
Abstract
Mucinous ovarian carcinoma is a rare tumor, but deserves separate attention, as its clinical behavior is quite different from other types of ovarian carcinoma. This has implications for both surgical therapy as well as adjuvant treatment.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
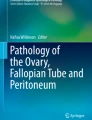
Mucinous carcinoma of the ovary is a rare ovarian cancer that is distinct from other epithelial subtypes based on specific clinical, histologic, and molecular features. Until recently, all epithelial ovarian cancers have been eligible for the same clinical trials, and treatment recommendations have been generalized to specific subtypes. Clinical decision making and prognostic information have been applied in a similar fashion to all subtypes, despite the difference in clinical behavior and outcomes between mucinous ovarian cancer (MOC) and other more common histologic subtypes. Since 2004, the subtleties of MOC have been investigated, and the clinical presentation, biologic behavior, and outcomes data appear to be specific to this histology [1, 2]. Comparative genomic hybridization (CGH) reveals differences between mutational profiles of mucinous and serous ovarian carcinomas. Mucinous carcinomas have fewer alterations (additions or deletions), while serous carcinomas have multiple alterations throughout the genome (Fig. 16.1).

(Courtesy of Drs/Treilleux, D Pissaloux and Pr/Ray-Coquard from centre leon berard, Lyon)
While the low incidence is a barrier to performing effective clinical trials specific to MOC, international involvement has been key to a better understanding of this entity and has resulted in improved diagnostics, assessment, and treatment.
Epidemiology
Mucinous carcinoma of the ovary is a rare subtype of epithelial ovarian cancer. The true incidence has been difficult to determine due to challenges in pathologic diagnosis in differentiating benign, borderline (low malignant potential), and metastatic tumors from primary invasive MOC [3, 4]. Most mucinous tumors are actually benign or borderline neoplasms; benign mucinous tumors account for 10–15 % of all benign ovarian neoplasms [5, 6]. Borderline (low malignant potential) tumors account for 67 % of tumors not considered strictly benign and thus are more common than invasive MOC [7]. Until recently, MOC was thought to account for 5–10 % of epithelial ovarian malignancies, but a systematic review to exclude tumors of low malignant potential and metastatic lesions from gastrointestinal, pancreatic, or other gynecologic primary tumors suggested that MOCs are less common and represent 2.4 % of all epithelial ovarian cancers [4]. Subsequently, Shimada et al. reviewed and reclassified 1400 cases of epithelial ovarian carcinoma. While 16 % were initially diagnosed as primary MOC, upon review only 4.9 % were found to be invasive, with the remainder intraepithelial, borderline, or metastatic in origin [3].
This low incidence is supported by a similar percentage enrollment of mucinous histology in cooperative group trials. In Gynecologic Oncology Group (GOG) trial 111, 14 of 410 patients (3.4 %) had MOC [8]. Intergroup trial IV-10 enrolled 30 of 680 patients (4.4 %) with mucinous histology [9]. Enrollment in GOG trial 132 included 16 of 614 patients (2.6 %) with mucinous histology [10], and enrollment in GOG trial 182 included 71 of 4312 patients (1.6 %) with mucinous histology [11].
The age at diagnosis of MOC is usually described between ages 20–50 years, which is younger than that for epithelial ovarian cancer in general [12]. While family history does not appear to be a risk factor, a history of smoking is associated with a twofold increase in the incidence of both invasive and borderline disease [13].
Pathology
The diagnosis and classification of mucinous tumors has been problematic and controversial. Accurate diagnosis is essential for appropriate treatment, as standard approaches for serous epithelial ovarian cancer are futile, failure to diagnose benign or borderline histology results in overtreatment, and failure to identify ovarian disease as metastatic leads to a missed diagnosis of a gastrointestinal primary and incorrect therapy [2].
Upon gross inspection, these tumors are typically large, unilocular, or multilocular cysts filled with mucoid liquid that becomes gelatinous at room temperature. The mean size at diagnosis is 18 cm, but these tumors can be massive and fill the abdomen and pelvis [1, 14].
The World Health Organization lists specific criteria for the diagnosis of intestinal-type mucinous borderline tumor. These include the following: (1) tumors contain cystic spaces lined by gastrointestinal-type mucinous epithelium with stratification and may form filiform papillae with at least minimal stromal support, (2) nuclei are slightly larger than those seen in cystadenomas, (3) mitotic activity is present, and (4) goblet cells and sometimes Paneth cells are present but stromal invasion is absent [15]. Marked cytologic atypia without stromal invasion represents intraepithelial carcinoma and is a separate entity [2].
