
Abstract
Keeping employees physically and psychologically healthy and thriving has increasingly become a challenge for organizations. Because poor health is associated with various negative consequences for the individual as well as at organizational level, researchers have started to investigate pathways for fostering, retaining, and restoring health and well-being in the work-place. Various studies underline the important role of leaders in creating work-place conditions that either positively or negatively influence employee health and well-being. In this chapter, we therefore differentiate between relationship-oriented and task-oriented leadership behaviors while providing an overview of the association between established leadership theories and indicators of employee health. Moreover, we focus on health-specific leadership styles, which are assumed to have a more direct effect on followers’ health than more general styles. We have assumed that health-focused leadership skills complement general leadership skills. Avenues for future research are discussed and practical conclusions provided.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Employees’ Health as a Challenge and Corporate Goal
Employees’ physical and psychological health has recently become a prominent topic for both organizational research and practice. There are various possible reasons for this development. First, ample research has demonstrated that poor health and well-being are associated with several negative outcomes on both the company and individual level. For instance, employees with health-related problems have been found to be less productive, to be absent from work more often, and to make poorer-quality decisions and fewer overall contributions to their organizations than their healthy colleagues (Danna and Griffin 1999). In addition, they may personally experience various physiological, psychological, and emotional costs (Bourbeau et al. 1996; Cartwright and Cooper 1993).
Second, recent data from Germany indicate that sick days increased by 28 % between 2006 and 2013. On average, persons in the German workforce miss 14.7 days per year because of poor health, generating considerable costs for both companies and social security systems (TK Gesundheitsreport 2014). Hence, organizations are becoming increasingly interested in exploring how to optimize working conditions to minimize costly sick days.
Third, health statistics from many developed economies indicate that employees’ psychological health is particularly jeopardized. The Organisation for Economic Co-operation and Development (OECD 2014) reported that in Switzerland mental health problems annually cost the economy 19 billion Swiss francs, which corresponds to 3.2 % of the gross domestic product. In addition, people with mental health problems account for almost 40 % of all new disability benefit claims. The situation is similar in Germany, where the number of psychologically induced sick days grew by a factor of 19 between 2004 and 2011, causing the German economy to lose 6.3 billion euros annually (Betriebskrankenkasse [BKK] 2012). While researchers debate whether an apparently more complex working life (e.g., intensified cost pressure, fierce competition, globalization, virtualization, and ubiquity) explains this ongoing increase, it can be concluded that, at minimum, there is a strong interrelationship between work and psychological health. In addition, persons with psychological illnesses are at particular risk of being marginalized in the labor market (Baldridge et al. in press) because of the widespread stigma associated with mental disability (Corrigan et al. 2005).
Fourth, employees’ health can be expected to become increasingly important because of the demographic changes in most industrialized countries, which are characterized by low birth rates, an increasing life expectancy, and the aging of the large baby-boom generation born between 1946 and 1964 (Craig and Paganelli 2000; Truxillo and Fraccaroli 2013). To take pressure off the pension system, there has been an increased rise in the mandatory retirement age in many countries (Börsch‐Supan 2003; Flynn 2010), accompanied by the abolishment of early retirement programs in most firms. Because of the substantial correlation between age and disability (Ilmarinen 1994, 2001; World Health Organization [WHO] 2011), it can be expected that many older employees will develop health constraints during their working lives. In support of this contention, studies show that older employees take more sick days. While persons take sick leave less frequently with increasing age, the duration of that leave increases (Badura et al. 2014). A recent report on workers’ health in German companies revealed that despite employees aged over 50 years comprising less than one third of the overall workforce in 2013, their health issues led to absenteeism corresponding to 46 % of the costs of the missed gross value added (Badura et al. 2014). This equals a loss of productivity of 42.6 billion euros. In addition, it has become much harder to opt out of working life and request early retirement because of health constraints (Muller-Camen et al. 2011). Therefore, now that organizations cannot “rejuvenate” their workforce by routinely dismissing older employees, they have to invest in the work ability of their personnel. Thus, health promotion has become a core component of managing an aging workforce (Boehm et al. 2013).
Taken together, companies face at least two major challenges regarding their employees’ health. To reach organizational goals, they have to invest in health promotion and ensure that their fit and healthy personnel retain a high capacity for work (i.e., they have to engage in prevention behaviors). Meanwhile, to secure the jobs and foster employees’ recovery with existing health constraints, organizations need to engage in activities to restore those employees’ health and well-being (i.e., they have to invest in intervention behaviors). Given both the importance of work for the self-concept of most individuals (Blustein 2008) and the negative economic implications of losing a job because of poor health, both organizations and society as a whole should have a key interest in fostering, retaining, and restoring health in the work-place.
As already stated, organizations seem to have recognized this challenge. Most companies currently invest in corporate health programs and worksite health promotion, including health education, screening, intervention programs, fitness and nutrition programs, and stress management seminars. The positive impact of such health promotion programs upon key financial indicators has been studied and proven extensively (Aldana 2001; Goetzel and Ozminkowski 2008; Heaney and Goetzel 1997; Pelletier 2001), providing further motivation for companies to engage in such activities. Recently, however, both research and practice seem increasingly interested in shedding light on additional organizational factors that might contribute to employees’ long-term health and well-being. It has been proposed that supervisors, particularly the leadership behavior they display to their followers, are one such decisive organizational factor (Gilbreath and Benson 2004).
