
Abstract
While relatively rare in the young child, the incidence of subaxial cervical fractures and dislocations in children over 8 years of age approaches adult rates. Horizontally oriented facet joints and the lack of uncovertebral joints predispose the immature spine to increased motion in the sagittal and coronal planes, respectively. Unilateral facet dislocations result from combined flexion-distraction and rotatory forces which typically occur after motor vehicle accidents or falls from heights. The presentation of these injuries can be subtle as children may complain only of neck pain. A careful physical examination is required to identify pretreatment neurologic deficits. Diagnosis is aided by advanced imaging studies, with Computed Tomography (CT) scans clearly delineating the bony injury while assisting in surgical planning. A pretreatment Magnetic Resonance Imaging (MRI) is recommended to evaluate for both disk herniation and injuries to the posterior ligamentous complex. Unilateral facet dislocations are characterized by a degree of rotational instability, with the axis of rotation centered around the intact contralateral facet. Persistent instability and worse long-term outcomes have been demonstrated with nonoperative treatment in the adult population. While closed reduction and prolonged external immobilization with a halo vest is possible, rigid internal surgical stabilization is preferred in the pediatric population. Solid arthrodesis is frequently attained and, in the absence of spinal cord injury, long-term outcomes are generally good.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others


1 Brief Clinical History
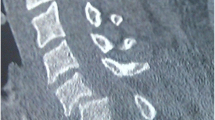
The patient is a 14-year-old female gymnast who was performing a handstand on blocks five feet above ground level when she fell and sustained an axial loading injury to her head and neck. She reported a brief loss of consciousness but was able to ambulate immediately after the injury. She complained of subaxial neck pain, right arm soreness, and right thumb numbness. Neurologic evaluation revealed no motor deficits, mild paresthesias distally in the right C6 dermatome, and an absence of hyperreflexia or pathologic reflexes. She was placed into a cervical collar and advanced imaging was attained. CT findings were notable for a right-sided unilateral facet dislocation at C5–6 with 5 mm of anterior listhesis and fractures of the right C6 pedicle and lateral mass (Fig. 1a–d). MRI demonstrated effacement of the spinal cord at the level of injury without disk herniation. Disruption of the posterior longitudinal ligament was also noted (Fig. 2a–b).

(a) Axial image at level of C5–6 facet joints demonstrating anterior dislocation of right C5 inferior articular facet. (b) Axial image at level of C6 pedicle demonstrating right-sided pedicle and lateral mass fractures. (c) Sagittal images demonstrating unilateral C5–6 facet dislocation. (d) Mid-sagittal image demonstrating anterior listhesis of C5 on C6

Sagittal T2 images showing spinal cord effacement (a, arrow) and edema within the posterior longitudinal ligament, indicative of a ligamentous tear (b, arrow)
3 Preoperative Problem List
-
1.
Unilateral facet fracture/dislocation at C5–6 with anterior listhesis, spinal cord effacement, and disruption of the posterior longitudinal ligament.
-
2.
Right C6 paresthesias without motor deficits
4 Treatment Strategy
The primary aim of treatment in a unilateral facet fracture dislocation is to restore and maintain cervical alignment while minimizing trauma to the spinal cord and nerve roots. Unilateral facet injuries represent a spectrum ranging from a minimally displaced superior articular facet fracture to frank dislocation. Involvement of both the bony and disco-ligamentous structures of the cervical spine is common (Dvorak et al. 2007). In the adult population, considerable controversy exists regarding diagnosis, the timing and manner of reduction, and the optimal technique for post-reduction stabilization (Dvorak et al. 2007; Sellin et al. 2014). The incidence of cervical facet injury in children has rarely been reported in the literature and treatment paradigms are even less clear (Parada et al. 2010; Chen et al. 2013; Sellin et al. 2014).
Closed reduction in the neurologically intact, cooperative, adult patient via skull tongs and sequentially added weight has been described as safe (Kwon et al. 2006). Recently, however, nonoperative treatment of these injuries demonstrated worsening pain and disability scores on validated, disease-specific health related quality of life measures (Dvorak et al. 2007). These findings, in concert with biomechanical studies demonstrating persistent instability after closed reduction and external immobilization, have led to the recommendation for operative treatment with rigid internal fixation in the pediatric population (Sellin et al. 2014).
5 Basic Principles
Prior to undertaking treatment, the importance of performing and documenting a careful neurologic examination cannot be understated. When performing a reduction under anesthesia, neuromonitoring with somatosenory evoked potentials (SSEPs) and transcutaneous motor evoked potentials (tcMEPs) is mandatory. The potentials should be evaluated supine and then again after prone positioning. Application of a halo allows rigid control of the head with the ability to adjust alignment of the cervical spine intraoperatively. Closed reduction is achieved via axial traction, initially in slight flexion, with movement to slight extension as serial lateral c-arm radiographs demonstrate facet alignment and subsequent reduction (Rathjen and Herring 2014).
Open reduction is indicated when closed reduction fails, in the presence of fracture-dislocations, and in the setting of neurologic compromise from disk herniations (Kwon et al. 2006). In the child, reduction can be safely performed through either an anterior or posterior approach (Sellin et al. 2014). Anteriorly, reduction is achieved after diskectomy via distraction pins placed into the vertebral bodies. Arthrodesis with bone graft and plating is then performed. Posterior reduction can be performed via distraction across the spinous processes or laminae. Posterior arthrodesis with lateral mass screws, interlaminar wiring, lateral mass plates, or interlaminar clamps has all been successful (Kwon et al. 2006; Chen et al. 2013; Sellin et al. 2014). Postoperatively, immobilization in a rigid cervical orthosis for a minimum of 3 months is recommended with close clinical and radiographic follow-up to ensure maintenance of reduction.
6 Images During Treatment
See Fig. 3.