The diagnosis of invasive mucinous carcinoma rests on the presence of stromal invasion more than 5 mm in depth or more than 10 mm in area. Invasive MOC is further subdivided into expansile (confluent) and infiltrative types. The expansile (confluent) type consists of a glandular growth pattern without intervening normal ovarian parenchyma, whereas the infiltrative pattern consists of glands, nest, or individual cells which infiltrate the stroma; the latter appears to be more clinically aggressive [16, 17].
The challenge of differentiating among these subtle diagnoses is compounded by the frequent coexistence of benign, borderline, intraepithelial, and/or invasive mucinous carcinoma within one mass. While this may suggest a continuum of malignancy from benign to invasive disease, direct evidence is lacking. These issues make accurate intraoperative diagnosis difficult due to limitations of sampling and time. The tumor size and coexistence of multiple degrees of malignancy may also lead to failure to diagnose a small focus of carcinoma within a large benign or borderline tumor [15].
An additional challenge in mucinous carcinoma is determining whether the source of the tumor is primary in the ovary or metastatic from another site. Primary ovarian tumors tend to be more often unilateral and larger than metastatic tumors (16–20 cm versus 11–12 cm). However, large size is not specific to primary disease, as 32–48 % of metastatic tumors are over 10 cm [1, 14]. Primary ovarian tumors are more likely to have coexistent benign or borderline components, an expansile (confluent) pattern of invasion, and other ovarian pathologies (e.g., mural nodule, Brenner tumor, or teratoma). Metastatic disease is more often associated with a prominent desmoplastic response, nodular or infiltrative pattern of invasion, small clusters of tumor cells within corpora lutea or albicantia, numerous pools of mucin dissecting the ovarian stroma (i.e., pseudomyxoma ovarii) in the absence of a coexistent teratoma, extensive signet-ring cell pattern, ovarian surface involvement, vascular invasion, and hilar involvement [18]. The most common primary sites for disease metastatic to the ovary are gastrointestinal, pancreas, cervix, breast, and uterus, and these sites should be clearly investigated as a source of malignancy when metastatic disease is suspected [4].
Molecular Biology and Genetics
Mucinous and serous epithelial ovarian cancers have distinct molecular characteristics, further supporting the functional separation between these histologic subtypes. In contrast to serous carcinomas, K-ras mutations are identified in 43–65 % of MOCs, mucinous borderline tumors, and mucinous cystadenomas [12, 17, 19–21]. Mutations in the p53 tumor suppressor gene occur less frequently than in serous ovarian carcinomas but are present in some cases (16 % versus 60 %) [22]. Gene expression profiling also differs between serous and mucinous histologies [23, 24]. MOC does not appear to be linked to BRCA gene mutations, as only about 2 % of ovarian cancers associated with BRCA mutations are of mucinous histology [25, 26]. One recent study has identified amplification of Her2 in 19 % of mucinous tumors, which may provide a rationale for directed therapy in these cancers [27, 28].
Other immunohistochemical and molecular alterations characterize mucinous tumors [29–32]. Mucinous tumors are more likely to express E-cadherin and less likely to express N-cadherin than serous tumors [33]. Matrix metalloproteinases and WT-1 have also been characterized [34]. Src kinase has been recently identified as a targetable non-receptor tyrosine kinase expressed in many MOCs and may represent a therapeutic strategy [35].
Clinical Presentation and Diagnosis
The constellation of symptoms at presentation, unilaterality, stage, lack of lymphatic involvement, and serum tumor markers may suggest a mucinous ovarian neoplasm. These tumors are usually quite large, with a median size of 18 cm, but may be extremely large, presenting with a mass effect or ureteral obstruction [36, 37]. Primary tumors are larger than metastatic tumors, and nearly 80 % of primary mucinous ovarian tumors are unilateral, a feature that distinguishes these tumors from serous ovarian carcinomas and from mucinous cancers metastatic to the ovary [16]. Based on these characteristics, Seidman has developed an algorithm to predict primary ovarian versus metastatic origin, in which a unilateral tumor great than 10 cm correctly predicts primary ovarian origin in 82 % of cases. Conversely, bilateral tumors less than 10 cm accurately predict metastatic disease in 95 % of cases [4].