2 Definition of Employees’ Health and Well-Being
In the preamble to the constitution of the WHO, health is defined as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity” (WHO 1946). Thus, health promotion has to go beyond sickness prevention to also focus on positive states of health. Regarding the relationship between leadership and health, a wide range of different outcomes have been investigated. In accordance with the research tradition of organizational behavior, soft health-related factors have mostly been studied. These have often been subsumed under the umbrella terms of positive and negative employee well-being, which conceptualizes well-being as having two distinct dimensions rather than being a continuum with two poles (Gregersen et al. 2014). Positive health-related outcomes of leadership include job satisfaction, perceived psychological and physical health, safety, and positive moods. Some studies even consider that more distal outcomes such as job performance are health-related (e.g., Kuoppala et al. 2008). Regarding negative health indicators, stress, strain, anxiety, exhaustion, burnout, and depression have been examined (Kelloway and Barling 2010; Kuoppala et al. 2008). However, few studies, and these are mainly in the field of medicine and rehabilitation, have investigated relatively hard outcomes of leadership, such as blood pressure (Karlin et al. 2003), cardiovascular diseases (Wager et al. 2003), work-place injuries and accidents (Mullen and Kelloway 2009), and sick leave and disability pensions (Kuoppala et al. 2008). Broadly speaking, the more objective the health indicator, the fewer empirical studies have been performed.
3 The Relationship Between Leadership and Followers’ Health and Well-Being
Research has clearly indicated that “good” leadership plays a key role in keeping employees healthy and happy (for recent reviews, see Kelloway and Barling 2010; Kuoppala et al. 2008). However, what constitutes “good” leadership in terms of fostering employees’ physical and psychological health is much less clear (Eriksson et al. 2010). Many of the existing studies on the leadership−health relationship have investigated the potential impact of established leadership styles such as leader−member exchange (LMX; e.g., McGee et al. 1987; Rousseau et al. 2008) and transformational leadership (TFL; e.g., Arnold et al. 2007; Sosik and Godshalk 2000).
Another line of research has taken a more focused approach and proposed that health-focused leadership (HFL) styles have a more direct effect on followers’ health than more general leadership styles (e.g., Gurt et al. 2011; Boehm and Baumgärtner 2014). In this chapter, we will present and discuss both of these approaches with the aim of providing readers with a holistic impression of the leadership−health relationship. In so doing, we will also discuss existing gaps in the literature and propose directions for future research.
First, however, we want to provide our definition of leadership. The subject of leadership is possibly one of the best researched topics in organizational behavior. Yukl (2012, p. 66) summarized the essence of leadership in organizations as “influencing and facilitating individual and collective efforts to accomplish shared objectives”. In general, leaders’ behavior can be classified into task-oriented (e.g., developing plans, determining schedules, clarifying goals, setting priorities, monitoring progress); relationship-oriented (e.g., supporting, developing, and empowering employees); change-oriented (e.g., encouraging innovation, facilitating learning, and communicating a vision); and externally oriented activities (e.g., networking, representing, boundary spanning) (Yukl 2006, 2012). In particular, task- and relationship-oriented behaviors seem likely to influence employees’ health and well-being, particularly given that supervisors have power that they can use to reward or penalize health-relevant employee behavior (Kelloway and Barling 2010). Therefore, we will now focus on the potential health impact of relationship-oriented leadership (i.e., consideration behaviors, LMX, and TFL) and task-oriented leadership behaviors (i.e., initiating structure and transactional leadership [TAL]).
4 The Impact of Established Leadership Concepts on Followers’ Health and Well-Being
4.1 Consideration and Initiating Structure
Consideration and initiating structure are two dimensions of a classical leadership concept developed in the 1950s at Ohio State University (Fleishman 1953). The consideration dimension is people-oriented and comprises leader behaviors that target employees’ welfare and foster interpersonal relationships, mutual trust, and friendship (Judge et al. 2004). Consideration-oriented leaders are perceived as being approachable, friendly, and treating followers equally. In contrast, initiating structure is task-oriented. Task-oriented leaders focus on accomplishing goals; they define roles, initiate actions, and organize group activities. They let followers know what is expected of them and request compliance with rules, standards, and procedures (Judge et al. 2004).
Both consideration and initiating structure are reportedly associated with indicators of health. Gregersen et al. (2014) found both consideration and initiating structure to be positively correlated with job satisfaction and general health and negatively with emotional exhaustion, depersonalization, and perceived strain. In a systematic review, Skakon et al. (2010) concluded that consideration is positively associated with the affective well-being of employees and negatively with low stress levels among employees. In their meta-analysis, Kuoppala et al. (2008) found weak evidence for an association between consideration and job satisfaction, very weak evidence for a relationship between consideration and job well-being, weak evidence for a link between consideration and job performance, and very weak evidence for an association between consideration and sick leave. They failed to identify any studies that investigated potential relationships with early retirement.
