
Abstract
In the 1950s, the observations of the American surgeon Arnold Kegel led to the recognition of the concept of pelvic floor rehabilitation and to the subsequent use of the muscular portion of the pelvic floor in the treatment of urinary incontinence and genital prolapse. In fact these specific muscular exercises became known as Kegel exercises. In the 1970s, this concept of a therapeutic approach to treat the dysfunctions of the pelvic floor was revived and proposed in Europe, above all by French professionals. Today the most distinguished medical organizations recognize the validity of pelvic floor rehabilitation and consider it a first-line therapeutic approach for the treatment of certain pathological conditions: fecal and urinary incontinence, pelvic organ prolapse, syndrome of chronic pelvic pain, sexual dysfunctions, alterations in the sensory control, and evacuation process of defecation.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Pelvic Floor
- Fecal Incontinence
- Maximum Voluntary Contraction
- Anal Sphincter
- Pelvic Floor Muscle Training
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
7.1 Introduction
In the 1950s, the observations of the American surgeon Arnold Kegel led to the recognition of the concept of pelvic floor rehabilitation and to the subsequent use of the muscular portion of the pelvic floor in the treatment of urinary incontinence and genital prolapse. In fact these specific muscular exercises became known as Kegel exercises. In the 1970s, this concept of a therapeutic approach to treat the dysfunctions of the pelvic floor was revived and proposed in Europe, above all by French professionals. Today the most distinguished medical organizations recognize the validity of pelvic floor rehabilitation and consider it a first-line therapeutic approach for the treatment of certain pathological conditions: fecal and urinary incontinence, pelvic organ prolapse, syndrome of chronic pelvic pain, sexual dysfunctions, alterations in the sensory control, and evacuation process of defecation.
The primary goal of all forms of pelvic floor rehabilitation (RT) is to improve pelvic floor and anal sphincter muscle strength, tone, endurance, and coordination to effect a positive change in function with a decrease in symptoms. Additional goals include increasing the patient’s awareness of their own muscles, improving rectal sensitivity, and reducing scar burden to allow for improved muscle function. Pelvic floor rehabilitation is performed under the guidance of a pelvic floor physical therapist, although nurses, physicians, and other staff can receive training to perform many of these interventions.
Pelvic floor rehabilitation has been used successfully in the treatment of fecal incontinence (FI) and can produce significant functional and quality of life benefits for patients. Most of the reported literature in this area has been in the form of case reports and nonrandomized prospective trials. In fact, more than 70 such uncontrolled studies have been published with a great range of treatment protocols. Almost all these studies show a significant benefit when using a rehabilitative approach, with the majority reporting a positive response range of 50–80 %. There has only been one published nonrandomized study which reported no benefit to treatment. The patients in that study uniformly had FI due to a neurogenic etiology, which might contribute to the lack of demonstrated benefit from pelvic rehabilitation [1].
7.2 Conservative Approaches
Conservative approaches are usually first-line therapy, particularly in patients with mild symptoms, and include dietary modifications, medication, muscle-strengthening exercises (Kegel exercises), biofeedback, and nonsurgical electrical nerve stimulation. Dietary modification, such as avoiding caffeine, citrus fruits, spicy foods, alcohol, and dairy products (in patients with lactose intolerance) may help, but definitive evidence for these restrictions is lacking. Smoking and sedentary lifestyle are associated with FI [2].
Behavior modification can also be explored with patients, including training on the establishment of a predictable pattern of bowel evacuation, timing of defecation relative to activities to limit incontinent episodes, techniques to reduce straining, proper defecation posture when sitting on the toilet, and fecal urge suppression techniques. Weight reduction is typically encouraged, as obesity is a well-documented risk factor for the development of FI [1].
Opinions differ as to whether the addition of dietary fiber is beneficial or detrimental in the treatment of FI; however, methylcellulose is resistant to fermentation by colonic microflora and may be less likely than some other forms of fiber to exacerbate diarrhea. Several medications are also available to treat FI. Antidiarrheal or antimotility agents, including loperamide or diphenoxylate, may be beneficial in patients with loose stools and urgency. Limited evidence suggests that drugs administered to enhance sphincter tone, such as phenylepinephrine and sodium valproate, may be helpful in patients with passive FI and normal anal sphincter function. In a clinical trial, the tricyclic antidepressant amitriptyline improved FI scores (scale, 1–18) from a median of 16 at baseline to 3 (P < 0.001) after 4 weeks of treatment. In an open-label uncontrolled study, clonidine, an alpha 2 adrenergic agonist, improved FI after 4 weeks of therapy; however, a randomized, placebo-controlled study showed that clonidine did not significantly improve the number of episodes of FI or quality of life [3].
