from the brain of a child with fatal encephalitis (Meyer et al. 1931; Howitt 1938). A related WEEV complex virus, Highlands J virus (HJV), was isolated in the eastern part of the USA in 1952 (Hayes and Wallis 1977).
SINV was first isolated in 1952 from mosquitoes collected near Sindbis, Egypt. Humans living in the Nile Delta at that time had a SINV seroprevalence of 27 %, but no disease was associated with infection (Taylor et al. 1955). The first human isolates of SINV were in 1961 from the blood of febrile patients in Uganda and in 1963 SINV was recognized as a cause of rash and arthritis in South Africa (Malherbe et al. 1963) and was developed as a mouse model of encephalomyelitis in 1965 (Johnson 1965). However, the first clear association of an alphavirus with arthritic disease was in 1953 when CHIKV was isolated from the sera of individuals in Tanzania with severe arthritis (Ross 1956). CHIKV neurologic disease began to be reported soon thereafter during outbreaks in India and Thailand (Nimmannitya et al. 1969; Thiruvengadam et al. 1965).
Natural Cycles of Infection, Transmission, and Evolution
Alphaviruses are maintained in a natural cycle between vertebrate and invertebrate hosts. The primary mode of transmission to vertebrates is through the bite of an infected mosquito. Mosquitoes become infected by feeding on a viremic host, are able to transmit the virus 4–10 days later (external incubation), and remain persistently infected. Mosquito virus titers in saliva are highest early after the mosquito is infected and decline, along with transmission rates, after 1–2 weeks. Maintenance of this cycle requires an amplifying host that develops a viremia of sufficient magnitude to infect feeding mosquitoes. For many alphaviruses humans are dead-end hosts with low-titered viremias.
Eastern equine encephalitis—EEEV is enzootic in the Americas along the Atlantic and Gulf coasts from eastern Canada to northern Argentina, in the Caribbean and in Central America (Gibney et al. 2011; Weaver et al. 2012; Carrera et al. 2013; Lubelczyk et al. 2013). Inland foci exist around the Great Lakes extending to South Dakota and Quebec (Chenier et al. 2010). Birds are the primary reservoir host and many avian species are susceptible to infection (Kissling et al. 1954). In North America the primary enzootic cycle is maintained in shaded swamps with the ornithophilic mosquito Culiseta melanura as the vector (Cupp et al. 2003; Scott and Weaver 1989). The amplifying species are wading birds, passerine birds, and starlings (Dalrymple et al. 1972; Estep et al. 2013; Molaei et al. 2013) and reptiles may be over-wintering hosts (Bingham et al. 2012; White et al. 2011). Outbreaks of equine and human encephalitis are facilitated when the virus spreads from the enzootic cycle into mosquito populations that feed on a variety of hosts (Mitchell et al. 1992; Cupp et al. 2003; Scott and Weaver 1989).
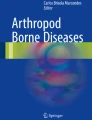
Small numbers of human cases of EEE are diagnosed in the USA each year (Fig. 1). There is no evidence that either horses or humans are important in the transmission cycle during epizootics. In South America, EEEV is enzootic along the north and east coasts and in the Amazon Basin. Sequence comparisons indicate that EEEV has evolved independently in North and South America with one subtype in North America and the Caribbean and three subtypes in South America (Brault et al. 1999). North American isolates are highly conserved, differing by less than 3 % in nucleotide sequence. The three South American subtypes diverged 1000–2000 years ago, are evolving locally with small mammals as reservoir hosts, and differ by up to 25 % in nucleotide sequence (Arrigo et al. 2010).

Numbers of human cases of eastern equine encephalitis reported annually in the United States since 1964. Data are from the Centers for Disease Control and Prevention
Western equine encephalitis—WEEV is endemic in the western portions of the United States and Canada and in South America. In North America WEEV is maintained in an endemic cycle involving domestic and passerine birds and Culex tarsalis, a mosquito adapted to irrigated agricultural areas (Calisher 1994). HJV is enzootic on the East Coast of the United States and is maintained in a cycle similar to that of EEEV with Cs. melanura the primary vector and migrating birds the primary reservoir. HJV can occasionally cause encephalitis in horses (Karabatsos et al. 1988) and is a recognized pathogen for turkeys, pheasants, partridges, ducks, emus, and whooping cranes (Ficken et al. 1993; Weaver et al. 1999).
WEEV in North America has caused seasonal epidemics of encephalitis in humans, horses, and emus. Major epizootics occurred every 2–3 years from 1931 to 1952 with attack rates up to 167/100,000 population (Calisher 1994). An average of 34 human cases of WEE occurred per year in the USA from 1955 to 1984, but numbers of cases have steadily declined with the last documented case in 1998 (Fig. 2). In rural areas of California endemic for WEEV seroprevalence in humans was 34 % in 1960 and 1.3–2.6 % in 1993–1995 (Froeschle 1964; Reisen and Chiles 1997). The reasons for this decline are not clear, but there is no evidence that it is due to a change in virus virulence or vector competence (Zhang et al. 2011; Reisen et al. 2008; Forrester et al. 2008).

Numbers of human cases of western equine encephalitis reported annually in the United States since 1964. Data are from the Centers for Disease Control and Prevention
WEEV is the result of a recombination between EEEV and a Sindbis-like virus (Hahn et al. 1988). There are four major lineages; two in South America and two widely distributed in the Americas and the Caribbean (Weaver et al. 1997; Bergren et al. 2014). The WEEV complex also includes HJV, Fort Morgan virus (FMV), and Aura virus (Calisher et al. 1988). HJV and FMV belong to lineages that diverged since recombination while Aura is a “pre-recombinant” virus (Allison et al. 2015; Cilnis et al. 1996). Sequence analysis of the viruses found at the initial focus of a 1982 WEE epizootic in Argentina indicated that the enzootic virus was the source of a virulent variant that emerged to cause the epizootic (Bianchi et al. 1993). The lack of significant human disease during equine outbreaks of WEE in South America may be related to the feeding habits of the vector or to a difference in virulence of South American strains of WEEV for humans and horses (Sabattini et al. 1985).
Chikungunya—In addition to Sub-Saharan Africa, CHIKV has caused large outbreaks of disease in India, Asia, and most recently on islands in the Indian Ocean and Caribbean and in South America (Carey et al. 1969; Halstead et al. 1969; Powers 2015; Renault et al. 2007). In Africa, the virus is maintained in a sylvatic cycle involving Aedes africanus and Ae. furcifer and nonhuman primates as well as an urban mosquito–human–mosquito cycle involving Ae. aegypti or Ae. albopictus. In India and Southeast Asia there is no evidence for a sylvatic cycle; transmission to humans in urban areas is by Ae. aegypti and in rural areas by Ae. albopictus (Ho et al. 2011; Powers et al. 2000). Three distinct lineages of CHIKV have been identified: West African; East, Central, and South African (ECSA); and Asian (Powers et al. 2000; Powers 2015). A mutation that results in an amino acid A226V substitution in the E1 protein of the ECSA genotype increased the efficiency of Ae. albopictus infection and likely facilitated the recent widespread outbreaks of disease in regions where Ae. aegypti is not prevalent (Vazeille et al. 2007; Hapuarachchi et al. 2010; Tsetsarkin et al. 2007).
Sindbis virus—SINV is a widespread alphavirus that has been isolated in Europe, India, Asia, Australia, and the Philippines from a variety of mosquito and vertebrate species (Lundstrom 1999; Lundstrom and Pfeffer 2010). The virus is maintained in a cycle between Culex spp. or Culiseta spp. mosquitoes and wild birds (Mackenzie et al. 1994). Five genotypes have been identified (Lundstrom and Pfeffer 2010) with clinical disease primarily in South Africa and northern Europe where it is known as Ockelbo disease, Pogosta disease, or Karelian fever (Espmark and Niklasson 1984; Jupp et al. 1986; Laine et al. 2004).
The Virus, Its Life Cycle, and Cellular Effects
Alphavirus virions are 60–70 nm in diameter and the RNA genome is composed of approximately 11,700 nucleotides, capped and polyadenylated. Multimers of a single capsid (C) protein arranged as an icosahedron with T = 4 symmetry are enclosed in a lipid envelope that is derived from the host cell plasma membrane and contains the viral-encoded glycoproteins, E1 and E2. E1-E2 heterodimers are grouped as trimers to form 80 spikes on the virion surface. E2 is involved in attachment to cellular receptors, while E1 forms a relatively flat skirt-like structure close to the virion surface and is important for fusion of the virus and cell membranes to initiate infection (Zhang et al. 2002; Li et al. 2010).
Binding of virus to the cell surface and entry into the cell is a multistep process that is dependent on E1 and E2 viral glycoproteins, cell surface molecules, low pH in the endosome, and fusion of membrane lipids. Variations in any of these components will affect the efficiency of infection and the likelihood that any particular cell will become infected in vivo. Because alphaviruses infect a wide range of hosts, often including birds, reptiles, mammals, and mosquitoes, they must either use an evolutionarily well-conserved cell surface molecule or multiple molecules as receptors for initiation of infection. None of the many receptors identified to date appears to be used exclusively, suggesting the possibility of several receptors. Alternatively, alphaviruses may use receptor–coreceptor combinations to achieve wide host range and the specific tropisms observed in vivo. The receptor important for alphavirus binding and entry into neurons is unknown.
Initial binding is often through glycosaminoglycans (GAGs) , negatively charged unbranched carbohydrates of repeating disaccharides found on the surface of most cells (Silva et al. 2014). In cell culture, basic amino acids in the E2 glycoprotein that increase the efficiency of virus attachment to cells through GAGs are rapidly selected (Klimstra et al. 1998). Improved GAG binding generally increases clearance from the blood and decreases virulence for mice after peripheral inoculation (Byrnes and Griffin 2000). However, natural isolates of EEEV are dependent on GAGs for infection of cells that correlate with neurovirulence (Gardner et al. 2011).
Entry requires endocytosis followed by a conformational change in the trimer of E1-E2 heterodimers induced by exposure to low pH (Helenius et al. 1980; White and Helenius 1980; Sanchez-San Martin et al. 2009). This conformational change results in dissociation of E2 from E1, formation of E1 trimers, fusion of the viral envelope with the endosomal membrane, and delivery of the nucleocapsid into the cytoplasm (Wahlberg et al. 1992; Wahlberg and Garoff 1992). Cholesterol and sphingomyelin are required for E1 binding and membrane fusion. Amino acid changes in E1 can affect the fusion capacity, the lipid requirements for the target cell membrane, and the optimal pH for fusion (Boggs et al. 1989; Chatterjee et al. 2002).
The genome is released from the nucleocapsid by ribosomal removal of C and then translated (Singh and Helenius 1992). The 5′ two-thirds of the message-sense genome encodes four nonstructural proteins (nsPs) that function in replication of the viral RNA and production of the subgenomic RNA (Strauss and Strauss 1994). nsPs are translated from genomic RNA as two polyproteins (P123 and P1234) that form replication complexes tethered to cytoplasmic vacuoles that are formed from modified endosomal membranes. The polyproteins are processed into individual proteins by a papain-like protease in the C-terminal portion of nsP2. NsP1 has methyl transferase and guanylyltransferase activities, is palmitoylated and binds the replication complex to membranes. The N-terminal domain of nsP2 has helicase, ATPase, GTPase, methyl transferase, and 5′-triphosphatase activity. nsP3 is a phosphoprotein that induces membrane remodeling necessary for the formation of cytoplasmic vacuoles. nsP4 is the RNA-dependent-RNA polymerase and in vivo viral fitness is dependent on its error-prone properties (Coffey et al. 2011).
RNA transcription is initiated by synthesis of a full-length minus-strand that then serves as the template for the synthesis of both subgenomic mRNA and genomic RNA. Replication complexes are formed as spherules at the plasma membrane and are then internalized to form a stable cytoplasmic compartment (Frolova et al. 2010; Spuul et al. 2010). RNA synthesis is regulated by sequential processing of the nsPs (Frolov et al. 2001). Early in infection, nsP2 cleaves P1234 into the minus-strand replicase, P123 plus nsP4. Later, P123 is cleaved into nsP1, nsP2, and nsP3 that changes the template specificity of the replicase to increase synthesis of plus strands and to shut off synthesis of minus strands. Only fully cleaved nsP1 + nsP2 + nsP3 + nsP4 complexes are functional in 26S RNA synthesis (Hardy and Strauss 1989; Shirako and Strauss 1994; Lemm et al. 1994).
