
Abstract
Anemia is one of the most common hematologic findings in children and adults. It is a condition that represents the end result of a diverse array of different inherited or acquired pathophysiologic processes. A thoughtful diagnostic approach to anemia can expediently lead to an understanding of its cause and avoids unnecessary laboratory testing. Across the age spectrum, iron deficiency is the most common nutritional cause of anemia, although its etiology tends to differ in children and adults. Other causes of anemia are quite diverse.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Case 1. Evaluation of Anemia
An 88-year-old man is referred for further evaluation of anemia. He has generally been in good health, and his active medical issues only include mild hypertension, which has been well controlled on a diuretic. Review of systems was unremarkable for fatigue, dyspnea, melena, or bright red blood per rectum. He was noted at the time of routine physical examination to have heme negative stool and on complete blood count was found to have a hemoglobin level of 13.0 g/dL, MCV 88 fL, RDW 14.0 %.
Question 1.
The finding of a hemoglobin of 13.0 g/dL in an 88-year-old man is:
-
A.
Potentially within the age appropriate normal range
-
B.
Clearly abnormal and warrants extensive further diagnostic evaluation, including endoscopy
-
C.
Clearly abnormal and warrants further laboratory diagnostic studies
-
D.
Clearly abnormal, but does not warrant further diagnostic evaluation because of patient age
Hemoglobin values change dramatically in the 2 months following birth, dropping from 18.5 ± 4 g/dL (mean ± 2 S.D.) the day after birth to 11.5 ± 2.5 g/dL at 2 months of age (Christensen et al. 2009). The MCV during that time also decreases from a 108 ± 10 to 96 ± 19 fL. The values in male and female infants are similar. Subsequently, over the course of childhood and adolescence, the values gradually rise toward adult levels, diverging in the two sexes due to the effect of androgens in males. In adults 18–49 years old, the normal hemoglobin is 14.0 ± 2 g/dL in females and 15.5 ± 2 g/dL in males. The hemoglobin values provided here and in Table 1 below are approximate, and the normal ranges vary depending upon the individual laboratory. Similar hemoglobin values are found in adults up to about age 70. However, over the next two decades of life, the normal range for females drops by about 0.2 g/dL, whereas for males it drops by more than 1 g/dL due to the drop off in androgen production (Nilsson-Ehle et al. 2000).
The key take away point here is that an individual’s age is relevant for making a diagnosis of anemia, as defined by a hemoglobin value below the normal range (usually two standard deviations below the mean). In particular, anemia should not be attributed to aging in women over 70 years of age, whereas a hemoglobin value modestly below the adult normal range may be observed in men over age 70.
Question 2.
A reticulocyte count for the 88-year-old man with the hemoglobin of 13.0 g/dL and hematocrit of 40 % is obtained and is found to be 1.7 %. The reticulocyte index is:
-
A.
0.8 %
-
B.
1.3 %
-
C.
1.5 %
-
D.
1.7 %
The reticulocyte count provides a relatively inexpensive way of narrowing the differential diagnosis of anemia that is present in an individual (Piva et al. 2015). It is appropriately elevated in response to blood loss or in various causes of hemolytic anemia and is low in various causes of hypoproliferative anemia or maturation abnormalities (Table 2). It can also be used to help monitor the response of either category of anemia to therapy. Understanding how to interpret the reticulocyte count that is reported by the laboratory is important.
Under normal circumstances, the approximately 1 % of red blood cells newly released each day from the bone marrow contain residual RNA that is degraded over the course of 24 h, and they are also slightly larger than the cohort of more mature cells. These features define the reticulocyte. When severe hemolytic anemia is present, a younger cohort of erythrocytes is released into the circulation, and these “shift” reticulocytes may persist for 2–3 days. On conventional Wright stained smears, reticulocytes appear as slightly larger bluish-red cells that have decreased central pallor. They can be enumerated manually by supravital staining with new methylene blue or by automated methods when stained with ethidium bromide. The reticulocyte count obtained by manual methods is reported as a percentage of total red cells; for automated methods, an absolute count can be obtained, although it is often converted into percentage. Whenever reported as a percentage when anemia is present, the reticulocyte count must be corrected for the degree of anemia using the formula:
The normal hematocrit used should be appropriate for the patient’s age and gender. An additional correction is sometimes made when severe hemolysis is present to correct for shift reticulocytes. Application of such correction factors for maturation produces the reticulocyte index. Although more complex formulas exist, if hemolysis is present and the hematocrit is about half normal, the corrected reticulocyte count should be halved. For example, a female patient with sickle cell anemia may have a hematocrit of 20 % and a reticulocyte count of 8 %. Following correction and adjustment for maturation, the reticulocyte index is 2 %, which is still an appropriate response. The need for correction for hematocrit is avoided when the absolute reticulocyte count is used in calculating the reticulocyte index.