Intraoperative images demonstrating a unilateral C5 facet dislocation pre-reduction (a, arrow) and post-reduction (b–arrow). Postoperative AP (c) and lateral (d) images after single level C5–6 posterior fusion with lateral mass screws
7 Technical Pearls
When performing a closed reduction in adults, many authors apply 10–15 pounds of weight for the head and then add 5–10 pounds of weight per level of injury (Kwon et al. 2006). It is important to note that safe weight limits have not been established in the pediatric population and application of halo traction weight should be dictated by surgeon experience and closely monitored with SSEPs and tcMEPs.
If difficulty is encountered when attempting an open posterior reduction, the superior articular facet can be burred away to help disengage the dislocated facets. This may increase instability once reduction is achieved (Kwon et al. 2006).
Lateral mass screw fixation can be safely performed in the pediatric population following the techniques established by either Roy-Camille or Magerl (Roy-Camille et al. 1989; Jeanneret et al. 1991).
8 Outcome Clinical Photos and Radiographs
See Fig. 4.

AP (a) and lateral (b) radiographs at 3 months postoperatively demonstrating early fusion mass consolidation and maintenance of facet reduction
9 Avoiding and Managing Problems
The clinician should maintain suspicion for unilateral facet dislocations in children presenting with neck pain after high energy injuries characterized by flexion-distraction with or without rotational forces. Careful scrutinization of plain radiographs and the use of advanced imaging allow recognition of these injuries. The importance of neuromonitoring when performing reduction is critical to avoid intraoperative neurologic injury. Changes in SSEPs or tcMEPs should prompt the surgeon to evaluate for potential disk herniations or nerve root compression intraoperatively.
As demonstrated by the recent literature, rigid internal fixation with either anterior or posterior arthrodesis can be safely performed in the pediatric population, lessens the risk of post-reduction instability, and has superior clinical outcomes compared to nonoperative treatment (Dvorak et al. 2007; Sellin et al. 2014).
10 Cross-References
References and Suggested Readings
Chen Y, Wang X, Chen D, Liu X (2013) Surgical treatment for unilateral cervical facet dislocation in a young child aged 22 months old: a case report and review of the literature. Eur Spine J 22(Suppl 3):S439–S442
Dvorak MF, Fisher CG, Aarabi B et al (2007) Clinical outcomes of 90 isolated unilateral facet fractures, subluxations, and dislocations treated surgically and nonoperatively. Spine 32(26):3007–3013
Jeanneret B, Magerl F, Ward EH, Ward JC (1991) Posterior stabilization of the cervical spine with hook plates. Spine 16(Suppl 3):S56–S63
Kwon BK, Vaccaro AR, Grauer JN et al (2006) Subaxial cervical spine trauma. J Am Acad Orthop Surg 14:78–89
Parada SA, Arrington ED, Kowalski KL, Molinari RW (2010) Unilateral cervical facet dislocation in a 9-year old boy. Orthopedics 33(12):929
Rathjen KE, Herring JA (2014) Spinal injuries. In: Herring JA (ed) Tachdjian’s pediatric orthopaedics, 5th edn. Elsevier Saunders, Philadelphia, pp 1224–1244
Roy-Camille R, Saillant G, Mazel C (1989) Internal fixation of the unstable cervical spine by a posterior osteosynthesis with plate and screw. In: Cervical Spine Research Society (ed) The cervical spine, 2nd edn. JB Lippincott, Philadelphia, pp 390–403
Sellin JN, Shaikh K, Ryan SL et al (2014) Clinical outcomes of the surgical treatment of isolated unilateral facet fractures, subluxations, and dislocations in the pediatric cervical spine: report of eight cases and review of the literature. Childs Nerv Syst 30:1233–1242
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Section Editor information
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this entry

Cite this entry
Kaufman, B.E., Heydemann, J.A., Shah, S.A. (2020). Unilateral Cervical Facet Fracture-Dislocation. In: Iobst, C., Frick, S. (eds) Pediatric Orthopedic Trauma Case Atlas. Springer, Cham. https://doi.org/10.1007/978-3-319-29980-8_70
Download citation
DOI: https://doi.org/10.1007/978-3-319-29980-8_70
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-29979-2
Online ISBN: 978-3-319-29980-8
eBook Packages: MedicineReference Module Medicine