The 26S subgenomic RNA is the mRNA for translation of the structural proteins (Strauss and Strauss 1994). Five potential structural proteins (C, E3, E2, 6K, and E1) are encoded in the subgenomic RNA as a polyprotein and an additional transframe protein (TF) is produced by −1 ribosomal frameshifting within the 6K coding region (Firth et al. 2008). C is autoproteolytically cleaved from the nascent chain and is rapidly assembled with genomic RNA into nucleocapsids. Precursor of E2 (PE2, E3 + E2), 6K, and E1 are synthesized in association with the endoplasmic reticulum. The cysteine-rich E3 protein serves as the signal sequence for E2, a transmembrane protein that has two or three N-linked glycosylation sites and contains the most important epitopes for neutralizing antibody. The cytoplasmic portion of E2 has a second stretch of hydrophobic amino acids that tethers it to the inner surface of the membrane. The 6K protein is the signal peptide for E1 and TF is an 8K protein important for assembly that is incorporated into the virion in small amounts (Snyder et al. 2013).
PE2 and E1 are transported as a noncovalently associated hetero-oligomeric complex through the cell secretory pathway to the plasma membrane. Late in the pathway PE2 is processed by a furin-like protease to E2 and E3, which is shed from the cell surface. The N-terminal portion of C is conserved, basic, and presumed to bind the viral genomic RNA while the C-terminal portion interacts with the cytoplasmic tail of E2 and with other copies of the C protein to form the nucleocapsid. At the plasma membrane, the specific association of E2 tails with nucleocapsids initiates a budding process that leads to the release of mature virions (Jose et al. 2009).
Alphaviruses replicate rapidly in most vertebrate cell lines with the release of progeny virus within 4–6 h after infection. Infection causes extensive cytopathic effect characterized by cell rounding, shrinkage, and cytoplasmic blebbing with apoptotic death of infected cells within 24–48 h. Viral proteins are concentrated in the surface blebs from which budding continues to occur. This process does not hamper, and may enhance, virus replication because inhibition of apoptosis usually decreases virus yield (Levine et al. 1993, 1996; Dhanwani et al. 2012).
Apoptosis of cultured cells can be initiated during SINV fusion when membrane-bound sphingomyelinases are activated releasing ceramide, an efficient inducer of cellular apoptosis (Jan and Griffin 1999; Jan et al. 2000). Subsequent early events include activation of poly(ADP ribose) polymerase and cellular caspases, cleavage of caspase-3 substrates and fragmentation of chromosomal DNA (Nargi-Aizenman et al. 2002; Ubol et al. 1996). Alphavirus-induced apoptosis can be slowed or prevented, often in virus strain- and cell type-dependent ways, by expression of ceramidase, expression of a dominant inhibitory form of Ras, inhibition of constitutive expression of NFkB, overexpression of Bcl-2 family member and interacting proteins (Liang et al. 1998; Lewis et al. 1999), phosphorylation of PKCδ, and inhibition of caspase activity (Jan et al. 2000; Joe et al. 1996).
Alphavirus-induced vertebrate cell death can also occur by nonapoptotic mechanisms. Alphaviruses efficiently shut down host protein and mRNA synthesis (Gorchakov et al. 2005), deplete NAD and energy stores (El-Bacha et al. 2004; Ubol et al. 1996), and induce dysfunction of Na+K+ATPase causing loss of membrane potential and altered intracellular cation concentrations (Bashford et al. 1985; Ulug et al. 1989). In vivo, immature neurons die by apoptosis, but mature neurons are more resistant to apoptotic cell death. In particular, mature motor neurons become pale and swollen and are not protected from death by Bcl-2 family member proteins (Havert et al. 2000; Kerr et al. 2002).
Clinical Disease in Humans
Eastern equine encephalitis—North American strains of EEEV are the most virulent of the encephalitic alphaviruses and cause high mortality in all age groups (Calisher 1994). South American strains usually cause only mild human disease, but encephalitis has recently been documented (Causey et al. 1961; Carrera et al. 2013). A prodromal illness consisting of 1–2 weeks of fever, chills, malaise, and myalgias begins days after the bite of an infected mosquito. In cases of encephalitis these prodromal symptoms are followed by the onset of headache, confusion, vomiting, restlessness, and irritability leading to seizures, obtundation, and coma. Children are most susceptible with 1 in 8 infections resulting in encephalitis compared with 1 in 23 infections in adults (Goldfield et al. 1968). Meningismus is frequent as are focal signs including cranial nerve palsies and paralysis. Hyponatremia due to inappropriate secretion of antidiuretic hormone is a common complication. The case-fatality rate is 30–40 %, with the highest rates in children and the elderly. Death typically occurs within 2–10 days after onset of encephalitis (Silverman et al. 2013; Deresiewicz et al. 1997; Feemster 1957).
CSF is almost always abnormal. Pressure and protein are increased, glucose is low to normal, red blood cells and xanthochromia are commonly present, and white cell counts range from 10 to 2000/μL. Polymorphonuclear leukocytes may be abundant early with a shift to mononuclear cells over the first few days. Electroencephalograph (EEG) abnormalities are relatively nonspecific, usually showing slowing. Computed tomographic (CT) scans may be normal or show only edema. Magnetic resonance imaging (MRI) scans are more often abnormal with focal lesions most commonly observed in the thalamus, basal ganglia, and brain stem (Silverman et al. 2013; Deresiewicz et al. 1997).
Poor outcome is predicted by high CSF white cell count or severe hyponatremia, not by the size of the radiographic lesions. Recovery is more likely in individuals who have a long (5–7 day) prodrome and do not develop coma. Sequelae, including paralysis, seizures, and cognitive impairment, are common and 35–80 % of survivors, particularly children, have significant long-term neurological problems (Silverman et al. 2013; Przelomski et al. 1988; Deresiewicz et al. 1997; Feemster 1957).
Western equine encephalitis—WEEV causes encephalitis with signs and symptoms similar to those of EEEV, but with a lower case fatality rate of 3 %. There is a 3–5 day prodrome of fever and headache that may progress to restlessness, tremor, irritability, nuchal rigidity, photophobia, altered mental status, and paralysis. CSF pleocytosis is typical with 100–1500 cells/μL. Neutrophils are present early in disease and mononuclear cells later. Infants often present with rigidity, seizures, and a bulging fontanel. Transplacental transmission results in perinatal infection manifesting within the first week of life as fever, failure to feed, and seizures (Finley et al. 1955; Longshore et al. 1956; Kokernot et al. 1953).
Clinically apparent disease is most common in the very young and those over 50. The estimated case to infection ratio is 1:58 in children under 5 years and 1:1150 in adults. In older children and adults, males are 2–3 times more likely to develop disease than females. Infants and young children are more likely to develop seizures, fatal encephalitis, and significant sequelae. In infants less than 1 year approximately 60 % of survivors have brain damage, and in some the disease is progressive. In older individuals recovery is typically rapid with remission of signs and symptoms within 5–10 days, and sequelae are less common (Longshore et al. 1956; Calisher 1994; Kokernot et al. 1953; Finley et al. 1955; Noran 1944).
Chikungunya—Arthralgia with or without rash occurs in approximately 85 % of those infected (Gerardin et al. 2008) and CNS disease occurs in 16 % (Chandak et al. 2009). Neurologic manifestations are most common in children and the elderly. Encephalitis, meningitis, seizures, encephalopathy, myelopathy, and peripheral neuropathy have been observed. There is a case-fatality rate of up to 5 % and neurologic sequelae are common in those that survive (Robin et al. 2008; Renault et al. 2007). MRI abnormalities may or may not be present and the EEG abnormalities are not specific. Cerebrospinal fluid is usually unremarkable, but viral RNA can often be detected by RT-PCR (Arpino et al. 2009; Tandale et al. 2009; Chandak et al. 2009; Robin et al. 2008).
Pathogenesis and Determinants of Outcome
The initial sites of virus replication probably vary with the virus and host. Mice have received most extensive study (Taylor et al. 2015). After subcutaneous inoculation alphaviruses may infect skeletal muscle, fibroblasts or macrophages at the local site or enter Langerhans cells in the skin (Gardner et al. 2010; Morrison et al. 2011; Couderc et al. 2008; Johnson 1965). Infection of antigen-presenting cells in the skin may be the most common mode of initiating natural mosquito-transmitted infection followed by transport of virus to the draining lymph node.
Initial replication is followed by a substantial plasma viremia in amplifying hosts and hosts susceptible to disease. The ability to sustain a viremia is dependent on the continued efficient production of virus at a primary site of replication, delivery of virus into the vascular system, and slow clearance from the blood. In mice, muscle, secondary lymphoid tissue, cardiac myocytes, osteoblasts, brain and spinal cord neurons and brown fat cells are frequent secondary sites of replication (Aguilar 1970; Liu et al. 1970; Monath et al. 1978). The ability to invade target organs is dependent in part on the duration and height of the viremia, but also on other invasive characteristics of the virus (Lustig et al. 1999).
The mechanism by which encephalitic alphaviruses enter the CNS is not entirely clear. Murine studies have shown infection or transport by cerebrovascular endothelial cells, infection of choroid plexus epithelial cells, infection of olfactory neurons, and transport by peripheral nerves. Once within the CNS virus can spread cell to cell or through the CSF (Paessler et al. 2004; Vogel et al. 2005; Phillips et al. 2013; Jackson et al. 1987, 1988; Thach et al. 2000; Cook and Griffin 2003). For most encephalitic alphaviruses targeted cells within the CNS are neurons and damage to this cell can be severe and irreversible (Liu et al. 1970; Jackson et al. 1988; Phillips et al. 2013).
Outcome is influenced by characteristics of both the host and the virus. Most alphaviruses show an age-dependent susceptibility to disease (Johnson et al. 1972; Couderc et al. 2008; Aguilar 1970; Morgan 1941). Resistance to fatal disease develops between 1 and 3 weeks of age in mice and is associated with decreased virus replication at the site of virus inoculation and in target tissues (e.g., brain) and not with changes in the ability of infected mice to mount an innate or virus-specific adaptive immune response (Johnson et al. 1972; Oliver et al. 1997; Griffin 1976). Maturation-dependent restriction of virus replication is also seen during differentiation of neurons in culture (Schultz et al. 2015; Vernon and Griffin 2005; Castorena et al. 2008). Genetic background of the host is an additional determinant of severity of encephalitis, but only a few specific susceptibility genes have been identified (Thach et al. 2000; Tucker et al. 1996). In mice, defects in acid sphingomyelinase and innate immune responses (e.g., IFN pathway genes) increase susceptibility to fatal disease (Ng and Griffin 2006; Byrnes et al. 2000; Ryman et al. 2000, 2007; Lenschow et al. 2007; Couderc et al. 2008). For SINV, C57BL/6 mice are more susceptible to fatal encephalomyelitis than BALB/c mice and this is determined in part by an unidentified gene on chromosome 2 (Thach et al. 2001).
Virus strains differ in virulence. Alphavirus strains with decreased virulence may replicate poorly even in newborn animals while virulent strains can replicate well and cause disease in adult, as well as newborn, animals. Peripheral replication, viremia, neuroinvasiveness (ability to enter the CNS efficiently), and neurotropism (ability to replicate in CNS cells) all contribute to virulence and are influenced by different molecular characteristics of the virus (Dubuisson et al. 1997). Many alphavirus strains lack neuroinvasiveness in that they can cause fatal encephalitis after intracerebral or intranasal inoculation, but not after subcutaneous or intraperitoneal inoculation. Induction of IFN and susceptibility to IFN-mediated inhibition of replication also affect virulence (Gardner et al. 2009; Cruz et al. 2010; Frolova et al. 2002; Aguilar et al. 2008).
Natural isolates vary in virulence. For instance, human encephalitis due to EEEV has only rarely been recognized in South America, but occurs regularly in North America (Causey et al. 1961; Carrera et al. 2013; Goldfield and Sussman 1968). South American strains are also less virulent in experimental animals (Gardner et al. 2011). Likewise, epizootic strains of WEEV appear to be optimized for viremia and neuroinvasiveness and are generally more virulent for mice and guinea pigs than are enzootic strains and North American strains are more virulent than South American strains (Forrester et al. 2008; Logue et al. 2009; Bianchi et al. 1993; Hardy et al. 1997). Viruses with altered virulence have also been selected after chemical mutagenesis, passage in tissue culture, passage in mice, isolation of plaque variants, and sequence manipulation of cDNA virus clones (Brown et al. 1975; Griffin and Johnson 1977; Tucker et al. 1993). Nucleotide and amino acid changes affecting virulence have been mapped to multiple regions of the genome, including the 5′ NTR, nsP1, nsP2, nsP3, E1 and E2 (Tucker et al. 1993; Dubuisson et al. 1997; Lustig et al. 1988; Tucker and Griffin 1991; Mcknight et al. 1996; Suthar et al. 2005).