Pelvic floor rehabilitation is a term which comprises many different therapeutic approaches, including, but not limited to, pelvic floor muscle training (PFMT) and biofeedback-guided electromyography (EMG), which is currently the most widely used rehabilitative treatment modality. The different rehabilitative techniques can be used independently but more frequently are used in conjunction with one another in a multimodal approach to produce the maximum benefit for the patient. Pelvic floor rehabilitation techniques include pelvic floor muscle training PFMT, biofeedback therapy, and the use of electrical stimulation [1].
7.2.1 Pelvic Floor Muscle Training (PFMT)
Kinesitherapy is a rehabilitative method that alleviates symptoms and obtains the greatest possible recovery of lost or altered function, by utilizing therapeutic exercise and movement of the body or part of it to treat disease [4]. Pelviperineal kinesitherapy or PFMT occupies a very important position in rehabilitation in the fields of urogynecology and proctology.
PFMT describes any number of different approaches for increasing strength, endurance, and coordination of the pelvic floor and anal sphincters. Thoracoabdominal pelvic muscle training has also been advocated, as it has been theorized that training all core muscles to work in tandem would be more effective than a narrow focus on the pelvic floor muscles alone. Particular attention is often paid to the transversus abdominis in such expanded approaches. PFMT typically consists of verbally guided instruction in pelvic floor and sphincter contractions (Kegel contractions).
Anal sphincter exercises are performed to strengthen the puborectalis muscle, which is continuous with the external anal sphincter (EAS) [3]. Patients can be taught to contract in a variety of ways. Some examples include maximal voluntary sustained sphincter contractions, submaximal sustained contractions, and fast-twitch or “quick-flick” contractions. A commonly reported PFMT technique is to compare the pelvic floor to an elevator, able to stop at different floors as it ascends and descends. Other reported methods include working on coordination of anal sphincter activity and working to isolate a contraction of the anal sphincter. Some practitioners use their hand placed externally, or a digit placed vaginally or rectally to help instruct the patient in the correct exercise techniques, but most would argue that this constitutes a form of low-tech biofeedback training.
The techniques are intended to achieve an improvement of the use of the levator ani muscle that carries out a double function: one as a sphincter and the other as an elevator. The aim of the rehabilitator is to facilitate the education, or the reeducation, of the automatisms of the perineal sphincter, according to the principles of motor development, with which we mean the “system by which humans acquire, modify and conserve movement patterns in their memory, so that they may utilize them whenever they desire to, or whenever it is necessary to do so” [5].
Fundamental to this is the use of feedback: function prevalently correlated to the control of posture and movement; regulated in particular by the cerebellum, the basal nuclei, and the frontal lobe; and finalized to refine specific motor programs [4]. The role of central nervous system (CNS) feedback is to detect errors; this enables consequent modification or interruption of altered motor parameters or patterns. This autocorrection initially leads the patient to achieve a refinement of motor skills and, later, after an adequate training period, to adapt to the new environmental body conditions and acquire the automatization of a new motor skill.
With reference to the general principals of rehabilitation, we consider two types of feedback:
-
An intrinsic one that represents all the information that comes from a single patient
-
An extrinsic one that registers stimuli and solicitations supplied by an external agent, the rehabilitator
Therefore, the feedback allows the automatization of the motor skills and functions; the rehabilitator specifically guides the patient during the therapy to experience error, thus making him capable of recognizing and then correcting it and in this way determining an actual effective training process.
The reacquisition phases, known as motor training of the competence of the pelvic floor after pelvic dysfunction or disease, are the following:
-
1.
Acquisition. This is the phase in which the individual begins to acquire or reacquire a particular movement, through a process of awareness of the different motor skills of the pelvic floor (contraction, relaxation, resting state, action of force of gravity).
