
Abstract
Apart from the common cavernous and small-vessel hemangiomas of the liver, there is a group of other but rare benign vascular tumors in the pediatric and adult liver. Multiple hepatic hemangiomas with a cavernous histology and different from infantile hepatic hemangioma/hemangioendothelioma exist in the pediatric age group and are termed congenital, neonatal, and infantile hemangiomatosis. These lesions can be accompanied with extrahepatic hemangiomas, e.g., those of the skin. One variant is characterized by a diffuse hemangiomatosis involving several organ systems. Diffuse hepatic hemangiomatosis also occurs in adult patients as a rare condition, whereby liver lobes are densely involved by vascular nodules of variable size. The disorder may be associated with splenic hemangiomatosis. Hepatic angiomatosis also develops in the setting of Osler’s disease. An unusual form of hepatic vascular tumor is intravascular papillary endothelial hyperplasia, a reactive lesion usually occurring in the skin and subcutis of adult patients. Hepatic hemangiomas can rarely be associated with proliferation of smooth muscle cells (angioleiomyoma). A further, very rare hepatic vascular tumor is hemangioblastoma, which occurs as a sporadic lesion or develops in the setting of von Hippel-Lindau disease.
Access provided by CONRICYT-eBooks. Download reference work entry PDF
Similar content being viewed by others


Keywords
- Cavernous Hemangioma
- Infantile Hemangioma
- Hepatic Hemangioma
- Littoral Cell
- Intravascular Papillary Endothelial Hyperplasia
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Congenital, Neonatal, and Infantile Hepatic Hemangiomatosis
Introduction
Apart from neonatal and infantile hepatic angiomatous tumors classified as hemangioendotheliomas (type 1 lesions), discussed in a special chapter, there are situations where cavernous vascular malformations (hemangiomas) of the skin are associated with similar lesions in the liver. This combination may be present at birth (congenital or neonatal hepatic hemangiomatosis), manifest postnatally, or later in infancy (infantile hemangiomatosis).
Congenital Hemangiomas Associated with Hepatic Vascular Tumors: Benign Neonatal Hemangiomatosis
A part of infantile hepatic hemangiomas develop in the context of congenital hemangiomas of the skin and other organs and in the setting of hemangiomatosis. A neonate with multiple hemangiomatosis can be categorized into two main clinical entities: (1) benign neonatal hemangiomatosis (BNH; Stern et al. 1981) and (2) diffuse or disseminated neonatal hemangiomatosis (DNH). Multiple cutaneous infantile hemangiomas (hemangiomatosis) are reported to arise in 10–25 % of infants with cutaneous hemangiomas (Achauer et al. 1997). Multiple hemangiomas of the skin in infants, in particular more than five lesions, are a marker of possible internal hemangiomatosis, with the liver being an important site (concurrent cutaneous and hepatic hemangiomas; Robinson and Hambleton 1977; Berman and Lim 1978; Metry et al. 2004). Among 47 patients with segmental hemangiomas of the skin, 79 % of the patients had their skin hemangiomas on the face, and 43 % showed liver hemangiomas, followed by the gastrointestinal tract (34 %) and the brain (34 %). Forty percent of the patients in this study fulfilled the criteria of PHACE syndrome (posterior fossa brain malformations, hemangiomas, arterial anomalies, coarctation of the aorta, cardiac defects, and eye abnormalities) (Metry et al. 2001, 2004). Multiple congenital hemangiomas of the skin in a neonate have been found to be associated with hepatic angiosarcoma (Nord et al. 2006).
Diffuse Neonatal Hemangiomatosis
In some of the patients with congenital hemangiomas, the development of the lesions follows a diffuse pattern (diffuse congenital/neonatal hemangiomatosis). Diffuse/disseminated neonatal hemangiomatosis (DNH) is a rare neonatal condition in which cutaneous and visceral hemangiomas coexist. The disorder is also termed multiple miliary neonatal hemangiomatosis (review: Enjolras and Mulliken 1998). DNH hemangiomas are either present at birth or develop during the first week of life and are twice as frequent in girls in comparison with boys (Holden and Alexander 1970; Golitz et al. 1986; Ho et al. 2000; Schulze et al. 2006; Wananukul et al. 2006; Gouedard et al. 2007; Al-Kaabi et al. 2009; Glick et al. 2012). The first sign of DNH is the appearance of cutaneous hemangiomas, which may become more numerous and extensive. In addition to multiple hemangiomas of the skin, other possibly involved organs include the liver and, less commonly, pleura, lungs, intestines, central nervous system, and eyes. Involvement is limited to the skin and liver in part of the patients. If left untreated, DNH is often fatal at an early age, carrying an estimated 60–95 % mortality, although novel treatments have improved prognosis.
DNH reveals liver angiomas with variable frequencies (Pavlenishvili and Nemsadze 1978; Young et al. 1981; Montgomery et al. 1990; Hurvitz et al. 2000; Gottschling et al. 2006). Hepatic hemangiomas arising in the setting of DNH may grow to large size (e.g., 4 cm diameter; Gottschling et al. 2006). Hepatic hemangiomas in DNH may be associated with cardiac insufficiency caused by blood shunting through the tumor’s vascular channels (Hurvitz et al. 2000; Gottschling et al. 2006). DNH with or without liver involvement may be associated with placental chorioangioma (Witters et al. 2003; Bakaris et al. 2004).
Previously, the mean age at death was 11 weeks (Stratte et al. 1996). In a retrospective analysis of the literature, it turned out that the mortality rate was 77.4 % in untreated patients and 27 % in treated patients, important risk factors for adverse outcome being congestive heart failure, coagulopathy, and the involvement of five or more organs (Lopriore and Markhorst 1999). Complications of DNH include high-output cardiac failure, marked thrombocytopenia with hemorrhage, consumption coagulopathy, and hepatic failure. In adult long-term survivors of DNH, visceral hemangiomas in the absence of cutaneous hemangiomas have been observed (Ohnishi et al. 2002). In some of these adults, DNH is visualized on CT images as multiple calcifications in the liver, spleen bowel wall, and adrenals (Latifi and Siegel 1992), representing dystrophic calcification of regressed hemangiomatous lesions. Rarely, DNH develops in congenital overgrowth syndromes, e.g., Simpson-Golabi-Behmel syndrome (Poetke et al. 2002).
The previous concept of DNH may require revision, specifically in regard to the exact types of vascular tumors involved. A recent evidence-based review of case reports of DNH was based on the hypothesis that many cases reported as DNH did in fact not have infantile hemangiomas and also other forms of neonatal vascular diseases. Between the years 1950 and 2009, 73 cases were selected from the literature and categorized into three groups: infantile or probable (P) infantile hemangioma (IH/P-IH), multifocal lymphangioendotheliomatosis with thrombocytopenia (MLT/P-MLT), and multifocal vascular lesions, not otherwise specified. Of these 73 cases, 43 had IH/P-IH, 17 had MLT/P-MLT, and 13 had multifocal vascular lesion NOS. Five percent of patients in the IH/P-IH group died, in contrast to a death rate of 65 % in the MNLT/P-MLT group (Glick et al. 2012).
Hepatic Hemangiomatosis of Infancy
There are published observations of infantile hemangioma, i.e., postneonatal hemangiomatosis characterized by the combination of cutaneous hemangiomas and visceral/hepatic hemangiomas, i.e., cavernomas and not hemangioendotheliomas (Robinson and Hambleton 1977; Rotman et al. 1980; Larcher et al. 1981; Vorse et al. 1983; Platokouki et al. 1998; Mendiratta et al. 2008). Hepatic hemangiomas may be combined with other visceral hemangiomas, in particular splenic lesions (Platokouki et al. 1998). Similar to the neonatal situations, large and/or multiple lesions can cause cardiac failure (Vorse et al. 1983).
Pathogenic Pathways
The concomitant development of angiomatous lesions in the skin and visceral organs is striking and suggests an abnormal multifocal angiogenic mechanism leading to the emergence of multiple circumscribed angiomatous malformations. The cause of this angiogenic response is not known, and we also do not know why such characteristic multifocal patterns arise and why certain organs and not others are involved. As some of the lesions can later undergo involution, a complex derangement of vascular growth versus vascular remodeling and regression through apoptosis may be operational. The transient growth of angiomatous lesions, in part modulated by external factors, in some way mimics the emergence of a definitive vascular network but with a highly abnormal growth overshoot.
