
Abstract
This chapter focuses on the preoperative coagulation assessment of patients undergoing cranial and spinal neurosurgery. Although it has been common, even standard, practice to obtain preoperative laboratory assessment of the platelet count, prothrombin time (PT)/international standardized ratio (INR), and activated partial thromboplastin time (aPTT) in adult patients in preoperative neurosurgical settings, the value of this practice has been questioned and the published evidence on this topic suggests that the routine use of these studies neither reliably identifies patients who will suffer surgical bleeding complications nor safely excludes those who will not. As a result, a variety of alternative laboratory assessments like bleeding time (BT), and platelet function tests such as the PFA-100 have sparked interest. Similarly, clinical assessment tools to formalize preoperative history taking with respect to coagulation issues have also been developed and continue to be refined. However, as of this writing none have clearly demonstrated a high sensitivity and specificity for the outcomes of interest. Nevertheless, understanding the various available laboratory tests and clinical assessment tools provides the basis for informed decision making with respect to patient care in this area.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Positive Predictive Value
- International Normalize Ratio
- Prothrombin Time
- Tuberous Sclerosis
- National Surgical Quality Improvement Program
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
This chapter focuses on the preoperative coagulation assessment of patients undergoing cranial and spinal neurosurgery. Although it has been common, even standard, practice to obtain preoperative laboratory assessment of the platelet count, prothrombin time (PT)/international standardized ratio (INR), and activated partial thromboplastin time (aPTT) in adult patients in preoperative neurosurgical settings, the value of this practice has been questioned and the published evidence on this topic suggests that the routine use of these studies neither reliably identifies patients who will suffer surgical bleeding complications nor safely excludes those who will not. As a result, a variety of alternative laboratory assessments like bleeding time (BT), and platelet function tests such as the PFA-100 have sparked interest. Similarly, clinical assessment tools to formalize preoperative history taking with respect to coagulation issues have also been developed and continue to be refined. However, as of this writing none have clearly demonstrated a high sensitivity and specificity for the outcomes of interest. Nevertheless, understanding the various available laboratory tests and clinical assessment tools provides the basis for informed decision making with respect to patient care in this area.
The Coagulation Cascade
The standard teaching of the coagulation cascade as divided into an extrinsic, intrinsic, and common pathway has been of value in understanding how particular coagulation assays work in the laboratory. However understanding in vivo coagulation requires a blurring of these two pathways. Davies et al. and Macfarland described the “waterfall” sequence of enzymes that are sequentially activated following exposure to a triggering bleeding event [1, 2]. Exposure of blood to glass in a laboratory resulted in activation of the intrinsic (contact-activated) enzyme cascade including factors XII, XI, IX, and VIII. Exposure of blood to calcium, phospholipid, and tissue factor resulted in activation of the extrinsic (tissue factor) pathway, including primarily factor VII. The products of either pathway lead to the activation of factor X which cleaves prothrombin to thrombin (IIa) which in turn converts fibrinogen to the fibrin that forms the actual clot. Fibrin is further acted upon by Factor XIII to cross-link the fibrin clot [3] (Fig. 21.1—Intrinsic, Extrinsic, and Common pathways). In vivo, the extrinsic, tissue factor pathway is the more important primary mechanism, while the intrinsic pathway performs a secondary role in the normal state. The current, cell-based model of blood clotting blurs the lines between these two separate pathways, focusing instead on phases of the coagulation process, namely initiation, amplification, propagation, stabilization, and finally attenuation. Blood clotting begins with the exposure of subendothelial von Willebrand’s Factor (vWF) and collagen, resulting in platelet adhesion. Adhered platelets subsequently undergo degranulation to become activated and release several coagulation cascade proteins (V, VIII) and stimulate production of thromboxane A2 (TxA2). TxA2 with ADP helps aggregate additional platelets to form the platelet plug. Coincident with the platelet process and interconnected with it, the initiation phase of coagulation begins with the exposure of circulating factor VII to tissue factor (TF) in the subendothelium forming an activated FVIIa-TF complex. This cleaves/activates Factor X to Xa, which generates thrombin (IIa) by a similar cleavage. However, this initial phase creates only a modest amount of thrombin. To form a robust clot, a second “amplification” stage is needed, in which thrombin from the initiation stage binds to platelets, promoting the release and activation of factors VIII and V from platelet granules. Subsequently, in the propagation phase, these factors significantly enhance the conversion of Factor X to Xa (tenase complex, on the surface of activated platelets, using FIXa, FVIIIa) and prothrombin to thrombin (prothrombinase complex, on the surface of activated platelets, using FXa, Va) in the propagation stage. Finally, the forming clot is stabilized as thrombin catalyzes factor XIII to XIIIa, which, as noted above, cross-links the Fibrin [3–6]. A fourth “attenuation” phase is often also included to describe the regulatory components that prevent excessive thrombosis (Fig. 21.2: Coagulation cascade—cell-based model).

