
Abstract
Recognizing the cutaneous manifestations of child abuse, including physical and sexual abuse, is an important component of the medical evaluation in both the hospital-based and outpatient setting. Subtle clues on the skin examination may indicate the need for further evaluation, and the provider needs to be able to distinguish the features of injuries suspicious for non-accidental trauma from accidental skin injuries, medical conditions such as vasculitis, and skin signs of cultural practices such as cupping. Clinicians should also be able to recognize the signs of child neglect, in particular in high-risk situations or in cases where child abuse is also suspected. With regard to anogenital skin findings, sexual abuse should be considered when the lesions present indicate trauma. Finally, the possibility of self-induced skin lesions should always be considered when the history and/or examination is not consistent with a defined skin disorder.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Child physical abuse
- Child sexual abuse
- Child neglect
- Ecchymoses
- Thermal burn
- Factitious disorder
- Pathological skin picking
Case 11.1
History
A healthy 22-month-old male was admitted to the hospital by his primary care pediatrician due to a petechial rash and lethargy . He had been acting well at home until the day of admission, when his mother noted he was tired appearing, fussy, and had developed a rash on his face. He had no fevers, vomiting, cough, abdominal pain, or pruritus. He was home with a babysitter during the day of admission while mother was at work. The babysitter did not report any trauma and stated that the rash developed after she gave him a piece of chocolate, and she thought he was having an allergic reaction. After giving him a dose of diphenhydramine with no change in symptoms or rash, the babysitter called his mother who came home early and brought him to the primary care pediatrician . Mother reports that he has met all appropriate developmental milestones.
Physical Exam
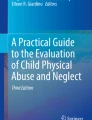
On physical examination , he is tired appearing and fussy. He is afebrile and mildly tachycardic. He has petechiae on his right ear, including the helix, antihelix, and posterior pinna, with small underlying ecchymoses (Fig. 11.1). Petechiae are also noted in the postauricular area without Battle’s sign. A few scattered petechiae are seen just inferior to the right eye. The tympanic membranes are normal without perforation or hemotympanum. He has no apparent abdominal pain and no joint swelling or tenderness. Neurologic assessment is grossly nonfocal.

On physical examination, grouped petechiae are noted on the pinna, helix, and antihelix
Laboratory Parameters
-
White blood cells: 11.4 (6.0–17.0 K/mcL)
-
Hemoglobin: 11.7 (11.5–13.5 g/dL)
-
Platelet count: 215 (135–466 K/mcL)
-
C-reactive protein: <0.21 (<+0.30 mg/dL)
-
Activated partial thromboplastin time (APTT): 22.6 (21.7–31.6 s)
-
Prothrombin time (PT): 11.5 (9.6–12.8 s)
-
Urinalysis: normal
Questions
-
1.
What is your differential diagnosis ?
-
2.
What further workup is appropriate for this patient?
Answer
The differential diagnosis of isolated petechiae with or without bruising includes inherited hematologic conditions including hemophilia and Von Willebrand (VW) disease , acquired platelet disorders including idiopathic thrombocytopenic purpura, other coagulopathies including vitamin K deficiency and disseminated intravascular coagulation, vasculitic disorders including Henoch–Schönlein purpura (HSP ) , and oncologic disorders including leukemia. Finally, accidental injury is a consideration when the mechanism described fits the location and extent of injuries and the developmental capabilities of the child.
In this patient, no history of trauma was provided, and laboratory evaluation including normal WBC, platelet count, APTT, and PT excludes the majority of the medical conditions on the differential. HSP is unlikely in this patient as the bruising does not involve dependent areas and he has no palpable purpura, abdominal pain, or joint swelling. The location of the petechiae and ecchymoses , normal hematologic evaluation, and lack of caregiver explanation for these clinical findings raise the suspicion for child abuse.