Diffuse Hepatic Hemangiomatosis of Adults
Introduction
Diffuse hepatic hemangiomatosis of adults is a very rare condition with so far not well-known etiology and natural history. The disorder is mostly known from infants and is much less common in adults. It is defined as the presence of numerous synchronous hemangiomas, mostly of the cavernous type, in one liver lobe, right and left lobe, or the entire liver, in the absence of extrahepatic hemangiomas. The difference between “numerous” hemangiomas (diffuse hemangiomatosis) and “multiple” hemangiomas has not been clearly worked out. For the diagnosis of diffuse hemangiomatosis, the distribution pattern of the lesions is crucial, i.e., involvement of large parts of the liver or the entire liver. The prevalence of diffuse hemangiomatosis of the liver is not well known. Among 26 patients with hepatic hemangiomas, six were diffuse lesions (Dickie et al. 2009). Sometimes, accompanying hemangiomatosis of the spleen is present (diffuse hepatosplenic hemangiomatosis; Tarazov et al. 1990; Langner et al. 2001). Most patients are women (Popa et al. 1984; Langsteger et al. 1990; Lehmann et al. 1999; Moon et al. 2000; Guzman-Valdivia Gomez et al. 2006; Kim et al. 2008).
Clinical and Imaging Features
The clinical presentation of hepatic hemangiomatosis is usually nonspecific and related to multiple mass effects and hepatomegaly. Some of the patients experience moderate to intense abdominal pain. Patients with diffuse liver hemangiomas sometimes produce significant tumor-associated shunts, followed by heart failure (Jayanthi et al. 2000). Diffuse hepatic hemangiomatosis with its enormous coagulative vascular surface with altered endothelial features can cause thrombocytopenia (Jayanthi et al. 2000). Extensive hemangiomatosis can cause sinusoidal compression/congestion, thereby causing a sinusoidal blockage and eventually portal hypertension with esophagogastric varices. The hemangiomas may behave in a stable way, with minor or absent change with time, but progressive forms extending from liver lobe to the other are known (Lehmann et al. 1999). Diffuse hepatic hemangiomatosis can be associated with secondary polycythemia (Popa et al. 1984). The cause of progressive growth is not established, but enhanced growth of hepatic hemangiomatosis was observed in two adults following postmenopausal estrogen replacement therapy (Ozakyol and Kebapci 2006). One patient with secondary polycythemia has been described (Popa et al. 1984).
Diffuse hepatic hemangiomatosis has characteristic imaging features on US, CT, and MR images (Crespo Uriguen et al. 1988; Feurle 1990; Langsteger et al. 1990; Frangides et al. 1995; Lehmann et al. 1999; Moon et al. 2000; Vilgrain et al. 2000; Mihalche and Dumitrache 2004; Guzman-Valdivia Gomez et al. 2006; Blondet et al. 2007). Ultrasonography shows small to large, hypoechoic masses with ill-defined margins to the adjacent liver substance, but confluent hyperechoic masses are also in evidence (Vilgrain et al. 2000). Contrast enhancement with a centripetal filling pattern of the entire tumors on the delayed phase of dynamic CT and inhomogeneous diffuse uptake of the entire tumor on delayed blood-pool images on 99mTc-labeled red blood cell scans are characteristic features (Kim et al. 2008). As the tumorous lesions have prominent flow, hepatic artery branches as the feeding vessels are dilated (Moon et al. 2000). On MR images, most tumors showed a low signal intensity on T1-weighted images and a high signal intensity on T2-weighted images. Areas with macroscopic cystic change have foci of lower intensity than the remainder of tumor on T1-weighted images and higher intensity than the remainder of tumor on T2-weighted images (Moon et al. 2000).
Pathology
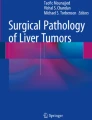
In most cases, the liver lobes are densely involved by hemangiomatous nodules of variable diameters (Fig. 1), resulting in distinct patterns summarized in Table 1. In part of patients, the entire liver is packed with typical, well-delineated angiomatous tumors, with thin and partly atrophic parenchymal bridges between the nodules (massive panhepatic hemangiomatosis, MPHH). In regard to the distribution of lesions, a diffuse pattern, in which numerous tumors are present as isolated, more or less evenly distributed hemangiomas, and nodular pattern consisting of multiple coalescent nodules measuring <5 mm in diameter have been distinguished (Jhaveri et al. 2011). Individual tumors may exceed 4 cm in diameter and therefore qualify for giant hemangiomas. In fact, hemangiomatosis can be associated with giant hepatic hemangiomas in a significant proportion of cases (Adam et al. 1970; Jhaveri et al. 2011). In a series of 22 patients with giant hepatic hemangioma, associated diffuse hemangiomatosis involving the right and left liver lobes was found in four patients (Adam et al. 1970). At laparoscopy, multiple to numerous medium-sized to large blue-black spongy masses are seen, sometimes bulging from the liver surface (Guzman-Valdivia Gomez et al. 2006). Pedunculated lesions also occur (Blondet et al. 2007). The number and size of hemangiomas may be such as to grossly mimic massive diffuse hepatic metastatic disease.

Hepatic hemangiomatosis of the adult. The liver contains several well-delineated foci of hemangioma, in part with fresh thrombosis
Most tumors show the typical histology of cavernous hemangiomas, with large, endothelium-lined channels prevailing in the core region of the tumors and smaller vascular channels at the periphery of the nodules, where also feeding vessels are found, and regressive changes in the center (fibrosis, thrombosis, granulation tissue). As in isolated giant liver hemangiomas, large tumors may show extended central fibrosclerosis or even hyalinosis and sometimes fresh or old infarctoid necrosis. The adjacent liver substance reveals perifocal parenchymal atrophy or fatty change of hepatocytes and may contain dilated veins or intermediate vessels, sometimes rather remote from the tumor nodules (Lehmann et al. 1999).
Diffuse Hemangiomatosis of the Liver and Spleen (Diffuse Hepatosplenic Hemangiomatosis)
In part of the patients with diffuse hemangiomatosis, the liver and spleen are synchronously involved (Tarazov et al. 1990, 1991; Langner et al. 2001). This entity may be associated with progressive liver failure, thrombocytopenia, and coagulopathy (Langner et al. 2001).
Focal and Diffuse Hemangiomatosis Associated with Giant Hepatic Hemangioma
Circumscribed or focal, or even diffuse, hemangiomatosis with the development of multiple small nodules may be noted in association with large cavernous hepatic hemangiomas (so-called giant hemangiomas; Melis 1954; Jhaveri et al. 2011). Among 42 cases of giant hepatic hemangioma, associated hepatic hemangiomatosis was detected in 18 patients (44 %). Twelve patients had a diffuse pattern of hemangiomatosis (67 %), and six patients showed a nodular pattern consisting of multiple coalescent nodules measuring <5 mm (33 %). There was no association between the size of the giant hemangioma and extent of hemangiomatosis (Jhaveri et al. 2011). The pathogenesis of this alteration has not been clarified. Theoretically, small and satellite-like hemangiomas in the vicinity of a large lesion may emerge due to the abnormal blood circulation surrounding the large lesion, or may reflect a field effect, i.e., emergence of multiple angiomas within an abnormal vascular bed, with one and large predominant lesion.
Hepatic Hemangiomas in Systemic Adult Hemangiomatosis (Polysomatic Hemangiomatosis)
Systemic hemangiomatosis (diffuse hemangiomatosis, hemangiomatosis diffusa) is a very rare condition characterized by the occurrence of cavernous hemangiomas in multiple organ systems, including the skin, bone, central nervous system, and visceral organs. The process has either been interpreted to be neoplastic or to represent a hamartoma-like malformation, but the involvement of numerous tissue and organ types together with continuous growth in at least part of the patients favors a highly abnormal angiogenic and probably neoplastic process. The disease is sporadic, without evidence of a familial trait (Fischer and Roeckl 1961; Tsukagoshi et al. 1998; Erdogan et al. 2003). Visceral manifestations can involve several intra-abdominal organs, e.g., the spleen, liver, intestine, peritoneum, and lymph nodes, in one and the same patient (Maeda et al. 1981; Ribback et al. 2011). Some cases have revealed an aggressive course with poor prognosis, owing to continuous growth of the lesions (Böhm et al. 1980).