4.2 Transactional Leadership
Transactional leadership refers to the bargain and exchange processes that typically occur between leaders and their followers (Burns 1978; Bass 1985). Transactional leaders have two dominant behavioral patterns (Howell and Avolio 1993). First, contingent reward refers to the establishment of constructive transactions or exchanges with their followers (Bass 1991). By clarifying the behaviors they expect from their employees and establishing rewards for meeting these demands, they provide motivation for followers to act according to agreed-upon objectives. Rewards may involve the leader’s recognition of work accomplished, bonuses, or merit increases (Judge and Piccolo 2004). Second, “management by exception” describes behavior that includes corrective criticism, negative feedback, and negative reinforcement when employees do not meet organizational demands. These interventions can either be executed actively, by continuously monitoring for and reacting to potential mistakes, or passively, by intervening only when problems arise.
Reported results of research on the health-related implications of TAL are inconsistent. Judge and Piccolo (2004) performed a meta-analysis comparing the effects of transformational, transactional, and laissez-faire leadership on various leadership criteria. Compared with the other leadership styles, they found that contingent reward leadership was the most highly correlated with employee job satisfaction. However, there were too few studies to subject the relationship between management by exception and job satisfaction to meta-analysis. The passive form of management by exception was moderately negatively correlated with group/organization performance; this was not true for the active dimension. In a more recent meta-analysis, Skakon et al. (2010) investigated the effects of different leadership styles on more directly health-related outcomes, such as affective well-being, employee stress, and burnout and reported inconsistent results. While some studies found a significant relationship between TAL and employee stress or well-being, others did not. However, in a current empirical study, Gregersen et al. (2014) provided evidence that contingent reward behavior is positively associated with job satisfaction (r = 0.45) and general health (r = 0.17) and negatively with emotional exhaustion (r = −0.25), depersonalization (r = −0.12), and perceived strain (r = −0.18).
4.3 Transformational Leadership
Transformational leadership has been developed as a strategy for complementing and eventually replacing TAL (Burns 1978). TFL is often defined in terms of its potential effects on individuals, teams, and whole organizations (Van Knippenberg and Sitkin 2013); these include instilling pride, trust, and respect, inspiring innovation and overcoming of the status quo, and shifting motivation from self-interest to collective interest, including higher-order needs; it thus enables followers to perform beyond expectations (Bass 1985; Conger and Kanungo 1987; Shamir et al. 1993). According to Bass and colleagues (Avolio and Bass 2004; Bass 1985; Bass and Riggio 2006), transformational leaders engage in four related, yet distinct leadership behaviors that together form the TFL construct. First, they engage in idealized influence behaviors by providing appropriate role models and showing concern for the ethical and moral dimensions of their activities. Second, they provide inspirational motivation by developing and communicating a compelling vision for their sphere of influence. Third, they ensure intellectual stimulation and foster employees’ thinking, thereby facilitating challenges to the status quo. Finally, they show individualized consideration by providing coaching and developmental activities for each of their followers. Hundreds of studies, including various meta-analyses (De Rue et al. 2011; Judge and Piccolo 2004; Lowe et al. 1996), have provided evidence that there is a positive relationship between TFL and various desirable outcome criteria at all levels of analysis.
As to effects on health, Gregersen et al. (2014) summarized the existing literature as showing a positive relationship between TFL and psychological affective well-being, job satisfaction, and other indicators of well-being and a negative relationship with burnout, stress, and strain. However, they also identified some studies that did not find support a negative relationship between TFL and negative well-being (i.e., stress and burnout). In their own empirical study, the authors confirmed the overall tendency described above and provided support for positive relationships between TFL and job satisfaction and general health, as well as negative relationships between TFL and emotional exhaustion, depersonalization, and perceived strain. This is in accordance with the findings of Judge and Piccolo’s (2004) meta-analysis, which found that TFL is positively associated with followers’ job satisfaction. Furthermore, in their overview of 12 published papers, Skakon et al. (2010) concluded that TFL is positively associated with job satisfaction and affective well-being and negatively with stress and burnout. However, Kuoppala et al. (2008) found only very weak evidence for relationships between TFL and job satisfaction and TFL and job well-being. These authors were unable to find any published studies regarding job performance, sick leave, and early retirement, which underlines the lack of studies investigating relationships between leadership behavior and more objective health-related outcome variables.
4.4 Leader−Member Exchange
Leader−member exchange (Graen 1976; Graen and Uhl-Bien 1995) is potentially the most well-known approach to operationalizing and assessing the quality of relationships between supervisors and their followers. LMX theory proposes that leaders develop different levels of exchange relationships with their followers (Sparrowe and Liden 1997), ranging from close, trusting, and reciprocal high-quality relationships to more exchange-based and formalized low-quality relationships (Gerstner and Day 1997; Graen and Uhl-Bien 1995; Wayne et al. 1997). Ample empirical research, including three meta-analyses, has demonstrated the positive effects of being in a high-quality relationship with one’s supervisor (Dulebohn et al. 2012; Gerstner and Day 1997; Ilies et al. 2007). These positive effects include more job-related information, increased interaction, greater personal concern, and greater job direction, as well as more feedback, support, training, and developmental opportunities from supervisors (Dunegan et al. 1992, 2002; Gerstner and Day 1997).