The stage at diagnosis in primary MOCs is more likely to be early stage than in serous ovarian carcinomas. Whereas 83 % of MOCs are stage I at diagnosis, only 4 % of serous ovarian cancers are stage I at diagnosis [38]. Lymphatic dissemination does not occur in mucinous ovarian tumors, a finding which affects not only stage but also the surgical staging procedure [39].
The profile of serum tumor markers elevated in MOC also suggests the histology and the primary disease site. Serum carcinoembryonic antigen (CEA) and CA19-9 are often elevated in primary mucinous ovarian cancer but to a lesser extent than in colorectal tumors. These markers do not help to determine the site of primary origin [40]. The ratio of CA125 to CEA, when greater than 25, suggests primary ovarian origin [17]. In total, CEA, elevated in over 30 % of all ovarian cancers, is the most useful marker in suggesting a preoperative diagnosis of MOC and in following a patient’s disease course following initial diagnosis. Other biomarkers that tend to be elevated in MOC include CA72-4, matrix metalloproteinase-9, CD40L, insulin-like growth factor-binding protein-1, myeloperoxidase, and tissue plasminogen activator-1 [41].
Initial Treatment
The cornerstone of treatment is surgery. Any suspected ovarian mass should be removed intact, typically with the involved adnexa being removed and sent for intraoperative pathologic evaluation. Pelvic washings are obtained upon entry into the peritoneal cavity. In a woman who has completed childbearing, surgery should consist of total hysterectomy and bilateral salpingo-oophorectomy. A benign mucinous cystadenomy requires no additional surgery. Upon return of pathology indicating a mucinous tumor of low malignant potential or invasive cancer, the entire abdominopelvic cavity is inspected with careful attention to the gastrointestinal tract to evaluate a possible focus of gastrointestinal primary, and the appendix is removed [42–44]. If there is no evidence of extra ovarian disease, the appendix may be retained, but this is controversial, and others advocate appendectomy even in the setting of a benign mucinous tumor [45]. Any extra ovarian disease is removed entirely with the goal of leaving no macroscopic residual disease. If the extent and distribution of disease precludes complete resection, surgery is directed to alleviate patient symptoms, surgery is stopped, and chemotherapy is initiated. Interval debulking surgery proceeds after 3 cycles of neoadjuvant chemotherapy if the patient responds [42, 46]. If no extra ovarian disease is identified, a staging procedure is performed, consisting of peritoneal biopsies, omentectomy, and biopsy of any suspicious area. The incidence of lymphatic metastases is extremely low in mucinous tumors, so lymphadenectomy is omitted from the staging procedure, but enlarged lymph nodes should be removed [39, 47]. Accurate determination of the presence of an invasive component may be difficult at the time of intraoperative pathology evaluation due to the size of the mass [48]. Therefore, staging is performed any time a mucinous tumor of low malignant potential or invasive cancer is identified.
The route of surgery in the setting of known metastatic disease should be through a vertical midline incision. In the absence of known metastatic disease, minimally invasive surgery may be superior in terms of postoperative recovery and is acceptable when the mass can be removed in a specimen retrieval bag without intentional spill or rupture [49, 50]. Rupture of the mass should be avoided, as this upstages the patient and may increase the risk of recurrence. Morcellation in the abdominal cavity or trocar sites should absolutely be avoided [16]. The correct technique involves placing the detached specimen into the specimen retrieval bag and drawing the edges of the bag out through one trocar site, enlarging it if necessary. Once the circumference of the bag opening is externalized, a large bore spinal needle or suction device is used to aspirate the fluid, decompress the cyst, and the mass is removed without contact with the peritoneum, subcutaneous tissues, or skin [51].
Patients who wish to retain childbearing potential may undergo fertility-sparing surgery, with conservation of the normal-appearing uterus and contralateral ovary in early-stage disease. A recent study reported 7 patients with clinically early-stage MOC who underwent fertility-sparing surgery; all were without evidence of recurrence at a median follow-up of 47.3 months, and one patient had a term pregnancy resulting in a live birth [52]. Another study found no differences in recurrence-free or disease-specific survival among 35 patients who underwent fertility-sparing surgery compared with 55 patients who underwent radical surgery for clinically apparent early-stage MOC [53]. Fertility-sparing surgery does not imply ovarian cystectomy, as the involved adnexa should be removed, nor does it obviate the need for staging.
