
Abstract
Chronic iron overload corresponds to a variety of genetic and acquired diseases. Genetic iron overload encompasses HFE and non-HFE-related hemochromatoses. Acquired iron overload is mainly due to multiple transfusions and to dyserythropoiesis. The damaging effect of iron excess concerns numerous organs and can therefore lead to miscellaneous clinical features, related especially to the liver, heart, pancreas, and rheumatological complications. Those complications alter not only the quality of life but also life expectancy. The diagnostic approach has become essentially noninvasive. It rests – beside clinical examination – on serum iron parameters (especially ferritin and transferrin saturation), on iron MRI, and, whenever indicated, on genetic testing. The treatment, in hepcidin deficiency-related iron overload, remains based on venesection therapy but should resort in the future to hepcidin supplementation. Posttransfusional iron overload has greatly benefited from the design of oral iron chelators.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Iron overload
- Hemochromatosis
- Hepcidin
- Ferroportin
- Hemojuvelin
- Transferrin receptor2
- Aceruloplasminemia
- Transfusions
- Dyserythropoiesis
- Ferritin
- Genetic testing
- MRI
- Venesections
- Iron chelation
- Desferrioxamine
- Deferiprone
- Deferasirox
Iron overload encompasses a variety of hereditary and acquired diseases and is responsible for significant morbidity and mortality. Major advances in iron overload pathophysiology, diagnostic tools, and pharmacotherapy have permitted significant improvements in the diagnostic and therapeutic management of human chronic iron excess. Four clinical cases illustrate these advances.
Case 1: A Classical Form of Hereditary Hemochromatosis
A 45-year-old man presents with chronic fatigue and painful handshake. He is diffusely hyperpigmented and presents moderate and firm hepatomegaly, without clinical signs of liver dysfunction. Blood tests show ferritin 2350 μg/L (N<300 μg/L), transferrin saturation 100 % (N<45 %), ALT 70 IU/L (N<45 IU/L), AST 60 IU/L (N<40 IU/L), prothrombin test 100 % (N: 100 %), and HFE test homozygosity for the C282Y mutation (now named p.Cys282Tyr). The diagnosis of type 1 HFE-related hemochromatosis is made.
Question 1.
Considering this overall profile, how would you categorize the disease stage?
-
A.
Grade 0
-
B.
Grade 1
-
C.
Grade 2
-
D.
Grade 3
-
E.
Grade 4
Expert Opinion
The phenotypic expression of C282Y homozygosity can be classified in five grades of increasing severity (HAS 2005). Grade 0 is the absence of clinical or biochemical expression (normal transferrin saturation, normal serum ferritin). Grade 1 corresponds to the absence of clinical signs but to increased transferrin saturation (>45 %) with normal serum ferritin (N usually <300 μg/L in men and <200 μg/L in women). Grade 2 has no clinical signs but increased serum transferrin saturation and ferritin. Grade 3 corresponds to increased transferrin saturation and ferritin, together with clinical symptoms that alter quality of life (chronic fatigue, impotence, bone and joint symptoms such as osteoporosis and mostly arthritis touching different joints with a very suggestive second and third metacarpophalangeal location which is notably responsible for painful handshake, non-insulin-dependent diabetes, non- or mildly fibrotic liver disease, hyperpigmentation). Grade 4 corresponds to the full-blown disease, with life-threatening organ damage concerning the liver (cirrhosis, hepatocellular carcinoma), pancreas (insulin-dependent diabetes), and heart (cardiomyopathy).
Question 2.
What are, among the following investigations, those that should be performed in this patient?
-
A.
Glycemia and testosteronemia
-
B.
Serum hepcidin level
-
C.
Liver biopsy
-
D.
Hand x-rays
-
E.
Hepatic iron MRI
Expert Opinion (Brissot et al. 2011)
-
Glycemia must be checked, given the risk of diabetes. Testosteronemia is also required, together with asking for erectile dysfunction.