Eastern equine encephalitis—EEEV is neurovirulent for marmosets, macaques, mice, guinea pigs, and hamsters and can initiate infection in the CNS by spread from the periphery to the choroid plexus (Liu et al. 1970; Paessler et al. 2004; Vogel et al. 2005). Young mice have extensive neuronal damage and rapid death while older mice become relatively resistant to infection by the peripheral, but not the intracerebral route of inoculation (Vogel et al. 2005; Liu et al. 1970). Strain-dependent inhibition of the IFN response is postulated to facilitate CNS infection (Gardner et al. 2008). Hamsters develop fatal encephalitis, hepatitis, and lymphadenitis characterized by extensive vasculitis and hemorrhage (Paessler et al. 2004) and marmosets and macaques develop encephalitis characterized by neuronal loss, perivascular cuffing, leptomeningitis, and neutrophil-rich inflammation similar to the changes seen in humans (Adams et al. 2008).
Western equine encephalitis—Newborn mice experimentally infected with WEEV die within 48 h with involvement of skeletal muscle, cartilage, and bone marrow. In weanling mice, brain, heart, lung, and brown fat appear to be the primary target tissues (Aguilar 1970). After intracerebral inoculation there is infection of the choroid plexus and ependyma with subsequent spread to neurons and glial cells in the cortex, cerebellum, and brain stem and to motor neurons in the spinal cord (Liu et al. 1970). After peripheral inoculation WEEV replicates in skeletal and cardiac muscle and occasionally spreads to the CNS (Liu et al. 1970; Monath et al. 1978). Infection of hamsters with relatively avirulent WEEV strains leads to progressive neuropathological changes consisting of perivascular inflammation, microcavitation, and astrocytic hypertrophy. Macaques develop fever and encephalitis with infection of neurons and mononuclear inflammation (Reed et al. 2005).
Chikungunya virus—Most studies have focused on arthritis and have shown that viral RNA persists in joint tissues (Hawman et al. 2013), but a few have explored the pathogenesis of neurologic disease in mice and macaques. In vitro, both neurons and astrocytes are susceptible to infection and recent strains with the A226V mutation in E1 replicate more efficiently in neuroblastoma cells (Priya et al. 2013; Das et al. 2015). Young mice are susceptible to CHIKV infection of the CNS after peripheral inoculation (Fraisier et al. 2014; Dhanwani et al. 2011; Ziegler et al. 2008; Priya et al. 2014). Older mice infected intranasally with the original Ross strain also develop neuronal infection (Powers and Logue 2007). Macaques develop neurological complications similar to those described in humans (Labadie et al. 2010).
Sindbis virus—In young mice SINV replicates to high titer and spreads rapidly, causing death in 3–5 days. In older mice virus replication is more restricted and animals often recover (Johnson et al. 1972). After peripheral inoculation virus replicates in muscle, produces a viremia, and then spreads to the brain and spinal cord where the primary target cells are neurons (Jackson et al. 1987).
Strains differing in virulence have been derived from independent isolates from Egypt (AR339), South Africa (SR86), and Israel (SV-Peleg). Variants of AR339 and SV-Peleg have been derived by passage in mice and in tissue culture (Lustig et al. 1992; Griffin and Johnson 1977). Virulence is determined primarily by sequences in the 5′ NTR and the E2 glycoprotein, but is influenced by changes in the E1 glycoprotein and the nsPs (Davis et al. 1986; Lustig et al. 1988; Mcknight et al. 1996; Suthar et al. 2005; Schoepp and Johnston 1993). In the 5′ NTR, a change in nucleotide 5 or 8 from A to G increases neurovirulence by unknown mechanisms (Dubuisson et al. 1997; Mcknight et al. 1996). A number of amino acid changes in the E2 glycoprotein affect virulence by altering efficiency of virus entry into the CNS or by enhancing neuronal infection (Bear et al. 2006; Davis et al. 1986; Tucker et al. 1993; Lee et al. 2002). Neuroinvasion is affected by changes at residues 55 and 190 of E2 (Dubuisson et al. 1997).
The neuroadapted strain , NSV, was derived from AR339 (Taylor et al. 1955) by passage through mouse brain and causes fatal encephalomyelitis in 4–12-week-old mice that is immune-mediated (Griffin and Johnson 1977; Kulcsar et al. 2014). NSV has the same cellular tropism (i.e., neurons) as AR339, but replicates to higher titers in the CNS (Jackson et al. 1988). A Gln to His change at E2-55 increases efficiency of infection of neurons and is a major determinant of increased virulence in older mice (Davis et al. 1986; Tucker and Griffin 1991; Tucker et al. 1993, 1997; Lee et al. 2002; Dropulic et al. 1997). Motor neurons in the brain and spinal cord are particularly susceptible to infection and paralysis is a frequent manifestation of disease (Jackson et al. 1987, 1988). C57BL/6 mice are more susceptible to fatal disease than BALB/c mice (Thach et al. 2000; Tucker et al. 1996).
In vitro studies of cultured cortical neurons showed that SINV infection induces both apoptotic and lytic neuronal cell death and that treatment with antagonists of glutamate excitotoxicity protects from early lytic death (Nargi-Aizenman and Griffin 2001). However, in vivo neuronal death in mature animals is not due to virus replication, but rather to the immune response and AMPA glutamate receptor antagonists protect from fatal paralysis by inhibiting the inflammatory response (Kulcsar et al. 2014; Nargi-Aizenman et al. 2004; Greene et al. 2008).
Immune Responses. Virus Clearance and Immune-Mediated Damage
Alphaviruses induce robust immune responses that include early innate cytokine responses that control initial virus replication followed by antibody and cellular immune responses that lead to infectious virus clearance, but can also lead to immune-mediated neuronal damage.
Innate Responses
IFN is an important part of the host response to alphavirus infection. Type I (α/β) IFN is abundantly induced after alphavirus infection of experimental animals and humans (Schilte et al. 2010; Sherman and Griffin 1990; Trgovcich et al. 1999; Vilcek 1964). Animals can be protected from disease if treated with IFN or IFN-inducers before or soon after infection (Gardner et al. 2010). IFN limits virus replication early, during the time the specific immune response is being induced. Animals unable to respond to IFN due to deletions of the IFN receptor or crucial IFN signaling molecules (e.g., STAT-1) develop fatal infections even when infected with normally avirulent strains of virus (Schilte et al. 2010; Couderc et al. 2008; Byrnes et al. 2000). In the absence of IFN signaling, virus replication may occur in cells normally resistant to infection (Ryman et al. 2000).
Strains of alphaviruses vary in their ability to induce IFN and the amount of IFN produced by infected cells is usually linked to the level of virus replication (Schilte et al. 2010; Schleupner et al. 1969; Postic et al. 1969; Sherman and Griffin 1990; Hackbarth et al. 1973; Gardner et al. 2009). In vitro, induction of IFN requires viral entry and RNA synthesis and results in activation of IFN regulatory factor (IRF)-3 (Schilte et al. 2010; Behr et al. 2001). Study of temperature sensitive (ts) mutants suggests that formation of dsRNA is necessary for IFN induction because viruses that cannot initiate plus strand RNA synthesis do not induce IFN (Hahn et al. 1989; Marcus and Fuller 1979). SINV stimulates formation of the IRF-3/CBP/p300 transcriptional activation complex for immediate early IFNs (Behr et al. 2001) but production of IFN is cell type-dependent (Ho and Breinig 1962; Burke et al. 2009).
Treatment of cells with IFN inhibits alphavirus replication (Ryman et al. 2002; Despres et al. 1995a), but the mechanism by which this occurs, and therefore the IFN-induced host responses important for control of replication, are only partially understood. IFN-induced proteins shown to have an effect on alphavirus replication include IFN-stimulated gene (ISG)-15 (Werneke et al. 2011; Lenschow et al. 2005, 2007), 2′3′-oligoadenylate synthetase (Brehin et al. 2009), and zinc finger antiviral protein (ZAP/PARP-13) that blocks translation of incoming viral genomic RNA (Guo et al. 2007; Zhang et al. 2007; Macdonald et al. 2007). Well-studied antiviral proteins PKR and RNase L have limited roles in the IFN-induced antiviral response in vitro or in vivo (Ryman et al. 2002). Interestingly, SINV-infected RNase L-deficient fibroblasts fail to shut off minus-strand RNA synthesis or to form stable replication complexes. The cells become persistently infected suggesting a direct or indirect role for RNase L in virus replication (Sawicki et al. 2003; Silverman 2007). Virus strains vary in their sensitivity to the antiviral activities of IFN and this may or may not correlate with virulence. Mutations associated with altered sensitivity to IFN have been mapped to the 5′ NTR, nsP1, and nsP2 (Simmons et al. 2010; Fros et al. 2010; Bordi et al. 2011).
In the CNS , neuronal infection leads to production of IFN-β by both neurons and glial cells that plays a role, independent of IFN-α, in early control of virus replication (Burdeinick-Kerr et al. 2007). Injured neurons can also produce IFN-γ, interleukin (IL)-6, and chemokines. Macrophages and glial cells become activated in response to neuronal infection and rapidly produce an additional array of cytokines and chemokines. Production of these factors results in the upregulation of MHC molecules on microglial cells and increased adhesion molecule expression on capillary endothelial cells which facilitate subsequent entry of inflammatory cells into the CNS (Metcalf et al. 2013; Lee et al. 2013).
IFN may also contribute to alphavirus-induced disease. Fever during the viremic phase of infection is probably a response to the IFN induced early after infection and it has been postulated that the rapidly fatal disease in newborn mice is due to the production of large amounts of IFN and other cytokines (Trgovcich et al. 1999). Acute phase responses induced by alphaviruses prior to the virus-specific adaptive immune response include increases in tumor necrosis factor (TNF)-α, IL-1, and IL-6 and levels generally correlate with the extent of virus replication (Klimstra et al. 1999; Wesselingh et al. 1994). Adult mice deficient in IL-1β have reduced mortality after CNS infection with a neurovirulent strain of SINV, again suggesting the possibility that cytokine effects may contribute to mortality (Liang et al. 1999).
Virus-Specific Adaptive Responses
Both humoral and cellular immune responses are induced by infection. In experimentally infected adult mice antiviral IgM antibody is usually detected in serum 3–4 days after infection (Griffin 1976; Paessler et al. 2004). The cellular immune response, manifested by the presence of virus-reactive lymphocytes in draining lymph nodes and blood and the infiltration of mononuclear cells into infected tissues, also begins 3–4 days after infection (Griffin and Johnson 1973; Mcfarland et al. 1972; Metcalf and Griffin 2011). Both appear to play a role in recovery from infection and protection against reinfection.
Humoral immunity —Virus-specific IgM is produced very early in human disease and often provides a means for rapid diagnosis of infection (Calisher et al. 1985, 1986). Likewise, in experimentally infected mice, IgM-secreting cells enter the CNS coincidentally with the clearance of infectious virus (Metcalf and Griffin 2011). IgG antibody appears in serum and IgG-secreting B cells enter the CNS within 7–14 days and are maintained for years (Calisher et al. 1983; Metcalf et al. 2013). Appearance of antibody correlates with cessation of viremia and many lines of evidence support the hypothesis that recovery from alphavirus infection is dependent in large part on the antibody response (Griffin and Johnson 1977; Olitsky et al. 1943; Zichis and Shaughnessy 1945). Rapidity of host antibody synthesis is predictive of outcome from encephalitis; patients without evidence of antibody at the time of onset of illness are most likely to die (Calisher et al. 1986).
Extensive experimental studies to define the antibody specificity and the mechanisms of antibody-mediated recovery and protection have been done using VEEV (see chapter “Venezuelan Equine Encephalitis”), WEEV and SINV infections of mice. Passive transfer of antibody before or after infection can provide protection. Both neutralizing antibodies, mostly anti-E2, and non-neutralizing antibodies, both anti-E1 and anti-E2, can protect against challenge and promote recovery suggesting that virus neutralization per se is not the only mechanism of protection (Stanley et al. 1986; Hunt and Roehrig 1985; Mendoza et al. 1988; Wust et al. 1989).
Antiviral antibody can inhibit alphavirus replication intracellularly and therefore promote clearance and recovery. Treatment of immunodeficient mice that are persistently infected with SINV with immune serum clears infectious virus from the CNS and antibodies specific for either of the neutralizing epitopes on SINV E2 can downregulate intracellular virus replication in vivo and in vitro by a noncytolytic mechanism (Levine et al. 1991). Anti-E1 MAbs may also be able to alter intracellular virus replication, but this has been less extensively studied (Chanas et al. 1982).
