
Abstract
Symptomatic thoracic disc herniations (TDHs) may severely incapacitate the patient while posing a significant challenge to the attending neurosurgeon. With the development of safer, less destructive surgical techniques, every symptomatic TDH may now be considered for surgical resection, provided it has enough impact on quality of life and conservative treatment has failed. While many open, endoscopic, or even percutaneous techniques have been developed using a posterior, posterolateral, or anterior route, today, thoracoscopic microdiscectomy (TMD) may be regarded as the golden standard because of its versatility, excellent results, and very low complication rates even in the most challenging cases. There are, however, a steep learning curve and a critical caseload to acquire and retain specific surgical skills. Moreover, close cooperation with a dedicated neuroradiologist, neuroanesthesiologist, and neurophysiologist is a prerequisite.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction and Core Message
Symptomatic thoracic disk herniations (TDHs) may severely incapacitate the patient while posing a significant challenge to the attending neurosurgeon. With the development of safer, less destructive surgical techniques, every symptomatic TDH may now be considered for surgical resection, provided it has enough impact on quality of life and conservative treatment has failed. While many open, endoscopic, or even percutaneous techniques have been developed using a posterior, posterolateral, or anterior route, today, thoracoscopic microdiskectomy (TMD) may be regarded as the golden standard because of its versatility, excellent results, and very low complication rates even in the most challenging cases. There are, however, a steep learning curve and a critical caseload to acquire and retain specific surgical skills. Moreover, close cooperation with a dedicated neuroradiologist, neuroanesthesiologist, and neurophysiologist is a prerequisite.
2 Incidence
TDHs are believed to be relatively rare as compared to their cervical and lumbar counterparts [1–3]. In their landmark paper (1950), Love and Kiefer estimated their incidence at 2–3 per thousand disk herniations [4]. However, more recently (1995) Wood et al. demonstrated a high prevalence of disk herniation (37 %) and spinal cord deformation (29 %) on MRI of the thoracic spine in asymptomatic individuals [5]. The true incidence of symptomatic TDHs is likely underestimated because of their variable and often misleading clinical presentation [4, 6–14]. However, with increased clinical awareness (directly linked to the development and implementation of safer surgical techniques) and advanced imaging techniques, more symptomatic cases are presented to the neurosurgeon nowadays. As a tertiary referral center, we have surgically treated almost 400 patients with one or more symptomatic TDHs over the past 14 years. This chapter is a reflection of our experience including some modifications of the original thoracoscopic microdiskectomy (TMD) technique [15, 16].
3 Diagnosis
3.1 Clinical Presentation
The symptomatic onset of TDH is gradual and without precipitating or traumatic event in the majority of cases [3]. In less than 5 %, however, it may be more (sub)acute [17]. Diagnosis is often difficult because of nonspecific presenting symptoms that may be a combination of myelopathy, coordination problems in one or both legs, axial pain, band-like pain (of medullary origin but often misinterpreted as radiculopathy), pain in one or both legs, bladder dysfunction, or even bowel dysfunction. Axial pain is often present but for unknown reasons may vary between profoundly incapacitating in some and completely absent in others with almost identical imaging. Band-like pain may mimic cardiac, gallbladder, gastric, or even gynecologic disease depending on level and lateralization of the TDH, due to the referred pain mechanism (see also Chap. 21) [9]. Moreover, patients may report the feeling of a heavy weight resting on their chest and the inability to take a deep breath. Clearly, to avoid significant diagnostic delay, the clinician must have an appropriately high level of suspicion.
Upper (T6–T7 and above) and even lower TDHs [14] may produce shoulder pain and a non-radicular, predominantly proximal brachial pain. Lifting objects especially above shoulder level will often exacerbate axial pain associated with (upper) TDHs. Lower TDHs including those at the thoracolumbar junction (T10–T11 till T12–L1) may present with any combination of upper and/or lower motor neuron disease or even cauda equina compression [10, 11, 13]. Those at T11–T12 are often accompanied by a 360° stenosis (short pedicles, hypertrophic facets, and hypertrophic flaval ligaments) (Fig. 19.1) and may present with predominantly lower motor neuron symptoms (weakness in the lumbosacral myotomes often presenting as progressive foot drop), a condition termed compressive lumbar myelopathy by Kleopa et al. [10].

Broad-based TDH at T11-T12 with hyperintense spot in the center of the spinal cord (a), accompanied by a 360º stenosis and medullar compression (b)
Anand [6] and Regan [15] introduced a clinical grading system for symptomatic TDHs (Table 19.1). In our experience, however, the frequently reported band-like pain (as in type 2, 3A, and 3B) rarely has a radicular origin. As the pain is dull, covers several dermatomes, and is not controlled by an intercostal nerve block, it should be regarded as an early myelopathic sign instead. In this regard, it should be noted that myelopathy associated with TDHs may not be manifest during routine neurological examination. Such patients may report coordination problems, a loss of automated movements, or a subjective loss of power in one or both legs and/or a micturition problem and should be classified as a type 4 (myelopathy without significant motor weakness).
3.2 Radiological Presentation and Some Pathophysiological Considerations
TDHs are often observed in association with Scheuermann’s disease (approximately two-thirds in our surgical series) and as such may be related to a growth disorder of the thoracic spine in the first two decades rather than to degenerative disk disease later in life (Fig. 19.2).