-
As to hepcidin (or better hepcidin/ferritin) determination, it is not routinely performed. Low values would favor the diagnosis but remain essentially of theoretical interest, by reflecting the underlying mechanism for iron overload. Indeed, hepcidin is the iron hormone (Nicolas et al. 2001). In HFE (or type1)-related hemochromatosis, it is low, leading to both increased duodenal absorption of iron and increased egress of splenic iron. This double mechanism (Ganz 2013) (Fig. 1) leads to chronic hypersideremia and increased transferrin saturation, which, in turn, generates non-transferrin-bound iron (NTBI) (Brissot et al. 2012). NTBI is very avidly taken up by the parenchymas (especially in the liver, pancreas, and heart), in contrast with transferrin-iron whose fate is essentially the bone marrow.
Fig. 1 
The two main mechanisms accounting for iron overload: (a) increased cellular entry; (b) decreased cellular egress
-
For the liver. Mild cytolysis, with transaminase levels usually <3 times the upper normal limits, is compatible with an iron overload origin. A key question concerns the liver biopsy indication. In so far as the patient cumulates the three symptoms, which individually would already justify a liver biopsy (namely, hepatomegaly, cytolysis, and ferritin>1000 μg/L) (Guyader et al. 1998), it is here fully indicated. This biopsy will inform on the quantity of iron excess (with possibility of a histological semiquantitative and/or biochemical quantitative evaluation) and on its cellular distribution (typically within the hepatocytes); it will also determine the degree of fibrosis, especially if there is cirrhosis (Deugnier and Turlin 2011).
-
For bone and joints: Hand x-rays will search for chondrocalcinosis and subchondral arthropathy. Bone scintigraphy is recommended due to the risk of osteoporosis (Guggenbuhl et al. 2011).
-
Hepatic “iron MRI” (magnetic resonance imaging for assessment of liver iron overload) (Gandon et al. 2004) has no real indication since a liver biopsy will be performed.
-
This work-up should also include electrocardiogram and echocardiography.

Question 3.
The patient had no diabetes and no hypotestosteronemia but had massive hepatocyte iron deposition with cirrhosis.
Indicate the appropriate therapeutic measures to be engaged:
-
A.
Iron-poor diet
-
B.
Venesections every week
-
C.
Venesections every month
-
D.
Iron chelation
-
E.
Liver ultrasound and serum AFP (alpha-fetoprotein) every year
Expert Opinion
-
Iron-poor diet is not required. However, the patient should of course avoid iron pills and vitamin C tablets (vitamin C increases iron absorption).
-
The recommended venesection schedule is a weekly one during the induction phase (= the phase aiming to eliminate iron excess) until the objective of serum ferritin of the order of 50 μg/L is reached. Afterward, during the maintenance phase (= the unlimited period during which iron overload reconstitution must be avoided), venesections will be performed every 1–3 months, with the objective of maintaining serum ferritin close to 50 μg/L.
-
Iron chelation has no indication as long as venesections are technically feasible.
-
Due to the presence of cirrhosis, liver ultrasound examination and serum AFP control must be performed every 6 months in order to detect the emergence of a hepatocellular carcinoma (Bruix et al. 2005).
Question 4.
The patient (= the proband) has two sisters, aged 42 and 40, and two children, aged 10 and 20. You start a family study. Among the following proposals, indicate the correct one:
-
A.
To check only iron blood parameters (transferrin saturation and ferritin) in all relatives
-
B.
To check only the C282Y mutation in all relatives
-
C.
To check the C282Y mutation and iron blood parameters in all relatives
-
D.
To check the C282Y mutation in both sisters and in the 20 years old child, without controlling iron blood parameters
-
E.
To check the C282 mutation in both sisters and in the 20 years old child, together with control of iron blood parameters
Expert Opinion (HAS 2005)
-
Searching for the C282Y mutation is essential in all individuals ≥18 years (with their written consent). Therefore, here, it has not to be checked in the 10 years old child. The information provided by this genetic study is critical: in the absence of C282Y mutation, there is no risk of hemochromatosis; C282Y heterozygosity does not expose to the risk of hemochromatosis (only risk of mutated gene transmission to the offspring); C282Y homozygotes (C282Y/C282Y) are at risk for developing the disease, but it should be noticed that it is not an obligatory evolution since only 30 % of men and 1 % of women may develop the clinically expressed disease.
-
Assessing iron blood parameters is recommended in all genetically tested relatives, since they permit, in those family members who happen to be C282Y homozygotes, to be, at the same time, informed on their degree of biochemical expression.