Liver involvement in the form of cavernous hemangiomas has been observed (Bargon and Yu 1968; Gordin et al. 1975; Maeda et al. 1981; Erdogan et al. 2003; Edlow et al. 2006). Liver involvement can be associated with angiomatous lesions of the intestine, spleen, and lymph nodes (Maeda et al. 1981). The angiomatous lesions developing in the liver may be extensive and cystic, resulting in a “honeycomb-like” liver (Tsukagoshi et al. 1998).
Hepatic Hemangiomas Combined with Skeletal Hemangiomatosis
Diffuse skeletal hemangiomatosis (disappearing bone disease) is a very uncommon disorder, which is characterized by osteolytic angiomatous lesions causing vanishing bone in part of the patients (syndrome of phantom bone or disappearing bone). An aggressive form of the disease that shows regional involvement and massive osteolysis, frequently involving the shoulder and hip areas, is called Gorham’s disease. In the marrow cavities of involved bones, numerous thin-walled and partly dilated vascular channels are present, with signs of bone substance lysis in the vicinity (Bezold 1951; Gorham et al. 1954; Ishida et al. 1994; Wallis et al. 1994, Clayer 2002).
The disorder is sometimes associated with visceral and in particular hepatic hemangiomas (Bargon and Yu 1968; Waldron and Zeller 1969; Kane and Newman 1973; van den Bosch et al. 1975; Rolain et al. 1978; Körster and Jansen 1981; Kiriyama et al. 2001). In an old female patient described by Kane and Newman (1973), marked hepatomegaly was found, tender to palpation. A large left lobe presented as an epigastric mass with a systolic bruit. A liver scan showed an enlarged pattern with increased uptake in the left lobe. Transfemoral visceral angiography demonstrated numerous diffuse capillary-sized hemangiomatous vessels accounting for hepatomegaly and bruit. There was rapid shunting to the hepatic veins and inferior vena cava and retrograde filling of the portal vein, coronary vein, and gastric and mesenteric collateral veins.
Hepatic Hemangioma in Cystic Angiomatosis of the Bone
Cystic angiomatosis of the bone (CAB, diffuse cystic angiomatosis of the bone; Gorham’s vanishing bone disease; Gorham’s massive osteolysis; Gorham-Stout syndrome; phantom bone disease; idiopathic massive osteolysis) is a rare, multicentric disease characterized by involvement of blood and lymph vessel systems, producing diffuse cystic lesions in the skeleton, predominantly affecting the trunk bones (review: Möller et al. 1999).
This intriguing disorder has been described in 1914 (Shennan 1914; “histologically nonmalignant angioma, with numerous metastases”), and the term CAB was coined in 1953 (Jacobs and Kimmelstiel 1953). In most cases, CAB will show a widespread distribution in the skeleton, but very rare localized forms have also be encountered, e.g., in the cranio-cervical region (Pavanello et al. 2007). Familial CAB has been observed in one family over four generations (Reid et al. 1989) and four siblings showing congenital generalized lipodystrophy accompanied by CAB (Brunzell et al. 1968). In its presentation, CAB is similar to diffuse angiomatosis of the bone, but the relationship between these two disorders has not yet been clarified. Histologically, CAB shows a contribution of lymph vessels, a feature usually lacking in diffuse angiomatosis of the bone. CAB causes osteolytic lesions with internal septation of the bone and a honeycomb appearance of the skeletal system (Jacobs and Kimmelstiel 1953; Ritchie and Zeier 1956; Boyle 1972; Shivaram et al. 2007; Pulido-Zamudia 2001; Malik et al. 2008).
CAB may be associated with chylothorax (Deveci et al. 2011) and with visceral hemangiomas, including hepatic hemangiomas and splenic angiomas/angiomatosis (Fernandez Jimenez et al. 2000; Vanhoenacker et al. 2003). In two patients found in the literature, only splenomegaly was noted (Shennan 1914). Lymphangioma of the spleen has been described in CAB (Boyle 1972), further supporting the involvement of the lymph vessel system and a systemic lymphangial disorder in CAB.
Hepatic Hemangiomas in Segmental Infantile Hemangioma and Reticular Infantile Hemangioma
Introduction
An uncommon form of cutaneous infantile hemangioma is characterized by a flat, blotchy lesion, which, in the past, has been called “port-wine stain-like”. When occurring in the face, this variant is called “segmental” and is known to be an indicator for posterior fossa brain malformations, hemangiomas, arterial anomalies, coarctation of the aorta, cardiac defects, and eye malformations (the PHACE association; Frieden et al. 1996; Haggstrom et al. 2010). Later, this variant of cutaneous hemangioma has been renamed, reticular infantile hemangioma, to denote this distinctive macular, network-like lesion (Mulliken et al. 2007).
Liver Involvement in Segmental Hemangioma
A total of 47 cases of solitary segmental hemangiomas of the skin in association with visceral hemangiomatosis has been reviewed. Among these cases, the liver was the most common internal organ involved by hemangiomas (43 % of the cases; Metry et al. 2004).
Liver Involvement in Reticular Hemangioma
In this hemangioma, liver manifestations may be present. In one male infant with reticular cutaneous hemangioma associated with arteriovenous shunting in the pelvis and lower extremity, the liver showed multiple nodular enhancing lesions on T2-weighted MRI, consistent with multiple hemangiomas (Mulliken et al. 2007).
Intravascular Papillary Endothelial Hyperplasia (IPEH) of the Liver
Introduction
Intravascular papillary endothelial hyperplasia (IPEH; synonyms: Masson’s pseudoangiosarcoma; Masson lesion; Masson’s tumor) was described by Masson in 1923 under the term, hémangioendothéliome végétant intra-vasculaire (vegetant intravascular hemangioendothelioma, Masson 1923; review: Steffen 2003). In 1932, the lesion was described again by use of a different terminology (thrombopoietic proliferating endovasculitis; Henschen 1932). IPEH is now regarded as a benign, nonneoplastic vascular lesion originating from an organizing vascular thrombus or, less frequently, from a hematoma, with unusual reactive proliferation of endothelial cells (Clearkin and Enzinger 1976; Hashimoto et al. 1983). Variants of PEH developing in an extravascular compartment and specifically in hematomas are termed extravascular papillary endothelial hyperplasia (EPEH; Pins et al. 1993; Sezgin et al. 2005).
The lesion typically occurs in adults, but pediatric cases have also been reported. IPEH has a propensity to occur in the skin and subcutis, but other locations are also well documented, including the breast and mammary subcutaneous tissue, oral cavity, hypopharynx and larynx, parotid gland, lung, intestinal tract, spleen, tendon sheaths, kidney, urinary bladder, renal vein, other large vessels and their aneurysms, adrenal, retroperitoneal space, bone, central nervous system, and liver (Hong et al. 2004; Kan et al. 2004). In the skin, IPEH may present as multiple recurrent dark to almost black papular lesions involving the entire body, resembling cutaneous metastases of malignant melanoma. IPEH is commonly a slow-growing lesion, but phases of rapid enlargement of the process may be caused by repeated bleeding into the lesion, and hemorrhage from IPEH may be massive (Jung et al. 2005; Rizza et al. 2009).
