
Abstract
Epidermoid cysts are benign congenital lesions arising from the accidental inclusion of normal ectodermal epithelial tissue during neural tube closure in early embryogenesis. They grow from the slow accumulation of the products of the desquamation of the stratified keratinized epithelium that constitutes the cyst walls. Intracranial epidermoid cysts are ubiquitous, but about half of intracranial epidermoid cysts are located in the cerebellopontine angle. They are occasionally encountered in the sellar region, where they usually present in middle-aged patients with nonspecific neurologic symptoms rather than endocrine disturbances, such as headaches, visual impairment, or cranial nerve deficits. Intrasellar epidermoid cysts are extremely rare and have been reported as a cause of hypophysitis or mimicking pituitary apoplexy. In cases of trigeminal neuralgia, specific extension into Meckel cave should be meticulously sought. Epidermoid cysts are commonly large when symptomatic because these slow-growing malleable masses softly insinuate into pericerebral cisterns, where at first they gently encase and surround cranial nerves and vessels, and only later, when bigger, displace, stretch, and finally exert mass effect on cerebral structures.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Epidermoid cysts are benign congenital lesions arising from the accidental inclusion of normal ectodermal epithelial tissue during neural tube closure in early embryogenesis. They grow from the slow accumulation of the products of the desquamation of the stratified keratinized epithelium that constitutes the cyst walls. Intracranial epidermoid cysts are ubiquitous, but about half of intracranial epidermoid cysts are located in the cerebellopontine angle. They are occasionally encountered in the sellar region, where they usually present in middle-aged patients with nonspecific neurologic symptoms rather than endocrine disturbances, such as headaches, visual impairment, or cranial nerve deficits. Intrasellar epidermoid cysts are extremely rare and have been reported as a cause of hypophysitis or mimicking pituitary apoplexy. In cases of trigeminal neuralgia, specific extension into Meckel cave should be meticulously sought. Epidermoid cysts are commonly large when symptomatic because these slow-growing malleable masses softly insinuate into pericerebral cisterns, where at first they gently encase and surround cranial nerves and vessels, and only later, when bigger, displace, stretch, and finally exert mass effect on cerebral structures.
On CT, epidermoid cysts appear hypodense with possible marginal calcifications. On MRI they have a fluid-like low-T1 signal intensity and high-T2 signal intensity, but are slightly brighter than CSF on both T1 and T2 WIs, and show no contrast enhancement after gadolinium administration. They may, however, be difficult to distinguish from arachnoid cysts based on the signal intensities only on those sequences. The shape and edges of these two cysts, however, are very different, as epidermoid cysts present with a unique irregular lobulated cauliflower-like outer surface (Fig. 49.1). With advances in MRI techniques, preoperative diagnosis of epidermoid cysts is now reliable and no longer poses a dilemma. On FLAIR sequence, epidermoid cysts can be easily differentiated from arachnoid cysts because the former show mixed iso- to hypersignal intensities, but with poor demarcation, while the signal of the latter is suppressed, like the signal of CSF. Heavily T2W 3D sequence, also called MR cisternography, demonstrates epidermoid cyst hypointense to CSF, and thus nicely demonstrates the lobulated margins of the tumor and clearly depicts its precise extent (Fig. 49.2). DWI offers a finding specific for extra-axial epidermoid cysts by showing a very high signal. Restricted ADC compared with CSF, almost comparable with that of the brain, and T2 shine-through effect both play an important role in the high signal intensity of epidermoid cyst at DWI. DWI is also crucial in the postoperative follow-up, as it allows confirmation of the presence of a possible residual tumor. Finally, MR spectroscopy may also be helpful, especially in cases of atypical epidermoid cysts, as it shows a unique pattern with only an elevated lactate peak.

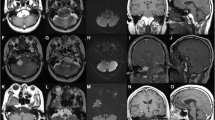
Suprasellar epidermoid cyst (asterisk). (a) Sagittal T1WI shows large, suprasellar hypointense cyst with posterior extension impinging mesencephalon and pons, and upward displacement of the floor of the third ventricle (thin arrows). (b) Coronal CE T1WI demonstrates no enhancement of this suprasellar cyst with typical ill-defined borders indenting the brain parenchyma laterally. (c) Coronal T2WI demonstrates the very high signal intensity of the lesion that becomes characteristically isointense on (d) FLAIR image. (e) Diffusion-weighted axial image reveals very suggestive hyperintense signal. (f) Long echo-time MR spectroscopy depicts only lactate in epidermoid cyst, a metabolite that appears as a negative doublet at 1.3 ppm

Suprasellar epidermoid cyst. (a) Sagittal CE T1WI and (b) Sagittal T2WI show a large, nonenhancing nebulous cyst filling the optochiasmatic cistern, encasing the pituitary stalk, and displacing the floor of the third ventricle upward. (c) Axial DWI shows the characteristic hyperintense signal of the epidermoid cyst (Courtesy of J. Savatovsky, MD)
Further Reading
Bonneville F, Savatovsky J, Chiras J (2007) Imaging of cerebellopontine angle lesions: an update. Part 2: intra-axial lesions, skull base lesions that may invade the CPA region, and non-enhancing extra-axial lesions. Eur Radiol 17(11):2908–2920
Ren X, Lin S, Wang Z et al (2012) Clinical, radiological, and pathological features of 24 atypical intracranial epidermoid cysts. J Neurosurg 116(3):611–621
Tuna H, Torun F, Torun AN et al (2008) Intrasellar epidermoid cyst presenting as pituitary apoplexy. J Clin Neurosci 15:1154–1156
Zada G, Lin N, Ojerholm E, Ramkissoon S, Laws ER (2010) Craniopharyngioma and other cystic epithelial lesions of the sellar region: a review of clinical, imaging, and histopathological relationships. Neurosurg Focus 28(4):E4
Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Bonneville, F. (2016). Epidermoid Cyst. In: MRI of the Pituitary Gland. Springer, Cham. https://doi.org/10.1007/978-3-319-29043-0_49
Download citation
DOI: https://doi.org/10.1007/978-3-319-29043-0_49
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-29041-6
Online ISBN: 978-3-319-29043-0
eBook Packages: MedicineMedicine (R0)