-
Checking transferrin saturation and ferritin to the age of 15 (after puberty) can be proposed.
Case 2: A Case of Juvenile Hemochromatosis
A 23-year-old sporty woman, whose past history was represented by secondary amenorrhea since the age of 16, experienced increasing dyspnea with palpitations, painful hepatomegaly, and leg edema. Clinical examination, joined to electrocardiogram and echocardiography, rapidly concluded to global cardiac failure due to severe dilated myocardiopathy with an ejection fraction of 15 %. She was hyperpigmented, with plasma transferrin saturation of 100 % and serum ferritin of 7000 μg/L (N<200 μg/L). The diagnosis of juvenile hemochromatosis was therefore highly suspected.
Question 5.
Among the following items, indicate those who are highly suggestive of juvenile hemochromatosis:
-
A.
Age
-
B.
Endocrine background
-
C.
Cardiac picture
-
D.
The level of transferrin saturation
-
E.
The level of serum ferritin
Expert Opinion (Brissot et al. 2011; Camaschella and Poggiali 2011)
-
Juvenile hemochromatosis should be evoked whenever major iron overload is suspected in a young person, aged less than 30.
-
Clinical expression is dominated by cardiac and endocrine symptoms.
-
A highly elevated transferrin saturation is not, by itself, indicative of juvenile hemochromatosis since it can be present at an early stage in type 1 hemochromatosis.
-
The very high level of serum ferritin also favors the diagnosis.
Question 6.
Among the following investigations, indicate those that, today , would be preferred to confirm the diagnosis:
-
A.
Cardiac biopsy
-
B.
Liver biopsy
-
C.
Liver MRI
-
D.
Cardiac MRI
-
E.
Genetic testing
Expert Opinion
-
Although endomyocardial biopsy is a key procedure to prove cardiac iron overload, it would be replaced today by noninvasive cardiac MRI.
-
For the same reason (especially considering cardiac failure), liver biopsy would be replaced, for iron overload assessment, by hepatic MRI.
-
Genetic testing provides the definitive diagnostic proof. In this patient, the C282Y mutation was absent, and compound heterozygosity for hemojuvelin gene mutations was present. Three main entities of juvenile hemochromatosis have been identified: mostly juvenile hemochromatosis type 2A related to HFE2 (or HJV) mutations (Papanikolaou et al. 2004) and juvenile hemochromatosis type 2B related to hepcidin gene (HAMP) (Roetto et al. 2003) mutations, but also type 3 hemochromatosis related to transferrin receptor 2 (TFR2) mutations (this latter disease can also affect adults) (Camaschella et al. 2000).
Question 7.
Indicate the appropriate therapeutic management:
-
A.
Symptomatic treatment of cardiac failure
-
B.
No venesections
-
C.
Weekly venesections alone
-
D.
Weekly venesections + iron chelator
-
E.
Vitamin C to be avoided
Expert Opinion
-
It is critical to adopt a powerful strategy for decreasing the iron burden. Weekly venesections may, therefore, be associated to chelation therapy.
-
Vitamin C must be avoided, not only because it facilitates iron absorption but, mostly, because it can promote the release of stored iron into the blood, which may worsen the cardiac status.
Case 3: A Case of Hereditary Aceruloplasminemia
A 63-year-old woman was explored for chronic microcytic anemia. Hemoglobin was 10.7 g/L. Serum iron and transferrin saturation were low (5.6 μmol/L, N 12–22 and 10 % N, 20–45 %, respectively). Reticulocyte, leukocyte, and platelet counts were normal. She was first investigated for possible gynecological or digestive blood losses, but all explorations were negative. In fact, serum ferritin was found markedly elevated, 1450 μg/L (N<200 μg/L), which led to the modification of etiological orientations.
Question 8.
Indicate, among the following situations, the one(s) that can lead to hyperferritinemia without increased transferrin saturation:
-
A.
Metabolic syndrome
-
B.
Inflammatory syndrome
-
C.
Ferroportin disease
-
D.
Ferritin-cataract syndrome
-
E.