Adjuvant Therapy
Patients with stage IA or IB grade 1 tumors do not require adjuvant therapy. According to the NCCN guidelines, patients with stage IB grade 2 tumors may undergo observation or 3–6 cycles of adjuvant chemotherapy. Patients with stage IC grade 3 disease or greater should receive 3–6 cycles of adjuvant chemotherapy [42]. However, adjuvant chemotherapy in the setting of early disease is not clearly of benefit. The two largest trials of adjuvant chemotherapy in this setting, ICON 1 and ACTION, enrolled a total of 180 patients with a mucinous-type tumor. While 18 % of patients overall relapsed, there were no differences in relapse rate or outcome of the treated patients compared with patients undergoing observation [54].
Definitive recommendations for effective chemotherapy are lacking based on poor results with paclitaxel and carboplatin, chemotherapy that is usually effective in this setting in serous ovarian carcinoma. The results of several retrospective analyses demonstrate resistance to this regimen. The Hellenic Cooperative Group reported a lower response rate (38.5 versus 70 %, p = 0.001) in 47 patients with advanced MOC when compared to 94 matched controls with serous ovarian cancers. Time to progression and overall survival were not significantly different [55]. A similar study from the Royal Marsden Hospital found a similar response rate but lower PFS (5.7 versus 14.1 months) and OS (12.0 versus 36.7 months) among 27 patients with MOC compared with 54 controls with serous ovarian carcinoma [1]. Additionally, a Dutch Cancer Registry showed that patients with advanced-stage MOC have a worse prognosis than patients with advanced-stage serous ovarian carcinoma (11 versus 26 % 5-year survival, p < 0.01) [56].
Although the percentage enrollment of primary MOC is small, pooled data from multiple cooperative group trials have demonstrated the limited efficacy of paclitaxel and carboplatin in patients with MOC (see Prognosis). A pooled analysis of 7 Gynecologic Cancer InterGroup trials including 8704 patients, 264 (3 %) of whom had mucinous tumors, reveals that despite a higher resection rate at primary surgery, the hazard ratio for progression was 2.1 and for death was 2.7 when compared to serous ovarian carcinomas [57]. Additionally, a pooled analysis of GINECO (French cooperative group) found that 5 % of enrolled patients had MOC, and these patients were less likely to have advanced disease and more likely to achieve complete cytoreduction, but had a worse prognosis with a greater proportion of visceral metastases, a lower response rate to paclitaxel and carboplatin, and a shorter progression-free (PFS) and overall survival (OS) when compared with serous ovarian carcinoma [58]. A pooled analysis of 7 Gynecologic Oncology Group (GOG) trials including 1896 patients, 34 (1.8 %) of whom had MOC and received 6 cycles of paclitaxel and carboplatin, revealed that these patients had a worse PFS (10.5 versus 16.9 months) and OS (14.8 versus 45.1 months) when compared with serous carcinoma [59].
The search for alternative, more effective chemotherapy has included regimens utilized for gastrointestinal cancer based on the histologic appearance and biologic similarities. The combination of oxaliplatin and a fluoropyrimidine using either 5-fluorouracil or capecitabine has been used, but there are no published data clearly supporting their use in this setting. An international combined cooperative group trial including the GCIG, GOG, NCRI, and NCT compared oxaliplatin and capecitabine with carboplatin and paclitaxel ± bevacizumab in each arm. This trial had slow accrual so was closed prior to completion [51]. Review of the preliminary results indicates difficulty in accurate diagnosis of primary disease, as many enrolled patients were in fact extraovarian primary malignancies metastatic to the ovary [personal communication, David Gershenson, January 19, 2016]. This highlights the need for prospective pathology evaluation in any trial involving primary MOC.
Recurrent Disease
A paucity of information exists on the treatment of recurrent mucinous ovarian cancer. Patients with platinum-sensitive disease (platinum-free interval greater than 6 months) also appear to do worse than their counterparts with recurrent serous ovarian cancer. In the only study to evaluate outcomes in the recurrent setting, the response rate to second-line treatment with platinum-based chemotherapy was lower in patients with mucinous histology (36 % versus 62 %, p = 0.04), PFS was worse (4.5 versus 8 months, p = 0.03), and OS was worse (17.9 versus 28.8 months, p = 0.003) [60].