LMX is reportedly a powerful resource regarding physical and psychological health outcomes. Studies have demonstrated that good-quality relationships are positively associated with employee job satisfaction and well-being and negatively with stress (Skakon et al. 2010). Gregersen et al. (2014) compared different leadership styles with regard to the following indicators of employee health: consideration, initiating structure, TFL, contingent reward, and LMX, and assessed the relationships between these indicators and job satisfaction, general health, emotional exhaustion, depersonalization, and perceived strain. The authors concluded that the quality of the relationship between supervisor and employee is the best predictor for well-being, particularly for job satisfaction, and that the other leadership constructs examined did not add substantial additional variance.
5 The Impact of Health-Focused Leadership Concepts on Followers’ Health and Well-Being
To date, research on the leadership−health relationship has mainly investigated the impact of rather broad leadership theories. However, there is agreement on the usefulness of specific predictors that predict specific behaviors (Ajzen and Fishbein 1977): congruence between predictor and outcome is associated with greater predictive validity (Schneider et al. 2011). Consequently, investigating a leader’s explicit engagement in health-supporting behaviors may be a promising avenue for predicting health-specific outcomes. Despite the promising potential of such a domain-specific leadership style (Barling et al. 2002) in the field of health promotion, theoretical and empirical research on this topic is “almost non-existent” (Gurt et al. 2011, p. 111). We will now describe some new approaches in this domain.
5.1 Health-Specific Leadership
Gurt et al. (2011) introduced the construct of “health-specific leadership (HSL)” as “the leaders’ explicit and therefore visible consideration of and engagement in employee health.” They argued that HSL influences employees’ health via two mechanisms: First, through a leader directly targeting promoting health; and second, through role modeling that positively affects employees’ health-related behaviors. Gurt et al. (2011) also included task- and relationship-related aspects of leadership in the HSL scale. The items in this scale mainly focus on health-promoting communication, more precisely on discussion with and information from the supervisor concerning health-related issues. In their study, Gurt et al. (2011) examined associations between HSL, general leadership behavior, and employee strain (measured by irritation), including three mediating variables (namely, climate for health, role ambiguity, and job satisfaction). They demonstrated that HSL can be clearly differentiated from general leadership practices and that neither HSL nor general leadership is directly associated with irritation. General leadership was significantly related to all three mediators: better climate for health, less role ambiguity, and greater job satisfaction. HSL showed a significantly positive relationship with both role ambiguity and climate for health. In turn, the mediating variables of role ambiguity and job satisfaction were significantly associated with employee irritation.
5.2 Health-Oriented Leadership
Franke et al. (2014) introduced the construct of health-oriented leadership (HoL), which combines follower-directed health-promoting leadership (StaffCare) and self-directed health-promoting leadership (SelfCare). This approach distinguishes StaffCare as an external resource from SelfCare as an internal resource. Whereas leaders more strongly influence the external conditions, such as the task and working context, followers add individual motivational, cognitive, and behavioral factors related to health. Both StaffCare and SelfCare consist of three distinct components; namely, (1) health behavior; (2) value of health; and (3) health awareness. Health behavior comprises actions relevant to the promotion of health. In terms of StaffCare, health behavior refers to creating health-promoting working conditions, reinforcing employees’ health-directed working behavior, and informing employees about issues that are relevant to health. “Value of health” captures the importance attached to health. In StaffCare, value of health is associated with leaders’ concern for the health of their followers and the degree to which they feel responsible for it. Health awareness comprises the degree to which leaders are sensitive and attentive to and reflective about the health of employees and the factors influencing it. The concept is summarized in the “house of HoL” (Franke et al. 2014, p. 143), in which the SelfCare of leaders is the foundation for StaffCare and for role modeling, which, in turn, is related to the SelfCare of followers.
These authors found that StaffCare is associated with followers’ health and well-being, namely with state of health, irritation, health complaints, and work-family conflict. StaffCare explains unique variance in health outcomes beyond TFL. As hypothesized, the relation between StaffCare and the outcome variables was mediated by followers’ health-related attributes (SelfCare). More precisely, the followers’ ratings of their supervisors’ StaffCare were positively related to their SelfCare, which, in turn, was positively linked to their health.