-
2.
Improvement. Improvement of a given performance and therefore of the altered muscular parameters of the pelvic floor includes hypoactivity, hyperactivity, and impaired coordination of functional activities. The aim here is to improve the quality and efficiency of the performance, reduce the frequency and degree of errors, and increase the safety of the movement. It is necessary for the patient to receive much feedback training, enabling him to adequately elaborate that which he has learned.
-
3.
Automatization. The patient transfers what he has learned during the therapy sessions to the actual symptom when it presents itself during various daily life situations.
From this we deduce that it would be simplistic to think that pelviperineal kinesitherapy specifically only serves to reinforce muscle strength. The concept of strength is not solely dependent on the muscular component but is actually the result of three coordinated factors: mechanical, muscular, and neural. The proposed exercises in rehabilitative treatment should take into account types of posture and the use of functional gestures employed in daily life activities.
The electrical activity at the perineal level is influenced by induction, through recall against resistance of various muscle groups, with individual variability. In particular, these groups are comprised of adductors and pelvic trochanter muscles, including both their abductor and external rotator components. Taking these fundamentals into account, it appears correct in the final phases of the therapeutic procedure to introduce combination exercises for the perineal floor and the agonist muscles, with the aim of strengthening a type of synergy that in the early phases is however inhibited in order to encourage an adequate awakening of the sensations of the perineal floor.
The general principles of muscular exercises take into account the following:
-
1.
Strength: maximum voluntary contraction defined as the recruitment of the greatest possible number of muscle fibers.
-
2.
Power: relationship between maximum strength and the time necessary to obtain it.
-
3.
Endurance: the period of time that the contraction is maintained or repeated.
-
4.
Repetition: the number of times a contraction is repeated with equal strength.
-
5.
Fatigue: exhaustion of the sustainment of the strength required or expected. This is a necessary component for an increase in endurance of muscular exercise [6].
When the muscular deficit is hypoactive, it is then necessary to:
-
(a)
Increase the strength with the use of the maximum voluntary action repeated a few times with the addition of resistance [7]
-
(b)
Increase the endurance and obtain a submaximal contraction [8]
-
(c)
Improve the strength and endurance, with the pause time between contractions lasting double the actual contraction time [9]
-
(d)
Use a maximum voluntary contraction, maintained for a period of 3–10 s, with 8–12 repetitions, performed three times a day; these repetitions are advised to be performed for 5 months. With the aim of obtaining a result [10], it is advised to employ a maximum voluntary contraction for a period of 3–10 s, repeated as many times possible with a rest period of approximately 4 s; this rest period can be reduced when the patient is able to maintain a contraction for 10 s.
Perineal kinesitherapy is organized into progressive sequential phases: a preliminary phase and four specific treatments.
-
1.
Preliminary phase. It is indispensible that the patient and rehabilitator establish a trusting collaborative rapport and that the objectives and steps of the treatment are clearly outlined. The issue of discomfort must be considered and discussed with the patient to help in setting up reasonable goals. The rehabilitator needs to attentively and thoroughly illustrate the ano-pelvic anatomy and physiology, with the aid of anatomic models and mirrors, and provide explanations and examples of the correct anal response. The muscular exercises should be explained and verified with positive verbal reinforcement; the rehabilitative treatment plan must be set up and carefully followed.
The patient must be well informed regarding the preferred strategies chosen to aid in acquiring a satisfactory autonomy while explaining the importance of bowel training and the sharpening of the sensitivity of the evacuation stimulus and the coordination of the action of the muscles of the pelvic floor and abdomen, even during sporadic conditions like the emission of a cough. It is also necessary to evaluate the patient in static equilibrium to correct any eventual postural alterations of the vertebral column and pelvis; these, in fact, constitute an important risk factor to the degree of continence, as relating to the altered distribution of intra-abdominal strength and the involvement of the perineal musculature.
-
2.
Specific treatment.
-
Gaining awareness of the perineal region, The perineal area has a scant primary motor and sensory representation in the brain cortex, with a consequential reduction in the flow of information between the CNS and the peripheral organs. This results in difficulty in learning automatisms that even more frequently, with the aging process, are lost altogether. The first approach, therefore, is proprioceptive, and all the neuromotor reeducation techniques are applied in order to activate the CNS and to provoke, through reflex, an adequate voluntary muscle activity. The techniques used are the placing under tension of the levator ani muscle and the stretch reflex.