Skin injuries are the most common manifestations of child abuse, and bruising and petechiae are the most common skin injuries in children. Victims of child physical abuse often sustain trauma to the face and neck. While bruising to the head and face can occur from accidental injuries in a mobile child, certain bruising locations should prompt suspicion for abuse, including injuries of the auricle. The mnemonic “TEN 4” has been suggested to identify bruises that are concerning for abuse; these include T = torso, E = ear, N = neck, and 4 = children less than or equal to 4 years of age and any bruising in infants under 4 months of age. Bruising of the anterior and posterior pinna is suggestive of pinching or pulling the ear, and bruising to the postauricular area and antihelix in particular are uncommon locations for accidental injuries in young children [1].
The American Academy of Pediatrics (AAP) has recommended a thorough evaluation for bleeding disorders in children who have bruising or bleeding as part of their manifestation of possible child physical abuse. This includes a complete family history, past medical history and review of systems to identify the possibility of a bleeding disorder. Without a clear injury history or witnessed trauma, children with bruising should undergo initial hematologic testing including PT, APTT, VWF antigen, VWF activity, Factor VIII and Factor IX levels and a complete blood count including platelet count [2].
Young children who are suspected victims of child physical abuse should undergo evaluation for occult injuries . This includes laboratory evaluation for occult abdominal trauma including aspartate aminotransferase (AST ) and alanine aminotransferase (ALT) , and radiographic evaluation for occult skeletal trauma, which often consists of a skeletal survey [3]. A skeletal survey is a systematically performed series of 21 radiographic images that encompasses the entire skeleton. Data has suggested that a skeletal survey should be obtained in all children less than 24 months of age with concerns of physical abuse, and should be strongly considered in children as old as 36 months of age [4]. In children older than 36 months, a skeletal survey may have utility for children with significant developmental delays and those who are nonverbal. Neuroimaging should be obtained to evaluate for intracranial injury in young infants, in children with significant head or facial trauma, and in those with an abnormal neurologic examination. As our patient sustained injuries to the ear and face and was lethargic on admission, computed tomography (CT) of the head is indicated.
Treatment
Treatment of victims of child physical abuse will vary depending on the extent of injuries. Therefore, meticulous evaluation for occult trauma is essential, and will guide necessary interventions and follow-up. Children with isolated cutaneous injuries including bruising and petechiae often require no specific treatment apart from analgesics as needed. When there is uncertainty regarding whether a skin finding is a bruise rather than a congenital skin lesion or other dermatologic condition, repeat examinations can be helpful to follow the natural course of the lesions. Additionally, children who received an initial skeletal survey to evaluate for occult skeletal trauma should receive a follow-up skeletal survey 10–14 days later to assess for any healing fractures that may not have been visible on the initial study [1].
Definitive treatment for these children is removal from the abusive perpetrator and/or environment. Physicians are mandated reporters, and therefore are legally obligated to report any concerns for child abuse to their local child protective services or law enforcement agency. Furthermore, any siblings of the patient should be evaluated with a thorough physical examination and any indicated laboratory or radiologic evaluation to assess for the possibility of physical abuse. Children who have suffered abuse or neglect warrant close monitoring by caregivers and primary care physicians for behavioral problems, physical symptoms, and signs of psychological stress [1]. Trauma-focused therapies have demonstrated utility in children who exhibit symptoms related to past traumatic events.
Case 11.2
History
An 18-month-old female was admitted for observation after sustaining a right parietal skull fracture and small underlying subdural hematoma . Her parents state this occurred while she was climbing on playground equipment and fell onto concrete. They state that her head impacted the ground and no other injuries were sustained. On admission she was overall well appearing with a normal neurologic examination. Her mother noted that she has had a “bad diaper rash ” for the past several days that has not been improving with use of a barrier cream. There is no history of diarrhea, urinary symptoms, or recent antibiotic use. Mother does note that they have been attempting to toilet train the patient recently, but she does continue to wear diapers during the day and night.