Coagulation cascade , fibrinolytic and pathway inhibitors such as Protein C, S, Antithrombin III omitted for simplicity

Preoperative Screening Guidelines
No formal guidelines on preoperative coagulation testing specific to neurosurgery patients exist. General guidelines relating to surgical patients have however appeared from a number of mostly European medical societies. The British Committee for Standards in Haematology published guidelines in 2008. The primary recommendation were as follows: one, routine use of presurgical laboratory screening in unselected patients was not recommended; two, a personal and family bleeding history and identification of consumed antithrombotic medications should be performed in all patients; three, in the face of a negative bleeding history no further laboratory studies are necessary; four, a positive history or observed clinically concerning condition such as liver failure necessitates a comprehensive assessment [7]. The evidentiary basis for these recommendations was limited by the rarity of high-quality prospective studies, such that these recommendations were all grade B or C recommendations, supported by level III or IV evidence. Conversely, the Italian Society for Hemostasis and Thrombosis recommended that aPTT, PT, and platelet count should be obtained in both adult and pediatric patients even in the face of a negative bleeding history. The evidence at the time of publication (2009) was essentially the same for both groups, but the Italian society specifically noted that they viewed the potential for failing to identify an avoidable bleeding complication as paramount and the cost of testing as less important [8]. The possible adverse medical consequences of falsely positive screening studies were not addressed directly. French and German Anesthetic societies published recent guidelines similar to the British guidelines [9, 10]. Specific to children, the Italian Society of Pediatric and Neonatal Anesthesia and Intensive Care recommended that children undergo a standardized questionnaire assessment and that coagulation tests be reserved for positive history or in cases with a specifically high risk of bleeding [11]. The American Society of Anesthesiologists advises that preoperative tests not be ordered routinely, but should be selectively used when clinical characteristics suggest a bleeding disorder, renal dysfunction, or liver dysfunction and “depending on the type and invasiveness of the procedure” [12].
The utility of preoperative screening depends in part on the frequency or prevalence of abnormalities. Considering the general presurgical patient, the incidence of laboratory abnormality on unselected patients ranges from 0.5 % to 16 % vs. up to 40 % where patients were selected for study on the basis of clinical history [9]. In the pediatric population, the incidence of congenital bleeding disorders is low. For example, Von Willebrand disease is the most frequent congenital bleeding abnormality with a prevalence of approximately 1:500; however only 1 in 10 to 1 in 20 of these patients are symptomatic. Hemophilia A (Factor VIII deficiency) and hemophilia B (Factor IX deficiency) occur at rates of 1 in 5000 and 1 in 25,000 male children respectively, reducing the practicality of preoperative testing [13]. As a consequence, the positive predictive values of abnormal coagulation studies (the % of patient with a positive test who actually have a bleeding disorder) in the general preoperative setting are low, ranging from a high of 22 %, to more commonly <10 % in nine studies identified in one guideline review [7].
When initial tests are abnormal, often, testing conditions rather than patient pathology are to blame. One study looking at pediatric patients undergoing routine testing prior to tonsillectomy noted that 0.1 % of 1600 patients had abnormal PT, PTT, or BT on initial screening, but in half of these repeat testing was normal [14].
Despite the aforementioned guidelines, preoperative hemostatic testing remains a common practice. It has been argued that laboratory studies could play an important role when preoperative history taking is inadequate either based on limitations of the provider to ask or the patient to provide the necessary information. Pediatric patients, particularly young pediatric patients , may not have had sufficient life exposure to hemorrhage inducing events. Or patients may recently have acquired a bleeding diathesis, as in the case of acquired von Willebrand disease in aortic valve stenosis [15].
Individual Hematologic Tests
Platelet Count
The platelet count measures the quantity of platelets in a cubic mm of whole blood. The normal range is 150,000–400,000/mm3. The test cannot assess platelet function. Neurosurgical procedural thresholds for platelets have typically been 100,000/mm 3 [16]. Because heparin use is extremely common in neurosurgical patients, repeat assessment of platelet count for patient on heparin therapy is important in detecting heparin-induced thrombocytopenia (HIT), with the absolute value of the count less important than the relative change [17]. Falsely thrombocytopenic values can occur with platelet clumping. Thrombocytopenia can be caused by processes that reduce platelet production, such myelodysplastic processes and their treatments, viral infections, splenic enlargement with trapping platelets, such as may occur in infectious mononucleosis, and platelet consumption as occurs in sepsis, thrombocytic thrombocytopenic purpura (TTP), and autoimmune processes such as HIT.