Antibody-mediated inhibition of intracellular virus replication requires bivalent antibody, but does not require the Fc portion of the antibody, complement, or other cells (Hirsch et al. 1979; Levine et al. 1991; Ubol et al. 1995). Soon after antibody binding, virion budding from the plasma membrane is inhibited, perhaps by restoring cellular Na+K+ATPase function and K+ flux or host protein synthesis (Despres et al. 1995b; Byrnes et al. 2000). IFN and antibody act synergistically to promote recovery from alphavirus infection both in vivo and in vitro, but the mechanisms by which these systems interact have not been identified. Mechanisms of virus clearance that depend on antibody may be particularly important in the CNS where limited expression of major histocompatibility complex antigens may restrict the role of T lymphocytes (Kimura and Griffin 2000).
Antibody is also important for protection from infection (Morgan et al. 1942). Delivered before or shortly after infection, passive transfer of antibody can protect from acute fatal disease, but may predispose to late disease associated with persistent infection, inflammation, and neuronal degeneration (Griffin and Johnson 1977; Kimura and Griffin 2003).
Cellular Immunity —Alphavirus infection induces virus-specific lymphoproliferative, cytokine and cytotoxic T lymphocyte responses (Griffin and Johnson 1973; Mokhtarian et al. 1982). Antigen-presenting cells travel to local lymph nodes where immune responses are induced and activated T cells enter the circulation and home to sites of virus replication. Activated T cells routinely cross the blood–brain barrier as part of normal immunologic surveillance of the CNS and with infection the entry of activated cells is enhanced (Irani and Griffin 1996). Infiltration of mononuclear cells into the CNS can be detected within 3–4 days after infection and includes natural killer cells, CD4+ and CD8+ T lymphocytes, B cells and macrophages. Proportions of different mononuclear cell populations in the CNS vary with time after infection (Moench and Griffin 1984; Rowell and Griffin 1999; Metcalf and Griffin 2011; Griffin 1976; Mcfarland et al. 1972; Irani and Griffin 1991).
Retention of T cells is immunologically specific and they have many roles during alphavirus infection (Irani and Griffin 1996). Viral RNA levels in the CNS of SINV-infected mice decrease more rapidly when CD8+ T cells are present (Kimura and Griffin 2000). IFN-γ is an important effector cytokine produced by T cells and mice lacking the ability to produce antibody can clear infectious virus from some populations of neurons through production of IFN-γ (Binder and Griffin 2001). IFN-γ treatment of infected mature neurons improves cellular protein synthesis and decreases viral RNA and protein synthesis, but the intracellular effectors of IFN-γ action are not known (Burdeinick-Kerr and Griffin 2005).
Mice deficient in production of both IFN-γ and antibody do not clear infectious virus, but titers of virus during persistence are lower than in mice with severe combined immunodeficiency, suggesting that additional factors contribute to virus clearance (Burdeinick-Kerr et al. 2007).
Immunopathology —Although in young animals, virus infection of neurons can lead to neuronal death, data from several model systems of alphavirus encephalomyelitis suggest that the virus-specific cellular immune response is the major contributor to neuronal damage in older animals (Kimura and Griffin 2003; Nargi-Aizenman et al. 2004; Rowell and Griffin 2002). Mice infected with NSV become paralyzed and die during the process of viral clearance. Outcome is improved in mice deficient in β2 microglobulin, αβ T cells, or CD4+ T cells, but is not affected by deficiencies in antibody, perforin, Fas, TNF-α receptor-1, IL-6, or IL-12, suggesting a role for T cells in immunopathology (Rowell and Griffin 2002; Kimura and Griffin 2000). Furthermore, protection of NSV-infected mice from paralysis and death by AMPA glutamate receptor antagonists despite delayed virus clearance is associated with a decrease in the inflammatory response (Nargi-Aizenman et al. 2004; Greene et al. 2008).
A detrimental role for T cells in outcome of NSV infection is also suggested by study of C57BL/6 mice protected from fatal disease by passive transfer of immune serum after infection. These mice clear infectious virus, but viral RNA and antigen persist. Progressive loss of parenchyma and development of terminal deoxynucleotidyl transferase-mediated dUTP nick end-labeling (TUNEL)-positive pyramidal neurons is correlated with infiltration of CD4+ T cells and macrophage/microglial cells (Kimura and Griffin 2003). CD4+ T cells have been further implicated in immunopathology by association of fatal disease with infiltration into the CNS of pathogenic Th17 cells that produce GM-CSF and IFN-γ, a process that is accelerated in the absence of the immunomodulatory cytokine IL-10 (Kulcsar et al. 2014).
Pathology
Much of the pathology observed during alphavirus encephalomyelitis is associated with the inflammatory response to infection and damage to infected neurons. Neuronal cell death may be apoptotic, particularly in young animals (Lewis et al. 1996), or may be characterized by cytoplasmic swelling, vacuolation, membrane breakdown, and cellular degeneration suggesting necrosis (Havert et al. 2000; Garen et al. 1999; Murphy and Whitfield 1970). Demyelination has occasionally been described as a consequence of EEEV and WEEV infection in humans and WEEV infection of mice, probably as a result of infection of oligodendrocytes (Bastian et al. 1975; Noran 1944).
Pathologic changes in the CNS of humans with fatal neurologic disease and mice with experimentally induced encephalomyelitis begin with infiltration of mononuclear and occasional polymorphonuclear cells into perivascular regions (Mcfarland et al. 1972; Moench and Griffin 1984). This phase can include perivascular extravasation of red blood cells and endothelial cell swelling and hyperplasia. Lymphocytes and monocytes then move from the perivascular regions to infiltrate areas of the parenchyma that contain virus-infected neurons. This inflammatory process is accompanied by gliosis and evidence of inflammatory and glial cell apoptosis (Garen et al. 1999).
Histopathology on fatal cases of EEE demonstrates a diffuse meningoencephalitis with widespread neuronal destruction, perivascular cuffing with polymorphonuclear as well as mononuclear leukocytes, and vasculitis with vessel occlusion in the cortex, basal ganglia, and brainstem. Virus antigen is localized to neurons and neuronal death is marked by cytoplasmic swelling and nuclear pyknosis. Apoptotic glial and inflammatory cells are frequently found in the regions of affected neurons (Garen et al. 1999; Silverman et al. 2013). Neonatal mice and human infants may die with widespread virus-induced neuronal cell death before the inflammatory process, a manifestation of the cellular immune response, can be initiated.
Pathology of acute cases of WEE shows leptomeningitis and perivascular cuffing with polymorphonuclear leukocyte infiltration in the earliest cases and lymphocytes, plasma cells, and macrophages at later times. Inflammation is accompanied by endothelial hyperplasia, petechial hemorrhages, and glial nodules in areas of neuronal degeneration. Lesions are found primarily in the basal ganglia, brain stem, cerebellum, cerebral cortex, and spinal cord. In addition, there are areas of focal necrosis and demyelination, particularly in the subcortical white matter and basal ganglia (Finley et al. 1955).
Persistence
Persistent infection can occasionally be established in mammalian cell cultures in vitro. Mutations in the nsP2 protein can lead to reduced SINV RNA synthesis and persistent infection (Frolova et al. 2002; Dryga et al. 1997) and mouse fibroblasts producing IFN can be persistently infected (Inglot et al. 1973; Weiss et al. 1980). Persistent infection can also be established if the cell infected, such as a mature neuron, is resistant to virus-induced apoptosis (Burdeinick-Kerr and Griffin 2005; Levine et al. 1993; Ubol et al. 1995; Vernon and Griffin 2005; Schultz et al. 2015).
In vivo, there is substantial evidence that alphaviruses can persist after appearance of an immune response and clearance of infectious virus from the circulation and from tissue (Levine and Griffin 1992; Tyor et al. 1992; Metcalf and Griffin 2011). Infants and children surviving months to years after onset of WEE (often with progressive disease) may have cystic lesions, gliosis, and demyelination with areas of active mononuclear inflammation (Herzon et al. 1957; Noran 1944). Chronic joint inflammation after CHIKV infection is associated with the persistent presence of viral RNA and antigen (Hawman et al. 2013; Labadie et al. 2010).
Mice clear infectious SINV from the CNS within 7–8 days but the decline in viral RNA occurs slowly (Griffin and Metcalf 2011). Viral RNA and proteins can be detected in the nervous system and memory deficits persist long after apparent recovery (Potter et al. 2015; Burdeinick-Kerr et al. 2007). It is postulated that persistence is due to failure to eliminate the infected cells. Therefore, one consequence of a nonlytic mechanism for clearance of virus from tissue is that the virus genome is not completely eliminated if the originally infected cells survive. This leads to a need for long-term control of virus replication to prevent reactivation of infection by continued presence of virus-specific T lymphocytes and antibody-secreting B cells within the CNS (Metcalf et al. 2013; Metcalf and Griffin 2011; Tyor et al. 1992).
Prevention, Diagnosis, and Treatment
A formalin-inactivated vaccine derived from a North American strain of EEEV (PE-6) is available for horses and emus and for investigational use to protect laboratory workers. This vaccine does not induce significant neutralizing or anti-E2 antibody to South American strains of EEEV (Strizki and Repik 1995). An inactivated WEEV vaccine is available for horses and as an experimental preparation for laboratory workers (Randall et al. 1947). Yearly booster doses are required for both. A live attenuated vaccine has been developed for CHIKV, but has not been licensed (Levitt et al. 1986). Many new potential vaccines for these alphaviruses are currently in preclinical development (Carossino et al. 2014).
Protection of human populations relies primarily on personal protection from mosquito bites. Mosquito populations can be monitored for infection by virus isolation, by nucleic acid amplification, or by seroconversion of sentinel pheasants or chickens. This information can be used to guide insecticide spraying to reduce adult and larval mosquito populations.
Diagnosis is based on virus isolation or detection of viral RNA or antiviral antibody. Virus can be isolated from CSF, blood, or CNS tissue by inoculation into newborn mice or onto a variety of tissue culture cells. Direct virus detection and identification in field and clinical samples can be accomplished through various nucleic acid amplification assays (Lambert et al. 2003). Antibody is usually measured by enzyme immunoassay with detection of IgM in serum and CSF particularly useful (Calisher et al. 1986).
No successful specific antiviral therapy has been identified for CNS infection and the mainstay of treatment remains vigorous supportive therapy including respiratory assistance, maintenance of electrolyte balance, and control of seizures and increased intracranial pressure.
Summary and Future Directions
Alphaviruses are mosquito-borne causes of acute encephalomyelitis with potential to spread to new regions of the world. Alphavirus infections of experimental animals have provided important model systems for understanding the pathogenesis of viral infections of the CNS and mechanisms of noncytolytic clearance of viruses from neurons. There is a need to determine the mechanisms by which different components of the innate and adaptive immune responses control replication and clear infectious virus from neurons without damage to the infected cells. Lastly, vaccines and treatments that interfere with virus replication and protect neurons from immune-mediated damage are needed.