Modern instruments for performing the complete blood count are also capable of providing a wealth of information regarding the hemoglobin content and size of the red cell (Thom 1990). In addition to the hemoglobin level and hematocrit, parameters commonly measured or calculated by most instruments include the mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC), and the red cell distribution width (RDW). Of these values, the MCV is most informative for the evaluation of anemia, followed by the RDW. Although the other red cell parameters (MCH, MCHC) may be of utility in certain special circumstances, they are not particularly helpful in identifying the cause of most types of anemia.
In contrast, MCV values facilitate the rapid categorization of anemia and are particularly helpful at the extremes: values less than 70 fL are generally indicative of moderate to severe iron deficiency or a thalassemia syndrome, and values greater than 110 fL are generally associated with folate or vitamin B12 deficiency, drug effects, or myelodysplastic syndromes. Table 3 illustrates the utility of the MCV in categorizing different causes of anemia. Whether the RDW adds to this categorization is debated by some clinicians. However, an elevated RDW does help differentiate certain conditions such as ß-thalassemia minor (RDW normal) from iron deficiency (RDW elevated) and aplastic anemia (RDW normal) from immune hemolytic anemia (RDW elevated). Further insight can be obtained by combining use of the reticulocyte count, MCV, and RDW to narrow the range of diagnostic possibilities.
Question 3.
One schistocyte per high-power field seen on this 88-year-old man’s smear indicates:
-
A.
Myelophthisis is likely to be present.
-
B.
Vitamin B12 deficiency may be present.
-
C.
Atypical hemolytic uremic syndrome may be present.
-
D.
A potentially normal finding.
The peripheral blood smear is an invaluable tool in the evaluation of anemia (Bain 2005). Information on red blood cell morphology can be obtained in the context of the number and morphology of other cell lineages. Morphology may reveal such findings as parasites (e.g., babesia or malaria) or may provide insight into organ function (Table 4). Despite the availability of many more sophisticated laboratory tests, the differential diagnosis can often be narrowed significantly by thoughtful review of a well-prepared and properly stained peripheral blood smear, and in some cases, specific diagnosis can be accomplished. Although there are many ways to approach the review of the peripheral blood smear, use of a systematic approach may be helpful:
-
1.
Determine if the smear is properly prepared and stained and choose an area for examination. Under medium to high power using the 40× or 100× objective, granules should normally be visible in neutrophils and platelets, and an area in which the individual red blood cells are separated by about 0.5–1 cell diameter should be used for further examination.
-
2.
Examine the other cell lines present before moving on to the erythrocytes. Do the neutrophils have normal morphology, or are they hyperlobulated indicating a megaloblastic process, or are toxic granulations present suggesting an infectious one? Are platelets present in relatively normal number (roughly 5 per high-power field), or are they reduced in number?
-
3.
Focus on the red blood cells examining size (normal erythrocyte diameter is about the size of a lymphocyte nucleus), distribution of size, and the area of central pallor (normally about one-third the cell diameter). Are the cells normochromic or hypochromic?
-
4.
Search for abnormal morphologic findings (e.g., schistocytes, spherocytes, echinocytes, acanthocytes, dacrocytes) and for red cell inclusions (e.g., Howell-Jolley bodies, ring forms indicative of babesia or malaria). Note that one or two schistocytes may be found per high-power field on normal peripheral blood smears. In addition, although degmacytes (bite cells), indicative of hemolysis due to oxidative stress in individuals with glucose-6-phosphate dehydrogenase deficiency (G-6-PD deficiency) and seen in Heinz body hemolytic anemia, are seen on conventional Wright stained blood smears, Heinz bodies themselves require supravital staining with new methylene blue for visualization.
Case 2. Evaluation of Nutritional and Other Causes of Anemia
A 27-year-old woman with no significant past medical history presents to her primary care physician for a routine visit. She occasionally takes ibuprofen for headaches but takes no other medications. On review, she notes mild fatigue but attributes this to long hours at work. She has never been pregnant, and notes regular, but heavy menses. Physical examination is essentially unremarkable. A complete blood count reveals a hemoglobin level of 10.5 g/dL with an MCV of 78 fL and RDW of 18 %.