Platelet Function Assays
Platelet function assays attempt to recreate platelet aggregation in vitro. The PFA-100 is one common example of this type of testing. Whole blood is tested for the rate at which it occludes an aperture in a testing membrane coated with either epinephrine or adenosine diphosphate. Normal closing times are <120 s. The study is frequently used to assess the impact of aspirin on platelet function, to which it is quite sensitive [18]. It has also been used to assess for von Willebrand disease. A recent meta-analysis suggests it performs well as a screening tool for this disorder in the setting of a specialty pediatric hematology clinic [13]. The test is, however, also sensitive to anemia, thrombocytopenia, and other pharmacological agents affecting platelet function.
The PFA-100 is not useful for assessing the degree of platelet inhibition from alternative agents such as clopidogrel. Clopidogrel is a commonly used antiplatelet thienopyridine that functions by blocking the P2Y12 receptor for ADP on the platelet surface. This blocks both platelet activation and limits the participation of platelets in fibrin cross-linking [19]. The extent to which P2Y12 inhibitors successfully block platelet activity is variable and the concept of Clopidogrel resistance or nonresponsiveness has been aggressively pursued in the cardiovascular medicine. Because agents like Clopidogrel also have an important role in neuroendovascular procedures, preoperative assessments of the extent of P2Y12 inhibition are becoming more common. The P2Y12 platelet function test, known commercially by names like Verify Now P2Y12, measures the effect of clopidogrel on platelet function by comparing the degree of aggregation caused by attempting to stimulate the P2y12 receptor pathway with adenosine diphosphate/prostacyclin E1 and comparing this to the degree of platelet aggregation caused by stimulation of the thrombin receptor activating peptide (TARP), which bypasses the P2Y12 pathway and serves as a baseline for comparison. Results are reported in both arbitrary units related to the change in optical properties of the specimen or as a ratio, or percentage of inhibition comparing the two parts of the assay. Whether using a thrombin-based platelet activation test as a baseline value is accurate is debated, and on/off clopidogrel testing may be more accurate [20].
The screen filtration pressure method (SFP) of platelet aggregation assessment is another alternative procedure in common use. This method assesses the changes in back pressure as blood is forced through a screen with openings 20–40 μm square [21]. To assess platelet aggregation, whole blood is mixed with ADP.
aPTT
The activated partial thromboplastin time (aPTT) tests the “contact” or intrinsic clotting pathway factors including factors XII, XI, and IX and to a lesser extent common pathway factors X, V, II, and fibrinogen. The patient’s serum is mixed with phospholipid (which lacks tissue factor, hence the partial thromboplastin time), and calcium against a contact surface such as silica or kaolin [7]. The formation of a clot is tracked usually by light transmission and the time measured in seconds. Normal values are between 20 and 35 s. Importantly, the aPTT does not assess factor VII, which is part of the extrinsic pathway [5]. As a clinical tool, it screens for factor deficiencies of >50 % in VII, IX, and XI [9]. Importantly aPTT is sensitive to inhibition of thrombin, and hence is used to monitor therapy with unfractionated heparin, but is relatively insensitive to alterations in Factor Xa levels and so insensitive to the effects of Xa inhibitors (see below). The aPTT will be prolonged in the presence of other inhibitors such as the lupus anticoagulant and fibrin split products, such as is seen in disseminated intravascular coagulation.
PT/INR
The prothrombin time measures the primary tissue factor-driven or extrinsic coagulation pathway. Thus it assesses factor VII and the common factors of II, V, X and Fibrinogen. Citrated plasma, calcium, and tissue thromboplastin (containing tissue factor) are combined and clot formation typically measured optically. Normal values are typically 10–15 s. The PT is prolonged in Vitamin K deficiency, Factor VII deficiencies, and, of course, warfarin therapy, for which the INR is usually followed [5, 7].
The International Normalized Ratio (INR) was introduced to standardize the PT time, given that there was some variability in the thromboplastin reagents used in the reaction. The INR = (Patient PT/mean normal PT)ISI. ISI is a value assigned to the specific reagents used. Normal values are 0.9–1.2 [22]. However, increases in reagent sensitivity mean that higher concentrations of factor VII are typically present at higher INR values than was previously the case. Matevosyan and colleague noted that in 25 neurosurgery patients with INR 1.3–1.7, the plasma concentrations of the important factors II, VII, and VII were all above generally accepted surgical thresholds and argued against correcting for INR values at these levels [23].
The level at which an elevated prothrombin time (PT) should be considered clinically relevant in neurosurgical patients has been debated. INR values were developed to assess patients taking Vitamin K antagonists, specifically Coumadin. It is common practice to see preoperative treatment initiated for INR > 1.3. West and colleagues surveyed the literature and concluded that patients with INR 1.5 or less, in the absence of clinical bleeding, should not be treated for this with FFP preoperatively [24].