References
Adams AP, Aronson JF, Tardif SD et al (2008) Common marmosets (Callithrix jacchus) as a nonhuman primate model to assess the virulence of eastern equine encephalitis virus strains. J Virol 82:9035–9042
Aguilar MJ (1970) Pathological changes in brain and other target organs of infant and weanling mice after infection with non-neuroadapted Western equine encephalitis virus. Infect Immun 2:533–542
Aguilar PV, Adams AP, Wang E et al (2008) Structural and nonstructural protein genome regions of eastern equine encephalitis virus are determinants of interferon sensitivity and murine virulence. J Virol 82:4920–4930
Allison AB, Stallknecht DE, Holmes EC (2015) Evolutionary genetics and vector adaptation of recombinant viruses of the western equine encephalitis antigenic complex provides new insights into alphavirus diversity and host switching. Virology 474:154–162
Arpino C, Curatolo P, Rezza G (2009) Chikungunya and the nervous system: what we do and do not know. Rev Med Virol 19:121–129
Arrigo NC, Adams AP, Weaver SC (2010) Evolutionary patterns of eastern equine encephalitis virus in North versus South America suggest ecological differences and taxonomic revision. J Virol 84:1014–1025
Bashford CL, Micklem KJ, Pasternak CA (1985) Sequential onset of permeability changes in mouse ascites cells induced by Sendai virus. Biochim Biophys Acta 814:247–255
Bastian FO, Wende RD, Singer DB, Zeller RS (1975) Eastern equine encephalomyelitis. Histopathologic and ultrastructural changes with isolation of the virus in a human case. Am J Clin Pathol 64:10–13
Bear JS, Byrnes AP, Griffin DE (2006) Heparin-binding and patterns of virulence for two recombinant strains of Sindbis virus. Virology 347:183–190
Behr M, Schieferdecker K, Buhr P et al (2001) Interferon-stimulated response element (ISRE)-binding protein complex DRAF1 is activated in Sindbis virus (HR)-infected cells. J Interferon Cytokine Res 21:981–990
Bergren NA, Auguste AJ, Forrester NL et al (2014) Western equine encephalitis virus: evolutionary analysis of a declining alphavirus based on complete genome sequences. J Virol 88:9260–9267
Bianchi TI, Aviles G, Monath TP, Sabattini MS (1993) Western equine encephalomyelitis: virulence markers and their epidemiologic significance. Am J Trop Med Hyg 49:322–328
Binder GK, Griffin DE (2001) Interferon-gamma-mediated site-specific clearance of alphavirus from CNS neurons. Science 293:303–306
Bingham AM, Graham SP, Burkett-Cadena ND et al (2012) Detection of eastern equine encephalomyelitis virus RNA in North American snakes. Am J Trop Med Hyg 87:1140–1144
Boggs WM, Hahn CS, Strauss EG, Strauss JH, Griffin DE (1989) Low pH-dependent Sindbis virus-induced fusion of BHK cells: differences between strains correlate with amino acid changes in the E1 glycoprotein. Virology 169:485–488
Bordi L, Meschi S, Selleri M et al (2011) Chikungunya virus isolates with/without A226V mutation show different sensitivity to IFN-a, but similar replication kinetics in non human primate cells. New Microbiol 34:87–91
Brault AC, Powers AM, Chavez CL et al (1999) Genetic and antigenic diversity among eastern equine encephalitis viruses from North, Central, and South America. Am J Trop Med Hyg 61:579–586
Brehin AC, Casademont I, Frenkiel MP, Julier C, Sakuntabhai A, Despres P (2009) The large form of human 2′,5′-Oligoadenylate Synthetase (OAS3) exerts antiviral effect against Chikungunya virus. Virology 384:216–222
Brown A, Vosdingh R, Zebovitz E (1975) Attenuation and immunogenicity of ts mutants of Eastern encephalitis virus for mice. J Gen Virol 27:111–116
Burdeinick-Kerr R, Griffin DE (2005) Gamma interferon-dependent, noncytolytic clearance of sindbis virus infection from neurons in vitro. J Virol 79:5374–5385
Burdeinick-Kerr R, Wind J, Griffin DE (2007) Synergistic roles of antibody and interferon in noncytolytic clearance of Sindbis virus from different regions of the central nervous system. J Virol 81:5628–5636
Burke CW, Gardner CL, Steffan JJ, Ryman KD, Klimstra WB (2009) Characteristics of alpha/beta interferon induction after infection of murine fibroblasts with wild-type and mutant alphaviruses. Virology 395:121–132
Byrnes AP, Griffin DE (2000) Large-plaque mutants of Sindbis virus show reduced binding to heparan sulfate, heightened viremia, and slower clearance from the circulation. J Virol 74:644–651
Byrnes AP, Durbin JE, Griffin DE (2000) Control of Sindbis virus infection by antibody in interferon-deficient mice. J Virol 74:3905–3908
Calisher CH (1994) Medically important arboviruses of the United States and Canada. Clin Microbiol Rev 7:89–116
Calisher CH, Emerson JK, Muth DJ, Lazuick JS, Monath TP (1983) Serodiagnosis of western equine encephalitis virus infections: relationships of antibody titer and test to observed onset of clinical illness. J Am Vet Med Assoc 183:438–440
Calisher CH, Meurman O, Brummer-Korvenkontio M, Halonen PE, Muth DJ (1985) Sensitive enzyme immunoassay for detecting immunoglobulin M antibodies to Sindbis virus and further evidence that Pogosta disease is caused by a western equine encephalitis complex virus. J Clin Microbiol 22:566–571
Calisher CH, Berardi VP, Muth DJ, Buff EE (1986) Specificity of immunoglobulin M and G antibody responses in humans infected with eastern and western equine encephalitis viruses: application to rapid serodiagnosis. J Clin Microbiol 23:369–372
Calisher CH, Karabatsos N, Lazuick JS, Monath TP, Wolff KL (1988) Reevaluation of the western equine encephalitis antigenic complex of alphaviruses (family Togaviridae) as determined by neutralization tests. Am J Trop Med Hyg 38:447–452
Carey DE, Myers RM, Deranitz CM, Jadhav M, Reuben R (1969) The 1964 chikungunya epidemic at Vellore, South India, including observations on concurrent dengue. Trans R Soc Trop Med Hyg 63:434–445
Carossino M, Thiry E, de la Grandiere A, Barrandeguy ME (2014) Novel vaccination approaches against equine alphavirus encephalitides. Vaccine 32:311–319
Carrera JP, Forrester N, Wang E et al (2013) Eastern equine encephalitis in Latin America. N Engl J Med 369:732–744
Castorena KM, Peltier DC, Peng W, Miller DJ (2008) Maturation-dependent responses of human neuronal cells to western equine encephalitis virus infection and type I interferons. Virology 372:208–220
Causey OR, Causey CE, Maroja OM, Macedo DG (1961) The isolation of arthropod-borne viruses, including members of two hitherto undescribed serological groups, in the Amazon region of Brazil. Am J Trop Med Hyg 10:227–249
Chanas AC, Gould EA, Clegg JC, Varma MG (1982) Monoclonal antibodies to Sindbis virus glycoprotein E1 can neutralize, enhance infectivity, and independently inhibit haemagglutination or haemolysis. J Gen Virol 58(Pt 1):37–46
Chandak NH, Kashyap RS, Kabra D et al (2009) Neurological complications of Chikungunya virus infection. Neurol India 57:177–180
Chatterjee PK, Eng CH, Kielian M (2002) Novel mutations that control the sphingolipid and cholesterol dependence of the Semliki Forest virus fusion protein. J Virol 76:12712–12722
Chenier S, Cote G, Vanderstock J, Macieira S, Laperle A, Helie P (2010) An eastern equine encephalomyelitis (EEE) outbreak in Quebec in the fall of 2008. Can Vet J 51:1011–1015
Cilnis MJ, Kang W, Weaver SC (1996) Genetic conservation of Highlands J viruses. Virology 218:343–351
Coffey LL, Beeharry Y, Borderia AV, Blanc H, Vignuzzi M (2011) Arbovirus high fidelity variant loses fitness in mosquitoes and mice. Proc Natl Acad Sci U S A 108:16038–16043
Cook SH, Griffin DE (2003) Luciferase imaging of a neurotropic viral infection in intact animals. J Virol 77:5333–5338
Couderc T, Chretien F, Schilte C et al (2008) A mouse model for Chikungunya: young age and inefficient type-I interferon signaling are risk factors for severe disease. PLoS Pathog 4:e29
Cruz CC, Suthar MS, Montgomery SA et al (2010) Modulation of type I IFN induction by a virulence determinant within the alphavirus nsP1 protein. Virology 399:1–10
Cupp EW, Klingler K, Hassan HK, Viguers LM, Unnasch TR (2003) Transmission of eastern equine encephalomyelitis virus in central Alabama. Am J Trop Med Hyg 68:495–500
Dalrymple JM, Young OP, Eldridge BF, Russell PK (1972) Ecology of arboviruses in a Maryland freshwater swamp. 3. Vertebrate hosts. Am J Epidemiol 96:129–140
Das T, Hoarau JJ, Jaffar Bandjee MC, Maquart M, Gasque P (2015) Multifaceted innate immune responses engaged by astrocytes, microglia and resident dendritic cells against Chikungunya neuroinfection. J Gen Virol 96:294–310
Davis NL, Fuller FJ, Dougherty WG, Olmsted RA, Johnston RE (1986) A single nucleotide change in the E2 glycoprotein gene of Sindbis virus affects penetration rate in cell culture and virulence in neonatal mice. Proc Natl Acad Sci U S A 83:6771–6775
Deresiewicz RL, Thaler SJ, Hsu L, Zamani AA (1997) Clinical and neuroradiographic manifestations of eastern equine encephalitis. N Engl J Med 336:1867–1874
Despres P, Griffin JW, Griffin DE (1995a) Antiviral activity of alpha interferon in Sindbis virus-infected cells is restored by anti-E2 monoclonal antibody treatment. J Virol 69:7345–7348
Despres P, Griffin JW, Griffin DE (1995b) Effects of anti-E2 monoclonal antibody on sindbis virus replication in AT3 cells expressing bcl-2. J Virol 69:7006–7014
Dhanwani R, Khan M, Alam SI, Rao PV, Parida M (2011) Differential proteome analysis of Chikungunya virus-infected new-born mice tissues reveal implication of stress, inflammatory and apoptotic pathways in disease pathogenesis. Proteomics 11:1936–1951
Dhanwani R, Khan M, Bhaskar AS et al (2012) Characterization of Chikungunya virus infection in human neuroblastoma SH-SY5Y cells: role of apoptosis in neuronal cell death. Virus Res 163:563–572
Dropulic LK, Hardwick JM, Griffin DE (1997) A single amino acid change in the E2 glycoprotein of Sindbis virus confers neurovirulence by altering an early step of virus replication. J Virol 71:6100–6105
Dryga SA, Dryga OA, Schlesinger S (1997) Identification of mutations in a Sindbis virus variant able to establish persistent infection in BHK cells: the importance of a mutation in the nsP2 gene. Virology 228:74–83
Dubuisson J, Lustig S, Ruggli N, Akov Y, Rice CM (1997) Genetic determinants of Sindbis virus neuroinvasiveness. J Virol 71:2636–2646
El-Bacha T, Menezes MM, Azevedo e Silva MC, Sola-Penna M, Da Poian AT (2004) Mayaro virus infection alters glucose metabolism in cultured cells through activation of the enzyme 6-phosphofructo 1-kinase. Mol Cell Biochem 266:191–198
Espmark A, Niklasson B (1984) Ockelbo disease in Sweden: epidemiological, clinical, and virological data from the 1982 outbreak. Am J Trop Med Hyg 33:1203–1211
Estep LK, Mcclure CJ, Vander Kelen P et al (2013) Risk of exposure to eastern equine encephalomyelitis virus increases with the density of northern cardinals. PLoS One 8, e57879
Feemster RF (1957) Equine encephalitis in Massachusetts. N Engl J Med 257:701–704
Ficken MD, Wages DP, Guy JS, Quinn JA, Emory WH (1993) High mortality of domestic turkeys associated with Highlands J virus and eastern equine encephalitis virus infections. Avian Dis 37:585–590
Finley KH, Longshore WA Jr, Palmer RJ, Cook RE, Riggs N (1955) Western equine and St. Louis encephalitis; preliminary report of a clinical follow-up study in California. Neurology 5:223–235
Firth AE, Chung BY, Fleeton MN, Atkins JF (2008) Discovery of frameshifting in Alphavirus 6K resolves a 20-year enigma. Virol J 5:108
Forrester NL, Kenney JL, Deardorff E, Wang E, Weaver SC (2008) Western equine encephalitis submergence: lack of evidence for a decline in virus virulence. Virology 380:170–172