Physical Exam
On physical examination she is awake, alert, and mildly fussy. She has right-sided scalp edema without overlying lacerations or abrasions, and her neurologic examination is normal. She has ecchymoses to her mons pubis and petechiae on both labia majora with underlying ecchymoses (Fig. 11.2). Internal genitalia are normal including the labia minora and clitoral hood, and there is a crescentic hymen. There is no vaginal bleeding or discharge present. Perianal examination is normal.

On physical examination, ecchymoses involving the mons pubis, scattered petechiae, and faint ecchymoses involving the labia majora are seen
Laboratory Parameters
-
Hemoglobin: 11.9 (11.5–13.5 g/dL)
-
Platelet count: 450 (135–466 K/mcL)
-
Activated partial thromboplastin time (APTT): 21.9 (21.7–31.6 s)
-
Prothrombin time (PT): 10.2 (9.6–12.8 s)
-
Urinalysis: normal
Questions
-
1.
What diagnostic considerations are important in this patient?
-
2.
What further workup is appropriate?
Answer
The physical findings noted in this patient—ecchymoses and petechiae of the external genitalia—indicate trauma concerning for child abuse. Accidental anogenital injury is relatively uncommon, particularly in children who wear diapers. Dermatitis is the most common vulvar condition seen in young children, and the most common dermatological condition seen in diapered children. Although the manifestations of diaper dermatitis can be extensive, including erythema, ulcerations, scaling and papules, evidence of ecchymoses or petechiae should alert the clinician to the possibility of trauma. As with other causes of bruising and petechiae, a hematologic evaluation is warranted to assess for coagulopathy, vasculitis, or other medical conditions predisposing to bruising. There is no evidence of a bleeding diathesis in this patient given her normal platelet count and coagulation studies. The indication of abusive injury to this child’s external genitalia necessitates a complete evaluation for occult injury, including AST and ALT levels to assess for abdominal trauma, and a skeletal survey to assess for skeletal trauma. A more detailed history regarding the patient’s head injury and a complete social assessment is also warranted.
Children who are victims of physical abuse may sustain injury to the genital or anal areas through a variety of mechanisms including burns, impact injury, biting, or penetrating trauma. Many abusive acts are in response to a child behavior that is negatively perceived by caregivers, and toilet training is a common trigger for physical abuse. However, it is important to recognize that children may sustain similar or identical injuries following sexual abuse. Therefore, although it can be difficult to distinguish whether the primary motivation of an injury is sexual in nature, an evaluation for further evidence of sexual abuse should be pursued [5].
When a history cannot be obtained from the patient due to developmental stage or other factors, the evaluation of possible sexual abuse includes a thorough physical examination and testing for evidence of sexual contact. Genital and anal examinations in children with concerns for sexual abuse should be performed by providers with adequate training and equipment to examine the patient, photo-document relevant findings, and make appropriate referrals. Sexually transmitted infections (STIs ) occur infrequently following sexual abuse in prepubertal children. Therefore, the decision to test for STIs depends on a risk assessment for each individual child [6]. If evaluation for sexual abuse occurs in the acute setting, forensic evidence collection may also be indicated. As with any form of child maltreatment, physicians are mandated reporters and are legally obligated to report any suspicion of physical or sexual abuse to their local child protection services or law enforcement agency [7].
Treatment
Treatment of child abuse involves recognizing and anticipating the physical, emotional, and behavioral consequences that result from this trauma. Primary treatment beyond any necessary medical stabilization is removal of the child from the abusive perpetrator and/or environment. In cases of prepubertal child sexual abuse, testing for STIs may be appropriate if certain risk factors are present, including a history of genital or anal contact, perpetrator with known STI (s), or patient symptoms of an STI . When testing is performed, confirmatory testing of any positive results is often required in prepubertal children and in any case that involves the legal system. Prophylactic treatment for STIs in prepubertal children is generally not indicated except in significantly high-risk situations. Finally, children who have experienced child sexual abuse should be referred to a mental health professional with expertise in addressing childhood trauma [5, 7].