Question 4.
What is the best testing strategy in this individual for the diagnosis of iron deficiency?
-
A.
Serum iron, serum transferrin
-
B.
Serum iron, serum total iron binding capacity
-
C.
Serum ferritin
-
D.
Serum soluble transferrin receptor
When any significant degree of anemia is present, the diagnosis of iron deficiency is usually straightforward (DeLoughery 2014). Red cell indices demonstrating a low MCV and elevated RDW especially in the context of a low reticulocyte count strongly suggest the diagnosis, which is further supported by the finding of hypochromia on review of the peripheral blood smear. In such a setting, the serum ferritin value is confirmatory, and there is usually little utility in obtaining serum iron and transferrin levels, as they do not provide additional clinically relevant information. Although serum iron is typically low and serum transferrin or total iron binding capacity is typically high in iron deficiency, differences in day-to-day oral iron intake can lead to the finding of serum iron levels in the normal range, and inflammatory conditions can lower the serum transferrin and total iron binding capacity. For reference, note that serum transferrin represents about 95 % of the total iron binding capacity.
The diagnosis of iron deficiency is somewhat more complicated when anemia is absent or only very mild because there is no perfect laboratory test for the assessment of body iron stores. However, in the absence of systemic disease such as infection, inflammation, or malignancy, a low serum ferritin level does correlate in a relatively reliable manner with the presence of iron deficiency. However, since ferritin is stored in the liver and is an acute phase reactant, both hepatic injury and the inflammatory response can lead to elevated serum ferritin levels even when iron deficiency is present. For example, iron deficiency may be present in individuals with rheumatoid arthritis even with serum ferritin levels of up to approximately 100 μg/L. In this setting, soluble transferrin receptor has been investigated as a marker of iron deficiency. Although somewhat promising, its utility for this purpose has yet to be fully established (Braga et al. 2014), especially since in most cases when anemia is present, the diagnosis can be established by integrating the information from red blood cell indices, the reticulocyte count, and review of the peripheral blood smear.
Question 5.
Some oval-shaped larger red blood cells (ovalocytes) and several neutrophils with five lobes are seen on review of the 27-year-old woman’s blood smear raising the possibility of a mixed picture anemia. What are the most appropriate tests to obtain in the evaluation for megaloblastic anemia?
-
A.
Serum folate, vitamin B12 level
-
B.
Red cell folate, vitamin B12 level
-
C.
Plasma homocysteine level, vitamin B12 level
-
D.
Plasma homocysteine level and methylmalonic acid level
In the past, there has been some controversy as to whether serum folate or red blood cell folate levels were more accurate in the diagnosis of folate deficiency. Serum folate levels reflect recent dietary intake, whereas red blood cell folate levels are thought to be more reflective of tissue folate stores over the course of several months, given the life span of the red blood cell. Though on theoretical grounds use of red blood cell folate might seem more accurate in the diagnosis of folate deficiency, this more expensive test does not seem to correlate with true deficiency any better than serum folate (Farrell et al. 2013).
If a borderline value of serum folate is observed or if there is still question as to whether or not true folate deficiency is present after a serum folate level is measured, a homocysteine level can be obtained. In the absence of renal failure and certain other conditions that lead to elevated homocysteine levels, a markedly elevated (about twice normal) plasma homocysteine level is generally indicative of folate deficiency.
As opposed to folate deficiency, which has become less common since the supplementation of flour with folate in developed countries, vitamin B12 deficiency may actually be increasing somewhat in incidence due to a variety of factors. Factors that have recently lead to an increased incidence of vitamin B12 deficiency include increased use of certain medications such as proton pump inhibitors and metformin, more widespread use of gastric bypass procedures, and an aging population that is subject to food-cobalamin malabsorption.
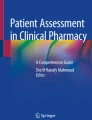
When vitamin B12 deficiency is suspected due to hematologic or neurologic findings, obtaining a serum vitamin B12 (cobalamin) level first is appropriate. Serum vitamin B12 levels less than 200 ng/L are almost always indicative of deficiency. Values above 350 ng/L are generally not associated with true deficiency. When values fall between 200 and 350 ng/L and anemia, macrocytosis, or neurologic symptoms are present, it is reasonable to obtain a methylmalonic acid level (Hunt et al. 2014). In the absence of renal failure and certain other conditions, the methylmalonic acid level measured by methods such as gas chromatography is a more accurate marker of deficiency than the vitamin B12 level itself, which is measured using a bioassay. Figure 1 illustrates a reasonable approach to diagnosis.