Hereditary aceruloplasminemia
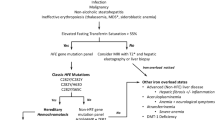
Expert Opinion (Fig. 2)

Diagnostic approach of hyperferritinemia
-
Dysmetabolic hyperferritinemia corresponds today to the most frequent cause of hyperferritinemia, still too often misdiagnosed as hemochromatosis. Its diagnosis rests on (i) clinical background associating more or less overweight, increased blood pressure, non-insulin-dependent diabetes, hyperlipidemia, and hyperuricemia; (ii) increased serum ferritin, usually less than 1000 μg/L; (iii) normal transferrin saturation (<45 %); and (iv) hepatic iron overload (as assessed by MRI) either absent or only moderate (corresponding then to the dysmetabolic iron overload syndrome (Mendler et al. 1999)).
-
The inflammatory syndrome involves (i) decreased serum iron due to hyperhepcidinemia which sequesters iron within the macrophages and impairs cellular iron release into the plasma (Nemeth et al. 2004) and (ii) increased serum ferritin because it is an acute phase-reactant protein.
-
The ferroportin disease (FD) (Montosi et al. 2001; Njajou et al. 2001), also named hemochromatosis type 4, is, in its usual form (type A), expressed by elevated serum ferritin (at levels often above 1000 μg/L) contrasting with normal or low transferrin saturation. The underlying mechanism is the impairment of cellular iron export due to mutations of the ferroportin gene (SLC40A1) affecting the export properties of ferroportin. Iron overload, in contrast to types 1, 2, and 3 hemochromatoses which involve excessive cellular iron entry due to hepcidin deficiency, is related to intracellular iron retention. Since ferroportin activity is especially important in macrophages, iron overload targets essentially the spleen. FD provides little visceral damage, probably due to the fact that, in the absence of increased transferrin saturation, there is neither circulating non-transferrin-bound iron (NTBI), and therefore no propensity to hepatocyte iron excess, nor formation of labile plasma iron (LPI), and therefore no potentially toxic form of blood iron (Brissot et al. 2012). Treatment still consists in venesections, but, due to the iron recycling difficulties which may lead to anemia, the iron depletion schedule should be less drastic than in hepcidin-deficient-related hemochromatosis. It should be noticed that another form of ferroportin disease, named type B, exists, characterized by a hepcidin resistance status which provides a phenotype similar to hepcidin-deficient hemochromatosis (Drakesmith et al. 2005).
-
The ferritin-cataract syndrome is due to mutations of the l-ferritin gene, located in the IRE loop of l-ferritin mRNA (Yin et al. 2014). Serum ferritin is high, transferrin saturation is not elevated, and there is neither hepatic nor splenic iron excess. It is a dominant disease. Some mutations (located in exon1) are only expressed by hyperferritinemia (no cataract) (Kannengiesser et al. 2009).
-
Hereditary aceruloplasminemia (HA) is also characterized by a marked contrast between strong elevation of serum ferritin concentration and low transferrin saturation. Like in ferroportin disease, tissue iron overload is due to cellular iron release impairment, probably related to the defect of ceruloplasmin oxidase activity.
Question 9.
What are, among the following features, the one(s) that should be looked for in order to support the diagnosis of HA:
-
A.
Diabetes
-
B.
Neurological symptoms
-
C.
Ophtalmological symptoms
-
D.
Prevailing hepatic iron overload
-
E.
Prevailing splenic iron overload
Expert Opinion (Kono 2013)
-
Diabetes is related to pancreatic iron deposition.
-
Neurological expression is a key feature of the disease. HA is the sole form of adult genetic iron overload in which excessive iron deposition occurs in the brain. Movement disorders can be present as well as psychiatric symptoms.
-
Retinal degeneration is one of the consequences of the disease.
-
Iron overload seems to target preferentially the hepatocytes, sparing the spleen. The precise mechanism accounting for this organ iron distribution, which mimics that observed in hepcidin-deficient-related hemochromatoses, remains to be elucidated.
Question 10.
Indicate, among the following items, the one(s) who look(s) appropriate:
-
A.
To perform abdominal and brain iron MRI
-
B.
To determine serum ceruloplasmin concentration
-
C.
To search for mutations in the ceruloplasmin gene
-
D.
To start venesection therapy
-
E.