5.3 Health-Focused Leadership
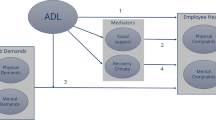
A third approach to health-related leadership behaviors stems from the work of Boehm and Baumgärtner (2014; see also Boehm and Dwertmann 2015 as well as Böhm and Baumgärtner 2016). Drawing from various disciplines such as organizational psychology, medicine, public health, and disability management, Boehm and Baumgärtner (2014) developed a conceptual and empirical model of HFL and postulated that prevention and intervention behaviors are significant predictors of employees’ health. Regarding prevention behaviors, leaders should aim at providing positive resources while avoiding harmful influences on their employees’ health such as constant work overload, overtime, and a paucity of opportunities to recover. Based on Tuomi et al.’s findings (2001) that a non-restful work environment, work overload, and dissatisfaction with work time arrangements negatively affect employees’ ability to work, Boehm and Baumgärtner (2014) suggested that preventive behaviors specifically targeted at reducing such negative factors are likely positively associated with followers’ ability to work. Consequently, supervisors should assign appropriate work-loads that match the personal and organizational resources of their followers (Demerouti et al. 2001). In addition, leaders should ensure that employees are able to achieve their goals within acceptable work hours and without regular overtime or forgoing holidays. Finally, supervisors should try to balance their followers’ demands over the long term, making sure that after periods of intensive engagement there are opportunities for employees to recover and recharge their energy levels (Bruch and Menges 2010; Dwertmann and Kunz 2012).
Second, at the first sign that an employee is ill (including physical and mental illness), leaders should clearly intervene, ensuring that employees understand that their supervisors care about them and their health. Ample research has demonstrated that early interventions are an effective tool for fostering the return-to-work and long-term ability to work of employees who have been absent because of sickness (e.g., Hoefsmit et al. 2012). Moreover, poor leader support correlates positively with the duration of work disability (Janssen et al. 2003; Krause et al. 2001). Therefore, leaders must have a key interest in recognizing employees’ health problems early and in reacting appropriately and in a timely manner. They must clearly communicate to followers that they do not regard illness as a “sign of weakness” and that they understand their employees’ difficulties. Further, leaders should demonstrate that they regard employees’ health as an important resource and that recovery has priority over short-term work goals. For followers with serious health issues, they should try to find joint solutions to handling and improving work conditions such as to support recovery. These solutions could include accommodating the work-place to the employee’s disabilities or restructuring work tasks or work time.
Boehm and Baumgärtner (2014) have developed and empirically tested a model of the two dimensions of HFL. They based their scale development and model testing on a qualitative study involving 153 employees of a German car manufacturer and two quantitative studies, one involving 96 members of the general German working population and the other 1277 employees of a German public service organization. They found that prevention and intervention behaviors are significant predictors of employees’ physical and psychological health states and that these, in turn, have significant relationships with both job performance and turnover intention. In a further study with 2858 employees of a German manufacturing company, they found a negative relationship of HFL with objectively measured sick days (measured in a 6-month period following the survey) over and above a potential effect of LMX.
6 Theoretical Considerations: Leadership and Employees’ Health: Lessons Learnt and Ways Forward
As we have described in this chapter, there is both a growing practical need for and scholarly interest in studying the effects of leadership on employees’ health and well-being. In light of the findings discussed in the previous sections, various avenues for further research seem promising.
First, from a theoretical point of view, it seems worth discussing and analyzing these new health-focused leadership approaches in an integrated manner. More specifically, scholars may wish to investigate how Gurt et al.’s (2011), Franke et al.’s (2014), and Boehm and Baumgärtner’s (2014) approaches relate to each other, what ideas they have in common, and whether they could eventually be combined to develop clear recommendations for the most health-friendly leadership behaviors. On a related aspect, both researchers and practitioners should be keen to ascertain whether these health-focused approaches could extend or replace existing leadership approaches. For instance, can successful leadership behavior be composed of various elements such as goal-oriented TAL as a base, vision- and identity-oriented TFL as a supplement, and a health-focused style as an additional component? Wegge et al. (2014) have recently introduced an integrative model of “five pathways between leadership behavior and employee health” in which they differentiate between interpersonal or dyadic, team or organizational, and environmental or work-system levels. Building on this model and explaining in more depth how leadership behavior at different levels of analysis fosters or hampers health, while simultaneously taking into account relevant moderators and mediators, seems to be strongly indicated.
Second, from an empirical point of view, it seems important to investigate the amount of unique variance in followers’ health and well-being that can be explained by each of these leadership approaches. Gregersen et al.’s study (2014), which compares several leadership approaches within one sample, is an example of such an approach. Such a study should include both established leadership approaches (e.g., LMX, TAL, TFL, authentic leadership, servant leadership) and health-focused approaches (e.g., HSL, HoL, HFL).
Third, and this is related to the previous suggestion, scholars should strive to investigate a variety of health-related outcome variables in such studies. In addition to more well-being-related constructs like job satisfaction, engagement, and commitment, it may be crucial to investigate more health-focused outcomes such as work ability and perceived health. Finally, the inclusion of objective, measurable health indicators such as blood pressure, cortisol concentration, sickness absence, early retirement, and disability pension may be the most promising strategy.
Finally, empirically strong designs should be used to investigate the potential benefits of health-focused leadership approaches. The statement “due to our cross-sectional data, we unfortunately cannot show causality and call for longitudinal and experimental future research” has unfortunately become a commonplace in organizational behavior research; this limitation is particular disappointing in studies on the leadership−health relationship. When investigating the health effects of leadership, researchers should try their utmost to identify effects rather than relationships. One approach to achieving this would be to borrow from medical research and perform randomized controlled trial designs. For example, a randomly selected group of supervisors could be trained and the health of their followers compared with the health of employees of untrained supervisors.