Prognosis
The prognosis of MOC varies by stage. Compared to patients with serous ovarian cancer, a greater proportion of patients with MOC are diagnosed at an early stage, and these patients have a 5-year survival of 90.8 % [36]. This is significantly better than the 5-year survival for serous carcinoma of the ovary, reported at 75.9 % [5]. A large analysis of the Dutch Cancer Registry confirmed these findings, demonstrating an improved prognosis for MOCs compared with serous ovarian carcinomas in early-stage disease (79 % versus 73 % 5-year survival, p < 0.01) [56]. Risk of recurrence is also lower than for other histologic subtypes, with a hazard ratio of 0.37, and 5-year survival independent of stage is better for mucinous than for serous when all patients are considered (58 % versus 40 % 5-years survival, p < 0.01) [56, 61]. Similarly, the median OS for over 6000 patients with ovarian cancer in the Swedish family study was also significantly better for mucinous than serous histology (970 versus 34 months) [62]. This is likely due to the preponderance of early-stage disease and its excellent prognosis.
Women with advanced-stage mucinous carcinoma of the ovary, however, do poorly and have a worse outcome than women with other histologic subtypes of ovarian cancer. This was demonstrated in a matched cohort study of patients with stage III and IV disease, in which 27 patients with mucinous ovarian cancer and 54 patients with other histologic subtypes were evaluated. The only factors that differed between groups were PFS (5.7 versus 14.1 months, p < 0.001) and OS (12.0 versus 36.7 months, p < 0.001) [1].
Future Research
Future research centers on finding active agents against MOC. Cell line studies have shown resistance to single-agent platinum and taxane agents, but some activity was demonstrated with oxaliplatin, etoposide, and 5-fluorouracil (5-FU). The most active combination was oxaliplatin and 5-FU. A mouse xenograft model confirmed these findings [63]. This has lead to a clinical trial currently enrolling women in Japan with advanced or recurrent MOC in a single-arm phase II trial of oxaliplatin in combination with S-1, a drug comprised of tegafur, gimeracil, and oteracil [2].
Other investigators have previously evaluated CPT-11 and mitomycin-C [64]. As noted, the GCIG initiated a 4-arm, phase III trial which randomized carboplatin and paclitaxel ± bevacizumab with oxaliplatin and capecitabine ± bevacizumab. The trial closed early due to low accrual [51].
Other areas of interest include the role of Src kinase, a non-receptor tyrosine kinase which regulated tumor progression. This is a mutation targetable with a novel agent which inhibits both Src signaling and pre-tubulin [35]. Additionally, therapeutics targeting the ras pathway may be useful to investigate in the recurrent setting.
Conclusions
Primary mucinous ovarian cancer is a distinct entity which differs from other histologic subtypes. Surgical management, including fertility-sparing surgery, is key in the management of these tumors. Early-stage tumors do not require chemotherapy and have an excellent prognosis. Late-stage and recurrent tumors, however, do not have a defined therapy at this time, as paclitaxel and carboplatin are not useful in this setting. Current research focuses on identifying active combination regimens and targeted therapy potentially useful in managing this difficult disease.
References
Hess V, A’Hern R, Nasiri N, et al. Mucinous epithelial ovarian cancer: a separate entity requiring specific treatment. J Clin Oncol. 2004;22:1040–4.
Frumovitz M, Schmeler KM, Malpica A, et al. Unmasking the complexities of mucinous ovarian carcinoma. Gynecol Oncol. 2010;117:491–6.
Shimada M, Kigawa J, Ohishi Y, et al. Clinicopathological characteristics of mucinous adenocarcinoma of the ovary. Gynecol Oncol. 2009;113:331–4.
Seidman JD, Kurman RJ, Ronnett BM. Primary and metastatic mucinous adenocarcinomas in the ovaries: incidence in routine practice with a new approach to improve intraoperative diagnosis. Am J Surg Pathol. 2003;27:985–93.
Mondal SK, Banyopadhyay R, Nag DR, et al. Histologic pattern, bilaterality and clinical evaluation of 957 ovarian neoplasms: a 10-year study in a tertiary hospital in eastern India. J Cancer Res Ther. 2011;4:433–7.
Koonings PP. Relative frequencies of primary ovarian neoplasms: a 10-year review. Obstet Gynecol. 1989;74:921–6.
Shappell HW, Riopel MA, Smith Sehdev AE, et al. Diagnostic criteria and behavior of ovarian seromucinous (endocervical-type mucinous and mixed cell-type) tumors: atypical proliferative (borderline) tumors, intraepithelial, microinvasive, and invasive carcinomas. Am J Surg Pathol. 2002;26:1529–41.