Case 11.3
History
A 4-year-old male with a history of asthma and mild atopic dermatitis is admitted for an acute asthma exacerbation. His mother reports that she “ran out of his asthma medications a while ago,” and she has not requested refills from his primary care provider. He has been in the ED five times over the last year for asthma exacerbations and has required hospitalization three times for asthma. His father smokes cigarettes in the home, and his mother notes that smoke exposure is a frequent trigger for his asthma. His mother reports that his eczema is generally well controlled with emollients, but she has noticed new lesions on his left arm, and is now requesting a topical corticosteroid medication. His mother states she noticed the lesions 2 days ago when she returned home from work. He was home with his father and 2-year-old sister during the day, and his father stated that he hadn’t noticed the lesions until the patient’s mother pointed them out. She states that the lesions were never pustular or vesicular, there is no history of any bleeding or drainage, and the only change to the lesions over the past 2 days is that some have started to crust. He is noted to be delayed on his immunizations, and has received only one dose of the varicella vaccine.
Physical Exam
On physical examination he is receiving nebulized albuterol and is awake and alert in moderate respiratory distress. He is noted to be thin, with diffuse xerosis and numerous areas of dirt and debris on the skin, in his hair, and under the fingernails and toenails. His clothing is noted to be dirty and worn. Eczematous patches are noted in his antecubital and popliteal fossae bilaterally. Along the lateral aspect of the mid portion of his left upper extremity, there are five grouped superficial ulcers (Fig. 11.3). Each lesion is circular with sharply defined borders and measures 5–8 mm in diameter. The lesions have a punched-out appearance and are each surrounded by a ring of erythema. He has poor dentition.

On physical examination, grouped, punched out circular superficial ulcers with surrounding erythema are noted involving the left arm
Laboratory Parameters
-
White blood cells: 7.1 (5.0–19.5 K/mcL)
-
Hemoglobin: 12.2 (11.5–13.5 g/dL)
-
Platelet count: 350 (135–466 K/mcL)
-
Bacterial culture (skin lesion): negative
-
Fungal culture (skin lesion): negative
Questions
-
1.
What is your differential diagnosis for this patient?
-
2.
What is the appropriate treatment?
Answer
The differential diagnosis for grouped round skin lesions consistent with erosions and/or superficial ulcers is broad. Possible etiologies include infectious conditions, excoriations associated with pruritic disorders such as atopic dermatitis or contact dermatitis, unique cultural practices, and inflicted injury. A careful history, physical examination, and laboratory analysis help to differentiate these conditions. Diagnostic considerations may include impetigo; bacterial or fungal pyoderma; viral exanthems, including varicella and coxsackievirus; and certain folk remedies or alternative healing practices such as moxibustion , which may result in lesions with a similar appearance to inflicted burns. This practice consists of placing ground herbs often in conjunction with acupuncture needles and heat on the patient’s skin, resulting in blistering and scarring at the site of impact. A careful history with specific questions regarding healing cultural practices will help uncover this diagnosis [8].
The lesions in this patient are consistent with inflicted cigarette burns . Accidental contact burns from a lit cigarette classically result in a single ill-defined oval or wedge-shaped lesion. They do not result in full-thickness skin injury due to the reflex withdrawal to pain of the affected body part. In contrast, inflicted cigarette burns have sharp round borders and usually appear in groups. Inflicted cigarette burns often produce a deep partial or full-thickness burn that is uniform in depth, and typically 5–10 mm in diameter depending on the size of the cigarette and the length of time it was applied to the skin. Lesions may blister, or may be dry and pale in appearance due to thermal coagulation of the involved tissue. These lesions heal gradually, often resulting in an atrophic scar with a hypopigmented center and hyperpigmented rim. Common locations for inflicted cigarette burns include the dorsum of hands and feet, face and limbs, although they can occur in any location.