IPEH of the Hepatobiliary System
IPEH can involve the gastrointestinal tract (Meadows et al. 2010). Very rarely, IPEH has been detected in the liver (Hong et al. 2004; Kan et al. 2004). A 69-year-old female showed, on abdominal CT scan, a 10 × 7 cm-sized, lobulated heterogeneous contrast-enhancing soft tissue mass involving the entire left liver lobe (Hong et al. 2004). In the arterial phase of CT, the mass had a focal nodular enhancement around its peripheral portion, whereas in the delayed phase, there was a persistent low-density noncontrast-enhancing portion in the tumor center. Angiography exhibited some tumor-supplying arteries originating from the left hepatic artery. The mass seen during operation was limited to the left liver lobe, of 10 × 7 cm size, and was a nonhomogeneous multinodular mass including focal necrosis. No major vessel invasion was observed. Histology of the resection specimen showed IPEH. The 65-year-old male patient described by Kan and coworkers (Kan et al. 2004) had a cystic, focally calcified mass of several cm diameter located within a dilated left ventricular cavity. This mass appeared to float between the ventricle and mitral valve area. Multiple hyperechoic hepatic nodules were also identified on an abdominal sonograph. Histology of the resected lesion showed IPEH, and similar alterations were found in liver biopsies. The liver nodules had the same papillary structures within the liver parenchyma but had spared the portal tracts.
Pathology
Based in the pattern of lesion development, IPEH is pathologically classified in three subtypes: a pure form, the most common, in which the lesion arises in dilated blood vessels; a mixed form in which IPEH arises in preexisting vascular alterations (hemangioma, aneurysm, arteriovenous malformation, and pyogenic granuloma), and an extravascular form, the latter called EPEH.
Histologically, two different papillary structures are observed: one defined as inflammatory papilla constantly associated with thrombotic material and the other defined as fibrous papilla in the absence of a visible thrombus (Eusebi et al. 1980). IPEH may mimic Kaposi’s sarcoma (Reed et al. 1984; Torres and Rodriguez 1984). Immunohistochemically, the endothelial structures are reactive for CD34, and the spindle cells are positive for vimentin and, in part, smooth muscle actin (Soares et al. 2008). Reactivity of endothelial cells for factor VIII-associated antigen was only observed in advanced or “mature” lesions, similar to what happens in organizing thrombi (Albrecht and Kahn 1990).
Pathogenesis
There is clear evidence that IPEH arises from an exuberant organizing reaction within a thrombus (organizing thrombus theory; Del Rio et al. 1992). Similar lesions are sometimes found within hematomas, i.e., outside vascular spaces (EPEH; see above; Pins et al. 1993; Aulicino et al. 1995; Sezgin et al. 2005).
Hepatic Angioleiomyoma
Introduction
Angioleiomyoma (angiomyoma, vascular leiomyoma) is a benign soft tissue tumor that usually develops in the subcutaneous tissue of the lower extremities. These circumscribed nodules consist of intertwined thick-walled, abnormal vessel structures formed by proliferating smooth muscle cells and narrow or slit-like vascular channels (reviews: Hachisuga et al. 1984; Ramesh et al. 2004).
Clinical and Imaging Findings
Angioleiomyoma commonly presents as a painful mass in about 60 % of the cases. Tumors located in the extremities, and specifically in the hand, typical display swelling with physical activity of the involved part (Hachisuga et al. 1984; Ramesh et al. 2004). Pain of the nodule (tuberculum dolorosum) is thought to be caused by local ischemia due to contraction of the tumor vessels. In an analysis of 229 cases, the lesions were detected in high incidence in the fourth to sixth decade, with a clear predilection for females (Katenkamp et al. 1988).
Cytogenetic Findings
Relatively few data are available concerning karyotypic aberrations in angioleiomyomas, including t(X;10)(q22;q23.2) (Sonobe et al. 1996), del(6)(p21p23), del(21)(q21)[12] (Heim et al. 1986), t(X;11)(p11.4;p15) (Hennig et al. 1999) ), and t(4;5)(p12;q33), der(13;15)(q10;q10) (Welborn et al. 2010), and del(6)(q13q23), add(8)(q24),del(19)(q10) (Welborn et al. 2010). Comparative genomic hybridization was employed to study relative DNA copy number changes in 33 angioleiomyomas. In about a third of the cases, DNA copy number changes involved one or two chromosomes with losses of chromosome 22 being the most common (Nishio et al. 2004).
Angioleiomyoma of the Hepatobiliary Tract
Angioleiomyoma of the liver has been described in 60-year-old woman with mild upper right quadrant pain for 1 month. Plain spiral CT scans showed a solitary, well-demarcated liver lesion of 4 cm diameter in liver segment VIII. CT with contrast revealed slight homogeneous enhancement (60 HU) of the tumor in relation to the surrounding normal liver substance. Tumor biopsy showed typical angioleiomyoma, with medium-sized blood vessels with thickened walls. The vessel wall cells were in concentric order with intervening radiant emission of spindle and epithelioid cells in intervascular bundles. The patient had an eventful course (Beissert et al. 2002). Angioleiomyoma has been observed in the gallbladder, sometimes causing hemobilia and acute colicky pain (Aschl et al. 1999; Segura-Sampedro et al. 2012).
Pathology
Histologically, four variants have been described, i.e., solid/capillary forms (18 %), venous forms (38 %), mixed/combined forms (43 %), and cavernous forms (<1 %) (Hachisuga et al. 1984; Katenkamp et al. 1988; Figs. 2 and 3). Mixed and cavernous forms seem to be more frequent in male patients (Katenkamp et al. 1988). Most of the cells forming the nodule are strongly reactive for alpha smooth muscle actin. Immunohistochemically, the tumor itself does not contain CD34-positive stromal cells, but bundles of such cells are present at the tumor border and in the adventitial tissue of the surrounding normal vessels (Nakayama et al. 2002). Subcutaneous smooth muscle tumors stain for p16 (Longano et al. 2010).

Hepatic angioleiomyoma. Slit-like vascular spaces with intervening smooth muscle cells (hematoxylin and eosin stain)

Hepatic angioleiomyoma. Numerous neoplastic spindle cells are reactive for smooth muscle actin (alpha-SMA immunostain)
Hemangioblastoma
ICD-O code 9161/1
Introduction
Hemangioblastoma (synonym, capillary hemangioblastoma) is a distinct benign vascular tumor of uncertain histogenesis characterized by a network of vascular channels admixed with often lipid-laden macrophages (the stromal cells). Most hemangioblastoma develops in the central nervous system, particularly in the area of the cerebellum and less often in the lateral ventricle, corpus callosum, spinal cord, retina, optic nerve, pituitary gland, pineal gland, and meninges. Up to 2.5 % of all intracranial tumors are hemangioblastomas. Hemangioblastomas occur as sporadic lesions or arise in the setting of von Hippel-Lindau disease. A distinct pathway is involved in angioblastomas developing in von Hippel-Lindau (VHL) disease. In this disorder, angioblastomas typically emerge in the retina and the central nervous system, but they may also occur in other parts of the body. Organs and tissue involved with sporadic hemangioblastoma outside the CNS include the kidney, adrenal gland, and retroperitoneum. In the lung, a novel hemangioblastoma-like clear cell stromal tumor was found that may have a relation to the hemangioblastoma-associated stromal cells (Falconieri et al. 2013). Few hemangioblastomas have been shown to contain complex differentiation patterns, e.g., rhabdoid features (Yin et al. 2012). Hemangioblastomas occurring in the setting of VHL contain mast cells that seem to be tumor-derived (Merrill et al. 2013).
Primary Hepatic Angioblastoma
Hemangioblastoma can very rarely develop in the liver, even as multifocal hyperechogenic lesions (Rojiani et al. 1991; McGrath et al. 1992; Hayasaka et al. 1999). These hypervascular and arterialized masses have been reported to show the same histologic pattern as the respective CNS tumors, i.e., a complex mixture of vascular structures and stromal cells mainly representing lipid-laden foamy macrophage-like cells (Rojiani et al. 1991; Hayasaka et al. 1999). This morphologic presentation is clearly different from typical hepatic hemangioma, which may rarely occur in VHL (Zeitlin 1942). A part of the hepatic hemangioblastomas were developed in the setting of VHL (Hayasaka et al. 1999). In one patient with VHL, multiple hepatic and pulmonary hemangioblastomas were demonstrated (McGrath et al. 1992).
Other Hepatic Lesions Associated with von Hippel-Lindau Disease
Patients with VHL can develop ordinary hepatic hemangiomas (Yavas et al. 2013) and hepatic cysts (Lee et al. 2010) as a part of the VHL-associated multiple cyst syndrome.
Differential Diagnosis
The very rare hepatic hemangioblastomas may histologically be confounded with other hepatic angiomatous lesions having small vascular channels, such as capillary or lobular hemangiomas.