7 Practical Considerations: What Companies Should Do to Foster Employees’ Health and Well-Being
Well-developed health-focused leadership skills complement good general leadership skills and protect employees’ psychological and physical health. Leadership development is a proven effective intervention in occupational health psychology (Kelloway and Barling 2010). Thus, organizations should train their leaders in health-focused leadership behaviors. For instance, they could organize staff training workshops that inform leaders of their responsibility for and effect on their followers’ health. Training content could be based on the job demands-resources model (Demerouti et al. 2001). Informing leaders about both work-related demands and resources and health-focused leadership approaches would provide them with starting points for promoting their employees’ health. Furthermore, leaders who successfully engage in health-focused leadership behaviors could be held up as examples and serve as role models for others. Finally, leaders could be asked to suggest ways of integrating health-focused leadership behaviors into their daily routines.
To create an organization-wide climate of health-focused leadership, these trainings should address different hierarchical levels within the organization. We recommend starting at the top management level and cascading health-focused leadership behaviors down the organization to all supervisors. This is in line with the current trend toward focusing on leadership climates within firms in published reports about leadership (e.g., Boehm et al. 2015).
Moreover, organizations would be well advised to complement trainings in health-focused leadership with other health promotion activities (Heaney and Goetzel 1997) with the aim of fostering a general health-promoting climate (Wilson et al. 2004). Such activities might include health-education programs, medical check-ups and screenings, prevention-oriented changes to the work-place, or individual stress management programs.
References
Ajzen I, Fishbein M (1977) Attitude-behavior relations: a theoretical analysis and review of empirical research. Psychol Bull 84(5):888–918
Aldana SG (2001) Financial impact of health promotion programs: a comprehensive review of the literature. Am J Health Promot 15(5):296–320
Arnold KA, Turner N, Barling J, Kelloway EK et al (2007) Transformational leadership and psychological well-being: the mediating role of meaningful work. J Occup Health Psychol 12(3):193–203
Avolio BJ, Bass BM (2004) Multifactor leadership questionnaire manual and sampler set, 3rd edn. Mind Garden, Redwood City
Badura B, Ducki A, Schröder H, Klose J, Meyer M (eds) (2014) Fehlzeiten-Report 2014: Erfolgreiche Unternehmen von morgen—gesunde Zukunft heute gestalten. Springer, Berlin (in German)
Baldridge D, Beatty J, Boehm SA, Kulkarni M, Moore M (in press) People with (dis)abilities. In Colella AJ, King EB (eds) The Oxford handbook of workplace discrimination. Oxford University Press, New York
Barling J, Loughlin C, Kelloway EK (2002) Development and test of a model linking safety-specific transformational leadership and occupational safety. J Appl Psychol 87(3):488–496
Bass BM (1985) Leadership and performance beyond expectations. Free, New York
Bass BM (1991) From transactional to transformational leadership: learning to share the vision. Organ Dyn 18(3):19–31
Bass BM, Riggio RE (2006) Transformational leadership, 2nd edn. Erlbaum, Mahwah
BKK (Betriebskrankenkassen); Federal Association of Company Health Insurance Funds) (2012) BKK Faktenspiegel—BKK Gesundheitsreport 2012. BKK Factsheet—BKK Health report. BKK Bundesverband, Essen
Blustein DL (2008) The role of work in psychological health and well-being: a conceptual, historical, and public policy perspective. Am Psychol 63(4):228–240
Boehm SA, Baumgärtner MK (2014) Health-focused leadership: prevention and intervention as enablers of followers’ health and performance. Paper presented at the 74th annual meeting of the Academy of Management, Philadelphia, 1–5 Aug 2014
Boehm SA, Dwertmann DJG (2015) Forging a single-edged sword: facilitating positive age and disability diversity effects in the workplace through leadership, positive climates, and HR practices. Work Aging Retire 1(1):41–63
Boehm SA, Schröder H, Kunze F (2013) Comparative age management: theoretical perspectives and practical implications. In: Field J, Burke R, Cooper C (eds) Sage handbook of aging, work and society. Sage, London, pp 211–237
Boehm SA, Dwertmann DJ, Bruch H et al (2015) The missing link? Investigating organizational identity strength and transformational leadership climate as mechanisms that connect CEO charisma with firm performance. Leader Q 26:156–171
Böhm SA, Baumgärtner MK (2016) Gesünder führen. Harv Bus Manag 38(2):6–9
Börsch‐Supan A (2003) Labor market effects of population aging. Labour 17:5–44
Bourbeau J, Brisson C, Allaire S (1996) Prevalence of the sick building syndrome symptoms in office workers before and after being exposed to a building with an improved ventilation system. Occup Environ Med 53(3):204–210