Segmental hydromyelia and marked hyperkyphosis in a patient with Scheuermann’s disease (a), note the presence of a small left paramedian TDH exactly at the apex of kyphosis where the spinal cord is very close to the posterior vertebral border and therefore more vulnerable to anterior compression (b)
Why most of them remain asymptomatic for many years or even throughout life remains unknown [2, 12, 18]. We do know, however, that cord compression depends on the dimensions of the disk herniation as well as its relation to the anterior cord surface (median, paramedian, or lateral position) and kyphotic curvature (the spinal cord being closer to the posterior vertebral border and therefore more vulnerable to anterior compression at the apex of the curvature) (Fig. 19.3).

Multiple TDHs in a patient with Scheuermann’s disease, note the presence of several degenerated disks (a) and a left paramedian TDH clearly influencing the spinal cord (b) in the upper thoracic spine
Therefore, a small (para)median disk herniation at the apex of an accentuated curvature may cause severe cord compression, and whenever such a disk herniation is suspected on screening sagittal T2-weighted MR images, high-resolution axial T2-weighted MR images should be acquired at that level (Fig. 19.4).


Small median TDH at T6–T7 near the apex of the curvature and clearly causing cord compression (preoperative sagittal (a) and axial (b) T2-weighted MR image and axial myelo-CT image (c), postoperative sagittal (d) and axial (e) T2-weighted MR image, axial CT image (f), and 3D CT reconstruction (g)). Note the limited bone resection to resect this small median TDH
However, in order to explain why some TDHs are symptomatic and some TDHs causing the same amount of cord compression are not, other factors besides mechanical cord compression must be involved. These may include ischemia caused by venous congestion [19] or even direct arterial compression [20], localized inflammation triggered even by smaller disk herniations causing limited cord compression, and finally a traumatic event acting as a catalyzator for an existing asymptomatic disk herniation to become symptomatic [21].
Conventional X-ray imaging may demonstrate hyperkyphosis (three consecutive segments with >5° angulation each are compatible with Scheuermann’s disease), Schmorl’s nodules, intervertebral disk calcifications, or even a completely calcified giant TDH. Abdominal CT may occasionally demonstrate a calcified TDH in patients investigated for unexplained thoracic or abdominal pain. CT myelography although largely abandoned in favor of MRI to investigate spinal cord compromise in the degenerative spine may still be considered the golden standard for TDHs [22]. It has the ability to exactly visualize every hernia (whether or not calcified) in relation to the surrounding bony structures (Fig. 19.5).

Axial (a) and sagittal (b) myelo-CT image demonstrating a median TDH just below the apex of kyphosis. Note the spinal cord follows the kyphotic curvature and is therefore situated in the anterior half of the spinal canal close to vertebral bodies and intervertebral disks (a,b)
This is especially useful in case of a giant TDH as an irregular surface facing the compressed spinal cord may correlate with transdural erosion complicating an already demanding procedure [23] (Fig. 19.6). Moreover, sagittal CT reconstructions may help construct a mental 3D image of the disk herniation and its attachment to the vertebral bodies, which is of paramount importance while planning and executing surgery for these challenging lesions (Fig. 19.6). Finally, CT myelography-guided transpleural puncture is our preferred technique to localize the hernia preoperatively [22]. Performed in prone position, it provides beautiful anatomical images, avoids wrong-level surgery, obviates the use of intraoperative X-ray imaging, and helps to choose the side of the approach depending on the relation disk herniation – spinal cord and aorta – spinal column at the involved level. Of note, the aorta moves to a more anteromedial position relative to the spine in prone position especially between T4 and T8 [24].

Calcified giant TDH; note the irregular surface facing the compressed spinal cord correlating with transdural erosion (a). Sagittal CT reconstructions (b) may help construct a mental 3D image of the disk herniation and its attachment to the vertebral bodies. Postoperative axial (c) and sagittal (d) CT images confirm complete resection
Sagittal T2-weighted MR imaging is the most valuable screening tool for the entire spine. It clearly demonstrates whether the disk herniation is solitary or not, whether it is situated at the apex of the kyphotic curvature, and whether it is accompanied by a segmental stenosis (often at T11–T12) (Fig. 19.1) and/or a myelopathy (Fig. 19.7).

Two somewhat dysplastic vertebrae, hypertrophic facets, and a broad-based TDH at T10–T11, note the presence of several degenerated disks in the lower thoracic spine (a) and a hyperintense spot on both sagittal (a) and axial (b) T2-weighted MR images corresponding to a myelopathy
However, MRI technicians should be well trained to make high-resolution axial T2-weighted slices through every level suspect for a disk herniation on screening sagittal images. The amount of spinal cord deformation (flattening) on such images and a position close to or at the apex of the kyphotic curvature are most useful parameters in looking for a symptomatic TDH especially in case of multilevel disease (Fig. 19.3).
4 Surgical Indications
For many years, surgical indications were limited to (progressive) myelopathy. With the development of safer, less destructive techniques, every symptomatic TDH may now be considered for surgical resection provided it has enough impact on quality of life and conservative treatment has failed.