To start chelation therapy
Expert Opinion
-
Iron MRI will show hepatic iron excess, no splenic iron overload, and brain iron overload, especially in the basal ganglia.
-
Very low, and often undetectable, ceruloplasmin concentration is a key phenotypic diagnostic feature (and, therefore, should not only suggest Wilson disease).
-
Finding mutations of the ceruloplasmin gene (CP) will provide the definitive proof of the disease.
-
Due to anemia, venesections are contraindicated in HA. The only option is chelation therapy. Desferrioxamine is efficient on hepatic iron overload but does not seem active on brain iron (Loreal et al. 2002). Deferasirox is an oral iron chelator, taken once daily, globally well tolerated (side effects concern mainly renal function, gastrointestinal discomfort, and rashes). In HA, it is effective in mobilizing hepatic iron (Finkenstedt et al. 2010; Suzuki et al. 2013), but provided contrasting results for brain iron (Finkenstedt et al. 2010; Suzuki et al. 2013).
Case 4: A Case of Thalassemia Intermedia
The medical history of this 31 years old black woman is the following: 9 years old, diagnosis of β-thalassemia intermedia; 10–21 years old, transfused every 4 weeks; 15 years old, splenectomy; 21–31 years old, desferrioxamine (2 g/day, 5 days a week; stopped 2 years, with monthly transfusions, during pregnancies). Her present checkup shows Hb 9 g/dL, MCV 80 μ3, leucocytes 14G/L, platelets 610G/L, serum iron 45 μmoL/L (N<22 μmol/L), transferrin saturation 95 % (N<45 %), serum ferritin 1500 μg/L (N<200 μg/L), and iron MRI, marked hepatic iron overload.
Question 11.
Indicate the correct proposal(s):
-
A.
Iron overload is, at least partly, of transfusional origin.
-
B.
Iron overload is, at least partly, due to dyserythropoiesis.
-
C.
Before relating serum ferritin increase to body iron overload, some confounding factors must be ruled out.
-
D.
In thalassemia, the degree of serum ferritin increase depends on iron cellular distribution.
-
E.
Abdominal iron MRI can provide information on the pathophysiology of iron overload.
Expert Opinion
-
Each transfusion provides 200–250 mg of iron which are stored in the macrophages (therefore mainly in the spleen) (Porter and Garbowski 2014). The human body having only very limited capacities for regulating iron excretion, tissue iron excess develops rapidly (after a few transfusions) and is globally maintained over time.
-
Dyserythropoiesis is another important factor contributing to iron overload. It may explain iron excess in thalassemia in the absence of (or before) any transfusion. Dyserythropoiesis leads to an increased production of the medullary hormone erythroferrone, which, in turn, decreases hepatic production of hepcidin (Kautz et al. 2014). Therefore, the iron overload phenotype related to dyserythropoiesis is close to that of hepcidin-deficient-related hemochromatosis.
-
The interpretation of elevated serum ferritin should always consider the possibility of confounding factors which can elevate ferritinemia independently of cellular iron excess. This is the case for the dysmetabolic syndrome, inflammation (see Case 3, Question 1), alcoholism, and cytolysis.
-
The interpretation of elevated serum ferritin should also consider iron organ distribution. It has been shown that, for equivalent amounts of stored iron, the corresponding serum ferritin levels are, in macrophagic (posttransfusional) iron deposition, approximately twice those found in parenchymal (dyserythropoiesis-related) iron excess (Taher et al. 2008).
-
The interest of abdominal iron MRI goes beyond the mere assertion and quantification of liver iron excess (St Pierre et al. 2005; Wood 2011). Indeed, when the spleen is still present, it is important to assess by IRM its iron content. Two types of liver-spleen imaging profiles can then be identified: (i) non-iron overloaded spleen + iron overloaded liver, corresponding to the usual features of dyserythropoiesis overload, as typically seen in non-transfusion-dependent thalassemia (NTDT); and (ii) iron overloaded spleen + iron overloaded liver, corresponding to the usual profile of thalassemia major (or transfusion-dependent thalassemia – TDT), where iron overload is due to both dyserythropoiesis and transfusions.
Question 12.
Indicate, among the following diagnostic and therapeutic proposals, the one(s) that is (are) appropriate:
-
A.
To check cardiac status
-
B.