Fraisier C, Koraka P, Belghazi M et al (2014) Kinetic analysis of mouse brain proteome alterations following Chikungunya virus infection before and after appearance of clinical symptoms. PLoS One 9, e91397
Froeschle JE (1964) Propagation of western equine encephalitis virus in mice following intramuscular and intranasal inoculation. Proc Soc Exp Biol Med 115:881–884
Frolov I, Hardy R, Rice CM (2001) Cis-acting RNA elements at the 5′ end of Sindbis virus genome RNA regulate minus- and plus-strand RNA synthesis. RNA 7:1638–1651
Frolova EI, Fayzulin RZ, Cook SH, Griffin DE, Rice CM, Frolov I (2002) Roles of nonstructural protein nsP2 and Alpha/Beta interferons in determining the outcome of Sindbis virus infection. J Virol 76:11254–11264
Frolova EI, Gorchakov R, Pereboeva L, Atasheva S, Frolov I (2010) Functional Sindbis virus replicative complexes are formed at the plasma membrane. J Virol 84:11679–11695
Fros JJ, Liu WJ, Prow NA et al (2010) Chikungunya virus nonstructural protein 2 inhibits type I/II interferon-stimulated JAK-STAT signaling. J Virol 84:10877–10887
Gardner CL, Burke CW, Tesfay MZ, Glass PJ, Klimstra WB, Ryman KD (2008) Eastern and Venezuelan equine encephalitis viruses differ in their ability to infect dendritic cells and macrophages: impact of altered cell tropism on pathogenesis. J Virol 82:10634–10646
Gardner CL, Yin J, Burke CW, Klimstra WB, Ryman KD (2009) Type I interferon induction is correlated with attenuation of a South American eastern equine encephalitis virus strain in mice. Virology 390:338–347
Gardner J, Anraku I, Le TT et al (2010) Chikungunya virus arthritis in adult wild-type mice. J Virol 84:8021–8032
Gardner CL, Ebel GD, Ryman KD, Klimstra WB (2011) Heparan sulfate binding by natural eastern equine encephalitis viruses promotes neurovirulence. Proc Natl Acad Sci U S A 108:16026–16031
Garen PD, Tsai TF, Powers JM (1999) Human eastern equine encephalitis: immunohistochemistry and ultrastructure. Mod Pathol 12:646–652
Gerardin P, Guernier V, Perrau J et al (2008) Estimating Chikungunya prevalence in La Reunion Island outbreak by serosurveys: two methods for two critical times of the epidemic. BMC Infect Dis 8:99
Gibney KB, Robinson S, Mutebi JP et al (2011) Eastern equine encephalitis: an emerging arboviral disease threat, Maine, 2009. Vector Borne Zoonotic Dis 11:637–639
Goldfield M, Sussman O (1968) The 1959 outbreak of Eastern encephalitis in New Jersey. I. Introduction and description of outbreak. Am J Epidemiol 87:1–10
Goldfield M, Welsh JN, Taylor BF (1968) The 1959 outbreak of Eastern encephalitis in New Jersey. 5. The inapparent infection:disease ratio. Am J Epidemiol 87:32–33
Gorchakov R, Frolova E, Frolov I (2005) Inhibition of transcription and translation in Sindbis virus-infected cells. J Virol 79:9397–9409
Greene IP, Lee EY, Prow N, Ngwang B, Griffin DE (2008) Protection from fatal viral encephalomyelitis: AMPA receptor antagonists have a direct effect on the inflammatory response to infection. Proc Natl Acad Sci U S A 105:3575–3580
Griffin DE (1976) Role of the immune response in age-dependent resistance of mice to encephalitis due to Sindbis virus. J Infect Dis 133:456–464
Griffin DE, Johnson RT (1973) Cellular immune response to viral infection: in vitro studies of lymphocytes from mice infected with Sindbis virus. Cell Immunol 9:426–434
Griffin DE, Johnson RT (1977) Role of the immune response in recovery from Sindbis virus encephalitis in mice. J Immunol 118:1070–1075
Griffin DE, Metcalf T (2011) Clearance of virus infection from the CNS. Curr Opin Virol 1:216–221
Guo X, Ma J, Sun J, Gao G (2007) The zinc-finger antiviral protein recruits the RNA processing exosome to degrade the target mRNA. Proc Natl Acad Sci U S A 104:151–156
Hackbarth SA, Reinarz AB, Sagik BP (1973) Age-dependent resistance of mice to sindbis virus infection: reticuloendothelial role. J Reticuloendothel Soc 14:405–425
Hahn CS, Lustig S, Strauss EG, Strauss JH (1988) Western equine encephalitis virus is a recombinant virus. Proc Natl Acad Sci U S A 85:5997–6001
Hahn YS, Strauss EG, Strauss JH (1989) Mapping of RNA- temperature-sensitive mutants of Sindbis virus: assignment of complementation groups A, B, and G to nonstructural proteins. J Virol 63:3142–3150
Halstead SB, Scanlon JE, Umpaivit P, Udomsakdi S (1969) Dengue and chikungunya virus infection in man in Thailand, 1962–1964. IV. Epidemiologic studies in the Bangkok metropolitan area. Am J Trop Med Hyg 18:997–1021
Hapuarachchi HC, Bandara KB, Sumanadasa SD et al (2010) Re-emergence of Chikungunya virus in South-east Asia: virological evidence from Sri Lanka and Singapore. J Gen Virol 91:1067–1076
Hardy WR, Strauss JH (1989) Processing the nonstructural polyproteins of sindbis virus: nonstructural proteinase is in the C-terminal half of nsP2 and functions both in cis and in trans. J Virol 63:4653–4664
Hardy JL, Presser SB, Chiles RE, Reeves WC (1997) Mouse and baby chicken virulence of enzootic strains of western equine encephalomyelitis virus from California. Am J Trop Med Hyg 57:240–244
Havert MB, Schofield B, Griffin DE, Irani DN (2000) Activation of divergent neuronal cell death pathways in different target cell populations during neuroadapted sindbis virus infection of mice. J Virol 74:5352–5356
Hawman DW, Stoermer KA, Montgomery SA et al (2013) Chronic joint disease caused by persistent Chikungunya virus infection is controlled by the adaptive immune response. J Virol 87:13878–13888
Hayes CG, Wallis RC (1977) Ecology of Western equine encephalomyelitis in the eastern United States. Adv Virus Res 21:37–83
Helenius A, Kartenbeck J, Simons K, Fries E (1980) On the entry of Semliki forest virus into BHK-21 cells. J Cell Biol 84:404–420
Herzon H, Shelton JT, Bruyn HB (1957) Sequelae of western equine and other arthropod-borne encephalitides. Neurology 7:535–548
Hirsch RL, Griffin DE, Johnson RT (1979) Interactions between immune cells and antibody in protection from fatal Sindbis virus encephalitis. Infect Immun 23:320–324
Ho M, Breinig MK (1962) Conditions for the production of an interferon appearing in chick cell cultures infected with Sindbis virus. J Immunol 89:177–186
Ho K, Ang LW, Tan BH et al (2011) Epidemiology and control of chikungunya fever in Singapore. J Infect 62:263–270
Howitt B (1938) Recovery of the virus of equine encephalomyelitis from the brain of a child. Science 88:455–456
Hunt AR, Roehrig JT (1985) Biochemical and biological characteristics of epitopes on the E1 glycoprotein of western equine encephalitis virus. Virology 142:334–346
Inglot AD, Albin M, Chudzio T (1973) Persistent infection of mouse cells with Sindbis virus: role of virulence of strains, auto-interfering particles and interferon. J Gen Virol 20:105–110
Irani DN, Griffin DE (1991) Isolation of brain parenchymal lymphocytes for flow cytometric analysis. Application to acute viral encephalitis. J Immunol Methods 139:223–231
Irani DN, Griffin DE (1996) Regulation of lymphocyte homing into the brain during viral encephalitis at various stages of infection. J Immunol 156:3850–3857
Jackson AC, Moench TR, Griffin DE, Johnson RT (1987) The pathogenesis of spinal cord involvement in the encephalomyelitis of mice caused by neuroadapted Sindbis virus infection. Lab Invest 56:418–423
Jackson AC, Moench TR, Trapp BD, Griffin DE (1988) Basis of neurovirulence in Sindbis virus encephalomyelitis of mice. Lab Invest 58:503–509
Jan JT, Griffin DE (1999) Induction of apoptosis by Sindbis virus occurs at cell entry and does not require virus replication. J Virol 73:10296–10302
Jan JT, Chatterjee S, Griffin DE (2000) Sindbis virus entry into cells triggers apoptosis by activating sphingomyelinase, leading to the release of ceramide. J Virol 74:6425–6432
Joe AK, Ferrari G, Jiang HH, Liang XH, Levine B (1996) Dominant inhibitory Ras delays Sindbis virus-induced apoptosis in neuronal cells. J Virol 70:7744–7751
Johnson RT (1965) Virus invasion of the central nervous system: a study of Sindbis virus infection in the mouse using fluorescent antibody. Am J Pathol 46:929–943
Johnson RT, Mcfarland HF, Levy SE (1972) Age-dependent resistance to viral encephalitis: studies of infections due to Sindbis virus in mice. J Infect Dis 125:257–262
Jose J, Snyder JE, Kuhn RJ (2009) A structural and functional perspective of alphavirus replication and assembly. Future Microbiol 4:837–856
Jupp PG, Blackburn NK, Thompson DL, Meenehan GM (1986) Sindbis and West Nile virus infections in the Witwatersrand-Pretoria region. S Afr Med J 70:218–220
Karabatsos N, Lewis AL, Calisher CH, Hunt AR, Roehrig JT (1988) Identification of Highlands J virus from a Florida horse. Am J Trop Med Hyg 39:603–606
Kerr DA, Larsen T, Cook SH et al (2002) BCL-2 and BAX protect adult mice from lethal Sindbis virus infection but do not protect spinal cord motor neurons or prevent paralysis. J Virol 76:10393–10400
Kimura T, Griffin DE (2000) The role of CD8(+) T cells and major histocompatibility complex class I expression in the central nervous system of mice infected with neurovirulent Sindbis virus. J Virol 74:6117–6125
Kimura T, Griffin DE (2003) Extensive immune-mediated hippocampal damage in mice surviving infection with neuroadapted Sindbis virus. Virology 311:28–39
Kissling RE, Chamberlain RW, Sikes RK, Eidson ME (1954) Studies on the North American arthropod-borne encephalitides. III. Eastern equine encephalitis in wild birds. Am J Hyg 60:251–265
Klimstra WB, Ryman KD, Johnston RE (1998) Adaptation of Sindbis virus to BHK cells selects for use of heparan sulfate as an attachment receptor. J Virol 72:7357–7366
Klimstra WB, Ryman KD, Bernard KA, Nguyen KB, Biron CA, Johnston RE (1999) Infection of neonatal mice with sindbis virus results in a systemic inflammatory response syndrome. J Virol 73:10387–10398
Kokernot RH, Shinefield HR, Longshore WA Jr (1953) The 1952 outbreak of encephalitis in California; differential diagnosis. Calif Med 79:73–77
Kulcsar KA, Baxter VK, Greene IP, Griffin DE (2014) Interleukin 10 modulation of pathogenic Th17 cells during fatal alphavirus encephalomyelitis. Proc Natl Acad Sci U S A 111:16053–16058
Labadie K, Larcher T, Joubert C et al (2010) Chikungunya disease in nonhuman primates involves long-term viral persistence in macrophages. J Clin Invest 120:894–906
Laine M, Luukkainen R, Toivanen A (2004) Sindbis viruses and other alphaviruses as cause of human arthritic disease. J Intern Med 256:457–471
Lambert AJ, Martin DA, Lanciotti RS (2003) Detection of North American eastern and western equine encephalitis viruses by nucleic acid amplification assays. J Clin Microbiol 41:379–385
Lee P, Knight R, Smit JM, Wilschut J, Griffin DE (2002) A single mutation in the E2 glycoprotein important for neurovirulence influences binding of sindbis virus to neuroblastoma cells. J Virol 76:6302–6310
Lee EY, Schultz KL, Griffin DE (2013) Mice deficient in interferon-gamma or interferon-gamma receptor 1 have distinct inflammatory responses to acute viral encephalomyelitis. PLoS One 8:e76412
Lemm JA, Rumenapf T, Strauss EG, Strauss JH, Rice CM (1994) Polypeptide requirements for assembly of functional Sindbis virus replication complexes: a model for the temporal regulation of minus- and plus-strand RNA synthesis. EMBO J 13:2925–2934
Lenschow DJ, Giannakopoulos NV, Gunn LJ et al (2005) Identification of interferon-stimulated gene 15 as an antiviral molecule during Sindbis virus infection in vivo. J Virol 79:13974–13983