McGuire WP, Hoskins WJ, Brady MF, et al. Cyclophosphamide and cisplatin compared with paclitaxel and cisplatin in patients with stage III and stage IV ovarian cancer. N Engl J Med. 1996;334:1–6.
Piccart MJ, Bertelsen K, James K, et al. Randomized intergroup trial of cisplatin–paclitaxel versus cisplatin–cyclophos-phamide in women with advanced epithelial ovarian cancer: three-year results. J Natl Cancer Inst. 2000;92:699–708.
Muggia FM, Braly PS, Brady MF, et al. Phase III randomized study of cisplatin versus paclitaxel versus cisplatin and paclitaxel in patients with suboptimal stage III or IV ovarian cancer: a gynecologic oncology group study. J Clin Oncol. 2000;18:106–15.
Bookman MA, Brady MF, McGuire WP, et al. Evaluation of new platinum-based treatment regimens in advanced-stage ovarian cancer: a Phase III Trial of the Gynecologic Cancer Intergroup. J Clin Oncol. 2009;27:1419–25.
Kelemen LE, Kobel M. Mucinous carcinomas of the ovary and colorectum: different organ, same dilemma. Lancet Oncol. 2011;12:1071–80.
Collaborative Group on Epidemiological Studies of Ovarian C; Beral V, Gaitskell K, et al. Ovarian cancer and smoking: individual participant meta-analysis including 28,114 women with ovarian cancer from 51 epidemiological studies. Lancet Oncol. 2012;13:946–56.
Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63:11–30.
Chiesa AG, Deavers MT, Veras E, et al. Ovarian intestinal type mucinous borderline tumors: are we ready for a nomenclature change? Int J Gynecol Pathol. 2010;29:108–12.
Lee KR, Scully RE. Mucinous tumors of the ovary: a clinicopathologic study of 196 borderline tumors (of intestinal type) and carcinomas, including an evaluation of 11 cases with ‘pseudomyxoma peritonei’. Am J Surg Pathol. 2000;24:1447–64.
Rodriguez IM, Prat J. Mucinous tumors of the ovary: a clinicopathologic analysis of 75 borderline tumors (of intestinal type) and carcinomas. Am J Surg Pathol. 2002;26:139–52.
Lee KR, Young RH. The distinction between primary and metastatic mucinous carcinomas of the ovary: gross and histologic findings in 50 cases. Am J Surg Pathol. 2003;27:281–92.
Gemignani ML, Schlaerth AC, Bogomolniy F, et al. Role of KRAS and BRAF gene mutations in mucinous ovarian carcinoma. Gynecol Oncol. 2003;90:378–81.
Mok SC, Bell DA, Knapp RC, et al. Mutation of K-ras protooncogene in human ovarian epithelial tumors of borderline malignancy. Cancer Res. 1993;53:1489–92.
Mackenzie R, Kommoss S, Winterhoff BJ, et al. Targeted deep sequencing of mucinous ovarian tumors reveals multiple overlapping RAS-pathway activating mutations in borderline and cancerous neoplasms. BMC Cancer. 2015;15:415. doi:10.1186/s12885-015-1421-8.
Schuijer M, Berns EM. TP53 and ovarian cancer. Hum Mutat. 2003;21:285–91.
Marchini S, Mariani P, Chiorino G, et al. Analysis of gene expression in early-stage ovarian cancer. Clin Cancer Res. 2008;14:7850–60.
Heinzelmann-Schwarz VA, Gardiner-Garden M, Henshall SM, et al. A distinct molecular profile associated with mucinous epithelial ovarian cancer. Br J Cancer. 2006;94:904–13.
Risch HA, McLaughlin JR, Cole DE, et al. Prevalence and penetrance of germline BRCA1 and BRCA2 mutations in a population series of 649 women with ovarian cancer. Am J Hum Genet. 2001;68:700–10.
Evans DG, Young K, Bulman M, et al. Probability of BRCA1/2 mutation varies with ovarian histology: results from screening 442 ovarian cancer families. Clin Genet. 2008;73:338–45.
Anglesio MS, Kommoss S, Tolcher MC, et al. Molecular characterization of mucinous ovarian tumours supports a stratified treatment approach with HER2 targeting in 19% of carcinomas. J Pathol. 2013;229:111–20.