Bruch H, Menges JI (2010) The acceleration trap. Harv Bus Rev 88(3):80–86
Burns JM (1978) Leadership. Harper and Row, New York
Cartwright S, Cooper C (1993) The psychological impact of mergers and acquisitions on the individual: a study of building society managers. Hum Relat 46:327–347
Conger JA, Kanungo RN (1987) Toward a behavioral theory of charismatic leadership in organizational settings. Acad Manage Rev 12(4):637–647
Corrigan PW, Kerr A, Knudsen L (2005) The stigma of mental illness: explanatory models and methods for change. Appl Prevent Psychol 11:179–190
Craig LA, Paganelli V (2000) Phased retirement: reshaping the end of work. Compensat Benefit Manage 16:1–9
Danna K, Griffin RW (1999) Health and well-being in the workplace: a review and synthesis of the literature. J Manage 25(3):357–384
Demerouti E, Bakker AB, Nachreiner F et al (2001) The job demands-resources model of burnout. J Appl Psychol 86(3):499–512
De Rue DS, Nahrgang JD, Wellman NED et al (2011) Trait and behavioral theories of leadership: an integration and meta‐analytic test of their relative validity. Pers Psychol 64(1):7–52
Dulebohn JH, Bommer WH, Liden RC et al (2012) A meta-analysis of antecedents and consequences of leader-member exchange integrating the past with an eye toward the future. J Manage 38(6):1715–1759
Dunegan KJ, Duchon D, Uhl-Bien M (1992) Examining the link between leader member exchange and subordinate performance: the role of task analyzability and variety as moderators. J Manage 18(1):59–76
Dunegan KJ, Uhl-Bien M, Duchon D (2002) LMX and subordinate performance: the moderating effects of task characteristics. J Bus Psychol 17(2):275–285
Dwertmann DJG, Kunz JJ (2012) HR strategies for balanced growth. In: Mennillo G, Schlenzig T, Friedrich E (eds) Balanced growth: finding strategies for sustainable development. Springer, Berlin, pp 137–161
Eriksson A, Axelsson R, Axelsson SB (2010) Development of health promoting leadership—experiences of a training programme. Health Educ 110(2):109–124
Fleishman EA (1953) The description of supervisory behavior. J Appl Psychol 37(1):1–6
Flynn M (2010) The United Kingdom government’s ‘business case’ approach to the regulation of retirement. Ageing Soc 30:421–443
Franke F, Felfe J, Pundt A (2014) The impact of health-oriented leadership on follower health: development and test of a new instrument measuring health-promoting leadership. Z Personalforschung 28(1−2):139–161
Gerstner CR, Day DV (1997) Meta-analytic review of leader–member exchange theory: correlates and construct issues. J Appl Psychol 82(6):827–844
Gilbreath B, Benson PG (2004) The contribution of supervisor behaviour to employee psychological well-being. Work Stress 18(3):255–266
Goetzel RZ, Ozminkowski RJ (2008) The health and cost benefits of work site health-promotion programs. Annu Rev Publ Health 29:303–323
Graen GB (1976) Role making processes within complex organizations. In: Dunnette MD (ed) Handbook of industrial and organizational psychology. Rand-McNally, Chicago, pp 1201–1245
Graen GB, Uhl-Bien M (1995) Relationship-based approach to leadership: development of leader-member exchange (LMX) theory of leadership over 25 years: applying a multi-level multi-domain perspective. Leader Q 6(2):219–247
Gregersen S, Vincent-Höper S, Nienhaus A (2014) Health–relevant leadership behaviour: a comparison of leadership constructs. Z Personalforschung 28(1–2):117–138
Gurt J, Schwennen C, Elke G (2011) Health-specific leadership: is there an association between leader consideration for the health of employees and their strain and well-being? Work Stress 25(2):108–127
Heaney CA, Goetzel RZ (1997) A review of health-related outcomes of multi-component worksite health promotion programs. Am J Health Promot 11(4):290–307
Hoefsmit N, Houkes I, Nijhuis FJ (2012) Intervention characteristics that facilitate return to work after sickness absence: a systematic literature review. J Occup Rehab 22(4):462–477
Howell JM, Avolio BJ (1993) Transformational leadership, transactional leadership, locus of control, and support for innovation: key predictors of consolidated-business-unit performance. J Appl Psychol 78(6):891–902
Ilies R, Nahrgang JD, Morgeson FP (2007) Leader-member exchange and citizenship behaviors: a meta-analysis. J Appl Psychol 92(1):269–277
Ilmarinen J (1994) Aging, work and health. In: Snel J, Cremer R (eds) Work and aging: a European perspective. Taylor and Francis, London, pp 47–63
Ilmarinen J (2001) Aging workers. Occup Environ Med 58:546–552
Janssen N, Van den Heuvel WPM, Beurskens AJHM et al (2003) The demand-control-support model as a predictor of return to work. Int J Rehabil Res 26(1):1–9
Judge TA, Piccolo RF (2004) Transformational and transactional leadership: a meta-analytic test of their relative validity. J Appl Psychol 89(5):755–768
Judge TA, Piccolo RF, Ilies R (2004) The forgotten ones? The validity of consideration and initiating structure in leadership research. J Appl Psychol 89(1):36–51