-
Elimination of agonist and antagonist synergies. Breathing must be deep and regular. The synergic musculature must not be contracted: the abdominal and pelvic muscles are antagonists.
-
Training of the levator ani muscle. Isotonic and isometric training exercises. The isometric exercises are used to improve the quality of endurance of the levator ani and/or of the external anal sphincter, while the isotonic exercises increase their strength.
-
Automatization of the activity of the perineal musculature in conjunction with daily stress. The exercises in this phase require the proper degree of cortical integration to permit rapid association-dissociation activity of different muscle groups. The patient must acquire at least a correct automatism of the perineal contraction in orthostatism and the regaining and reinforcing of the anal closing reflex under pressure.
-
Kinesitherapy also provides exercises that are to be performed by the patient at home. These exercises are an integral part of the pelvic rehabilitation program and their aim can be outlined in two points:
-
1.
Improvement of the work done with the rehabilitator
-
2.
Maintenance of the acquired results after the termination of the treatment sessions
Only one clinical trial, by Norton et al. in 2003, compared pelvic rehabilitation to a bowel education and retraining program. This study demonstrated comparable benefit in all treatment groups, and the authors concluded that no added benefit was seen with pelvic rehabilitation compared with education alone. However, the education treatment group received instruction in a “bowel urge resistance program” which included training to hold stool in the rectal vault while sitting on the toilet for increasing amounts of time. It is not clear whether such urge suppression techniques are substantially different from pelvic floor muscle strength training with sustained submaximal contractions, and therefore this study’s reported conclusions that there is no benefit from PFMT, apart from educational instruction, may not be valid. PFMT without the concurrent use of biofeedback has been well established for use in patients with urinary incontinence. However, there have not been many trials that have looked at PFMT apart from biofeedback training in the treatment of FI. Three studies have shown digitally taught PFMT to be equivalent to PMFT combined with biofeedback. Only one RCT has been done to evaluate the difference between varied types of pelvic floor exercises. Bartlett et al. in 2011 found no difference in outcomes between two separate PFMT techniques, both trained with biofeedback guidance (sustained submaximal anal and pelvic floor exercises versus rapid squeeze plus sustained submaximal exercises). Both groups had significant improvement in FI [1].
7.2.2 Biofeedback Therapy
Biofeedback therapy (BFB) is a term that can be used to describe many different types of training regimens for the pelvic floor. Biofeedback is defined as the process of gaining greater awareness of many physiological functions, primarily using instruments that provide information on the activity of those same systems, with a goal of being able to manipulate them at will. BFB has been used in medicine for more than 30 years and has been used for the treatment of FI since as early as 1974. For pelvic floor rehabilitation purposes, the most common type of biofeedback is EMG biofeedback therapy, which was first introduced in 1979 [1].
Biofeedback is performed using visual, auditory, or verbal feedback techniques with an anorectal manometry or EMG probe inserted into the anorectum to display pressure changes [11].
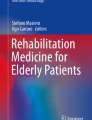
Data are recorded either through surface electrodes or via the use of intravaginal or intrarectal sensors. Other forms of pelvic floor biofeedback therapy include the use of ultrasound (either intrarectal, intravaginal, or perineal), rectal balloons, digital guidance (the use of an intrarectal/intravaginal finger or hand placed on the perineum), and anorectal manometry [1] (Fig. 7.1 ). More recent studies have found a difference between pelvic muscle exercises alone and exercises with biofeedback (the addition of a rectal balloon, electrical stimulation, or EMG), in favor of adding BFB [11].