5 Surgical Technique
5.1 From Laminectomy Toward Safer, Minimally Incisional Techniques
In 1969 Perot and Munro [25] presented a summary of outcomes after decompressive laminectomy for TDHs [7, 25]. Out of 91 subjects studied, 56 % improved, 19.8 % did not improve, 17.6 % developed paraplegia, and 6.6 % died. The paper became a turning point away from decompressive laminectomy (nowadays considered obsolete) toward the posterolateral (costotransversectomy, lateral extracavitary, and transpedicular) approach [26–31] and the anterior (thoracotomy) approach [25]. Over the years, surgical techniques have been refined to obtain at least equivalent results with less soft-tissue disruption. Drawbacks of a costotransversectomy are the limited access to the contralateral disk without spinal cord retraction, a limited working window when performing broader decompressions for larger TDHs, retraction trauma of the ipsilateral paraspinal musculature, and an often unavoidable rhizotomy [27]. Advantages of a thoracotomy especially when confronted with large, central, and transdural TDHs prompted its adoption as the standard in TDH surgery. However, besides the neurosurgeons’ unfamiliarity with intrathoracic anatomy, drawbacks were the approach-related morbidities including pulmonary dysfunction, scapular dysfunction, intercostal neuralgia [32], and last but not the least the feared post-thoracotomy pain syndrome occurring in up to 50 % of patients [3].
To minimize exposure-related morbidity, Rosenthal and Regan (1994) introduced the video-assisted thoracoscopic microdiskectomy (TMD) technique as a minimally incisional (rather than minimally invasive) technique [15, 16] (see also Chap. 17). The technique has been successfully adopted in several high-volume centers around the world, but not in many low-volume centers for several reasons: the learning curve associated with 2D visualization of complex 3D anatomy, manipulation of instruments around a target relatively far away, management of complications using endoscopic techniques, instrumentation setup cost, and the need for dedicated nursing and anesthesiological staff that may be unavailable when case load is limited [3, 32]. For these reasons, some surgeons have adopted a mini-open approach [3, 33, 34], which should combine the best of two worlds (little soft-tissue disruption and 3D visualization). Bartels et al. (2007) reported a retrospective cohort study on mini-thoracotomy (n = 21) versus TMD (n = 7) for calcified TDHs [34]. They prefer the mini-thoracotomy, which they consider as a minimally invasive technique that allows bimanual technique without a steep learning curve. This may be true for low-volume centers; however, one may argue that TDHs are rarely, if ever, a true surgical emergency [17] and should therefore be referred to a high-volume center, which is conform to recent trends toward concentration of complex (surgical) pathology. Arts et al. (2013) reported a comparative cohort study on anterior (mini-thoracotomy, n = 56) versus posterior (transpedicular, n = 44) diskectomies [33]. They observed clinical improvement in most cases, but significantly longer surgery, more blood loss, higher complication rate, and longer hospital stay in the mini-thoracotomy group. These differences, however, were largely attributed to different TDH characteristics as those in the mini-thoracotomy group tended to be larger and harder. They concluded that large, medial, calcified TDHs should be operated through an anterior approach, while the smaller, lateral ones may be treated through a posterior approach as well.
Wait et al. recently reported a retrospective review of 121 TMDs and 39 thoracotomies [35]. Their current selection criteria for TMD are small (<40 % of spinal canal area), anterior, mid-thoracic (T4–T11), non-ossified TDHs, no more than two symptomatic disk herniations, no morbid obesity, and favorable chest anatomy. They no longer approach large (>40 % of spinal canal area) ossified TDHs thoracoscopically but use an open approach instead, which enables them to use multiple points of dissection and leverage to lift out the lesion en bloc while avoiding manipulation of the spinal cord. We do not agree with these authors. Over the past 14 years, we have surgically treated almost 400 patients for one or more symptomatic TDHs, including 349 TMDs, 32 mini-thoracotomies, 6 transaxillay approaches (T3–T4), 5 posterolateral approaches, and 1 sternotomy (T2–T3). In the early series, we chose a mini-thoracotomy in case of a giant TDH or a previous posterior approach at another institution in order to safely remove the TDH and stabilize the involved segment in a single session. In more recent years, however, we completely abandoned mini-thoracotomy in favor of TMD (n = 146 including 24 giant TDHs) and never had to convert to open surgery even in case of transdural extension. In case we need to stabilize the involved segment, we would now prefer a percutaneous posterior approach a few days later.
At present, TMD may be considered the golden standard in surgical treatment of TDHs, combining excellent results with very low complication rates and accounting for most well-documented published patient series [6, 15, 16, 35, 36]. The technique may be used for every TDH regardless of level (T4–T5 till T11–T12), laterality, size, consistency, and multiplicity, unless of course in rare cases of severe pleural adhesions and/or pulmonary disease [32]. An anterior approach is strongly recommended for central TDHs, whether or not calcified, even in the smaller ones that may significantly impinge on the spinal cord especially around the apex of the kyphotic curvature (Fig. 19.4). The safety of an anterior approach combined with the decreased tissue trauma of a thoracoscopic approach is important not only when confronted with the most challenging cases (giant central calcified TDHs) but also when counseling patients who merely suffer pain without signs of a myelopathy. Whereas the introduction of HD and 3D-HD camera systems, virtual and laboratory training of residents in endoscopic techniques are likely to increase TMD implementation, alternative transthoracic, costotransversectomy, lateral extracavitary, transpedicular, or transfacet approaches remain viable, effective procedures for surgeons experienced in these techniques who possess limited experience with thoracoscopic surgery [36].
5.2 Basic TMD Technique
5.2.1 Patient Positioning and Overall Set-Up
-
The patient is positioned on a vacuum mattress in lateral decubitus with both arms on individual supports (Fig. 19.8).