Lenschow DJ, Lai C, Frias-Staheli N et al (2007) IFN-stimulated gene 15 functions as a critical antiviral molecule against influenza, herpes, and Sindbis viruses. Proc Natl Acad Sci U S A 104:1371–1376
Levine B, Griffin DE (1992) Persistence of viral RNA in mouse brains after recovery from acute alphavirus encephalitis. J Virol 66:6429–6435
Levine B, Hardwick JM, Trapp BD, Crawford TO, Bollinger RC, Griffin DE (1991) Antibody-mediated clearance of alphavirus infection from neurons. Science 254:856–860
Levine B, Huang Q, Isaacs JT, Reed JC, Griffin DE, Hardwick JM (1993) Conversion of lytic to persistent alphavirus infection by the bcl-2 cellular oncogene. Nature 361:739–742
Levine B, Goldman JE, Jiang HH, Griffin DE, Hardwick JM (1996) Bc1-2 protects mice against fatal alphavirus encephalitis. Proc Natl Acad Sci U S A 93:4810–4815
Levitt NH, Ramsburg HH, Hasty SE, Repik PM, Cole FE Jr, Lupton HW (1986) Development of an attenuated strain of chikungunya virus for use in vaccine production. Vaccine 4:157–162
Lewis J, Wesselingh SL, Griffin DE, Hardwick JM (1996) Alphavirus-induced apoptosis in mouse brains correlates with neurovirulence. J Virol 70:1828–1835
Lewis J, Oyler GA, Ueno K et al (1999) Inhibition of virus-induced neuronal apoptosis by Bax. Nat Med 5:832–835
Li L, Jose J, Xiang Y, Kuhn RJ, Rossmann MG (2010) Structural changes of envelope proteins during alphavirus fusion. Nature 468:705–708
Liang XH, Kleeman LK, Jiang HH et al (1998) Protection against fatal Sindbis virus encephalitis by beclin, a novel Bcl-2-interacting protein. J Virol 72:8586–8596
Liang XH, Goldman JE, Jiang HH, Levine B (1999) Resistance of interleukin-1beta-deficient mice to fatal Sindbis virus encephalitis. J Virol 73:2563–2567
Liu C, Voth DW, Rodina P, Shauf LR, Gonzalez G (1970) A comparative study of the pathogenesis of western equine and eastern equine encephalomyelitis viral infections in mice by intracerebral and subcutaneous inoculations. J Infect Dis 122:53–63
Logue CH, Bosio CF, Welte T et al (2009) Virulence variation among isolates of western equine encephalitis virus in an outbred mouse model. J Gen Virol 90:1848–1858
Longshore WA Jr, Stevens IM, Hollister AC Jr, Gittelsohn A, Lennette EH (1956) Epidemiologic observations on acute infectious encephalitis in California, with special reference to the 1952 outbreak. Am J Hyg 63:69–86
Lubelczyk C, Mutebi JP, Robinson S et al (2013) An epizootic of eastern equine encephalitis virus, Maine, USA in 2009: outbreak description and entomological studies. Am J Trop Med Hyg 88:95–102
Lundstrom JO (1999) Mosquito-borne viruses in western Europe: a review. J Vector Ecol 24:1–39
Lundstrom JO, Pfeffer M (2010) Phylogeographic structure and evolutionary history of Sindbis virus. Vector Borne Zoonotic Dis 10:889–907
Lustig S, Jackson AC, Hahn CS, Griffin DE, Strauss EG, Strauss JH (1988) Molecular basis of Sindbis virus neurovirulence in mice. J Virol 62:2329–2336
Lustig S, Halevy M, Ben-Nathan D, Akov Y (1992) A novel variant of Sindbis virus is both neurovirulent and neuroinvasive in adult mice. Arch Virol 122:237–248
Lustig S, Halevy M, Ben-Nathan D, Rice CM, Kobiler D (1999) The role of host immunocompetence in neuroinvasion of Sindbis virus. Arch Virol 144:1159–1171
Macdonald MR, Machlin ES, Albin OR, Levy DE (2007) The zinc finger antiviral protein acts synergistically with an interferon-induced factor for maximal activity against alphaviruses. J Virol 81:13509–13518
Mackenzie JS, Lindsay MD, Coelen RJ, Broom AK, Hall RA, Smith DW (1994) Arboviruses causing human disease in the Australasian zoogeographic region. Arch Virol 136:447–467
Malherbe H, Strickland-Cholmley M, Jackson AL (1963) Sindbis virus infection in man. Report of a case with recovery of virus from skin lesions. S Afr Med J 37:547–552
Marcus PI, Fuller FJ (1979) Interferon induction by viruses. II. Sindbis virus: interferon induction requires one-quarter of the genome—genes G and A. J Gen Virol 44:169–177
Mcfarland HF, Griffin DE, Johnson RT (1972) Specificity of the inflammatory response in viral encephalitis. I. Adoptive immunization of immunosuppressed mice infected with Sindbis virus. J Exp Med 136:216–226
Mcknight KL, Simpson DA, Lin SC et al (1996) Deduced consensus sequence of Sindbis virus strain AR339: mutations contained in laboratory strains which affect cell culture and in vivo phenotypes. J Virol 70:1981–1989
Mendoza QP, Stanley J, Griffin DE (1988) Monoclonal antibodies to the E1 and E2 glycoproteins of Sindbis virus: definition of epitopes and efficiency of protection from fatal encephalitis. J Gen Virol 69(Pt 12):3015–3022
Metcalf TU, Griffin DE (2011) Alphavirus-induced encephalomyelitis: antibody-secreting cells and viral clearance from the nervous system. J Virol 85:11490–11501
Metcalf TU, Baxter VK, Nilaratanakul V, Griffin DE (2013) Recruitment and retention of B cells in the central nervous system in response to alphavirus encephalomyelitis. J Virol 87:2420–2429
Meyer KF, Hring CM, Howitt B (1931) The etiology of epizootic encephalomyelitis of horses in the San Joaquin Valley. Science 74:227–228
Mitchell CJ, Niebylski ML, Smith GC et al (1992) Isolation of eastern equine encephalitis virus from Aedes albopictus in Florida. Science 257:526–527
Moench TR, Griffin DE (1984) Immunocytochemical identification and quantitation of the mononuclear cells in the cerebrospinal fluid, meninges, and brain during acute viral meningoencephalitis. J Exp Med 159:77–88
Mokhtarian F, Griffin DE, Hirsch RL (1982) Production of mononuclear cell chemotactic factors during Sindbis virus infection of mice. Infect Immun 35:965–973
Molaei G, Andreadis TG, Armstrong PM et al (2013) Vector-host interactions and epizootiology of eastern equine encephalitis virus in Massachusetts. Vector Borne Zoonotic Dis 13:312–323
Monath TP, Kemp GE, Cropp CB, Chandler FW (1978) Necrotizing myocarditis in mice infected with Western equine encephalitis virus: clinical, electrocardiographic, and histopathologic correlations. J Infect Dis 138:59–66
Morgan IM (1941) Influence of age on susceptibility and on immune response of mice to eastern equine encephalomyelitis virus. J Exp Med 74:115–132
Morgan IM, Schlesinger RW, Olitsky PK (1942) Induced resistance of the central nervous system to experimental infection with equine encephalomyelitis virus: I. Neutralizing antibody in the central nervous system in relation to cerebral resistance. J Exp Med 76:357–369
Morrison TE, Oko L, Montgomery SA et al (2011) A mouse model of chikungunya virus-induced musculoskeletal inflammatory disease: evidence of arthritis, tenosynovitis, myositis, and persistence. Am J Pathol 178:32–40
Murphy FA, Whitfield SG (1970) Eastern equine encephalitis virus infection: electron microscopic studies of mouse central nervous system. Exp Mol Pathol 13:131–146
Nargi-Aizenman JL, Griffin DE (2001) Sindbis virus-induced neuronal death is both necrotic and apoptotic and is ameliorated by N-methyl-D-aspartate receptor antagonists. J Virol 75:7114–7121
Nargi-Aizenman JL, Simbulan-Rosenthal CM, Kelly TA, Smulson ME, Griffin DE (2002) Rapid activation of poly(ADP-ribose) polymerase contributes to Sindbis virus and staurosporine-induced apoptotic cell death. Virology 293:164–171
Nargi-Aizenman JL, Havert MB, Zhang M, Irani DN, Rothstein JD, Griffin DE (2004) Glutamate receptor antagonists protect from virus-induced neural degeneration. Ann Neurol 55:541–549
Ng CG, Griffin DE (2006) Acid sphingomyelinase deficiency increases susceptibility to fatal alphavirus encephalomyelitis. J Virol 80:10989–10999
Nimmannitya S, Halstead SB, Cohen SN, Margiotta MR (1969) Dengue and chikungunya virus infection in man in Thailand, 1962–1964. I. Observations on hospitalized patients with hemorrhagic fever. Am J Trop Med Hyg 18:954–971
Noran HH (1944) Chronic equine encephalitis. Am J Pathol 20:259–267
Olitsky PK, Schlesinger RW, Morgan IM (1943) Induced resistance of the central nervous system to experimental infection with equine encephalomyelitis virus: II. Serotherapy in western virus infection. J Exp Med 77:359–374
Oliver KR, Scallan MF, Dyson H, Fazakerley JK (1997) Susceptibility to a neurotropic virus and its changing distribution in the developing brain is a function of CNS maturity. J Neurovirol 3:38–48
Paessler S, Aguilar P, Anishchenko M, Wang HQ, Aronson J, Campbell G, Cararra AS, Weaver SC (2004) The hamster as an animal model for eastern equine encephalitis—and its use in studies of virus entrance into the brain. J Infect Dis 189:2072–2076
Phillips AT, Stauft CB, Aboellail TA, Toth AM, Jarvis DL, Powers AM, Olson KE (2013) Bioluminescent imaging and histopathologic characterization of WEEV neuroinvasion in outbred CD-1 mice. PLoS One 8:e53462
Postic B, Schleupner CJ, Armstrong JA, Ho M (1969) Two variants of Sindbis virus which differ in interferon induction and serum clearance. I. The phenomenon. J Infect Dis 120:339–347
Potter MC, Baxter VK, Mathey RW, Alt J, Rojas C, Griffin DE, Slusher BS (2015) Neurological sequelae induced by alphavirus infection of the CNS are attenuated by treatment with the glutamine antagonist 6-diazo-5-oxo-l-norleucine. J Neurovirol 21:159–173
Powers AM (2015) Risks to the Americas associated with the continued expansion of chikungunya virus. J Gen Virol 96:1–5
Powers AM, Logue CH (2007) Changing patterns of chikungunya virus: re-emergence of a zoonotic arbovirus. J Gen Virol 88:2363–2377
Powers AM, Brault AC, Tesh RB, Weaver SC (2000) Re-emergence of Chikungunya and O’nyong-nyong viruses: evidence for distinct geographical lineages and distant evolutionary relationships. J Gen Virol 81:471–479
Priya R, Dhanwani R, Patro IK, Rao PV, Parida MM (2013) Differential regulation of TLR mediated innate immune response of mouse neuronal cells following infection with novel ECSA genotype of Chikungunya virus with and without E1:A226V mutation. Infect Genet Evol 20:396–406
Priya R, Patro IK, Parida MM (2014) TLR3 mediated innate immune response in mice brain following infection with Chikungunya virus. Virus Res 189:194–205
Przelomski MM, O’rourke E, Grady GF, Berardi VP, Markley HG (1988) Eastern equine encephalitis in Massachusetts: a report of 16 cases, 1970–1984. Neurology 38:736–739
Randall R, Mills JW, Engel LL (1947) The preparation and properties of a purified equine encephalomyelitis vaccine. J Immunol 55:41–52
Reed DS, Larsen T, Sullivan LJ, Lind CM et al (2005) Aerosol exposure to western equine encephalitis virus causes fever and encephalitis in cynomolgus macaques. J Infect Dis 192:1173–1182
Reisen WK, Chiles RE (1997) Prevalence of antibodies to western equine encephalomyelitis and St. Louis encephalitis viruses in residents of California exposed to sporadic and consistent enzootic transmission. Am J Trop Med Hyg 57:526–529
Reisen WK, Fang Y, Brault AC (2008) Limited interdecadal variation in mosquito (Diptera: Culicidae) and avian host competence for Western equine encephalomyelitis virus (Togaviridae: Alphavirus). Am J Trop Med Hyg 78:681–686
Renault P, Solet JL, Sissoko D et al (2007) A major epidemic of chikungunya virus infection on Reunion Island, France, 2005–2006. Am J Trop Med Hyg 77:727–731
Robin S, Ramful D, LE Seach F, Jaffar-Bandjee MC, Rigou G, Alessandri JL (2008) Neurologic manifestations of pediatric chikungunya infection. J Child Neurol 23:1028–1035
Ross RW (1956) The Newala epidemic. III. The virus: isolation, pathogenic properties and relationship to the epidemic. J Hyg (Lond) 54:177–191
Rowell JF, Griffin DE (1999) The inflammatory response to nonfatal Sindbis virus infection of the nervous system is more severe in SJL than in BALB/c mice and is associated with low levels of IL-4 mRNA and high levels of IL-10-producing CD4+ T cells. J Immunol 162:1624–1632