(a) Vaginal and anorectal probes. (b) Pelvy Tutor System for biofeedback therapy
There are three main methods for the effective use of biofeedback as part of pelvic floor rehabilitation for FI. The most common type is for strength and endurance training for the pelvic floor and/or anal sphincter. The biofeedback apparatus gives information about how strong the muscles are being contracted, and the patient can use that information to learn how to do the pelvic floor exercises more effectively. It is also thought that biofeedback motivates the patient to improve by giving information on performance and progress. The theory behind strength and endurance training is that if the sphincter muscles are stronger, the patient will be able to hold in the stool for a longer period of time and enable them to make it to the restroom with fewer accidents. The second treatment modality is to use biofeedback therapy to improve rectal sensitivity or compliance. This type of treatment has also been termed volumetric rehabilitation or discrimination training and is typically done with rectal balloons. The balloon is inflated with air or water to determine the first sensation of rectal filling. It is then gradually inflated with decreasing amounts of air or water to teach the patient to appreciate stool in the rectal vault at progressively lower volumes. The rationale behind sensory retraining is to allow the patient to detect smaller volumes of stool at an earlier moment, again making it possible for them to reach the restroom before an accident occurs. It also allows for the patient to have more time to perform a voluntary anal sphincter contraction before the volume of stool in the rectal vault overwhelms the patient’s ability to hold it.
Rectal balloons can also be used on patients with fecal urgency and rectal hypersensitivity. The balloons are in these cases simply inflated to progressively larger volumes, which the patient is then coached on how to tolerate without feeling the need to expel the rectal contents.
The third biofeedback therapy approach deals with coordination training for the anal sphincter. Multiple balloons are again inserted, a large one in the rectum itself and one or two smaller ones in the anal canal. These are typically connected to a manometric pressure-recording device. When the larger balloon is inflated, the rectal–anal inhibitory reflex is triggered, and the patient is taught to appreciate the momentary internal anal sphincter relaxation that results. The patient can then be taught to do a voluntary external sphincter contraction to counteract the involuntary relaxation of the internal sphincter.
This type of coordination training is not as commonly studied today as it was in the past. More recent studies have referred to “coordination training” instead as a combination between motor skills training and sensory discrimination training [1].
7.2.3 Electrical Stimulation
Electrical stimulation is another modality that has been proposed for the rehabilitative treatment of FI. The goal of electrical stimulation is to enhance the strength and/or endurance of striated muscle contraction with the target being typically the external anal sphincter in the case of patients with FI. Another goal can be to allow patients with decreased kinesthetic awareness to become more cognizant of where their pelvic floor muscles are in space and what it feels like when the muscles and sphincter are contracting. Electrical stimulation has been shown to transform fast-twitch muscle fibers to slow-twitch muscle fibers, which is thought to help with improving endurance. It also increases capillary density, allowing more blood flow to the oxidative slow-twitch fibers. Electrical stimulation can be delivered to the pelvic floor and anal sphincter in many different forms, including via surface electrodes or intrarectal probes and with many different stimulation parameters and treatment protocols. Low-frequency stimulation (LFS) has typically been the norm, although a new form of amplitude-modulated medium-frequency (AM-MF) stimulation has recently been proposed. All forms of electrical stimulation are often used in conjunction with PFMT or biofeedback training, although stimulation can be used without any other concurrent rehabilitative treatment. Electrical stimulation can also be used to augment a volitional contraction once the contraction threshold reaches a predefined level, and such a strategy has also been employed in trials [1].
7.2.4 Comparison Among Rehabilitative Procedures
There is no universally accepted therapeutic algorithm and no specific criteria for evaluating the efficacy of RT. The techniques used, such as biofeedback therapy, kinesitherapy, anal-electrostimulation, and volumetric rehabilitation, can vary greatly in rehabilitation programs among centers. For this reason, the results of studies are not comparable.
Eighteen randomized trials sustain the use of biofeedback therapy in FI. Biofeedback therapy is aimed at improving voluntary EAS contraction. Another effect is training of synchrony for anal sphincter responses during rectal distention. Finally, biofeedback therapy may be used to improve rectal sensation and sphincter responsiveness to balloon distention with the use of instruments that simultaneously monitor sphincter contractions. Some authors have combined biofeedback therapy with kinesitherapy for the pelvic and perineal muscles as supported by two randomized controlled trials. Nevertheless, when used alone, one randomized controlled trial shows that biofeedback therapy is superior to pelvic floor exercises. RT could improve rectal sensations. Such RT may be performed through biofeedback therapy (“sensory retraining”) or volumetric rehabilitation, using an inflated balloon, or water enemas of decreasing volume. Neither biofeedback therapy nor volumetric rehabilitation is supported by randomized controlled trials.