To check liver status
-
C.
To check bone status
-
D.
To start again desferrioxamine
-
E.
To start oral chelation
Expert Opinion
-
It is important to assess cardiac status. Besides clinical examination, electrocardiogram, and echocardiogram for evaluating cardiac function, cardiac MRI is essential for assessing iron load (Wood and Noetzli 2010). If excessive cardiac iron is expected in case of massive hepatic iron overload, it may still be so in a chelated patient despite moderate residual hepatic iron overload, because kinetics of iron removal is lower in the heart than in the liver.
-
The liver and biliary tract should also be explored. For the liver, several harmful factors may cumulate such as iron overload, C and B viral hepatitis (considering the transfusion history), and, more rarely, portal or hepatic vein thrombosis related to the hypercoagulability status. The global consequence may be the development of hepatic fibrosis with the risks of cirrhosis and hepatocellular carcinoma. The latter two complications can now be observed since life expectancy of thalassemia has markedly improved due to the chelation therapy advances. As to the biliary tract, ultrasound examination is recommended since 30–60 % of patients develop gallbladder lithiasis, with choledocolithiasis in approximately 20 %.
-
Osteoporosis is a common feature in thalassemia and should be diagnosed, especially by osteodensitometry.
-
Desferrioxamine, despite its powerful chelating properties, is not orally absorbed and has a very short half-life, obliging to use a parenteral (subcutaneous) administration route, 12 h a day and 5 days a week, which represents an important constraint especially for children. This is why it has been replaced by oral chelation, usually resorting now more to deferasirox than to deferiprone (due to the need to be taken three times a day and mostly to the exceptional, but unpredictable, occurrence of agranulocytosis which requires a weekly control of blood cell count) (Deugnier et al. 2011; Hoffbrand et al. 2012; Cassinerio et al. 2015). Deferiprone, however, is efficient in case of severe cardiac iron overload. Whenever, after dose escalation of a single chelator, efficacy remains insufficient, it should be considered to switch to the other oral chelator, to combine the oral chelator to desferrioxamine (Aydinok et al. 2015), or even to combine the two oral chelators (Totadri et al. 2015).
Key Points
-
A thorough clinical examination should remain a prerequisite of iron overload management.
-
C282Y/C282Y hemochromatosis is, by far, the most frequent disease in Caucasians.
-
Non-HFE-related hemochromatoses are rare diseases but not confined to Caucasians.
-
In thalassemia, iron overload is due not only to transfusions but also to dyserythropoiesis.
-
The diagnostic approach of iron overload has become a noninvasive one, based – besides clinical data – on serum ferritin and transferrin saturation concentrations, on hepatic and splenic MRI data, and on genetic testing whenever indicated.
-
Low plasma serum iron and transferrin concentration levels can be observed despite major tissue iron overload in some forms of non-HFE-related genetic iron overload (ferroportin disease and hereditary aceruloplasminemia).
-
The therapeutic approach of iron overload rests mainly on venesections in hepcidin-deficient-related hemochromatosis.
-
The therapeutic future of hepcidin-deficient-related hemochromatoses is hepcidin supplementation.
Answers
-
Question 1. E
-
Question 2. A, C, D
-
Question 3. B, E
-
Question 4. E
-
Question 5. A, B, C, E
-
Question 6. C, D, E
-
Question 7. A, D, E
-
Question 8. A, B, C, D, E
-
Question 9. A, B, C, D
-
Question 10. A, B, C, E
-
Question 11. A, B, C, D, E
-
Question 12. A, B, C, E
References
Aydinok Y, Kattamis A, Cappellini MD, El-Beshlawy A, Origa R, Elalfy M, Kilinc Y, Perrotta S, Karakas Z, Viprakasit V, et al. Effects of deferasirox-deferoxamine on myocardial and liver iron in patients with severe transfusional iron overload. Blood. 2015;125:3868-77.
Brissot P, Bardou-Jacquet E, Jouanolle AM, Loreal O. Iron disorders of genetic origin: a changing world. Trends Mol Med. 2011;17:707–13.
Brissot P, Ropert M, Le Lan C, Loreal O. Non-transferrin bound iron: a key role in iron overload and iron toxicity. Biochim Biophys Acta. 2012;1820:403–10.