Fig. 19.8 
The patient is positioned on a vacuum mattress in lateral decubitus; the OR table bended underneath the thorax to enlarge the thoracic cage. Note careful padding of possible pressure points and an air blanket to keep the patient warm
-
A small cushion is positioned under the upper thorax to prevent pressure injury to the brachial plexus on the dependent side. Over-abduction of the arm is avoided to prevent traction injury to the brachial plexus on the surgical side [30]. The OR table is bended underneath the thorax to enlarge the thoracic cage (Fig. 19.8). This will widen individual intercostal spaces and lower the diaphragm facilitating access to the lower thoracic levels and thoracolumbar junction. At this point, the vacuum mattress is activated, avoiding pressure on the abdomen to keep the diaphragm low. Every pressure point is carefully padded with special attention to the ulnar nerve at the medial epicondyle and the common peroneal nerve at the fibular head.
-
A left- or right-sided approach is chosen depending on the exact relation disk herniation/spinal cord and the patients’ medical history (e.g., previous intrathoracic surgery). Disadvantages of a left-sided approach are the aorta, which may be in a posterior position especially in mid-thoracic segments [24], and the heart pushing the collapsed lung backward. However, with some experience, these can be easily overcome.
-
Single-lung ventilation using double-lumen tube or bronchial blocker is surprisingly well tolerated even in the elderly, provided there is no significant restrictive lung disease. An occasional O2 saturation drop due to right–left shunting may be corrected by infusing 100 % O2 in the airway of the non-ventilated lung. An experienced anesthesiologist is mandatory to manage specific problems such as anatomical variants in the bronchial tree.
-
Motor evoked potential (MEP) monitoring should be used in patients with severe spinal cord compromise.
-
We advise soft rubber trocars and pre-incision intercostal nerve blocks with long-acting local anesthetic in order to prevent intercostal nerve irritation. Three portals are placed in a triangulated fashion directed toward the pathological level (Fig. 19.9)
Fig. 19.9 
Three portals will be introduced in a triangulated fashion, directed towards the pathological level(s)
-
The viewing portal is the most posterior one and is positioned slightly anterior to the spinal column (posterior axillary line) to allow an unobstructed line of sight to the posterior intervertebral disk and compressed spinal cord using a 10 mm 30° endoscope.
-
Unlike trauma surgeons standing behind the patient and working away from the spinal cord, neurosurgeons stand in front of the patient and work toward the spinal cord. The neurosurgeon faces the thorax while the scrub nurse faces the abdomen standing next to him, both regarding the same screen (preferably an HD screen which greatly improves overall image quality and sense of depth) (Fig. 19.10).
Fig. 19.10 
Surgeon and scrub nurse stand in front of the patient
-
Another screen is needed in case another surgeon holding the scope is standing behind the patient. However, we prefer a pneumatic arm fixed to the back of the table holding the scope in any desired position (Endoboy, Geyser SA, Coudes, France) (Fig. 19.11).
Fig. 19.11 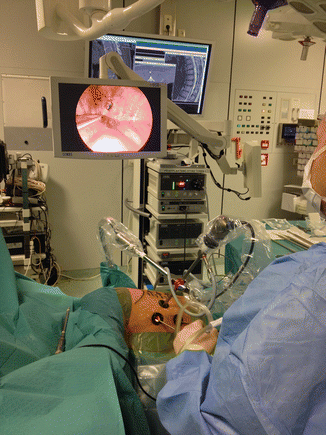
A pneumatic arm holds the scope in any desired position
-
The anesthesiologist is asked to deflate the ipsilateral lung once the patient is draped and all equipment is ready. A repeat dose of curarization may be necessary to relax the diaphragm (depending on induction and positioning times), which will greatly facilitate the approach especially below T9.
-
For lower thoracic levels, an additional portal caudal to the viewing portal (overlying the dome of the diaphragm) allows introduction of a disposable fan to retract diaphragm and/or ipsilateral lung. However, with optimal positioning and curarization, this may not be necessary for levels as low as T10–T11 or even T11–T12. Because of a variable number of ribs or an eventual lumbosacral transitional anomaly, we strongly recommend an MRI of the entire cervicothoracic spine to correctly count the symptomatic level top-down [22]. We also recommend preoperative localization of the involved level using CT myelography-guided transpleural puncture, avoiding wrong-level surgery and obviating intraoperative X-ray imaging [22].




5.2.2 Initial Surgical Approach
-
The first surgical step is to open the parietal pleura using monopolar coagulation starting at the rib head overlying the posterior intervertebral disk and adjacent vertebrae, except for T10–T11 and T11–T12 where the rib articulates below the intervertebral disk and may be spared (Video 19.1).
-
The costovertebral joint is opened underneath the rib head using monopolar coagulation and a blunt dissecting tool. The rib is then transected immediately above the head using an oscillating saw (MIASPAS TL, Aesculap, B Braun Melsungen AG, Germany) [16] or a high-speed drill (Tapered Tool, Midas Rex Legend EHS, Medtronic, MN, USA). We recommend the latter because of the superior power and control of a true high-speed drill in combination with a 5 mm diamond drill.
-
The pleura overlying the posterolateral vertebral bodies is removed using monopolar coagulation. The segmental vessels crossing at the midcorporeal level are spared; however, in case they are inadvertently damaged or deliberately obliterated while approaching a large hernia that requires more extensive bone removal, collaterals running up and down in between the neural foramina should prevent spinal cord ischemia. Nevertheless, in case of contiguous multilevel TMDs, we advise not to obliterate more than two consecutive segmental arteries.