Bleeding Time (BT)
Bleeding time should be the ideal tool for assessing the likelihood of excessive surgical bleeding, since it would appear to assess all aspects of the clotting process, recreating surgical tissue trauma in a controlled fashion. It is generally considered to be an assay of platelet function more than other aspects of the clotting pathway, and is used in assessing von Willebrand disease (vWD), as well as other disorders of platelet-vessel wall interactions. However, practically, the bleeding time has not been shown to correlate with clinically important surgical hemorrhage outcomes and is not widely used [25]. The test is conducted by making a standardized small laceration to the forearm while a blood pressure cuff is inflated on the upper arm to 40 mmHg. Normal range is usually <10 min [5].
Thrombin Time (TT)
Thrombin time measures the rate of clot formation, typically measured by changes in light transmission. Thrombin is added to patient plasma. Time to clot formation is typically 10–20 s. As noted below, this test can be important in assessing whether a patient has activity from a direct thrombin inhibitor such as dabigatran. Other factors raising the TT include fibrin split products, heparin, and quantitative or qualitative fibrinogen loss [5].
Fibrinogen
Fibrinogen as the final factor in the clotting cascade can be directly measured. Levels less than 150 mg/dL are abnormal. In preoperative settings, causative factors include liver impairment and malnutrition, as well as inherited factor deficiency. Consumption of factor such as in DIC and surgical or traumatic blood loss and transfusion therapy can also lead to low levels.
ACT
The activated clotting time (ACT) is primarily used as a rapid assessment tool for measuring the degree of anticoagulation achieved by unfractionated heparin for bypass and angiographic procedures. Both the pre- and post-heparinization values are needed. The normal range is from 80 to 160 s. The test measures the function of the intrinsic coagulation pathway and has many similarities with aPTT testing; however it not sensitive to low levels of anticoagulation and is not a typical preoperative lab test.
Other Assays
Anti-Xa levels are measured to assess the effect of direct Xa inhibitors including enoxaparin. Fibrin split products (FSP) or fibrin degradation products are measured to evaluate for excessive fibrinolysis such as seen in disseminated intravascular coagulation. Reptilase is a snake enzyme that functions like thrombin but is not sensitive to inactivation by antithrombin III, the enzyme heparin promotes to achieve its anticoagulant effects. In the heparinized patient, Reptilase times (RT) will still be normal, while patient with factors that interfere with fibrin polymerization, like FSP, will show elevated RTs.
Viscoelastic Measures of Coagulation
Viscoelastic measures of coagulation assess the physical properties of a developing clot as it arises out of whole blood. The appeal is that this assesses the interaction between platelets and clotting cascade, and by following clot formation over time, can assess the various stages of the clotting process noted above. The test measures the changing physical properties of the blood sample over time as it is rotated, while a clot forms. Four values are produced by the test: the R value indicated the time to first clot formation, akin to the initiation phase; the K value represents the time to a set clot expansion, and is focused on clot amplification; the MA value measures the strength of the clot, assessing the stabilization phase; and the Coagulation Index (CI) is a calculated summary measure [26]. Neurosurgical experience with this modality is limited and not conclusive and includes trauma, endovascular procedures, and stroke care [27–29].
The impact of a variety of clinical conditions on common preoperative laboratory tests is given in Table 21.1.
Effect of Newer Anticoagulation Agents on Coagulation Tests
While older antiplatelet and anticoagulant agents such as heparin, coumadin, and clopidogrel are familiar to neurosurgeons, a variety of “single target” or newer oral anticoagulants and antiplatelet agents have come into widespread use. These include direct thrombin inhibitors such as dabigatran, and factor Xa inhibitors including rivaroxaban and apixaban. Unlike Warfarin, which can be properly monitored by PT/INR, single-target agents cannot reliably be followed in a similar fashion. A normal INR does not exclude treatment effect with Dabigatran, for example [30]. Dabigatran effect should elevate aPTT and will certainly elevate Thrombin Time (TT) [19]. Rivaroxaban, as a Factor Xa inhibitor, will show an increase in PT, but not always at the dosing trough, when anticoagulant activity will still be present. Similarly, aPTT is not sensitive to low drug concentrations [19]. Apixaban effect is not assessed by either PT or aPTT. Anti-Xa levels should be informative in these later two agents, given their mechanism, but published experience is limited [31]. At least one paper has assessed TEG in the management of a subdural hematoma in a patient on Dabigatran whose TT was prolonged [32].