Anal-electrostimulation can be used to treat FI. The assumption is that anal-electrostimulation can induce muscle contraction by direct stimulation or indirectly via peripheral nerve stimulation. A Cochrane Library review on four randomized trials raised concerns on the utility of anal-electrostimulation in FI because:
-
(a)
In clinical practice anal-electrostimulation would seldom be given in isolation without exercises and other advice
-
(b)
There is no sufficient evidence for assessing the effectiveness of anal-electrostimulation
-
(c)
There is not enough evidence on how to select patients suitable for anal-electrostimulation nor on which modality of electrical stimulation is optimal
Anal sphincter exercises (pelvic floor muscle training) and biofeedback therapy have been used alone and in combination for the treatment of FI.
A single-center randomized controlled study indicated that a regimen of pelvic floor exercises with biofeedback was nearly twice as effective as pelvic floor exercises alone, with 44 % versus 21 % of patients achieving complete continence at 3 months, respectively (P = 0.008). In addition, symptom relief was reported for 76 % of patients using biofeedback and pelvic floor exercises compared with 41 % of patients performing pelvic floor exercises alone (P < 0.01), and patients adjunctively using biofeedback had greater reductions in Fecal Incontinence Severity Index (FISI) scores.
In a more recent randomized study comparing 2 different pelvic floor exercise regimens, both with biofeedback, 59 of the 69 patients (86 %) had improved continence with 20 % fully continent, with no statistically significant differences between exercise regimens.
A 2012 systematic review of randomized or quasi randomized controlled trials of patients performing anal sphincter exercises and/or receiving biofeedback and/or surface electrical stimulation of the anal sphincter concluded that the addition of biofeedback or electrical stimulation was superior to exercise alone in patients who had previously failed to respond to other conservative treatments. As indicated above, nonsurgical (surface) electrical stimulation, alone or in combination with biofeedback, has also proven useful. One study found the combination of electrical stimulation 20 min twice daily, and biofeedback was superior to electrical stimulation alone: 53.8 % of 39 patients receiving the combination were continent at the end of treatment versus none of 41 patients in the electrical stimulation-alone group [3] (Table 7.1).
7.3 Transcutaneous and Percutaneous Posterior Tibial Nerve Stimulation
Transcutaneous and percutaneous posterior tibial nerve stimulations have been tried in patients with FI. In a randomized, double-blind, sham-controlled trial, 144 patients were randomly assigned to receive either active or sham stimulations for 3 months. No statistically significant difference was seen between active and sham transcutaneous electrical nerve stimulation (TENS) in terms of an improvement in the median number of FI/urgency episodes per week. Thirty-four patients (47 %) who received the active TENS treatment exhibited a >30 % decrease in the FI severity score compared with 19 patients (27 %) who received the sham treatment. No differences in delay to postpone defecation, patient self-assessment of treatment efficacy, or anorectal manometry were seen between the two groups [12]. A recent double-blind, randomized controlled trial compared the short-term efficacy of percutaneous tibial nerve stimulation (PTNS) against sham electrical stimulation in adults with fecal incontinence in 227 patients. In this study PTNS given for 12 weeks did not confer significant clinical benefit over sham electrical stimulation in the treatment of adults with fecal incontinence. Further studies are warranted to determine its efficacy in the long term and in patient subgroups (i.e., those with urgency) [13].
7.4 Rehabilitation Versus Other Therapeutic Techniques
There are no suitable trials testing drug treatment versus another conservative treatment including RT. There are no studies on the usefulness of RT before surgery. Only one randomized trial has studied adjuvant biofeedback therapy following sphincter repair: there was no difference between the groups as regards continence scores, but adjuvant biofeedback therapy improved the patient’s QoL. This report confirmed data from previous studies showing partial improvement with biofeedback therapy used after sphincteroplasty. A review on functional disorders after rectal cancer resection examined the effects of rehabilitative treatment on FI taken from 15 papers, including 11 nonrandomized prospective studies. The methodological quality of the studies was evaluated according to the methodological index for nonrandomized studies (MINORS) scale. The review concluded that RT improves postsurgical anorectal function.