Diagnostic approach to vitamin B12 deficiency
Usually, the cause of anemia is suggested by review of the complete blood count and thoughtful review of the peripheral blood smear and is often confirmed by additional testing that can be performed on peripheral blood. Additional or more invasive testing, such as the uncomfortable and expensive procedure of bone marrow aspirate and biopsy, can therefore often be avoided. For example, when normocytic anemia with normal morphology is found in the setting of type 2 diabetes mellitus and a mildly elevated serum creatinine, a serum erythropoietin level can be obtained. This will often demonstrate that a low or inappropriately normal erythropoietin level is responsible for the anemia present (Bosman et al. 2001).
Ultimately, the decision regarding when to proceed to perform a bone marrow examination in the evaluation of anemia relies heavily on clinical judgment based upon the individual setting and totality of the evidence available for evaluation. Aside from obvious situations, such as when other cell lineages are affected or when abnormal leukocytes are present in the blood, certain features associated with anemia should provoke consideration of performing this diagnostic procedure sooner rather than later.
In the setting of a normal MCV, the finding of dacrocytes (teardrop cells) on review of the peripheral blood smear should provoke earlier consideration of the utility of a bone marrow examination. The reason for this is that this evaluation will effectively provide an explanation in a number of these cases given that the underlying process responsible for the morphologic abnormality resides there. These processes include marrow replacement with hematologic malignancies (e.g., lymphoma, myeloma), metastatic disease (e.g., breast cancer, small cell lung cancer), infectious processes, or fibrosis (myelofibrosis).
Case 3. Common Diagnostic Entities in Children and Adults
A previously well 1-year-old male is found on screening to have a hemoglobin value of 9 g/dL on a screening test performed at a routine visit to the pediatrician. His mother notes nothing out of the ordinary in his behavior. He is in the 90th percentile for weight and is taking cereal along with pureed fruits and vegetables in his diet while he continues to breast feed.
Question 6.
The most likely diagnosis in this child is:
-
A.
Diamond-Blackfan syndrome
-
B.
Transient erythroblastopenia of childhood
-
C.
Congenital dyserythropoietic anemia
-
D.
Iron deficiency anemia
Iron deficiency is the most common cause of anemia found in pediatric primary care (Powers et al. 2015). Less commonly, anemia may be a prominent associated feature of other hereditary or acquired conditions, such as Diamond-Blackfan syndrome or sickle cell disease. Diagnostic considerations include, among others, transient erythroblastopenia of childhood, a condition of unknown etiology which resolves spontaneously without intervention (van den Akker et al. 2014).
In children, iron deficiency anemia presents with microcytosis and an increased RDW. A confounding factor may be the concomitant presence of lead poisoning. Lead poisoning in the absence of iron deficiency is not commonly associated with microcytic anemia. However, it may be associated with the occurrence of punctate basophilic stippling, which is not a finding in iron deficiency. Of particular note, iron deficiency increases the risk for lead poisoning because this condition is associated with increased absorption of lead (Eden and Sandoval 2012). Although zinc protoporphyrin levels are increased in iron deficiency, they are markedly increased (greater than 150 μg/dL) when lead poisoning is also present, and this may be helpful in identifying the latter (Hershko et al. 1985).
In adults, as in children, iron deficiency is by far the most common cause of anemia (Killip et al. 2007). Roughly 5 % of women of reproductive age in developed countries have iron deficiency anemia due to menstrual blood loss and inadequate dietary intake. Iron deficiency anemia is also a common cause of anemia in men and postmenopausal women primarily due to gastrointestinal blood loss. Therefore, with rare exception, the diagnosis of iron deficiency anemia in men and older women should provoke specialty referral to identify the source of blood loss. Another cause of anemia commonly observed in adult primary care is the normocytic anemia associated with mild renal insufficiency in the setting of type 2 diabetes mellitus.
In older adults, the incidence of different types of anemia shifts somewhat (Joosten 2004). Aside from the physiologic decline in hemoglobin concentration that is expected in men over the age of 70, anemia associated with renal insufficiency and vitamin B12 deficiency is more prevalent in this age group, as well as, less commonly, folate deficiency. In addition, more worrisome causes of anemia, such as myelodysplastic syndromes and multiple myeloma, require consideration.