Structured Clinical History
As noted above for general presurgical guidelines, and below for specific studies in neurosurgical patients, the predictive values of preoperative laboratory tests for adverse bleeding outcomes are limited. Assessment of bleeding risk by clinical history of both the patient and family, by contrast, is generally recommended in published guidelines [7–10, 12, 33]. However, clinical studies assessing the accuracy of clinical history to predict operative bleeding show variable predictive values. Houry et al. evaluated 3242 general surgical patients with a 3.2 % underlying prevalence rate of hematoma formation. Using a standardized, but nonvalidated questionnaire 951 (28 %) reported affirmative answers. Of these, 38 (PPV = 4 %) developed postoperative hematoma. The negative predictive value (NPV) of the screen was 97 %; thus 2.8 % with a negative screen still had bleeding complications, not much lower than the underlying prevalence. Laboratory assessments of bleeding risk did not perform better [34]. Gabriel et al. studied 1479 children undergoing tonsillectomy. Again, using a previously described but nonvalidated instrument, 13 (1 %) reported an abnormal bleeding history. Three of these had excessive intraoperative or postoperative bleeding as assessed by surgeon (PPV = 23 %). Of 1466 patients with a negative bleeding screen, 148 had bleeding complication, giving a negative predictive value (NPV) of 90 %, but meaning that 10 % of those with a negative bleeding screen still experienced increased bleeding. Again, laboratory assessment did not more accurately predict bleeding risk [35].
Validated questionnaires do exist for von Willebrand disease, and in particular, the Pediatric Bleeding Questionnaire has been assessed in a number of publications [36]. The questionnaire focuses on epistaxis, cutaneous bruising, bleeding from minor wounds, oral cavity bleeding, including dental extraction, gastrointestinal bleeding, prior surgical bleeding, menorrhea, and postpartum hemorrhage, where applicable, muscle hematomas and hemarthrosis. The full questionnaire can be found at the World Federation of Hemophilia web site at http://www.wfh.org/en/resources/bleeding-assessment-tool-pediatric-bleeding, as of this writing. However, this tool has been validated only in the setting of specialized coagulation clinics for the detection of Von Willebrand disease, and not in the general adult or pediatric operative population and not in neurosurgery patients specifically [13, 36]. Absent a validated instrument for the preoperative setting, suggestions for specific history questions are identified in Table 21.2 [9, 37]. A partial list of medications that can raise the risk of bleeding complications is given in Table 21.3, as an aid to history taking.
Neurosurgery-Specific Studies
A modest body of literature deals specifically with preoperative testing in neurosurgery patients. Schramm et al. reported on 1211 patients undergoing cranial (56 %), spinal (33 %), and other (11 %) neurosurgical procedures. Three quarters of patients underwent preoperative coagulation testing and 7.2 % of these had either low platelet count, or prolonged PT or aPTT. Postoperative bleeding was predicted by preoperative elevated aPTT, but not PT or platelet count, and most of 14 patients with both elevated aPTT and postoperative bleeding had an identifiable risk factor on clinical history [38]. Dutzmann and colleagues sought to evaluate whether preoperative assessment of prothrombin time (PT) was essential in routinely planned neurosurgical procedures [39]. They studied 4310 consecutive patients undergoing elective cranial and spinal procedures. Considering a PT of >1.28 as abnormal, 1.8 % (78 patients) were found to have an abnormally elevated PT preoperatively, but all but five of these had obvious causes for the PT elevation such as coumadin use or liver disease. Thus the sensitivity of history for elevated PT was 93.5 %. Of the five with unexpectedly elevated PTs, two were given replacement factor, three were not, and none had hemorrhagic complications. Among the >4000 patient cohort, 33 patients (0.77 %) suffered a bleeding complication requiring reoperation and 31 patients of these had a normal pre-op PT. Of the two patients who had abnormal PTs and suffered bleeding complications, both had concerning histories (cancer, recent Warfarin use, and hepatocellular carcinoma). The authors noted a positive predictive value (PPV) of preoperative elevated PT to indicate hemorrhage was 2.5 % (2/78), although this rate appears to discount that many or most patients in this study who had preoperatively elevated PTs were treated with factor replacement [39].
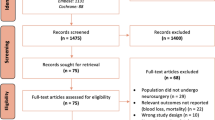
The largest analysis of preoperative coagulation testing in neurosurgery , by number of patients included, also assessed the relative utility of preoperative history for bleeding risk vs. preoperative coagulation studies using the National Surgical Quality Improvement Program database (NSQIP) . Patients were considered to have a positive history for bleeding history based on self-reported medical history of bleeding disorders, high-risk medication use, chronic steroid use, disseminated cancer, and renal or liver disease. The study included 11,804 patients. Sixty percent of patients underwent PT and aPTT testing and 90 % had preoperative platelet count. While 4 % had at least one abnormal result, less than 1 % had a severely abnormal result. Given the large sample size, it is unsurprising that each of the abnormal laboratory values was statistically associated with a variety of outcome measures including mortality, transfusion, and return to the OR. However, all coagulation measures had low sensitivity (<0.2) for the outcome measures. A positive clinical history was associated with a 3.5-fold increasing the likelihood of one or more abnormal coagulation tests, and the likelihood of detecting the various clinical outcomes was similar with history vs. one or more abnormal coagulation tests. Concerningly, even when history and abnormal laboratory assessment were combined, only about 1/3 of patients with the outcomes of interest were identified. The authors concluded that there was “limited or absent benefit from routine or standing preoperative hemostatic screening .” They further estimated that limiting testing to those with an abnormal history would save $82 million annually in the United States (2012 dollars) [40].