Bruix J, Sherman M, Practice Guidelines Committee AAftSoLD. Management of hepatocellular carcinoma. Hepatology. 2005;42:1208–36.
Camaschella C, Poggiali E. Inherited disorders of iron metabolism. Curr Opin Pediatr. 2011;23:14–20.
Camaschella C, Roetto A, Cali A, De Gobbi M, Garozzo G, Carella M, Majorano N, Totaro A, Gasparini P. The gene TFR2 is mutated in a new type of haemochromatosis mapping to 7q22. Nat Genet. 2000;25:14–5.
Cassinerio E, Roghi A, Orofino N, Pedrotti P, Zanaboni L, Poggiali E, Giuditta M, Consonni D, Cappellini MD. A 5-year follow-up in deferasirox treatment: improvement of cardiac and hepatic iron overload and amelioration in cardiac function in thalassemia major patients. Ann Hematol. 2015;94:939–45.
Deugnier Y, Turlin B. Pathology of hepatic iron overload. Semin Liver Dis. 2011;31:260–71.
Deugnier Y, Turlin B, Ropert M, Cappellini MD, Porter JB, Giannone V, Zhang Y, Griffel L, Brissot P. Improvement in liver pathology of patients with beta-thalassemia treated with deferasirox for at least 3 years. Gastroenterology. 2011;141:1202–11. 1211 e1201-1203.
Drakesmith H, Schimanski LM, Ormerod E, Merryweather-Clarke AT, Viprakasit V, Edwards JP, Sweetland E, Bastin JM, Cowley D, Chinthammitr Y, et al. Resistance to hepcidin is conferred by hemochromatosis-associated mutations of ferroportin. Blood. 2005;106:1092–7.
Finkenstedt A, Wolf E, Hofner E, Gasser BI, Bosch S, Bakry R, Creus M, Kremser C, Schocke M, Theurl M, et al. Hepatic but not brain iron is rapidly chelated by deferasirox in aceruloplasminemia due to a novel gene mutation. J Hepatol. 2010;53:1101–7.
Gandon Y, Olivie D, Guyader D, Aube C, Oberti F, Sebille V, Deugnier Y. Non-invasive assessment of hepatic iron stores by MRI. Lancet. 2004;363:357–62.
Ganz T. Systemic iron homeostasis. Physiol Rev. 2013;93:1721–41.
Guggenbuhl P, Brissot P, Loreal O. Haemochromatosis: the bone and the joint. Best Pract Res Clin Rheumatol. 2011;25:649–64.
Guyader D, Jacquelinet C, Moirand R, Turlin B, Mendler MH, Chaperon J, David V, Brissot P, Adams P, Deugnier Y. Noninvasive prediction of fibrosis in C282Y homozygous hemochromatosis. Gastroenterology. 1998;115:929–36.
HAS. French recommendations for management of HFE hemochromatosis. 2005. Haute Autorité de Santé www.has-sante.fr.
Hoffbrand AV, Taher A, Cappellini MD. How I treat transfusional iron overload. Blood. 2012;120:3657–69.
Kannengiesser C, Jouanolle AM, Hetet G, Mosser A, Muzeau F, Henry D, Bardou-Jacquet E, Mornet M, Brissot P, Deugnier Y, et al. A new missense mutation in the L ferritin coding sequence associated with elevated levels of glycosylated ferritin in serum and absence of iron overload. Haematologica. 2009;94:335–9.
Kautz L, Jung G, Valore EV, Rivella S, Nemeth E, Ganz T. Identification of erythroferrone as an erythroid regulator of iron metabolism. Nat Genet. 2014;46:678–84.
Kono S. Aceruloplasminemia: an update. Int Rev Neurobiol. 2013;110:125–51.
Loreal O, Turlin B, Pigeon C, Moisan A, Ropert M, Morice P, Gandon Y, Jouanolle AM, Verin M, Hider RC, et al. Aceruloplasminemia: new clinical, pathophysiological and therapeutic insights. J Hepatol. 2002;36:851–6.
Mendler MH, Turlin B, Moirand R, Jouanolle AM, Sapey T, Guyader D, Le Gall JY, Brissot P, David V, Deugnier Y. Insulin resistance-associated hepatic iron overload. Gastroenterology. 1999;117:1155–63.