-
The inferior pedicle is an important landmark behind the lower vertebral body, below the neuroforamen, immediately caudal to the level of the intervertebral disk. Underneath the pedicle, the surgeon will find the peridural venous plexus and lateral dura which serves as a starting point to dissect the TDH from the underlying dura.
-
The posterior part of the intervertebral disk is resected, and the adjacent vertebral bone drilled away until the disk herniation is reached, which may be strongly attached to a densely calcified intervertebral disk. An irrigation system attached to the drill emulsifies bone dust and blood, which are continuously sucked away to keep the surgical field clean. When the drill reaches the posterior vertebral cortex, a change of color is noted (dense cortical bone has an ivory aspect as opposed to spongious bone). The posterior wall is gently perforated with the drill immediately above or below the disk herniation where the dura mater may be identified. Very often, there will be some oozing from the peridural venous plexus lateral to the dura. In case of a large or giant TDH, the engorged plexus may bleed fiercely [23]. In such patients, one should not open the spinal canal widely until most of the disk herniation has been drilled away leaving only an outer shell compressing the dura mater. Aggressive venous bleeding even through a small breach in the posterior wall can be controlled by a plug of an absorbable hemostatic gelatin.
5.2.3 Resection of the TDH and Closure
-
Once the base of the disk herniation has been detached from the intervertebral disk and surrounding vertebral bone, it is merely attached to the underlying dura. At this point, the disk herniation is gently pulled into the resection cavity and resected in a piecemeal fashion using microhook and small up- and down-biting Kerrison punches. The proposed technique has the potential to significantly reduce bleeding time and blood loss. Once decompression is complete, venous oozing is controlled with gentle irrigation and a few pieces of an absorbable hemostatic gelatin applied on the dura. Alternatively, FloSeal Hemostatic Matrix (Baxter, IL, USA) may be used.
-
After copious irrigation of the pleural cavity to remove any debris, a thorax drain is inserted and the lung is re-insufflated. Suction is applied on the drain except in patients with a dural tear in which it is put on water seal to prevent a potentially lethal subarachnoid-pleural fistula [37].
Little is known about the biomechanics of thoracic diskectomy [38] let alone TMD. The thoracic spine has unique anatomical and biomechanical properties, including a natural-occurring moment arm anterior to the spine that tends to increase kyphosis whenever the anterior column is not preserved or weakened as a consequence of surgery [38]. However, bone resection restricted to the posterior half of the vertebral bodies and ipsilateral pedicle should not significantly affect stability even when multiple levels are decompressed consecutively (Fig. 19.12). Importantly, in our experience, segmental stabilization using either direct anterior fixation or second-stage posterior fixation is not necessary to cure preoperative axial pain that may result from mechanical cord compression and other factors such as local inflammation as mentioned before.

3D CT reconstruction after a three-level consecutive TMD. Segmental stabilization is not needed
5.3 Advanced TMD Technique
Multiple TDHs
Based on a single case with a compression fracture following contiguous level TMD, Wait et al. [35] advocate that contiguous level TMDs require additional fixation. Moreover, they advocate open thoracotomy instead of thoracoscopy if three or more TDHs have to be removed. We do not agree with these authors as we have performed six three-level contiguous TMDs (four T6–T9, one T7–T10, and one T8–T11) and many more two-level contiguous and noncontiguous TMDs without any problem. These are often patients with Scheuermann’s disease and multiple TDHs near the apex of an accentuated curvature. As long as these are not very large, enough bone can usually be spared in between individual levels to preserve stability (Fig. 19.12).
Giant TDHs
Hott et al. [23] defined giant TDHs as those occupying more than 40 % of the spinal canal area; however, they may be much larger, nearly fill the spinal canal, and merely leave a few millimeters of compressed spinal cord (Fig. 19.6). According to these authors, such disk herniations should not be removed thoracoscopically because leverage may occur when trying to remove the deepest part of the disk herniation once it has been completely detached from the vertebral bodies and intervertebral disk. Gently lifting the disk herniation on one side may tilt the other side toward the fragile spinal cord. In our experience, this can be avoided using a third hand (second surgeon) to stabilize the residual disk herniation with a grasping forceps while the senior surgeon continues working with suction, dissection, and resection tools. Moreover, since 2004, we have used intraoperative motor evoked potential (MEP) monitoring for every giant TDH and other TDHs with a perceived high risk (severe cord compression, severe or rapidly progressive myelopathy, etc.). An experienced anesthesiologist keeping mean arterial pressure above 80 mmHg at all times is equally important [17]. In combining MEP monitoring with meticulous technique, we have not encountered a single case of permanent neurological deterioration in over 70 high-risk procedures in the past 10 years.
In case a giant TDH has eroded the dura mater, the defect should be meticulously closed in order to prevent a potentially lethal subarachnoid-pleural fistula [23, 37]. The defect is covered with an onlay dural substitute, a layer of fibrin glue, an autologous fat graft (harvested through an existing incision and large enough to fill the vertebral defect), and another layer of fibrin glue. The thorax drain is put on water seal, and an external lumbar drain may be used to divert cerebrospinal fluid for 5 days in case of a large defect. Stabilization if needed (e.g., in case of previous posterior surgery) may be done either during the same session (anterior fixation) or during another session (posterior fixation) using one of several commercially available plating systems (e.g., MACS-TL, Aesculap, B Braun Melsungen AG, Germany) depending on surgeons’ preference and experience (Fig. 19.13).