Children with signs of physical abuse are also at risk for neglect, which includes physical neglect, emotional/psychological neglect, educational neglect, and medical neglect. Maltreatment by burning may be secondary to inflicted injury or supervisory neglect. Delayed presentation and lack of wound care prior to seeking medical attention are warning signs that a burn may be secondary to abuse or neglect. Burns resulting from abuse or neglect are also more likely to involve deeper tissue and require skin grafting [9]. Although this child’s injury is consistent with intentional burning with a cigarette, he also manifests signs concerning for both physical and medical neglect including poor hygiene and attire, and a failure to provide appropriate care for his asthma and routine health maintenance.
Treatment
Children with inflicted burn injuries are at risk for other abusive injuries. In reports in the literature, intentional cigarette burns are frequently accompanied by other injuries, including blunt force injuries, evidence of sexual abuse, and occult fractures [10]. Current recommendations are to evaluate children with inflicted burns who are less than 24 months of age with a skeletal survey to assess for occult skeletal trauma [11]. In this 4-year-old patient, a full cutaneous and musculoskeletal examination is warranted to evaluate for any sign of further injuries.
When the diagnosis is uncertain, repeat examinations over the course of several days can help distinguish the expected progressive resolution of inflicted cigarette burns from the evolution of infectious conditions. Children who are verbal and of a certain cognitive and emotional maturity may be able to engage in a forensic interview to discuss how the lesions occurred.
Treatment of thermal burns is often supportive, and may involve analgesics, moisturizers, and topical antibiotics such as silver sulfadiazine to prevent and treat infections. Definitive treatment of child abuse involves removal of the child from the abusive perpetrator and/or environment, and anticipating the physical, emotional, and behavioral consequences that may result from the experienced trauma.
Neglect has the potential to adversely affect a child’s psychosocial, cognitive, and emotional development, and has been shown to be a precursor for other forms of maltreatment, including physical abuse. Therefore, early detection of neglect has the potential to prevent further neglect as well as subsequent abuse. A multidisciplinary assessment is ideal in diagnosing neglect, and may include contact with the primary care provider, school, daycare setting, and other services that interact with the child. A social services assessment of the family including food insecurity, financial stressors, and living conditions in the home can significantly aid in the diagnosis of neglect. Just as in the diagnosis of neglect, treatment is most effective when done as a multidisciplinary effort, and involves addressing both the physical and psychosocial aspects of neglect. A treatment team may include the primary care physician, child behavioral specialists, social workers, home visitors, parent and child educators, and mental health professionals. While a report to child protective services is mandatory in cases of suspected neglect, a determination of removal from the home is made on an individual basis, and in some cases, services may be provided to the family while the child remains in the home. Appropriate reporting and service referral can help ameliorate the significant risks associated with maltreatment secondary to neglect .
Case 11.4
History
A 16-year-old girl with a history of anxiety is admitted with a several month history of a chronic, asymptomatic rash on her chest and a 3-week history of right axillary lymphadenitis. There is no history of fever or arthralgias. Prior outpatient evaluation of the rash was remarkable for methicillin-resistant Staphylococcus aureus (MRSA) on superficial bacterial culture; prior treatment with both topical mupirocin ointment and oral trimethoprim-sulfamethoxazole as prescribed by her primary care provider were of limited efficacy and the rash has persisted. She denies symptoms such as pain or pruritus, and denies picking or scratching. She is unable to provide a history of the eruption. She has a history of anxiety and her grandfather has been recently diagnosed with leukemia. Current medications include fluoxetine and clindamycin.
Physical Exam
She was well appearing and afebrile on examination. Involving the superior portion of the breasts, there are several scattered, discrete 5–10 mm erythematous crusted round erosions and a few superficial ulcers admixed with resolving erythematous slightly atrophic macules (Fig. 11.4). There is a 3 cm tender, non-fluctuant minimally erythematous subcutaneous nodule in the right axillae .