Pathogenic Pathways
Hemangioblastomas composed of a probably still immature endothelial lineage and stromal cells seem to represent a mimicker of an early mesodermal phase of angiogenesis. The potential involvement of an early mesodermal switch is supported by the reactivity of these tumors for the mesodermal transcription factor, brachyury/Bra (Barresi et al. 2012). The typical stromal cells of hemangioblastoma are thought to be committed stem cells, because they express both CD133 and Oct4, and are suggested to produce the distinct CD133-positive endothelium of these tumors (Welten et al. 2012). It has also been proposed that the tumors might derive from neoplastic transformation of neural stem cells in a specific niche (Ma et al. 2011) or from embryologic multipotent cells (Park et al. 2007). In the cerebella of patients with VHL, developmentally arrested structural elements (arrest of angioblastic lineage) were detected (Vortmeyer et al. 2003). These structures are composed of poorly differentiated cells expressing hypoxia-inducible factor (HIF)2alpha, but not HIF1alpha or brachyury. These elements were mainly found in the molecular layer of the dorsum cerebelli, structures proposed to be developmentally arrested hemangioblast progenitor cells (Shively et al. 2011).
The cell systems involved in the pathogenesis of hemangioblastoma are subject to the complex metabolic alterations associated with von Hippel-Lindau disease (VHL), an autosomal-dominant disorder (OMIM 193300). Patients with VHL suffer from familial and sporadic hemangioblastomas, clear cell carcinoma of the kidney, pheochromocytoma, distinct neuroendocrine tumors, epididymal papillary cystadenomas, microcystic adenomas of the pancreas, endolymphatic sac tumors, cysts in several organs (mainly pancreas), and inherited forms of erythrocytosis (review: Maher et al. 2011). VHL is caused by germ line mutations of the VHL tumor suppressor gene and of the gene product, pVHL (review: Kortmeyer et al. 2013).
pVHL, which is localized to the cytoplasm of normal and neoplastic cells (Corless et al. 1997). has a central role in the regulation of oxygen sensing via the hypoxia-inducible factor (HIF) signaling cascade. HIFs are heterodimeric oxygen-sensing transcription factors that are crucially involved in the cellular adaptation to low oxygen environments. The extensive transcriptional program regulated by HIFs involves the induction of genes that control angiogenesis, cell proliferation and apoptosis, and mechanisms involved in metastasis. HIFs are heterodimers consisting of HIF-alpha and HIF-beta subunits. HIF-2alpha-dependent gene expression, such as ANGPLT4 and erythropoietin, are regulated by PARP-1/poly(ADP-ribose) polymerase-1 in the hypoxic response (Gonzalez-Flores et al. 2014). VHL acts as a master regulator of HIF activity by recognizing the substrate-recognition component of an E3 ubiquitin ligase complex that ubiquitinylates the hydroxylated catalytic alpha subunit of HIF for oxygen-dependent degradation (review: Haase 2009). Three cellular oxygen sensors mark the HIFs for pVHL-mediated degradations, i.e., the prolyl hydroxlyases PHD1, PHD2, and PHD3 (Pientka et al. 2012; Jaakkola and Rantanen 2013; Myllyharju and Koivunen 2013). The stability of HIF1alpha is increased by interaction of the transitionally controlled tumor protein/TCTP and degradation of pVHL. In hypoxic tumor tissues, VEGF expression is positively regulated by histone deacetylase 1/HDAC1 and negatively regulated by the pVHL via HIF1alpha (Reynoso-Roldan et al. 2012). HIF2alpha is regulated, in its action as a proangiogenic factor, by the orphan nuclear receptor TLX (Zeng et al. 2012). The role of HIFs as proliferation-stimulating factors depend on their role as an mTORC1 activator (Elorza et al. 2012).
pVHL binds to two subunits of the transcription elongation complex elongin, causing a decreased activity of this complex, suggesting that pVHL functions as a negative regulator of transcription elongation. There is evidence that regulated accumulation of HIF caused by failure of pVHL-mediated HIF degradation is an important factor in oncogenic pathways operating in VHL, e.g., in clear cell renal carcinoma. A second proposed oncogenic mechanism related to HIF involves E-cadherin, an adhesion molecule playing a significant role in cancerogenesis. pVHL promotes an E2-box-dependent E-cadherin transcription by HIF-mediated regulation of the transcription repressors SIP1 and snail (Evans et al. 2007). pVHL is also involved in the control of genomic stability. In response to DNA double-strand breaks, the suppressor of cytokine signaling 1 (SOCS1) promotes nuclear redistribution and K63 ubiquitinylation of pVHL. Loss of pVHL function in VHL compromises its K63 ubiquitinylation and attenuates the DNA-damage response, causing persistence of DNA double-strand breaks and promoting genomic instability and tumorigenesis (Metcalf et al. 2013). A further important role of pVHL, proposed to be involved in tumorigenesis, is related to cilial function. Primary cilium formation in renal cells requires the action of pVHL (Lutz and Burk 2006), and defective function of pVHL in VHL may thus promote renal and other cysts by failure of ciliogenesis (Rankin et al. 2006). This effect of pVHL on ciliogenesis depends of the phosphorylating factor, Nek1 (Patil et al. 2013). The high frequency of renal carcinomas in VHL may also be connected with a cilial connection of pVHL. It was found that human renal carcinomas have a lower frequency of cilia than the neighboring parenchymal tissue (Basten et al. 2013). Mice with targeted inactivation of the VHL gene developed hepatic cavernous hemangiomas (Haase et al. 2001), while in another murine model, VHL and PTEN conditional deletions caused multiple cavernous liver lesions in a coordinated manner (Chen et al. 2010). The probability of developing familial or recurrent sporadic hemangioblastoma in patients with mutated VHL is higher in the presence of a vitronectin M381T polymorphism (Huang et al. 2009).
Liver Involvement in Splenic Littoral Cell Tumors
Introduction
Littoral cell vascular tumors of the spleen form a unique group of vascular neoplasms are derived from cells of the red pulp, with a variable biology of disease. Littoral cell angioma, the most common form within the group, was first described in 1991 (Falk et al. 1991). Since then, other variants have been defined. The neoplastic cell is regarded as the transformed offspring of splenic littoral cells or venous sinus-lining cells (Rosso et al. 1995, 1996; Johnson et al. 2007; Kranzfelder et al. 2012; Larsen et al. 2013). The tumors can be divided into splenic littoral cell angioma (SLCA), splenic littoral cell hemangioendothelioma (SLCH), and littoral cell angiosarcoma (SLCAS) (He et al. 2014).
SLCA is regarded as benign and usually occurs in adults without gender predilection. The solitary or multiple nodules can cause significant asymptomatic or symptomatic splenomegaly. Multiple nodules are found in 85 % of cases. SLCA can occur with concomitant visceral malignancies, such as colorectal cancer, pancreatic carcinoma, renal cell carcinoma, urologic cancer, ovarian cancer, and lung carcinomas, and was also observed in association with melanoma and lymphoma. SLCH shows a protracted course (Ben-Izhak et al. 2001) and can behave in a low-grade malignant manner. SLCAS exists as low- and high-grade malignancy lesions (Rosso and Paulli 2004). Histologically, littoral cell vascular tumors are composed of a network of ectatic blood-filled channels lined by plump, bland, or atypical cells that may form intraluminal papillary fronds and show erythrophagocytosis. There seems to be a transition from littoral cell angioma to low-grade malignant forms (Fernandez et al. 2006). Immunohistochemically, the littoral tumor cells are reactive for CD31, CD68, CD21, and CD163 but negative for CD34 . This unique cell therefore expresses both endothelial and macrophage/histiocyte markers (Fernandez et al. 2006; Larsen et al. 2013). Littoral cells or splenic venous sinus-lining cells highly express the formin homology domain protein 1, the red blood cell Duffy antigen receptor for chemokines, CD8 a/a, and SIRPa (CD172a).