Rowell JF, Griffin DE (2002) Contribution of T cells to mortality in neurovirulent Sindbis virus encephalomyelitis. J Neuroimmunol 127:106–114
Ryman KD, Klimstra WB, Nguyen KB, Biron CA, Johnston RE (2000) Alpha/beta interferon protects adult mice from fatal Sindbis virus infection and is an important determinant of cell and tissue tropism. J Virol 74:3366–3378
Ryman KD, White LJ, Johnston RE, Klimstra WB (2002) Effects of PKR/RNase L-dependent and alternative antiviral pathways on alphavirus replication and pathogenesis. Viral Immunol 15:53–76
Ryman KD, Meier KC, Gardner CL, Adegboyega PA, Klimstra WB (2007) Non-pathogenic Sindbis virus causes hemorrhagic fever in the absence of alpha/beta and gamma interferons. Virology 368:273–285
Sabattini MS, Monath TP, Mitchell CJ, Daffner JF, Bowen GS, Pauli R, Contigiani MS (1985) Arbovirus investigations in Argentina, 1977–1980. I. Historical aspects and description of study sites. Am J Trop Med Hyg 34:937–944
Sanchez-San Martin C, Liu CY, Kielian M (2009) Dealing with low pH: entry and exit of alphaviruses and flaviviruses. Trends Microbiol 17:514–521
Sawicki DL, Silverman RH, Williams BR, Sawicki SG (2003) Alphavirus minus-strand synthesis and persistence in mouse embryo fibroblasts derived from mice lacking RNase L and protein kinase R. J Virol 77:1801–1811
Schilte C, Couderc T, Chretien F et al (2010) Type I IFN controls chikungunya virus via its action on nonhematopoietic cells. J Exp Med 207:429–442
Schleupner CJ, Postic B, Armstrong JA, Atchison RW, Ho M (1969) Two variants of Sindbis virus which differ in interferon induction and serum clearance. II. Virological characterizations. J Infect Dis 120:348–355
Schoepp RJ, Johnston RE (1993) Directed mutagenesis of a Sindbis virus pathogenesis site. Virology 193:149–159
Schultz KL, Vernon PS, Griffin DE (2015) Differentiation of neurons restricts Arbovirus replication and increases expression of the alpha isoform of IRF-7. J Virol 89:48–60
Scott TW, Weaver SC (1989) Eastern equine encephalomyelitis virus: epidemiology and evolution of mosquito transmission. Adv Virus Res 37:277–328
Sherman LA, Griffin DE (1990) Pathogenesis of encephalitis induced in newborn mice by virulent and avirulent strains of Sindbis virus. J Virol 64:2041–2046
Shirako Y, Strauss JH (1994) Regulation of Sindbis virus RNA replication: uncleaved P123 and nsP4 function in minus-strand RNA synthesis, whereas cleaved products from P123 are required for efficient plus-strand RNA synthesis. J Virol 68:1874–1885
Silva LA, Khomandiak S, Ashbrook AW et al (2014) A single-amino-acid polymorphism in Chikungunya virus E2 glycoprotein influences glycosaminoglycan utilization. J Virol 88:2385–2397
Silverman RH (2007) Viral encounters with 2′,5′-oligoadenylate synthetase and RNase L during the interferon antiviral response. J Virol 81:12720–12729
Silverman MA, Misasi J, Smole S, Feldman HA, Cohen AB, Santagata S, Mcmanus M, Ahmed AA (2013) Eastern equine encephalitis in children, Massachusetts and New Hampshire, USA, 1970–2010. Emerg Infect Dis 19:194–201, quiz 352
Simmons JD, Wollish AC, Heise MT (2010) A determinant of Sindbis virus neurovirulence enables efficient disruption of Jak/STAT signaling. J Virol 84:11429–11439
Singh I, Helenius A (1992) Role of ribosomes in Semliki Forest virus nucleocapsid uncoating. J Virol 66:7049–7058
Snyder JE, Kulcsar KA, Schultz KL et al (2013) Functional characterization of the alphavirus TF protein. J Virol 87:8511–8523
Spuul P, Balistreri G, Kaariainen L, Ahola T (2010) Phosphatidylinositol 3-kinase-, actin-, and microtubule-dependent transport of Semliki Forest virus replication complexes from the plasma membrane to modified lysosomes. J Virol 84:7543–7557
Stanley J, Cooper SJ, Griffin DE (1986) Monoclonal antibody cure and prophylaxis of lethal Sindbis virus encephalitis in mice. J Virol 58:107–115
Strauss JH, Strauss EG (1994) The alphaviruses: gene expression, replication, and evolution. Microbiol Rev 58:491–562
Strizki JM, Repik PM (1995) Differential reactivity of immune sera from human vaccinees with field strains of eastern equine encephalitis virus. Am J Trop Med Hyg 53:564–570
Suthar MS, Shabman R, Madric K, Lambeth C, Heise MT (2005) Identification of adult mouse neurovirulence determinants of the Sindbis virus strain AR86. J Virol 79:4219–4228
Tandale BV, Sathe PS, Arankalle VA et al (2009) Systemic involvements and fatalities during Chikungunya epidemic in India, 2006. J Clin Virol 46:145–149
Taylor RM, Hurlbut HS, Work TH, Kingston JR, Frothingham TE (1955) Sindbis virus: a newly recognized arthropodtransmitted virus. Am J Trop Med Hyg 4:844–862
Taylor A, Herrero LJ, Rudd PA, Mahalingam S (2015) Mouse models of alphavirus-induced inflammatory disease. J Gen Virol 96:221–238
Ten Broeck C, Merrill MH (1933) A serological difference between eastern and western equine encephalomyelitis virus. Proc Soc Exp Biol Med 31:217–220
Thach DC, Kimura T, Griffin DE (2000) Differences between C57BL/6 and BALB/cBy mice in mortality and virus replication after intranasal infection with neuroadapted Sindbis virus. J Virol 74:6156–6161
Thach DC, Kleeberger SR, Tucker PC, Griffin DE (2001) Genetic control of neuroadapted sindbis virus replication in female mice maps to chromosome 2 and associates with paralysis and mortality. J Virol 75:8674–8680
Thiruvengadam KV, Kalyanasundaram V, Rajgopal J (1965) Clinical and pathological studies on chikungunya fever in Madras city. Indian J Med Res 53:729–744
Trgovcich J, Aronson JF, Eldridge JC, Johnston RE (1999) TNFalpha, interferon, and stress response induction as a function of age-related susceptibility to fatal Sindbis virus infection of mice. Virology 263:339–348
Tsetsarkin KA, Vanlandingham DL, Mcgee CE, Higgs S (2007) A single mutation in chikungunya virus affects vector specificity and epidemic potential. PLoS Pathog 3:e201
Tucker PC, Griffin DE (1991) Mechanism of altered Sindbis virus neurovirulence associated with a single-amino-acid change in the E2 Glycoprotein. J Virol 65:1551–1557
Tucker PC, Strauss EG, Kuhn RJ, Strauss JH, Griffin DE (1993) Viral determinants of age-dependent virulence of Sindbis virus for mice. J Virol 67:4605–4610
Tucker PC, Griffin DE, Choi S, Bui N, Wesselingh S (1996) Inhibition of nitric oxide synthesis increases mortality in Sindbis virus encephalitis. J Virol 70:3972–3977
Tucker PC, Lee SH, Bui N, Martinie D, Griffin DE (1997) Amino acid changes in the Sindbis virus E2 glycoprotein that increase neurovirulence improve entry into neuroblastoma cells. J Virol 71:6106–6112
Tyor WR, Wesselingh S, Levine B, Griffin DE (1992) Long term intraparenchymal Ig secretion after acute viral encephalitis in mice. J Immunol 149:4016–4020
Ubol S, Levine B, Lee SH, Greenspan NS, Griffin DE (1995) Roles of immunoglobulin valency and the heavy-chain constant domain in antibody-mediated downregulation of Sindbis virus replication in persistently infected neurons. J Virol 69:1990–1993
Ubol S, Park S, Budihardjo I et al (1996) Temporal changes in chromatin, intracellular calcium, and poly(ADP-ribose) polymerase during Sindbis virus-induced apoptosis of neuroblastoma cells. J Virol 70:2215–2220
Ulug ET, Garry RF, Bose HR Jr (1989) The role of monovalent cation transport in Sindbis virus maturation and release. Virology 172:42–50
Vazeille M, Moutailler S, Coudrier D et al (2007) Two Chikungunya isolates from the outbreak of La Reunion (Indian Ocean) exhibit different patterns of infection in the mosquito, Aedes albopictus. PLoS One 2:e1168
Vernon PS, Griffin DE (2005) Characterization of an in vitro model of alphavirus infection of immature and mature neurons. J Virol 79:3438–3447
Vilcek J (1964) Production of interferon by newborn and adult mice infected with Sindbis virus. Virology 22:651–652
Vogel P, Kell WM, Fritz DL, Parker MD, Schoepp RJ (2005) Early events in the pathogenesis of eastern equine encephalitis virus in mice. Am J Pathol 166:159–171
Wahlberg JM, Garoff H (1992) Membrane fusion process of Semliki Forest virus. I: low pH-induced rearrangement in spike protein quaternary structure precedes virus penetration into cells. J Cell Biol 116:339–348
Wahlberg JM, Bron R, Wilschut J, Garoff H (1992) Membrane fusion of Semliki Forest virus involves homotrimers of the fusion protein. J Virol 66:7309–7318
Weaver SC, Kang W, Shirako Y, Rumenapf T, Strauss EG, Strauss JH (1997) Recombinational history and molecular evolution of western equine encephalomyelitis complex alphaviruses. J Virol 71:613–623
Weaver SC, Powers AM, Brault AC, Barrett AD (1999) Molecular epidemiological studies of veterinary arboviral encephalitides. Vet J 157:123–138
Weaver SC, Winegar R, Manger ID, Forrester NL (2012) Alphaviruses: population genetics and determinants of emergence. Antiviral Res 94:242–257
Webster LT, Wright FH (1938) Recovery of eastern equine encephalomyelitis virus from brain tissue of human cases of encephalitis in Massachusetts. Science 88:305–306
Weiss B, Rosenthal R, Schlesinger S (1980) Establishment and maintenance of persistent infection by Sindbis virus in BHK cells. J Virol 33:463–474
Werneke SW, Schilte C, Rohatgi A, Monte KJ, Michault A, Arenzana-Seisdedos F, Vanlandingham DL, Higgs S, Fontanet A, Albert ML, Lenschow DJ (2011) ISG15 is critical in the control of Chikungunya virus infection independent of UbE1L mediated conjugation. PLoS Pathog 7:e1002322
Wesselingh SL, Levine B, Fox RJ, Choi S, Griffin DE (1994) Intracerebral cytokine mRNA expression during fatal and nonfatal alphavirus encephalitis suggests a predominant type 2 T cell response. J Immunol 152:1289–1297
White J, Helenius A (1980) pH-dependent fusion between the Semliki Forest virus membrane and liposomes. Proc Natl Acad Sci U S A 77:3273–3277
White G, Ottendorfer C, Graham S, Unnasch TR (2011) Competency of reptiles and amphibians for eastern equine encephalitis virus. Am J Trop Med Hyg 85:421–425
Wust CJ, Nicholas JA, Fredin D et al (1989) Monoclonal antibodies that cross-react with the E1 glycoprotein of different alphavirus serogroups: characterization including passive protection in vivo. Virus Res 13:101–112
Zhang W, Mukhopadhyay S, Pletnev SV, Baker TS, Kuhn RJ, Rossmann MG (2002) Placement of the structural proteins in Sindbis virus. J Virol 76:11645–11658
Zhang Y, Burke CW, Ryman KD, Klimstra WB (2007) Identification and characterization of interferon-induced proteins that inhibit alphavirus replication. J Virol 81:11246–11255
Zhang M, Fang Y, Brault AC, Reisen WK (2011) Variation in western equine encephalomyelitis viral strain growth in mammalian, avian, and mosquito cells fails to explain temporal changes in enzootic and epidemic activity in California. Vector Borne Zoonotic Dis 11:269–275
Zichis J, Shaughnessy HJ (1945) Successful treatment of experimental western equine encephalomyelitis with hyperimmune rabbit serum. Am J Public Health Nations Health 35:815–823
Ziegler SA, Lu L, da Rosa AP, Xiao SY, Tesh RB (2008) An animal model for studying the pathogenesis of chikungunya virus infection. Am J Trop Med Hyg 79:133–139
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Griffin, D.E. (2016). Neurotropic Alphaviruses. In: Reiss, C. (eds) Neurotropic Viral Infections. Springer, Cham. https://doi.org/10.1007/978-3-319-33133-1_7
Download citation
DOI: https://doi.org/10.1007/978-3-319-33133-1_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-33131-7
Online ISBN: 978-3-319-33133-1
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)