
Abstract
This patient had breast augmentation in Thailand with round, smooth, silicone implants in the submuscular position. When she flexes her pectoral muscles, she gets a double-bubble appearance. The Group discussed whether this was a true double bubble or not, the implant size and type to correct the problem, and insertion of the implants into the subglandular position.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Submitted by Kirby: February 20, 2013
This is a 22-year-old young woman who had a breast augmentation performed in Thailand, supposedly 300 mL MP silicone, smooth, round, submuscular, and transaxillary approach. Bra size before the surgery was 10 B and is now 10 D to DD.
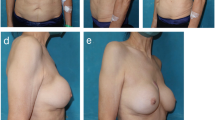
At rest the cosmetic effect is excellent (Fig. 65.1), but when she flexes her pectoral muscles, she gets the above appearance (Fig. 65.2). Any suggestions regarding causes and options for corrective surgery? She is keen on larger implants if she has to have a revision.

Following transaxillary breast augmentation

With flexion of the pectoral muscles
Mangubat
Send preoperative pictures if you have them. I suspect it will show her breast base diameter to be much smaller than the implant and perhaps a small constriction. This is a good example of the disadvantage of large implants in small breasts especially if there is a constriction deformity.
Topchian
I think this is an example of “window shading” where the muscle compresses the implant and causes the obvious movement and deformity shown. Also, the inferior mammary fold (IMF) ligament is attached to the pectoralis major, so when the muscle contracts it pulls on the old IMF.
Although the current implants are said to be “submuscular,” the dissection must have detached the lower part of the pectoralis major in order to allow for lower pole fill and allow insertion of the implants. So it is probably more likely a dual plane technique.
The solution, in my opinion, would be simply to place the implants on top of the muscle. The same ones could be reused; however, if she is to have a reoperation, consideration should be given to polyurethane implants because of their known advantages. I would recommend an IMF incision for the revision surgery, with drains for 1–2 days.
Prochazka
I would agree with Tony’s (Mangubat) assessment. She should have had inframammary approach, submammary pockets and posterior scoring of the breast parenchyma to spread it out, and small-diameter ultra-high-profile implants.
This is the problem with the Thai cosmetic surgery tourism industry. The surgeons there just do the operation the same way every time, knowing that the client cannot stay around to harass them if the result is no good. People who get good results there can count themselves lucky. I have heard some appalling stories and seen some appalling results. I have had patients break down in front of me and wail “Why was I so stupid?”
Still, it is what it is and here to stay.
Chan: February 21, 2013
This is a typical case of active breasts. There is not much you can do for this. This only occurs on flexing the muscle and can only be seen out of clothes. This occurs in 10–15 % of the breast augmentation population.
Do nothing; reassure the patient, no surgery required. By going larger, it will not eliminate active breast. This is inherent to her. If she definitely wants this gone, she needs to go subglandular.
I think the Thai surgeon work is good. But I am not for overseas surgery as it is so variable. I have corrected quite a lot of overseas work.
This is not double bubble (DB). DB occurs at rest where one can see the old IMF on the breast. At rest her results are good. Most double bubble can be eliminated at surgery by dissecting the IMF fascia and the ligament.
Kirby
Thank you for your comments so far.
Regarding Tony Mangubat’s reply, unfortunately I do not have her preoperative photos as her surgery was performed in Thailand.
Secondly, I was somewhat confused; as my understanding of double bubble was that the deformity is there at rest. In this case, the deformity is only visible when there is active constriction of the pectoral muscles, as the transverse line that is visible is obviously the lower border of the pectoral muscles exerting their pull. I wondered if the medial attachment of the muscle was inadequately released with the transaxillary approach.
I take on board that one of the possible solutions is subglandular placement, maybe with polyurethane implants as she was only a 10 B cup size preoperatively, with not much breast tissue cover. However, if she wishes to go larger, a similar medium-profile polyurethane implant may be more detectable as the edge of these stiffer implants is sometimes felt at the top, or beneath the scar, although not seen. The teardrop option would not provide the same projection or cleavage at the top.
I would appreciate any further comments or suggestions about this case, as well as preferences for types of polyurethanes used by others. Round vs. teardrop, high vs. medium or low profile, etc.
Thank you again for all of the comments so far. They have been very valuable.
Higgs
This is a classic case of “double-bubble” deformity, also referred to as “double-fold” deformity. The lower fold is the lowest part of the implant and the upper fold is due to the persistent inframammary fold ligament, which is attached to the pectoralis major fascia and the dermis.
This deformity can be avoided by not dissecting below the native fold, i.e., having the implant sit above the fold or deliberately destroying the attachments of the ligament to the pectoralis fascia, difficult but not impossible via the axilla. An Agris-Dingman dissector can be used for this. However, the best way to avoid this is to use a subglandular or subfascial plane in the first place. In order to open into the subglandular plane, it is necessary to open through the attachment of the inframammary fold ligament to the pectoralis fascia. This is why double bubble is not seen with subglandular augmentation.
I would revise her through an inframammary incision in the new fold and put the implants in new subglandular pockets. The weight of the implant will close the old pocket. No drains will be required. I would counsel her against a larger implant, explaining she has had one complication and does not want further problems that increase with implant size. It is ok to use the same implants; in fact, there is experimental evidence to show returning an implant coated with the patient’s own protein causes less reaction than a new silicone implant [1].
Beldholm: February 22, 2013
Definitely not double fold. As you correctly noted, there is minimal deformity at rest. I have also found that double folds tend to settle with time (I have had a few, but in girls that have tight folds I always score the lower pole intraoperative). I have not had double fold that persisted past 12 months.
I think most likely the pectoralis muscle was not divided adequately at the operation. It is difficult to do this via the transaxillary approach. I also note that her breast folds are not equal. The left being more superior, I would lower this at a revision.
The easiest solution would be to make a new pocket above the muscle and use the same implants. She certainly has an adequate size that fits her figure. If she was a B cup beforehand, then there should be enough coverage.
Unfortunately in my experience, if they want bigger, then they are not going to be happy even if you solve her main issue, unless you give her bigger implants.
Then it comes down to what result she wants: round breast, “fake” looking or natural.
If I had to go bigger, then I would use polyurethane above the muscle. The implant would depend on the breast base, and I would check this with an actual implant to make sure it will fit and look appropriate. If you go bigger than 360 mL, then most likely high profile and you would run the risk of visible implant edge above the muscle. Teardrop I think has much less chance of having visible implant edge in the superior pole of the breast.
Reference
Marques M, Brown SA, Cordeiro NDS, Rodrigues-Pereira P, Cobrado ML, Morales-Helguera A, Queiros L, Luis A, Freitas R, Goncalves-Rodrigues A, Amarante J (2011) Effects of coagulase-negative staphylococci and fibrin on breast capsule formation in a rabbit model. Aesthet Surg J 31(4):420–428
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Kirby, R. et al. (2016). Case 157: Classic Double Bubbles. In: Higgs, M., Shiffman, M. (eds) Cosmetic Breast Cases. Springer, Cham. https://doi.org/10.1007/978-3-319-27714-1_65
Download citation
DOI: https://doi.org/10.1007/978-3-319-27714-1_65
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-27712-7
Online ISBN: 978-3-319-27714-1
eBook Packages: MedicineMedicine (R0)