Liver Involvement in Littoral Cell Hemangioendothelioma and Littoral Cell Angiosarcoma
Both SLCH and SLCAS can metastasize to the liver (Fernandez et al. 2006; Wang et al. 2013; He et al. 2014). In SLCH, two forms have been shown to metastasize to the liver, a more common typical hemangioendothelioma with nuclear atypia and necrosis, and an uncommon variant with bland, plump cells (Fernandez et al. 2006). Most cases of SLCAS metastasizing to the liver form metastatic nodular masses, but diffuse spread to the liver is also known. Specifically, low-grade SLCAS can spread to the liver with a diffusely infiltrating pattern (Larsen et al. 2013). SLCH and SLCAS metastasizing to the liver show the same histology and immunohistochemical phenotype as the primary splenic tumors.
Hepatic Hemangioendothelioma with Epithelioid Morphology and Eosinophilia
Introduction
Vascular tumors are characterized by an epithelioid phenotype of endothelial cells from a complex group of neoplasms with a broad spectrum of biologic behavior, ranging from benign to potentially malignant and frankly malignant (the family of epithelioid vascular tumors; Tsang and Chan 1993). The most common epithelioid vascular tumor of the liver is epithelioid hemangioendothelioma (HEHE), but there are few lesions with an epithelioid phenotype that deviate from the features of HEHE. Hepatic hemangioendothelioma with epithelioid morphology and eosinophilia is a very rare example of such unusual vascular liver tumors.
Clinical Features
As described in the original report (Kimura et al. 2006), a 33-year-old man was found to have hepatosplenomegaly, an itchy eczematous rash scattered on the trunk and the extremities, marked peripheral blood eosinophilia, markedly elevated IgE serum levels, and an increased serum IL-5. A bone marrow biopsy showed a hypercellular hemopoietic tissue with increased eosinopoiesis but without signs of malignancy. No chromosomal anomalies were detected in marrow cells. Liver biopsy revealed an eosinophil infiltrated and a vascular proliferation characterized by well-formed blood vessels lined with plump endothelial cells (positive for CD31 and factor VIII-associated antigen but not for CD34) with eosinophilic cytoplasm and a large vesicular nucleus. Steroid therapy improved the skin lesions and hydroxyurea normalized eosinophilia, but 1 year after diagnosis, liver failure ensued causing death.
Pathology
Autopsy revealed massive hepatomegaly (4,160 g) and ill-defined multiple spongy lesions scattered throughout the liver. In addition, nodular gray to white areas, 2–6 cm in diameter, were observed in this organ.
Microscopically, the lesions were composed of vascular proliferations with epithelioid endothelial cells as already seen in the liver biopsy. A part of these endothelial cells had a vacuolated cytoplasm. Dilated vascular channels and solid areas with few vascular spaces were noted.
The histologic phenotype somewhat resembles other vascular proliferations with an inflammatory response, encompassing such entities as angiolymphoid hyperplasia with eosinophilia (ALHE), inflammatory angiomatous nodules, atypical pyogenic granuloma, histiocytoid hemangioma, and Kimura’s disease.
References
Achauer BM, Chang CJ, Vander Kam VM (1997) Management of hemangioma of infancy: review of 245 patients. Plast Reconstr Surg 99:1301–1308
Adam YG, Huvos AG, Fortner JG (1970) Giant hemangiomas of the liver. Ann Surg 172:239–245
Albrecht S, Kahn HJ (1990) Immunohistochemistry of intravascular papillary endothelial hyperplasia. J Cutan Pathol 17:16–21
Al-Kaabi A, Yanofsky R, Bunge M, Hyman J, Rafay MF (2009) Diffuse hemangiomatosis with predominant central nervous system involvement. Pediatr Neurol 40:54–57
Aschl G, Wallner M, Tuppy H, Frohler W, Kramar R (1999) Angioleiomyoma of the gallbladder: a rare cause of hemobilia in a patient on dialysis (in German). Dtsch Med Wochenschr 124:13–16
Aulicino MR, Kaneko M, Uinger PD (1995) Excessive endothelial cell proliferation occurring in an organizing thyroid hematoma: report of a case and review of the literature. Endocr Pathol 6:153–158
Bakaris S, Karabiber H, Yuksel M, Parmaksiz G, Kiran H (2004) Case of large placental chorioangioma associated with diffuse neonatal hemangiomatosis. Pediatr Dev Pathol 7:258–261
Bargon G, Yu D (1968) Diffuse hemangiomatosis of the skeleton, liver, kidney and soft tissues (in German). Fortschr Geb Röntgenstr Nuklearmed 109:805–808
Barresi V, Vitarelli E, Branca G, Antonelli M, Giangaspero F, Barresi G (2012) Expression of brachyury in hemangioblastoma: potential use in differential diagnosis. Am J Surg Pathol 36:1052–1057
Basten SG, Willekers S, Vermaat JS, Slaats GG, Voest EE, van Diest PJ, Giles RH (2013) Reduced cilia frequencies in human renal cell carcinomas versus neighboring parenchymal tissue. Cilia 2:2
Beissert M, kenn W, Schultz G, Keberle M, Eck M, Hahn D (2002) Hepatic angiomyoma: CT and MRI findings. Abdom Imaging 27:40–42
Ben-Izhak O, Bejar J, Ben-Eliezer S, Vlodavsyl E (2001) Splenic littoral cell haemangioendothelioma: a new low-grade variant of malignant littoral cell tumour. Histopathology 39:469–475
Berman B, Lim H (1978) Concurrent cutaneous and hepatic hemangiomata in infancy: report of a case and a review of the literature. J Dermatol Surg Oncol 4:869–873
Bezold K (1951) A case of disseminated bone hemangiomatosis (in German). Fortschr Geb Röntgenstr 75:636–641
Blondet A, Ridereau-Zins C, Michalak S, Pessaux P, Aubertin A, Aubé C (2007) Multiple pedunculated liver hemangiomas presenting with volvulus (in French). J Radiol 88:891–894
Böhm N, Behrens R, Imm W, Nöldge G (1980) Generalized hemangiomatosis. A hamartoma-like malformation of the vascular system with poor prognosis (in German). Med Welt 31:1291–1294
Boyle WJ (1972) Cystic angiomatosis of bone. A report of three cases and review of the literature. J Bone Joint Surg 54:626–636
Brunzell JD, Shankle SW, Bethune JE (1968) Congenital generalized lipodystrophy accompanied by cystic angiomatosis. Ann Intern Med 69:501–516
Chen S, Sanford CA, Sun J, Choi V, Van Dyke T, Samulski RJ, Rathmell WK (2010) VHL and PTEN loss coordinate to promote mouse liver vascular lesions. Angiogenesis 13:59–69
Clayer M (2002) Skeletal angiomatosis in association with gastrointestinal angiodysplasia and paraproteinemia: a case report. J Orthop Surg (Hong Kong) 10:85–88
Clearkin KP, Enzinger FM (1976) Intravascular papillary endothelial hyperplasia. Arch Pathol Lab Med 100:441–444
Corless CL, Kibel AS, Iliopoulos O, Kaelin WG (1997) Immunostaining of the von Hippel-Lindau gene product in normal and neoplastic human tissues. Hum Pathol 28:459–464
Crespo Uriguen M, Martinez Torres D, Miyar Gonzalez A (1988) Diffuse giant cavernous hemangioma of the liver: apropos of 2 cases 8 (in Spanish). Rev Esp Enferm Apar Dig 73:289–292