As noted above, Factor XIII plays an important role in the stabilization phase of clot formation, being essential for cross-linking of the fibrin to create a stable polymer. Gerlach and colleagues assessed Factor XIII levels preoperatively in 910 patients undergoing cranial neurosurgery in addition to PT, aPTT, and fibrinogen. In 4.3 % there was a postoperative hemorrhage requiring surgical intervention. Preoperative Factor XIII and Fibrinogen levels were correlated with hemorrhage, whereas PT and aPTT were not. Specifically, patients with Factor XIII levels less than 80 % had a fourfold increase in risk of hematoma [41]. However these study results have not been reproduced [42]. Additionally, Adelman et al. studied 290 patients undergoing craniotomy with a 2.4 % rate of severe bleeding requiring reoperation. No differences in preoperative Factor XIII were seen between the groups, nor were differences in PT, PTT, or platelet count. A fibrinogen level of <200 mg/dl was associated with a tenfold increase in the odds of postoperative hemorrhage, and had a sensitivity of 86 % and specificity of 62 % [43].
Evaluating pediatric patients undergoing craniofacial reconstruction , Genecov et al. retrospectively assessed 168 patients. All had a normal PT, but 6 (3.6 %) had an abnormal PTT and were found to have Factor XI deficiencies (3pts), von Willebrand+low FXII (1 patient), and circulating inhibitors (2 patients) [44].
Karger and colleagues assessed the role of Platelet Function Analysis , specifically the PFA-100, in 93 patients undergoing craniotomy for mass lesion. Patients with abnormally elevated closure times were administered DDAVP. Surgical outcomes were compared to a retrospective cohort and were found to be similar with no reduction in bleeding events in the screened and treated group vs. historical controls. The authors concluded that routine screening and treatment was unnecessary [18].
Patients undergoing epilepsy surgery would appear to have a number of treatment-specific risk factors for hemorrhage. Valproic acid, a common anticonvulsant, has been demonstrated to produce both platelet and coagulation pathway dysfunction, although the clinical importance of these findings has been debated. The ketogenic diet has been reported to induce platelet aggregation deficiencies. Pacione et al. prospectively evaluated 39 children undergoing epilepsy surgery with an extensive battery of laboratory testing through a hematology clinic that included von Willebrand antigen, ristocetin cofactor testing (as part of a vWD work-up), factor VIII assay, and platelet aggregation tests. Fifteen children had Tuberous Sclerosis (TS) . Twenty-five percent of patients had abnormal platelet function or a coagulation panel abnormality. One third of children with TS were affected, all with platelet abnormalities. Two of these five children had a negative clinical history screen and one developed a subdural hematoma, despite preoperative platelet transfusion. Twenty percent of children without TS were affected with all suffering coagulation abnormalities. Three of these had negative history, but two had minor enough abnormalities that no treatment was prescribed and no bleeding complications occurred. The authors suggest that children with TS undergoing epilepsy surgery may be at increased risk for hemorrhage and may benefit from more extensive preoperative testing [45].
As noted above, the platelet inhibitor clopidogrel plays an important role in preventing ischemic complications after neuroendovascular procedures. Kashiwazaki and colleagues prospectively evaluated 66 Asian patients undergoing carotid stenting and intracranial stent/coiling procedures, who were all receiving both aspirin and clopidogrel preoperatively. Prior to the procedure, platelet function was assessed using the VerifyNow P2Y12 assay. Based on ROC curve analysis, response to clopidogrel therapy was considered subtherapeutic, when the percent inhibition was <25 % (19 patients), adequate when between 25 % and 75 % (32 patients), and supratherapeutic when >75 % (15 patients). The rates of ischemic complications in the three groups were 37 %, 19 %, and 0 % while the rates of bleeding complications were 0 %, 6 %, and 40 % respectively. All ischemic complications were abnormalities on postprocedure diffusion-weighted imaging and did not appear to have a clinical correlation. Bleeding complications were groin hematomas in six patients, optic disc hemorrhage, and epistaxis [46].