McAlpine JN, Wiegand KC, Vang R, et al. HER2 overexpression and amplification is present in a subset of ovarian mucinous carcinomas and can be targeted with trastuzumab therapy. BMC Cancer. 2009;9:433.
Vang R, Gown AM, Barry TS, et al. Cytokeratins 7 and 20 in primary and secondary mucinous tumors of the ovary: analysis of coordinate immunohistochemical expression profiles and staining distribution in 179 cases. Am J Surg Pathol. 2006;30:1130–9.
Moh M, Krings G, Ates D, Aysal A, Kim GE, Rabban JT. SATB2 expression distinguishes ovarian metastases of colorectal and appendiceal origin from primary ovarian tumors of mucinous or endometrioid type. Am J Surg Pathol. 2016;40:419–32.
Cao D, Ji H, Ronnett BM. Expression of mesothelin, fascin, and prostate stem cell antigen in primary ovarian mucinous tumors and their utility in differentiating primary ovarian mucinous tumors from metastatic pancreatic mucinous carcinomas in the ovary. Int J Gynecol Pathol. 2005;24:67–72.
Oien KA. Pathologic evaluation of unknown primary cancer. Semin Oncol. 2009;36:8–37.
Sarrio D, Moreno-Bueno G, Sanchez-Estevez C, et al. Expression of cadherins and catenins correlates with distinct histologic types of ovarian carcinomas. Hum Pathol. 2006;37:1042–9.
Brun JL, Cortez A, Commo F, Uzan S, Rouzier R, Darai E. Serous and mucinous ovarian tumors express different profiles of MMP-2, -7, -9, MT1-MMP, and TIMP-1 and -2. Int J Oncol. 2008;33:1239–46.
Matsuo K, Masato M, Nishimura M, et al. Targeting Src in mucinous ovarian carcinoma. Clin Cancer Res. 2011;17:5367–78.
Riopel MA, Ronnett BM, Kurman RJ. Evaluation of diagnostic criteria and behavior of ovarian intestinal-type mucinous tumors: atypical proliferative (borderline) tumors and intraepithelial, microinvasive, invasive, and metastatic carcinomas. Am J Surg Pathol. 1999;23:617–35.
Tait DL, Miller DS. Multicystic ovarian tumor weighing 156 lbs: the second largest tumor in Texas. Tex Med. 1997;93:89.
Seidman JD, Horkayne-Szakaly I, Haiba M, et al. The histologic type and stage distribution of ovarian carcinomas of surface epithelial origin. Int J Gynecol Pathol. 2004;23:41–4.
Schmeler KM, Tao X, Frumovitz M, et al. Prevalence of lymph node metastasis in primary mucinous carcinoma of the ovary. Obstet Gynecol. 2010;116:269–73.
Kelly PJ, Archbold P, Price JH, et al. Serum CA19.9 levels are commonly elevated in primary ovarian mucinous tumours but cannot be used to predict the histological subtype. J Clin Pathol. 2010;63:169–73.
Nolen B, Marrangoni A, Velikokhatnaya L, et al. A serum based analysis of ovarian epithelial tumorigenesis. Gynecol Oncol. 2009;112:47–54.
NCCN guidelines – ovarian cancer. Version 2.2013. Accessed on 20 Jan 2016.
Schilder JM, Thompson AM, DePriest PD, et al. Outcome of reproductive age women with stage IA or IC invasive epithelial ovarian cancer treated with fertility-sparing therapy. Gynecol Oncol. 2002;87:1–7.
Wright JD, Shah M, Mathew L, et al. Fertility preservation in young women with epithelial ovarian cancer. Cancer. 2009;115:4118–26.
Lin JE, Seo S, Kushner DM, Rose SL. The role of appendectomy for mucinous ovarian neoplasms. Am J Obstet Gynecol. 2013;208:46e41–4.
Bristow RE, Tomacruz RS, Armstrong DK, et al. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: a meta-analysis. J Clin Oncol. 2002;20:1248–59.
Cho YH, Kim DY, Kim JH, et al. Is complete surgical staging necessary in patients with stage I mucinous epithelial ovarian tumours? Gynecol Oncol. 2006;103:878–82.
Naik JD, Seligmann J, Perren TJ. Mucinous tumours of the ovary. J Clin Pathol. 2012;65:580–4.