Del Rio E, Aguilar A, Sanchez Yus E (1992) Intravascular papillary endothelial hyperplasia: a reorganizing thrombus. Int J Dermatol 31:713–714
Deveci M, Inan N, Corapcioglu F, Ekingen G (2011) Gorham-Stout syndrome with chylothorax in a six-year-old boy. Indian J Pediatr 78:737–739
Dickie B, Dasgupta R, Nair R, Alonso MH, Ryckman FC, Tiao GM, Adams DM, Aizikhan RG (2009) Spectrum of hepatic hemangiomas: management and outcome. J Pediatr Surg 44:125–133
Edlow BL, Burnett MG, Belasco J, Marcotte PJ, D’Angio G, Furth EE (2006) Recurring polysomatic hemangiomatosis: a new syndrome? J Pediatr Hematol Oncol 28:471–475
Elorza A, Soro-ARnaiz I, Melendez-Rodriguez F, Rodriguez-Vaello V, Marsboom G et al (2012) HIF2a acts as an mTORC1 activator through the amino acid carrier SLC7A5. Mol Cell 48:681–691
Enjolras O, Mulliken JB (1998) Vascular tumors and vascular malformations (new issues). Adv Dermatol 13:375–422
Erdogan B, Sen O, Aydin VM, Yildirim T, Birçan S, Altinors N (2003) Multi-organ cavernous hemangiomas: case report. Neurol Res 25:92–94
Eusebi V, Fanti PA, Fedeli F, Mancini AM (1980) Masson’s intravascular vegetant hemangioendothelioma. Tumori 66:489–498
Evans AJ, Russell RC, Roche O, Burry TN, Fish JE, Chow VW, Kim WY, Saravanan A et al (2007) VHL promotes E2 box-dependent E-cadherin transcription by HIF-mediated regulation of SIP1 and snail. Mol Cell Biol 27:157–169
Falconieri G, Mirra M, Michal M, Suster S (2013) Hemangioblastoma-like clear cell stromal tumor of the lung. Adv Anat Pathol 20:130–135
Falk S, Stutte HJ, Frizzera G (1991) Littoral cell angioma. A novel splenic vascular lesion demonstrating histiocytic differentiation. Am J Surg Pathol 15:1023–1033
Fernandez Jimenez I, Alvarez Muñoz V, Pelaez Mata D, Diaz Blanco M, Galbe Sada M et al (2000) Cystic angiomatosis (in Spanish). Ann Esp Pediatr 52:389–391
Fernandez S, Cook GW, Arber DA (2006) Metastasizing splenic littoral cell hemangioendothelioma. Am J Surg Pathol 30:1036–1040
Feurle GE (1990) Arteriovenous shunting and cholestasis in hepatic hemangiomatosis associated with metoclopramide. Gastroenterology 99:258–262
Fischer C, Roeckl H (1961) A case of systemized hemangiomatosis (in German). Hautarzt 12:79–82
Frangides C, Kounis NG, Papadaki PJ, Goudevenos J, Zavras GM (1995) Diffuse hepatic haemangiomatosis in the elderly. Br J Clin Pract 49:215–216
Frieden IJ, Reese V, Cohen D (1996) PHACE syndrome. The association of posterior fossa brain malformations, hemangiomas, arterial anomalies, coarctation of the aorta and cardiac defects and eye abnormalities. Arch Dermatol 132:307–311
Glick ZR, Frieden IJ, Garzon MC, Mully TW, Drolet BA (2012) Diffuse neonatal hemangiomatosis: an evidence-based review of case reports in the literature. J Am Acad Dermatol 67:898–903
Golitz LE, Rudikoff J, O’Meara OP (1986) Diffuse neonatal hemangiomatosis. Pediatr Dermatol 3:145–152
Gonzalez-Flores A, Aguilar-Quesada R, Siles E, Pozo S, Rodriguez-Lara MI, Lopez-Jimenez L et al (2014) Interaction between PARP-1 and HIF-2a in the hypoxic response. Oncogene 33:891–898
Gordin et al. 1975 PubMed PMID 128276
Gorham LW, Wright AW, Shultz HH, Maxon FC (1954) Disappearing bone: a rare form of massive osteolysis. Report of two cases, one with autopsy finding. Am J Med 17:674–682
Gottschling S, Schneider G, Meyer S, Reinhard H, Dill-Mueller D, Graf N (2006) Two infants with life-threatening diffuse neonatal hemangiomatosis treated with cyclophosphamide. Pediatr Blood Cancer 46:239–242
Gouedard C, Dupé-Goetghebeur D, Gagneur A, Sannier K, Misery L (2007) Neonatal haemangiomatosis in identical twins with twin-twin transfusion syndrome (in French). Ann Dermatol Venereol 134:863–866
Guzman-Valdivia Gomez G, Lazaro-Martinez VM, Aguilar-Cruz E, Kuri-Osorio J, Zaga-Minian I (2006) Case study of diffuse hemangiomatosis of the liver (in Spanish). Gac Med Mex 142:341–344
Haase VH (2009) The VHL tumor suppressor: master regulator of HIF. Curr Pharm Des 15:3895–3903
Haase VH, Glickman JN, Socolovsky M, Jaenisch R (2001) Vascular tumors in livers with targeted inactivation of the von Hippel-Lindau tumor suppressor. Proc Natl Acad Sci U S A 98:1583–1588
Hachisuga T, Hashimoto H, Enjoji M (1984) Angioleiomyoma. A clinicopathologic reappraisal of 562 cases. Cancer 54:126–130
Haggstrom AN, Garzon MC, Baselga E, Chamlin SL, Frieden IJ, Holland K, Maguiness S et al (2010) Risk for PHACE syndrome in infants with large facial hemangiomas. Pediatrics 126:e418–e426
Hashimoto H, Daimaru Y, Enjoji M (1983) Intravascular papillary endothelial hyperplasia: a clinicopathologic study of 91 cases. Am J Dermatopathol 5:539–546
Hayasaka K, Tanaka Y, Satoh T, Mutoh H (1999) Hepatic hemangioblastoma: an unusual presentation of von Hippel-Lindau disease. J Comput Assist Tomogr 23:565–566
He P, Yan XD, Wang JR, Guo RC, Zhang HB (2014) Splenic littoral cell hemangioendothelioma: report of a case with hepatic metastases and review of the literature. J Clin Ultrasound 42:308–312
Heim S, Mandahl N, Kristoffersson U, Mitelman F, Rööser B, Rydholm A, Willén H (1986) Structural chromosome aberrations in a case of angioleiomyoma. Cancer Genet Cytogenet 20:325–330
Hennig Y, Caselitz J, Stern C, Barnitzke S, Bullerdiek J (1999) Karyotype evolution in a case of uterine angioleiomyoma. Cancer Genet Cytogenet 108:79–80
Henschen P (1932) L’endovasculite proliférante thrombopoétique dans la lésion vasculaire locale. Ann Anat Pathol 9:113–121
Ho V, Krol A, Bhargava R, Osiovich H (2000) Diffuse neonatal haemangiomatosis. J Paediatr Child Health 36:286–289
Holden KR, Alexander F (1970) Diffuse neonatal hemangiomatosis. Pediatrics 46:411–421
Hong SG, Cho HM, Chin HM, Park IY, Yoo JY, Hwang SS, Kim JG, Park WB, Chun CS (2004) Intravascular papillary endothelial hyperplasia (Masson’s hemangioma) of the liver: a new hepatic lesion. J Korean Med Sci 19:305–308
Huang JS, Lin CM, Cheng YC, Hung KL, Chien CC, Chen CK, Chang CJ, Chen CW et al (2009) A vitronectin M381T polymorphism increases risk of hemangioblastoma in patients with VHL gene defect. J Mol Med (Berl) 87:613–622
Hurvitz et al 2000 PubMed PMID 11132222
Ishida T, Dorfman HD, Steiner GC, Norman A (1994) Cystic angiomatosis of bone with sclerotic changes mimicking osteoblastic metastases. Skelet Radiol 23:247–252
Jaakkola PM, Rantanen K (2013) The regulation, localization, and functions of oxygen-sensing prolyl hydroxylase PHD3. Biol Chem 394:449–457
Jacobs JE, Kimmelstiel P (1953) Cystic angiomatosis of the skeletal system. J Bone Joint Surg Am 35(A2):409–420
Jayanthi V, Shankar TR, Ravindran C, Sudalaimuthu S, Chandrasekar TS (2000) Diffuse hepatic hemangiomatosis: case report. Trop Gastroenterol 21:188–189
Jhaveri KS, Vlachou PA, Guindi M, Fischer S, Khalili K, Cleary SP, Ayyappan AP (2011) Association of hepatic hemangiomatosis with giant cavernous hemangioma in the adult population: prevalence, imaging appearance, and relevance. AJR Am J Roentgenol 196:809–815