Putting It All Together
Preoperative assessment for bleeding risk should be based primarily on history and physical exam including the identification of medications that increase bleeding risk. Laboratory tests, such as PT/PTT and Platelet Count or other more specific tests, can be reserved for situations in which there are concerning features by history or exam, although given the lack of prospective evidence specific to neurosurgery, the practice of routine laboratory assessment cannot be completely excluded for neurosurgical procedures, particularly where there is limited opportunity to identify and manage hemorrhage, such as in ventriculostomy or deep brain electrode placement . Patients presenting with hemorrhagic events , either spontaneous or traumatic, should be considered at high risk for coagulopathy and assessed accordingly. Preoperative consultation with a hematologist is appropriate in the setting of either a worrisome clinical or laboratory assessment.
References
Davie E, Ratnoff O. Waterfall sequence for intrinsic blood clotting. Science. 1964;145:1310–2.
Macfarlane R. An enzyme cascade in the blood clotting mechanism, and its function as a biochemical amplifier. Nature. 1964;202:498–9.
Achneck HE, et al. Pathophysiology of bleeding and clotting in the cardiac surgery patient: from vascular endothelium to circulatory assist device surface. Circulation. 2010;122(20):2068–77.
Palta S, Saroa R, Palta A. Overview of the coagulation system. Indian J Anaesth. 2014;58(5):515–23.
Thiruvenkatarajan V, Pruett A, Adhikary SD. Coagulation testing in the perioperative period. Indian J Anaesth. 2014;58(5):565–72.
De Caterina R, et al. General mechanisms of coagulation and targets of anticoagulants (Section I). Position paper of the ESC Working Group on Thrombosis—task force on anticoagulants in heart disease. Thromb Haemost. 2013;109(4):569–79.
Chee YL, et al. Guidelines on the assessment of bleeding risk prior to surgery or invasive procedures. British Committee for Standards in Haematology. Br J Haematol. 2008;140(5):496–504.
Cosmi B, et al. Assessment of the risk of bleeding in patients undergoing surgery or invasive procedures: Guidelines of the Italian Society for Haemostasis and Thrombosis (SISET). Thromb Res. 2009;124(5): e6–12.
Bonhomme F, et al. Pre-interventional haemostatic assessment: Guidelines from the French Society of Anaesthesia and Intensive Care. Eur J Anaesthesiol. 2013;30(4):142–62.
Zwisser B. Preoperative evaluation of adult patients prior to elective, non-cardiac surgery. Joint recommendations of German Society of Anesthesiology and Intensive Care Medicine, German Society of Surgery and German Society of Internal Medicine. Urologe. 2011;50(9):1169–82.
Serafini G, et al. Preoperative evaluation in infants and children: recommendations of the Italian Society of Pediatric and Neonatal Anesthesia and Intensive Care (SARNePI). Minerva Anestesiol. 2014;80(4): 461–9.
Committee on Standards and Practice Parameters, et al. Practice advisory for preanesthesia evaluation: an updated report by the American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Anesthesiology. 2012;116(3):522–38.
Guay J, et al. Ability of hemostatic assessment to detect bleeding disorders and to predict abnormal surgical blood loss in children: a systematic review and meta-analysis. Paediatr Anaesth. 2015;25(12):1216–26.
Burk CD, et al. Preoperative history and coagulation screening in children undergoing tonsillectomy. Pediatrics. 1992;89(4 Pt 2):691–5.
Rapaport SI. Preoperative hemostatic evaluation: which tests, if any? Blood. 1983;61(2):229–31.
Samama CM, et al. Perioperative platelet transfusion: recommendations of the Agence Francaise de Securite Sanitaire des Produits de Sante (AFSSaPS) 2003. Can J Anaesth. 2005;52(1):30–7.
Greinacher A. Clinical Practice. Heparin-induced thrombocytopenia. N Engl J Med. 2015;373(3): 252–61.
Karger R, et al. The Platelet Function Analyzer (PFA-100) as a screening tool in neurosurgery. ISRN Hematol. 2012;2012:839242.
Kimpton G, Dabbous B, Leach P. New oral anticoagulant and antiplatelet agents for neurosurgeons. Br J Neurosurg. 2015;29(5):614–21.
Lordkipanidze M, et al. Assessment of VerifyNow P2Y12 assay accuracy in evaluating clopidogrel-induced platelet inhibition. Ther Drug Monit. 2008;30(3):372–8.
Swank RL, Prichard KH. The screen-filtration pressure method for detecting particular matter in fluid. Ann N Y Acad Sci. 1969;158:753–60.
Poller L. International Normalized Ratios (INR): the first 20 years. J Thromb Haemost. 2004;2(6):849–60.
Matevosyan K, et al. Coagulation factor levels in neurosurgical patients with mild prolongation of prothrombin time: effect on plasma transfusion therapy. J Neurosurg. 2011;114(1):3–7.