Karlin WA, Brondolo E, Schwartz J (2003) Workplace social support and ambulatory cardiovascular activity in New York City traffic agents. Psychosom Med 65(2):167–176
Kelloway EK, Barling J (2010) Leadership development as an intervention in occupational health psychology. Work Stress 24(3):260–279
Krause N, Dasinger LK, Deegan LJ et al (2001) Psychosocial job factors and return‐to‐work after compensated low back injury: a disability phase‐specific analysis. Am J Ind Med 40(4):374–392
Kuoppala J, Lamminpää A, Liira J et al (2008) Leadership, job well-being, and health effects—a systematic review and a meta-analysis. Occup Environ Med 50(8):904–915
Lowe KB, Kroeck KG, Sivasubramaniam N (1996) Effectiveness correlates of transformational and transactional leadership: a meta-analytic review of the MLQ literature. Leader Q 7(3):385–425
McGee GW, Goodson JR, Cashman JF (1987) Job stress and job dissatisfaction: influence of contextual factors. Psychol Rep 61:367–375
Mullen JE, Kelloway EK (2009) Safety leadership: a longitudinal study of the effects of transformational leadership on safety outcomes. J Occup Organ Psychol 82(2):253–272
Muller-Camen M, Croucher R, Flynn M et al (2011) National institutions and employers’ age management practices in Britain and Germany: ‘path dependence’ and option exploration. Hum Relat 64:507–530
OECD (2014) Mental health and work: Switzerland, doi:10.1787/9789264204973-en. Available from http://dx.doi.org/10.1787/9789264204973-en. Accessed 27 Jan 2014
Pelletier KR (2001) A review and analysis of the clinical-and cost-effectiveness studies of comprehensive health promotion and disease management programs at the worksite: 1998−2000 update. Am J Health Promot 16(2):107–116
Rousseau V, Aube C, Chiocchio F et al (2008) Social interactions at work and psychological health: the role of leader-member exchange and work group integration. J Appl Soc Psychol 38(7):1755–1777
Schneider B, Erhart MG, Macey WH (2011) Perspectives on organizational climate and culture. In: Zedeck S (ed) Handbook of industrial and organizational psychology. American Psychological Association Press, Washington, pp 373–414
Shamir B, House RJ, Arthur MB (1993) The motivational effects of charismatic leadership: a self-concept based theory. Organ Sci 4(4):577–594
Skakon J, Nielsen K, Borg V et al (2010) Are leaders’ well-being, behaviours and style associated with the affective well-being of their employees? A systematic review of three decades of research. Work Stress 24(2):107–139
Sosik JJ, Godshalk VM (2000) Leadership styles, mentoring functions received, and job-related stress: a conceptual model and preliminary study. J Organ Behav 21(4):365–390
Sparrowe RT, Liden RC (1997) Process and structure in leader-member exchange. Acad Manage Rev 22(2):522–552
TK Gesundheitsreport (2014) Gesundheitsreport 2014—Veröffentlichungen zum Betrieblichen Gesundheitsmanagement der TK, Band 29. Techniker Krankenkasse, Hamburg (in German)
Truxillo DM, Fraccaroli F (2013) Research themes on age and work: introduction to the special issue. Eur J Work Organ Psychol 22(3):249–252
Tuomi K, Huuhtanen P, Nykyri E et al (2001) Promotion of work ability, the quality of work and retirement. Occup Med 51(5):318–324
Van Knippenberg D, Sitkin SB (2013) A critical assessment of charismatic–transformational leadership research: back to the drawing board? Acad Manage Ann 7(1):1–60
Wager N, Fieldman G, Hussey T (2003) The effect on ambulatory blood pressure of working under favourably and unfavourably perceived supervisors. Occup Environ Med 60(7):468–474
Wayne SJ, Shore LM, Liden RC (1997) Perceived organizational support and leader-member exchange: a social exchange perspective. Acad Manage J 40(1):82–111
Wegge J, Shemla M, Haslam SA (2014) Leader behavior as a determinant of health at work: specification and evidence of five key pathways. Z Personalforschung 28(1–2):6–23
WHO (1946) Preamble to the constitution of the World Health Organization as adopted by the international health conference, New York, 19−22 June 1946
WHO (2011) World report on disability 2011. World Health Organization, Geneva
Wilson MG, Dejoy DM, Vandenberg RJ et al (2004) Work characteristics and employee health and well‐being: test of a model of healthy work organization. J Occup Organ Psychol 77(4):565–588
Yukl G (2006) Leadership in organizations, 6th edn. Pearson, Upper Saddle River
Yukl G (2012) Effective leadership behaviors: what we know and what questions need more attention. Acad Manage Perspect 26(4):66–85
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Boehm, S.A., Baumgärtner, M.K., Kreissner, L.M. (2016). The Relationship Between Leadership and Health: A Comparison of General and Health-Focused Leadership Approaches. In: Wiencke, M., Cacace, M., Fischer, S. (eds) Healthy at Work . Springer, Cham. https://doi.org/10.1007/978-3-319-32331-2_7
Download citation
DOI: https://doi.org/10.1007/978-3-319-32331-2_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-32329-9
Online ISBN: 978-3-319-32331-2
eBook Packages: Business and ManagementBusiness and Management (R0)