Anterior endoscopic fixation system (MACS-TL, Aesculap, B Braun Melsungen AG, Germany) (a, b) or posterior percutaneous fixation system (c, d) in antero-posterior (a, c) and lateral (b, d) view. Either system may be applied in case of a large vertebral defect or previous (posterior) surgery
Transaxillary approach (T3–T4)
Even though the 30° endoscope may visualize the entire thoracic cage through a single trocar, the scapula blocks a direct approach to T3–T4 and above. Disk herniations at this level (six patients, 1.5 %, in our series) require a right-sided transaxillary approach because the aortic arch is in the way on the left. An endoscope and instruments are introduced through a single curved incision in the lower axilla while the arm is hanging in a 120° abduction. Large segmental veins at T3–T4 and above are another complicating factor. A rare disk herniation at T2–T3 may require a sternotomy (one patient in our series).
5.4 Postoperative Care
The patient is carefully observed overnight even though symptomatic bleeding in the resection cavity is exceedingly rare (one case in the entire series). Next morning, a chest X-ray is performed to exclude any residual pneumothorax or rarely hemothorax that may result in restrictive lung capacity if left untreated. A CT scan is scheduled before mobilization (extensive bone resection) or before discharge (any other case). An MRI scan may be scheduled 3 months postoperatively demonstrating decompression and possibly re-expansion of the spinal cord. In the first few days, pain is controlled with intravenous morphine administered through a PCA (patient-controlled analgesia) pump. Thereafter, analgesics (including nonsteroidal anti-inflammatory drugs, except in cases of additional arthrodesis) should be continued long enough to avoid severe pain exacerbations after discharge. Physiotherapy and heavy lifting are not recommended in the first 6 weeks postoperatively.
5.5 The Surgical Process in Summary
-
Take enough time to position the patient optimally, and choose your incisions wisely.
-
Open the pleura with monopolar coagulation starting at the involved rib that will lead you to the intervertebral disk.
-
Remove (part of) the head of the rib and expose the pedicle immediately below the intervertebral disk. Exposure depends on size, laterality, and consistency of the hernia.
-
Remember the position of the anterior border of the head of the rib as it roughly correlates with the position of the anterior border of the spinal canal inside.
-
Start drilling above and below the intervertebral disk approximately 1 cm anterior to the (removed) head of the rib.
-
Identify the posterior wall where the bone has an ivory color and some venous oozing invariably occurs.
-
Find the interface between hernia and dura by going around the hernia or from within (as in anterior cervical diskectomy).
-
Gently pull the hernia into the resection cavity and take it down with a small up- and down-biting Kerrison punch.
-
Giant TDHs are a different story; they are extremely challenging lesions that require additional skills, a very experienced team, and MEP monitoring support.
6 Tips and Tricks
-
Always ask for an MRI of the entire cervicothoracic spine to count the symptomatic level top-down and not to miss multiple TDHs.
-
CT (myelography)-guided localization with an intrapleural needle directly above the involved rib allows easy identification of the involved level inside the thorax. Moreover, it allows optimal positioning of the portals directly above target as the proximal end of the needle sticks out of the back at the exact craniocaudal level of the disk herniation [22].
-
CT (myelography) images are very useful during surgery because the important landmarks are bony (head of the rib, pedicle, posterior vertebral wall, etc.).
-
The OR table should be bended to open up the ipsilateral rib cage allowing a smoother approach in between the ribs. This will also significantly lower the diaphragm allowing an easier access to the thoracolumbar junction.
-
Familiarize yourself with the relevant anatomy (including cadaver work), and keep in mind those landmarks!
-
Always use an HD camera system.
-
Ask your anesthesiologist for a repeat dose of curarization (especially when operating below T8–T9) as soon as you enter the thorax, as the diaphragm is the first muscle to wake up especially after a relatively long start-up phase.
-
Try to stay away lateral to the dura avoiding the peridural venous plexus, and look for the interface between dura and hernia more anteriorly.
-
Use irrigation and gentle tamponade to control venous oozing that will improve as soon as the dura is adequately decompressed.
-
Make sure not to overlook (part of) the hernia that may be hidden behind a dural fold or the posterior longitudinal ligament that should always be removed.
7 Summary
7.1 Clinical and Radiological Characteristics
-
The true incidence of symptomatic TDHs is underestimated because of their variable and often misleading clinical presentation [5, 12].
-
TDHs may be present long before they produce symptoms. When they do, it is gradual and without precipitating or traumatic event in the majority of cases [1, 3, 5, 17, 22].
-
Diagnosis is often difficult because of protean, nonspecific presenting symptoms that may be a combination of pain and myelopathy [6, 8, 12, 14].
-
Upper TDHs may produce precordial pain, epigastric pain, shoulder pain, and a non-radicular, predominantly proximal brachial pain [14].
-
Lower TDHs and especially those at T11–T12 are often accompanied by a 360° stenosis and may present with predominantly lower motor neuron symptoms, a condition termed compressive lumbar myelopathy [10].
-
TDHs are often observed in association with Scheuermann’s disease and as such may be related to a growth disorder of the thoracic spine [5, 12].
-
Cord compression not only depends on the dimensions of the disk herniation but also on its relation to the anterior cord surface and kyphotic curvature. As such, small TDHs may severely compress the spinal cord especially near the apex of kyphosis.