Montosi G, Donovan A, Totaro A, Garuti C, Pignatti E, Cassanelli S, Trenor CC, Gasparini P, Andrews NC, Pietrangelo A. Autosomal-dominant hemochromatosis is associated with a mutation in the ferroportin (SLC11A3) gene. J Clin Invest. 2001;108:619–23.
Nemeth E, Rivera S, Gabayan V, Keller C, Taudorf S, Pedersen BK, Ganz T. IL-6 mediates hypoferremia of inflammation by inducing the synthesis of the iron regulatory hormone hepcidin. J Clin Invest. 2004;113:1271–6.
Nicolas G, Bennoun M, Devaux I, Beaumont C, Grandchamp B, Kahn A, Vaulont S. Lack of hepcidin gene expression and severe tissue iron overload in upstream stimulatory factor 2 (USF2) knockout mice. Proc Natl Acad Sci U S A. 2001;98:8780–5.
Njajou OT, Vaessen N, Joosse M, Berghuis B, van Dongen JW, Breuning MH, Snijders PJ, Rutten WP, Sandkuijl LA, Oostra BA, et al. A mutation in SLC11A3 is associated with autosomal dominant hemochromatosis. Nat Genet. 2001;28:213–4.
Papanikolaou G, Samuels ME, Ludwig EH, MacDonald ML, Franchini PL, Dube MP, Andres L, MacFarlane J, Sakellaropoulos N, Politou M, et al. Mutations in HFE2 cause iron overload in chromosome 1q-linked juvenile hemochromatosis. Nat Genet. 2004;36:77–82.
Porter JB, Garbowski M. The pathophysiology of transfusional iron overload. Hematol Oncol Clin North Am. 2014;28:683–701, vi.
Roetto A, Papanikolaou G, Politou M, Alberti F, Girelli D, Christakis J, Loukopoulos D, Camaschella C. Mutant antimicrobial peptide hepcidin is associated with severe juvenile hemochromatosis. Nat Genet. 2003;33:21–2.
St Pierre TG, Clark PR, Chua-anusorn W, Fleming AJ, Jeffrey GP, Olynyk JK, Pootrakul P, Robins E, Lindeman R. Noninvasive measurement and imaging of liver iron concentrations using proton magnetic resonance. Blood. 2005;105:855–61.
Suzuki Y, Yoshida K, Aburakawa Y, Kuroda K, Kimura T, Terada T, Kono S, Miyajima H, Yahara O. Effectiveness of oral iron chelator treatment with deferasirox in an aceruloplasminemia patient with a novel ceruloplasmin gene mutation. Intern Med. 2013;52:1527–30.
Taher A, El Rassi F, Isma’eel H, Koussa S, Inati A, Cappellini MD. Correlation of liver iron concentration determined by R2 magnetic resonance imaging with serum ferritin in patients with thalassemia intermedia. Haematologica. 2008;93:1584–6.
Totadri S, Bansal D, Bhatia P, Attri SV, Trehan A, Marwaha RK. The deferiprone and deferasirox combination is efficacious in iron overloaded patients with beta-thalassemia major: a prospective, single center, open-label study. Pediatr Blood Cancer. 2015;62:1592–6.
Wood JC. Impact of iron assessment by MRI. Hematol Educ Program Am Soc Hematol Am Soc Hematol Educ Program. 2011;2011:443–50.
Wood JC, Noetzli L. Cardiovascular MRI in thalassemia major. Ann N Y Acad Sci. 2010;1202:173–9.
Yin D, Kulhalli V, Walker AP. Raised serum ferritin concentration in hereditary hyperferritinemia cataract syndrome is not a marker for iron overload. Hepatology. 2014;59:1204–6.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Brissot, P. (2016). Iron Overload: Diagnosis, Complications, and Management. In: Abutalib, S., Connors, J., Ragni, M. (eds) Nonmalignant Hematology. Springer, Cham. https://doi.org/10.1007/978-3-319-30352-9_11
Download citation
DOI: https://doi.org/10.1007/978-3-319-30352-9_11
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-30350-5
Online ISBN: 978-3-319-30352-9
eBook Packages: MedicineMedicine (R0)