West KL, Adamson C, Hoffman M. Prophylactic correction of the international normalized ratio in neurosurgery: a brief review of a brief literature. J Neurosurg. 2011;114(1):9–18.
Peterson P, et al. The preoperative bleeding time test lacks clinical benefit: College of American Pathologists’ and American Society of Clinical Pathologists’ position article. Arch Surg. 1998;133(2): 134–9.
Trapani L. Thromboelastography: current applications, future directions. Open J Anesthesiol. 2013;3:23–7.
Windelov NA, et al. The prognostic value of thrombelastography in identifying neurosurgical patients with worse prognosis. Blood Coagul Fibrinolysis. 2011;22(5):416–9.
McTaggart RA, et al. Use of thromboelastography to tailor dual-antiplatelet therapy in patients undergoing treatment of intracranial aneurysms with the Pipeline embolization device. J Neurointerv Surg. 2015;7(6): 425–30.
McDonald MM et al. Thrombelastography does not predict clinical response to rtPA for acute ischemic stroke. J Thromb Thrombolysis. 2015 [Epub ahead of print].
van Ryn J, Baruch L, Clemens A. Interpretation of point-of-care INR results in patients treated with dabigatran. Am J Med. 2012;125(4):417–20.
Cuker A, et al. Laboratory measurement of the anticoagulant activity of the non-vitamin K oral anticoagulants. J Am Coll Cardiol. 2014;64(11):1128–39.
Neyens R, et al. Dabigatran-associated subdural hemorrhage: using thromboelastography (TEG((R))) to guide decision-making. J Thromb Thrombolysis. 2014;37(2):80–3.
Sandset PM, Francis C, Key N. Guidelines of the Italian Society for Haemostasis and Thrombosis (SISET). Thromb Res. 2009;124(5):515.
Houry S, et al. A prospective multicenter evaluation of preoperative hemostatic screening tests. The French Associations for Surgical Research. Am J Surg. 1995;170(1):19–23.
Gabriel P, Mazoit X, Ecoffey C. Relationship between clinical history, coagulation tests, and perioperative bleeding during tonsillectomies in pediatrics. J Clin Anesth. 2000;12(4):288–91.
Biss TT, et al. Quantitation of bleeding symptoms in children with von Willebrand disease: use of a standardized pediatric bleeding questionnaire. J Thromb Haemost. 2010;8(5):950–6.
Laine C, Williams SV, Wilson JF. In the clinic. Preoperative evaluation. Ann Intern Med. 2009;151(1):ITC1–15. quiz ITC16.
Schramm B, et al. Coagulation studies in preoperative neurosurgical patients. Anaesth Intensive Care. 2001;29(4):388–92.
Dutzmann S, et al. On the value of routine prothrombin time screening in elective neurosurgical procedures. Neurosurg Focus. 2012;33(5):E9.
Seicean A, et al. Use and utility of preoperative hemostatic screening and patient history in adult neurosurgical patients. J Neurosurg. 2012;116(5):1097–105.
Gerlach R, et al. Increased risk for postoperative hemorrhage after intracranial surgery in patients with decreased factor XIII activity: implications of a prospective study. Stroke. 2002;33(6):1618–23.
Idris Z, et al. Association of perioperative factor XIII activity levels and other haemostatic markers with the risk of postoperative intracranial haematoma in a selected cohort of neurosurgical patients. Acta Neurochir (Wien). 2012;154(5):887–93. discussion 893–4.
Adelmann D, et al. Fibrinogen but not factor XIII deficiency is associated with bleeding after craniotomy. Br J Anaesth. 2014;113(4):628–33.
Genecov DG, et al. Preoperative screening for coagulopathy using prothrombin time and partial thromboplastin time in patients requiring primary cranial vault remodeling. Plast Reconstr Surg. 2005;116(2):389–94.
Pacione D, et al. Coagulation abnormalities in children undergoing epilepsy surgery. J Neurosurg Pediatr. 2011;7(6):654–9.
Kashiwazaki D, et al. The roles and issues of P2Y12 percent inhibition assessed by VerifyNow assay for patients undergoing neurointervention: a prospective study. J Stroke Cerebrovasc Dis. 2014;23(7):1830–6.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Garton, H.J.L. (2016). Coagulation Studies in Preoperative Neurosurgery Patients. In: Loftus, C. (eds) Anticoagulation and Hemostasis in Neurosurgery. Springer, Cham. https://doi.org/10.1007/978-3-319-27327-3_21
Download citation
DOI: https://doi.org/10.1007/978-3-319-27327-3_21
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-27325-9
Online ISBN: 978-3-319-27327-3
eBook Packages: MedicineMedicine (R0)