-
Besides mechanical compression, TDH pathophysiology likely involves ischemia, localized inflammation, and occasionally a traumatic event acting as a catalyzator [19–21].
-
CT myelography may still be considered the golden standard for TDH imaging, while MR imaging is complementary and strongly recommended to exclude multilevel disease [22].
7.2 Surgical Strategy
-
TDHs are rarely, if ever, a true surgical emergency. They should be removed at a convenient time by an experienced team. There is simply no excuse for a suboptimal setting [17].
-
Decompressive laminectomy has been completely abandoned and is considered obsolete [25–30].
-
Large, medial, and/or calcified TDHs should be operated through an anterior approach with very rare exceptions (severe pulmonary disease, clearly lateralized TDH, and contralateral spinal cord that does not extend posterior to the disk herniation). Small, lateral, noncalcified TDHs may be treated through a posterior or posterolateral approach [33]; however, those familiar with an anterior (thoracoscopic) approach including myself would definitely favor a TMD even in such cases.
-
Although many alternative anterior, lateral, posterolateral, and even posterior approaches have been proposed in recent years [3, 23, 26, 28, 33, 34], none of them has been as widely adopted as the TMD technique. Despite a steep learning curve, TMD may be considered the golden standard in TDH surgery, combining excellent results with very low complication rates [6, 15–17, 35, 36].
-
TMD is well tolerated even in the elderly and may be used for any TDH regardless of level (T4–T5 till T11–T12 or even T12–L1), laterality, size, and consistency. Multiple levels may be decompressed in a single session.
-
The Adamkiewicz artery should not be a problem even in a left-sided approach to the lower thoracic spine as collaterals running up and down at foraminal level should be able to take over supply to the Adamkiewicz artery in case the direct segmental supply (artery running at midcorporeal level) is interrupted.
-
TMD performed by a very experienced team with MEP monitoring support can be safely applied to giant calcified TDHs as well (personal experience), even though some authors reported to have abandoned thoracoscopy in such cases [23]
-
Segmental stabilization is not necessary to cure preoperative axial/segmental pain and can be avoided in the vast majority of patients including those with very large or multiple TDHs (personal experience).
-
Since no well-conducted RCTs comparing various surgical approaches to treat TDH are available, only the above guidelines can be given, but no high level of evidence exists about the superiority of one technique above another.
References
Awwad EE, Martin DS, Smith KR Jr, Baker BK (1991) Asymptomatic versus symptomatic herniated thoracic discs: their frequency and characteristics as detected by computed tomography after myelography. Neurosurgery 28:180–186
McInerney J, Ball PA (2000) The pathophysiology of thoracic disc disease. Neurosurg Focus 9:e1
Uribe JS, Smith WD, Pimenta L, Hartl R, Dakwar E, Modhia UM, Pollock GA, Nagineni V, Smith R, Christian G, Oliveira L, Marchi L, Deviren V (2012) Minimally invasive lateral approach for symptomatic thoracic disc herniation: initial multicenter clinical experience. J Neurosurg Spine 16:264–279
Love JG, Kiefer EJ (1950) Root pain and paraplegia due to protrusions of thoracic intervertebral disks. J Neurosurg 7:62–69, illust
Wood KB, Garvey TA, Gundry C, Heithoff KB (1995) Magnetic resonance imaging of the thoracic spine. Evaluation of asymptomatic individuals. J Bone Joint Surg Am 77:1631–1638
Anand N, Regan JJ (2002) Video-assisted thoracoscopic surgery for thoracic disc disease: classification and outcome study of 100 consecutive cases with a 2-year minimum follow-up period. Spine (Phila Pa 1976) 27:871–879
Arseni C, Nash F (1960) Thoracic intervertebral disc protrusion: a clinical study. J Neurosurg 17:418–430
Benson MK, Byrnes DP (1975) The clinical syndromes and surgical treatment of thoracic intervertebral disc prolapse. J Bone Joint Surg Br 57:471–477
Eleraky MA, Apostolides PJ, Dickman CA, Sonntag VK (1998) Herniated thoracic discs mimic cardiac disease: three case reports. Acta Neurochir 140:643–646
Kleopa KA, Zamba-Papanicolaou E, Kyriakides T (2003) Compressive lumbar myelopathy presenting as segmental motor neuron disease. Muscle Nerve 28:69–73
Lyu RK, Chang HS, Tang LM, Chen ST (1999) Thoracic disc herniation mimicking acute lumbar disc disease. Spine (Phila Pa 1976) 24:416–418
Overvliet GM, Beuls EA, Ter Laak-Poort M, Cornips EM (2009) Two brothers with a symptomatic thoracic disc herniation at T11–T12: clinical report. Acta Neurochir 151:393–396
Tokuhashi Y, Matsuzaki H, Uematsu Y, Oda H (2001) Symptoms of thoracolumbar junction disc herniation. Spine (Phila Pa 1976) 26:E512–E518
Wilke A, Wolf U, Lageard P, Griss P (2000) Thoracic disc herniation: a diagnostic challenge. Man Ther 5:181–184