Leys CM, Gasior AC, Hornberger LH, St. Peter SD. Laparoscopic resection of massive ovarian mucinous cystadenoma. J Laparoendosc Adv Surg Tech. 2012;22:307–10.
Eltabbakh GH, Charbonneau AM, Eltabbakh NG. Laparoscopic surgery for large benign ovarian cysts. Gynecol Oncol. 2008;108:72–6.
Ledermann JA, Luvero D, Shafer A, O’Connor D, Mangili G, Friedlander M, Pfisterer J, Mirza MR, Kim JW, Alexandre J, Oza A, Brown J. Gynecologic Cancer InterGroup (GCIG) consensus review for mucinous ovarian carcinoma. Int J Gynecol Cancer. 2014;24(9 Suppl 3):S14–9.
Park JY, Heo EJ, Lee JW, Lee YY, Kim TJ, Kim BG, Bae DS. Outcomes of laparoscopic fertility-sparing surgery in clinically early-stage epithelial ovarian cancer. J Gynecol Oncol. 2016;27(2):e20.
Lee JY, Kim TH, Kim HS, Kim MA, Kim JW, Parek NH, Song YS. Safety of fertility-soaring surgery in primary mucinous carcinoma. Cancer Res Treat. 2015;47(2):290–7.
Trimbos JB, Parmar M, Vergote I, et al. International Collaborative Ovarian Neoplasm trial 1 and Adjuvant ChemoTherapy In Ovarian Neoplasm trial: two parallel randomized phase III trials of adjuvant chemotherapy in patients with early- stage ovarian carcinoma. J Natl Cancer Inst. 2003;95:105–12.
Pectasides D, Fountzilas G, Aravantinos G, et al. Advanced stage mucinous epithelial ovarian cancer: the Hellenic Cooperative Oncology Group experience. Gynecol Oncol. 2005;97:436–41.
Simons M, Ezendam N, Bulten J, Nagtegall I, Massuger L. Survival of patients with mucinous ovarian carcinoma and ovarian metastases: a population-based cancer registry study. Int J Gynecol Cancer. 2015;25(7):1208–15.
Mackay HJ, Brady MF, Oza AM, et al. Prognostic relevance of uncommon ovarian histology in women with stage III/IV epithelial ovarian cancer. Int J Gynecol Cancer. 2010;20:945–52.
Alexandre J, Ray-Coquard I, Selle F, et al. Mucinous advanced epithelial ovarian carcinoma: clinical presentation and sensitivity to platinum-paclitaxel-based chemotherapy, the GINECO experience. Ann Oncol. 2010;21:2377–81.
Winter WE, Maxwell GL, Tian C, et al. Prognostic factors for stage III epithelial ovarian cancer: a gynecologic oncology group study. J Clin Oncol. 2007;25:3621–7.
Pignata S, Ferrandina G, Scarfone G, et al. Activity of chemotherapy in mucinous ovarian cancer with a recurrence free interval of more than 6 months: results from the SOCRATES retrospective study. BMC Cancer. 2008;8:252.
Vergote I, De Brabanter J, Fyles A, et al. Prognostic importance of degree of differentiation and cyst rupture in stage I invasive epithelial ovarian carcinoma. Lancet. 2001;357:176–82.
Ji J, Forsti A, Sundquist J, Lenner P, Hemminki K. Survival in ovarian cancer patients by histology and family history. Acta Oncol. 2008;47:1133–9.
Sato S, Itamochi H, Kigawa J, et al. Combination chemotherapy of oxaliplatin and 5-fluorouracil may be an effective regimen for mucinous adenocarcinoma of the ovary: a potential treatment strategy. Cancer Sci. 2009;100:546–51.
Shimizu Y, Umezawa S, Hasumi K. A phase II study of combined CPT-11 and mitomycin-C in platinum refractory clear cell and mucinous ovarian carcinoma. Ann Acad Med Singapore. 1998;27:650–6.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Brown, J., Frumovitz, M. (2017). Mucinous Carcinoma of the Ovary. In: Pujade-Lauraine, E., Ray-Coquard, I., Lécuru, F. (eds) Ovarian Cancers. Springer, Cham. https://doi.org/10.1007/978-3-319-32110-3_16
Download citation
DOI: https://doi.org/10.1007/978-3-319-32110-3_16
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-32108-0
Online ISBN: 978-3-319-32110-3
eBook Packages: MedicineMedicine (R0)