Management of Patients Who Do Not Respond to RT
It is not clear how nonresponsive patients should be managed. In one study reported, a mini-irrigation system was used in 50 patients with passive FI and/or evacuation difficulty who had not responded to biofeedback therapy. Two-thirds of the patients believed their symptoms were improved and wanted to continue using the system. Rehabilitation can identify those “nonresponders” who should be next in line for more invasive therapeutic procedures [14].
Medium- and Long-Term Effects of RT
Lasting improvement has been observed in patients with FI up to 1 year after rehabilitative treatment. In a randomized study comparing biofeedback therapy versus kinesitherapy, 53 % of biofeedback therapy patients reported adequate relief at a 12-month follow-up compared with 35 % of patients in the kinesitherapy group. Improvement in fecal urgency and subjective rating of bowel control was also maintained at 2 years of follow-up in incontinent patients who had undergone biofeedback therapy with different exercise regimens [14] (Table 7.2).
References
Scott KM. Pelvic floor rehabilitation in the treatment of fecal incontinence. Clin Colon Rectal Surg. 2014;27:99–105.
Townsend MK, Mattews CA, Whithehead WE, Grodstein F. Risk factors for fecal incontinence in older women. Am J Gastroenterol. 2013;108:113–9.
Rao SSC. Current and emerging treatment options for fecal incontinence. J Clin Gastroenterol. 2014;48:752–64.
Umphred D. Neurological rehabilitation. Mosby Elsevier: St. Louis; 2007.
Shumway-Cook A, Woollacott M. Motor control: theory and practical applications. Baltimore: Lippincott, Williams and Wilkins; 1995.
Haslam J, Laycock J. Biofeedback. In: Haslam J, Laycock J, editors. Therapeutic management of incontinence and pelvic pain pelvic organ disorders. Springer-Verlag London Limited; 2008.
Giruaudo D, Lamberti G. Esercizio terapeutico nel rinforzo muscolare del pavimento pelvico. In: Giraudo- Lamberti, editor. Incontinenza urinaria femminile. Ed. Ermes Bologna, Italy; 2007.
Dorey G, Speakman M, Feneley R, et al. Randomised controlled trial of pelvic floor muscle exercises and manometric biofeedback for erectile dysfunction. Br J Gen Pract. 2004;54:819–25.
Di Benedetto P. Riabilitazione uro-ginecologica. Ed. Minerva Medica, Torino, Italy; 2004.
Bø K, Mørkved S, Frawley H, Sherburn M. Evidence for benefit of transversus abdominis training alone or in combination with pelvic floor muscle training to treat female urinary incontinence: a systematic review. NeurourolUrodyn. 2009;28:368–73.
Meyer I, Richter HE. An evidence-based approach to the evaluation, diagnostic assessment and treatment of fecal incontinence in women. Curr Obstet Gynecol Rep. 2014;3:155–64.
Leroi AM, Siproudhis L, Etienney I, et al. Transcutaneous electrical tibial nerve stimulation in the treatment of fecal incontinence: a randomized trial (CONSORT 1a). Am J Gastroenterol. 2012;107:1888–96.
Knowles CH, Horrocks EJ, Bremner SA et al. CONFIDeNT Study Group. Percutaneous tibial nerve stimulation versus sham electrical stimulation for the treatment of faecal incontinence in adults (CONFIDeNT): a double-blind, multicentre, pragmatic, parallel-group, randomised controlled trial. Lancet. 2015;386(10004):1640–8.
Italian Society of Colorectal Surgery (SICCR), Italian Association of Hospital Gastroenterologists (AIGO). Diagnosis and treatment of faecal incontinence: Consensus statement of the Italian Society of Colorectal Surgery and the Italian Association of Hospital Gastroenterologists. Dig Liv Dis. 2015;47:628–45.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
d’Alba, L., Rivera, M. (2016). Pelvic Floor Rehabilitation. In: Mongardini, M., Giofrè, M. (eds) Management of Fecal Incontinence. Springer, Cham. https://doi.org/10.1007/978-3-319-32226-1_7
Download citation
DOI: https://doi.org/10.1007/978-3-319-32226-1_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-32224-7
Online ISBN: 978-3-319-32226-1
eBook Packages: MedicineMedicine (R0)