Regan JJ, Mack MJ, Picetti GD 3rd (1995) A technical report on video-assisted thoracoscopy in thoracic spinal surgery. Preliminary description. Spine (Phila Pa 1976) 20:831–837
Rosenthal D, Rosenthal R, de Simone A (1994) Removal of a protruded thoracic disc using microsurgical endoscopy. A new technique. Spine (Phila Pa 1976) 19:1087–1091
Cornips EM, Janssen ML, Beuls EA (2011) Thoracic disc herniation and acute myelopathy: clinical presentation, neuroimaging findings, surgical considerations, and outcome. J Neurosurg Spine 14:520–528
Wood KB, Blair JM, Aepple DM, Schendel MJ, Garvey TA, Gundry CR, Heithoff KB (1997) The natural history of asymptomatic thoracic disc herniations. Spine (Phila Pa 1976) 22:525–529, discussion 529–530
Roger EP, Chamczuk AJ, Hagan MC (2013) Thoracic venous congestion caused by thoracic disc herniation. Brain Behav 3:207–210
Reynolds JM, Belvadi YS, Kane AG, Poulopoulos M (2014) Thoracic disc herniation leads to anterior spinal artery syndrome demonstrated by diffusion-weighted magnetic resonance imaging (DWI): a case report and literature review. Spine J 14:e17–e22
Cornips EM (2014) Crippling upper back pain after whiplash and other motor vehicle collisions caused by thoracic disc herniations: report of 10 cases. Spine (Phila Pa 1976) 39:988–995
Cornips E, Beuls E, Geskes G, Janssens M, van Aalst J, Hofman P (2007) Preoperative localization of herniated thoracic discs using myelo-CT guided transpleural puncture: technical note. Childs Nerv Syst: ChNS: Off J Int Soc Pediatr Neurosurg 23:21–26
Hott JS, Feiz-Erfan I, Kenny K, Dickman CA (2005) Surgical management of giant herniated thoracic discs: analysis of 20 cases. J Neurosurg Spine 3:191–197
Huitema GC, Cornips EM, Castelijns MH, van Ooij A, van Santbrink H, van Rhijn LW (2007) The position of the aorta relative to the spine: is it mobile or not? Spine (Phila Pa 1976) 32:1259–1264
Perot PL Jr, Munro DD (1969) Transthoracic removal of midline thoracic disc protrusions causing spinal cord compression. J Neurosurg 31:452–458
Bransford R, Zhang F, Bellabarba C, Konodi M, Chapman JR (2010) Early experience treating thoracic disc herniations using a modified transfacet pediclesparing decompression and fusion. J Neurosurg Spine 12:221–231
Hulme A (1960) The surgical approach to thoracic intervertebral disc protrusions. J Neurol Neurosurg Psychiatry 23:133–137
Khoo LT, Smith ZA, Asgarzadie F, Barlas Y, Armin SS, Tashjian V, Zarate B (2011) Minimally invasive extracavitary approach for thoracic discectomy and interbody fusion: 1-year clinical and radiographic outcomes in 13 patients compared with a cohort of traditional anterior transthoracic approaches. J Neurosurg Spine 14:250–260
Le Roux PD, Haglund MM, Harris AB (1993) Thoracic disc disease: experience with the transpedicular approach in twenty consecutive patients. Neurosurgery 33:58–66
Stillerman CB, Chen TC, Day JD, Couldwell WT, Weiss MH (1995) The transfacet pedicle-sparing approach for thoracic disc removal: cadaveric morphometric analysis and preliminary clinical experience. J Neurosurg 83:971–976
Stillerman CB, Chen TC, Couldwell WT, Zhang W, Weiss MH (1998) Experience in the surgical management of 82 symptomatic herniated thoracic discs and review of the literature. J Neurosurg 88:623–633
Perez-Cruet MJ, Fessler RG, Perin NI (2002) Review: complications of minimally invasive spinal surgery. Neurosurgery 51:S26–S36
Arts MP, Bartels RH (2014) Anterior or posterior approach of thoracic disc herniation? A comparative cohort of mini-transthoracic versus transpedicular discectomies. Spine J 14:1654–1662
Bartels RH, Peul WC (2007) Mini-thoracotomy or thoracoscopic treatment for medially located thoracic herniated disc? Spine (Phila Pa 1976) 32:E581–E584
Wait SD, Fox DJ Jr, Kenny KJ, Dickman CA (2012) Thoracoscopic resection of symptomatic herniated thoracic discs: clinical results in 121 patients. Spine (Phila Pa 1976) 37:35–40
Oskouian RJ, Johnson JP (2005) Endoscopic thoracic microdiscectomy. J Neurosurg Spine 3:459–464
Cornips EM, Staals J, Stavast A, Rijkers K, van Oostenbrugge RJ (2007) Fatal cerebral and cerebellar hemorrhagic infarction after thoracoscopic microdiscectomy. Case report. J Neurosurg Spine 6:276–279
Wakefield AE, Steinmetz MP, Benzel EC (2001) Biomechanics of thoracic discectomy. Neurosurg Focus 11:E6
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
1 Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Video 19.1
The video illustrates a right-sided thoracoscopic microdiscectomy at T6–T7 removing a noncalcified herniation in a thin, female patient (MP4 617783 kb)
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Cornips, E.M.J. (2016). Endoscopic Resection of Thoracic Disk Herniations. In: van de Kelft, E. (eds) Surgery of the Spine and Spinal Cord. Springer, Cham. https://doi.org/10.1007/978-3-319-27613-7_19
Download citation
DOI: https://doi.org/10.1007/978-3-319-27613-7_19
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-27611-3
Online ISBN: 978-3-319-27613-7
eBook Packages: MedicineMedicine (R0)