On physical examination, there are scattered erythematous crusted round erosions, superficial ulcers, and resolving erythematous slightly atrophic macules on the upper chest
Laboratory Parameters
-
WBC: 7.1 (4.5–13.5 K/mcL)
-
Erythrocyte sedimentation rate: 8 (<20 mm/h)
-
C-reactive protein: 0.3 (<1.0 mg/dL)
-
HSV PCR (skin lesion): negative
-
VSV PCR (skin lesion): negative
-
Bacterial culture (skin lesion): negative
-
Skin biopsy: ulceration of the epidermis with serosanguinous crust, mild mixed inflammation of the superficial dermis
Questions
-
1.
What is your differential diagnosis for these clinical findings?
-
2.
What diagnostic clues can facilitate arriving at the correct diagnosis?
Answer
Diagnostic considerations for localized cutaneous erosions and superficial ulcers may include infection (more commonly bacterial (e.g., Staphylococcal, Streptococcal ecthyma, or other presentation) or viral (e.g., herpes simplex virus, varicella zoster virus, or enterovirus), arthropod infestation (e.g., scabies, bedbugs), vasculitis, inflammatory dermatoses such as pityriasis lichenoides et varioliformis acuta and some presentations of collagen vascular disease, and autoimmune bullous disease (e.g., dermatitis herpetiformis). The differential diagnosis also includes a self-inflicted skin lesion (SISL ) , historically referred to as dermatitis artefacta. On the basis of the history of anxiety, inability of the patient to provide a concrete history for the cutaneous manifestations, clinical features, negative diagnostic testing, and skin biopsy supportive of induced trauma, a diagnosis of a factitious skin disorder was rendered.
SISLs in children can present a significant diagnostic dilemma, and they are often not considered in the differential diagnosis of a cutaneous eruption. The European Society for Dermatology and Psychiatry defines SISL as “any skin lesion actively and directly produced by the patient on his/her skin, mucosa or integument that is not better explained as a consequence of another physical or mental disorder” [12]. These clinical behaviors are the result of a maladaptive response to one or more internal psychological stressors. If the presentation involves the deliberate invocation of the cutaneous manifestations for secondary gain (e.g., avoidance of school or an abusive caregiver), and the behavior is denied, malingering is diagnosed; if there is no secondary gain but the behavior is denied, a factitious disorder is diagnosed. If the patient readily admits to inducing the skin lesions, a compulsive or impulsive skin picking/skin damaging syndrome is diagnosed. The presence of an associated mental health disorder such as depression or anxiety is common, and in adults, SISL appears more commonly in women. Examples of common SISL in children and adolescents include trichotillomania, acne excorièe, and factitial purpura [13, 14].
Clues to the diagnosis may include a vague or “hollow” history; skin lesions that are bizarre or oddly geometric; involvement of readily accessible areas such as the anterior extremities, face, chest, and upper back; lesions that do not conform in distribution and morphology to any known dermatologic disease or condition; and the appearance that the patient is indifferent to the cutaneous manifestations.
Evaluation may necessitate performing a skin biopsy or other diagnostic testing to exclude other diagnostic considerations and to convince the patient and caregivers of the correct diagnosis. The diagnosis is one of exclusion, although it is often suspected clinically.
Treatment
Perhaps the most critical component of treatment of self-induced skin lesions in children is the establishment of a trusting and therapeutic physician–patient–caregiver relationship [13]. Patients and caregivers need to feel supported in a nonjudgmental manner, which can be a challenge for the provider as many patients and caregivers are very resistant to the concept of a self-induced process and are determined to seek an alternative diagnosis. As such, it may take several encounters with the patient and caregiver for the provider to establish the degree of rapport needed to be able to introduce the idea of a SISL while minimizing the risk of alienating the patient and caregiver. Excluding a diagnosis of a primary skin disease or other primary disorder with cutaneous manifestations is also an important component of management.