Anemia is particularly an issue in the inpatient setting. About 10 % of hospitalized patients are found to be anemic (Rachoin et al. 2013). Acute blood loss anemia, the anemia of renal disease, and the anemia of inflammation (also known as the anemia of chronic disease) are among the most common types of anemia observed in hospitalized adults. All three of these conditions generally present as normocytic anemia, although the anemia of inflammation may present with a modest microcytosis. Chronic blood loss anemia is also not infrequently observed, usually due to intermittent or ongoing gastrointestinal blood loss. Distinguishing between these various causes can be somewhat challenging in the acute care setting because of potential overlap in the diagnostic laboratory values of these entities, which may present with a low reticulocyte count.
Blood loss with surgical procedures and phlebotomy may lead to anemia in a significant proportion of hospitalized patients. In the immediate aftermath of blood loss or in the setting of other comorbid conditions, the reticulocyte count may not yet be increased. Though the anemia due to erythropoietin deficiency associated with severe chronic kidney disease or kidney failure is well recognized, anemia due to this same mechanism may also occur in the setting of mild to moderate chronic kidney disease. This is particularly the case in individuals with diabetes mellitus. Diabetic nephropathy manifesting with modestly increased creatinine values just above the normal range may be associated with erythropoietin deficiency and moderate to severe anemia (Singh et al. 2009). In this particular setting, it is important to remember that an erythropoietin value in the normal range is actually abnormal. Even a modest decrement in hemoglobin should be associated with an erythropoietin level above the normal range (Erslev 1991).
The anemia of inflammation is associated with various infectious diseases, rheumatologic conditions, and malignancies and therefore is particularly common among hospitalized medical patients. In addition, patients are not infrequently hospitalized for further evaluation or management of upper or lower gastrointestinal bleeding associated with intermittent or chronic blood loss. Laboratory features that can help distinguish these common causes of anemia are noted in Table 5.
Case 4. Undiagnosed Congenital Causes of Anemia in Adulthood
A 36-year-old woman is referred to the clinic for further evaluation of mild anemia. She has no significant past medical history and takes no medications. Her family is of northern European decent, and she does note that her mother and sister have also been told at times that they are anemic. Physical examination is notable for a palpable spleen tip, but the remainder of the examination is normal. The complete blood count reveals a hemoglobin of 11.8 g/dL, MCV 90 fL, RDW 15 %. A reticulocyte count is 2.4 %. Review of the peripheral blood smear does not reveal abnormal morphology to be present.
Question 7.
The most likely hereditary cause of anemia in this woman is:
-
A.
Alpha-thalassemia trait
-
B.
Glucose-6-phosphate dehydrogenase deficiency
-
C.
Homozygous hemoglobin E
-
D.
Hereditary spherocytosis
Individuals with certain congenital causes of anemia, such as sickle cell anemia and ß-thalassemia major, generally present early in life and are diagnosed as infants or young children. On the other hand, there are several hereditary conditions that may go unnoticed until well into adulthood or even throughout life. Individuals may be asymptomatic, and the finding of a hemoglobin value below the normal range on a routine complete blood count is the only finding that provokes further diagnostic evaluation. Consideration of these hereditary conditions in the differential diagnosis of an adult with mild to moderate anemia can help direct the evaluation and avoid unnecessary diagnostic testing.
Such undiagnosed types of anemia may be divided into asymptomatic conditions that have been continually manifest since childhood, some of which tend to become more apparent with age and conditions that may only manifest transiently (Table 6). The α-thalassemia types involving deletion of two of the four α-globin genes may be associated with mild anemia with hemoglobin values about 0.5–1 g/dL below the lower limit of normal and a marked microcytosis with MCV values of 65–75 fL (DeLoughery 2014). Appropriate identification of the etiology of the microcytosis in these individuals is important in order to avoid inappropriate empiric iron supplementation. Because of the wide range of expression that may be associated with ß-globin mutations, certain individuals with sickle cell ß+-thalassemia may be entirely asymptomatic or may have such mild manifestations of sickle cell disease, such that they go undiagnosed until they are adults. Hemoglobin E is prevalent in Southeast Asia, and homozygotes have microcytic red blood cells accompanied by minimal anemia (Rees et al. 1998). Individuals with mutations in glucose-6-phosphate dehydrogenase may have intermittent hemolysis that is provoked by oxidant stress associated with viral infections, pharmaceuticals, and even certain foods (Cappellini and Fiorelli 2008). Mild cases of hereditary spherocytosis, which is most common in individuals of northern European decent, may go unnoticed until adulthood. Associated findings in adults with mild cases of hereditary spherocytosis may include mild scleral icterus associated with modestly increased bilirubin levels, and the diagnosis may also be associated with symptoms or radiographic findings of gallstones. Adults may even have previously undergone cholecystectomy. Although osmotic fragility was previously the primary screening test available for hereditary spherocytosis, the eosin-5′-maleimide-binding test, which is performed using flow cytometry, is more sensitive and is increasingly used for this purpose (King and Zanella 2013). Some other conditions that are sometimes encountered are also listed in Table 6.