Involving a behavioral health provider such a pediatric clinical psychologist early in the process can be helpful, though the initial referral may seek to address concerns such as coping or stress [13]. Cognitive behavioral therapy and other forms of psychotherapy are an important component of treatment. Psychopharmacologic intervention may be considered for patients with associated mental health comorbidities that cannot be adequately addressed with psychotherapy alone, and should be made with the assistance of a psychiatrist or other mental health provider with expertise in this area. Medical therapy consists predominantly of wound care, if appropriate, including management of any secondary infection.
The prognosis for SISL in children appears more favorable than that in adults, and younger children appear to have the best prognosis, although the course may be protracted over several years and characterized by chronicity and intermittent recurrences.
References
Christian CW, Committee on Child A, Neglect AAoP. The evaluation of suspected child physical abuse. Pediatrics. 2015;135(5):e1337–54.
Anderst JD, Carpenter SL, Abshire TC, Section on HO, Committee on Child A, Neglect of the American Academy of P. Evaluation for bleeding disorders in suspected child abuse. Pediatrics. 2013;131(4):e1314–22.
Harper NS, Feldman KW, Sugar NF, Anderst JD, Lindberg DM, Examining Siblings To Recognize Abuse I. Additional injuries in young infants with concern for abuse and apparently isolated bruises. J Pediatr. 2014;165(2):383–8 e1.
Lindberg DM, Berger RP, Reynolds MS, Alwan RM, Harper NS, Examining Siblings To Recognize Abuse I. Yield of skeletal survey by age in children referred to abuse specialists. J Pediatr. 2014;164(6):1268–73 e1.
Kellogg N, American Academy of Pediatrics Committee on Child A, Neglect. The evaluation of sexual abuse in children. Pediatrics. 2005;116(2):506–12.
Girardet RG, Lahoti S, Howard LA, Fajman NN, Sawyer MK, Driebe EM, et al. Epidemiology of sexually transmitted infections in suspected child victims of sexual assault. Pediatrics. 2009;124(1):79–86.
Jenny C, Crawford-Jakubiak JE, Committee on Child A, Neglect, American Academy of P. The evaluation of children in the primary care setting when sexual abuse is suspected. Pediatrics. 2013;132(2):e558–67.
Faller-Marquardt M, Pollak S, Schmidt U. Cigarette burns in forensic medicine. Forensic Sci Int. 2008;176(2–3):200–8.
Chester DL, Jose RM, Aldlyami E, King H, Moiemen NS. Non-accidental burns in children—are we neglecting neglect? Burns. 2006;32(2):222–8.
Kemp AM, Maguire SA, Lumb RC, Harris SM, Mann MK. Contact, cigarette and flame burns in physical abuse: a systematic review. Child Abuse Rev. 2014;23(1):35–47.
Degraw M, Hicks RA, Lindberg D, Using Liver Transaminases to Recognize Abuse Study I. Incidence of fractures among children with burns with concern regarding abuse. Pediatrics. 2010;125(2):e295–9.
Gieler U, Consoli SG, Tomas-Aragones L, Linder DM, Jemec GB, Poot F, et al. Self-inflicted lesions in dermatology: terminology and classification—a position paper from the European Society for Dermatology and Psychiatry (ESDaP). Acta Derm Venereol. 2013;93(1):4–12.
Shah KN, Fried RG. Factitial dermatoses in children. Curr Opin Pediatr. 2006;18(4):403–9.
Chiriac A, Brzezinski P, Pinteala T, Chiriac AE, Foia L. Common psychocutaneous disorders in children. Neuropsychiatr Dis Treat. 2015;11:333–7.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Simonton, K., Shah, K.N. (2016). Abuse and Factitious Disorders. In: Hogeling, M. (eds) Case-Based Inpatient Pediatric Dermatology. Springer, Cham. https://doi.org/10.1007/978-3-319-31569-0_11
Download citation
DOI: https://doi.org/10.1007/978-3-319-31569-0_11
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-31567-6
Online ISBN: 978-3-319-31569-0
eBook Packages: MedicineMedicine (R0)