Answers
-
Question 1. A
-
Question 2. C
-
Question 3. D
-
Question 4. C
-
Question 5. A
-
Question 6. D
-
Question 7. D
References
Bain BJ. Diagnosis from the blood smear. N Engl J Med. 2005;353:498–507.
Bosman DR, Winkler AS, Marsden JT, Macdougall IC, Watkins PJ. Anemia with erythropoietin deficiency occurs early in diabetic nephropathy. Diabetes Care. 2001;24:495–9.
Braga F, Infusino I, Dolci A, Panteghini M. Soluble transferrin receptor in complicated anemia. Clin Chim Acta. 2014;431:143–7.
Cappellini MD, Fiorelli G. Glucose-6-phosphate dehydrogenase deficiency. Lancet. 2008;371:64–74.
Christensen RD, Henry E, Jopling J, Wiedmeier SE. The CBC: reference ranges for neonates. Sem Perinatol. 2009;33:3–11.
DeLoughery T. Microcytic anemia. N Engl J Med. 2014;371:1324–31.
Eden AN, Sandoval C. Iron deficiency in infants and toddlers in the United States. Pediatr Hematol Oncol. 2012;29:704–9.
Erslev AJ. Erythropoietin. N Engl J Med. 1991;324:1339–44.
Farrell CJ, Kirsch SH, Herrmann M. Red cell or serum folate: what to do in clinical practice? Clin Chem Lab Med. 2013;51:555–69.
Hershko C, Konijn AM, Link G, Moreb J, Grauer F, Weissenberg E. Combined use of zinc protoporphyrin (ZPP), mean corpuscular volume and haemoglobin measurements for classifying microcytic RBC disorders in children and young adults. Clin Lab Haematol. 1985;7:259–69.
Hunt A, Harrington D, Robinson S. Vitamin B12 deficiency. BMJ. 2014;349:g5226.
Joosten E. Strategies for the laboratory diagnosis of some common causes of anemia in elderly patients. Gerontology. 2004;50:49–56.
Killip S, Bennett JM, Chambers MD. Iron deficiency anemia. Am Fam Physician. 2007;75:671–8.
King M-J, Zanella A. Hereditary red cell membrane disorders and laboratory diagnostic testing. Int J Lab Hematol. 2013;35:237–43.
Nilsson-Ehle H, Jagenburg R, Landahl S, Svanborg A. Blood haemoglobin declines in the elderly: implications for reference intervals from age 70 to 88. Eur J Haematol. 2000;65:297–305.
Piva E, Brugnara C, Spolaore F, Plebani M. Clinical utility of reticulocyte parameters. Clin Lab Med. 2015;35:133–63.
Powers JM, McCavit TL, Buchanan GR. Management of iron deficiency anemia: a survey of pediatric hematology/oncology specialists. Pediatr Blood Cancer. 2015;62:842–6.
Rachoin JS, Cerceo E, Milcarek B, Hunter K, Gerber DR. Prevalence and impact of anemia in hospitalized patients. South Med J. 2013;106:202–6.
Rees DC, Styles L, Vichinsky EP, Clegg JB, Weatherall DJ. The hemoglobin E syndromes. Ann N Y Acad Sci. 1998;850:334–43.
Singh DK, Winocour P, Farrington K. Erythropoietic stress and anemia in diabetes mellitus. Nat Rev Endocrinol. 2009;5:204–10.
Thom R. Automated red cell analysis. Baillieres Clin Haematol. 1990;3:837–50.
van den Akker M, Dror Y, Odame I. Transient erythroblastopenia of childhood is an underdiagnosed and self-limiting disease. Acta Paediatr. 2014;103:e288–94.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Marks, P.W. (2016). Evaluation of Anemia in Children and Adults. In: Abutalib, S., Connors, J., Ragni, M. (eds) Nonmalignant Hematology. Springer, Cham. https://doi.org/10.1007/978-3-319-30352-9_1
Download citation
DOI: https://doi.org/10.1007/978-3-319-30352-9_1
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-30350-5
Online ISBN: 978-3-319-30352-9
eBook Packages: MedicineMedicine (R0)