Johnson C, Goyal M, Kim B, Wasdahl D, Nazinitsky K (2007) Littoral cell angioma. Clin Imaging 31:27–31
Jung TY, Jung S, Lee MC, Kim IY, Kang SS, Kim SH (2005) Papillary endothelial hyperplasia associated with repeated bleeding. Br J Neurosurg 19:428–431
Kan CD, Yae CT, Yang YJ (2004) Left ventricular haemangioma with papillary endothelial hyperplasia and liver involvement. Heart 90:e49
Kane RC, Newman AB (1973) Diffuse skeletal and hepatic hemangiomatosis. Calif Med 118:41–44
Katenkamp D, Kosmehl H, Langbein L (1988) Angiomyoma. A pathologo-anatomic analysis of 229 cases (in German). Zentralbl Allg Pathol 134:423–433
Kim EH, Park SY, Ihn YK, Hwang SS (2008) Diffuse hepatic hemangiomatosis without extrahepatic involvement in an adult patient. Korean J Radiol 9:559–562
Kimura T, Mukai M, Kaneko Y, Hirakata M, Okamoto S, Sakamoto M, Okada Y, Ikeda Y (2006) Unusual hemangioendothelioma of the liver with epithelioid morphology associated with marked eosinophilia: autopsy case. Pathol Int 56:694–701
Kiriyama K, Yabu M, Taniguti M, Katou T, Manabe N, Matusima N, Himeno S (2001) A case of giant hepatic hemangiomas which associated with skeletal hemangiomas (in Japanese). Nihon Shokakibyo Gakkai Zasshi 98:1362–1367
Körster R, Jansen H (1981) Diffuse skeletal hemangiomatosis with involvement of internal organs (in German). Röfo 134:69–74
Kortmeyer AO, Falke EA, Gläsker S, Li J, Oldfield EH (2013) Nervous system involvement in von Hippel-Lindau disease: pathology and mechanisms. Acta Neuropathol 125:333–350
Kranzfelder M, Bauer M, Richter T, Rudelius M, Huth M, Wagner P, Friess H, Stadler J (2012) Littoral cell angioma and angiosarcoma of the spleen: report of two cases in siblings and review of the literature. J Gastrointest Surg 16:863–867
Langner C, Thonhofer R, Hegenbarth K, Trauner M (2001) Diffuse hemangiomatosis of the liver and spleen in an adult (in German). Pathologe 22:424–428
Langsteger W, Lind P, Költringer P, Eber O (1990) An unusual case of hepatic hemangiomatosis: sonographic, CT, and 99m-Tc-RBC findings. AJR Am J Roentgenol 143:423
Larcher VF, Howard ER, Mowat AP (1981) Hepatic haemangiomata: diagnosis and management. Arch Dis Child 56:7–14
Larsen BT, Bishop MC, Hunter GC, Renner SW (2013) Low-grade, metastasizing splenic littoral cell angiosarcoma presenting with hepatic cirrhosis and splenic artery aneurysm. Int J Surg Pathol 21:618–626
Latifi HR, Siegel MJ (1992) Diffuse neonatal hemangiomatosis: CT findings in an adult. J Comput Assist Tomogr 16:971–973
Lee SH, Park BJ, Kim TS, Lim YJ (2010) Long-term follow-up clinical courses of cerebellar hemangioblastoma in von Hippel-Lindau disease: two case reports and a literature review. J Korean Neurosurg Soc 48:263–267
Lehmann FS, Beglinger C, Schnabel K, Terracciano L (1999) Progressive development of diffuse liver hemangiomatosis. J Hepatol 30:951–954
Longano AB, Beech PA, Nelva P (2010) P16 staining of subcutaneous smooth muscle tumours. Pathology 42:173–174
Lopriore E, Markhorst DG (1999) Diffuse neonatal haemangiomatosis: new views on diagnostic criteria and prognosis. Acta Paediatr 88:93–97
Lutz MS, Burk RD (2006) Primary cilium formation requires von Hippel-Lindau gene function in renal-derived cells. Cancer Res 66:6903–6907
Ma D, Zhang M, Chen L, Tang Q, Tang X, Mao Y, Zhou L (2011) Hemangioblastomas might derive from neoplastic transformation of neural stem cells/progenitors in the specific niche. Carcinogenesis 32:102–109
Maher ER, Neumann HP, Richard S (2011) Von Hippel-Lindau disease: a clinical and scientific review. Eur J Hum Genet 19:617–623
Malik R, Malik R, Tandon S, Tandon P (2008) Skeletal angiomatosis – rare cause of bone destruction: a case report with review of the literature. Indian J Pathol Microbiol 51:515–518
Masson P (1923) Hémangioendothéliome végétant intravasculaire. Bull Soc Anat Paris 93:517–523
McGrath FP, Gibney RG, Morris DC, Owen DA, Erb SR (1992) Case report: multiple hepatic and pulmonary haemangioblastomas – a new manifestation of von Hippel-Lindau disease. Clin Radiol 45:37–39
Maeda et al. 1981 PubMed PMID 7234417
Meadows MC, Sun X, Dardik M, Tarantino DR, Chamberlain RS (2010) Intraabdominal intravascular papillary endothelial hyperplasia (Masson’s tumor): a rare and novel cause of gastrointestinal bleeding. Case Rep Gastroenterol 4:124–132
Melis M (1954) Hemangiomatosis of the liver with voluminous angiocavernoma; anatomicopathological study (in Italian). Arch Ital Anat Istol Patol 26:520–530
Mendiratta V, Anand R, Chander R, Harjai B, Gupta T (2008) Multiple neonatal haemangiomatosis with liver hemangiomas and anaemia. Australas J Dermatol 49:42–43
Merrill MJ, Edwards NA, Lonser RR (2013) Hemangioblastoma-associated mast cells in von Hippel-Lindau disease are tumor derived. Blood 121:859–860
Metcalf JL, Bradshaw PS, Komosa M, Greer SN, Stephen Meyn M, Ohh M (2013) K63-ubiquitylation of VHL by SOCs1 mediates DNS double-strand break repair. Oncogene 33:1055–1065
Metry DW, Dowd CF, Barkovich AJ, Frieden IJ (2001) The many faces of PHACE syndrome. J Pediatr 139:117–123
Metry DW, Hawrot A, Altman C, Frieden IJ (2004) Association of solitary, segmental hemangiomas of the skin with visceral hemangiomatosis. Arch Dermatol 140:591–596
Mihalche C, Dumitrache D (2004) Diffuse hepatic hemangiomatosis – case report (in Romanian). Rev Med Chir Soc Med Nat Iasi 108:366–368
Möller G, Priemel M, Amling M, Werner M, Kuhlmey AS, Delling G (1999) The Gorham-Stout syndrome (Gorham’s massive osteolysis). J Bone Joint Surg 81:501–506
Montgomery SP, Guillot AP, Barth RA (1990) MRI of disseminated neonatal hemangiomatosis: case report. Pediatr Radiol 20:204–205
Moon WS, Yu HC, Lee JM, Kang MJ (2000) Diffuse hepatic hemangiomatosis in an adult. J Korean Med Sci 15:471–474
Mulliken et al. 2007 PubMed PMID 17845155
Myllyharju J, Koivunen P (2013) Hypoxia-inducible factor prolyl 4-hydroxylases: common and specific roles. Biol Chem 394:435–448
Nakayama H, Enzan H, Miyazaki E, Kuroda N, Toi M (2002) Lack of CD34 positive stromal cells within angiomyomas (vascular leiomyomas). J Clin Pathol 55:395–396
Nishio J, Iwasaki H, Ohjimi Y, Ishiguro M, Kobayashi K, Nabeshima K, Naito M, Kikuchi M (2004) Chromosomal imbalances in angioleiomyomas by comparative genomic hybridization. Int J Mol Med 13:13–16
Nord KM, Kandel J, Lefkowitch JH, Lobritto SJ, Morel KD, North PE, Garzon MC (2006) Multiple cutaneous infantile hemangiomas associated with hepatic angiosarcoma: case report and review of the literature. Pediatrics 118:e907–e913
Ohnishi S, Miyagishima T, Nakagawa M, Kamata T, Kishimoto A, Choi GH, Kudo M, Okabe M (2002) Diffuse neonatal hemangiomatosis without cutaneous lesions in an adult – a case report. Angiology 53:235–237
Ozakyol A, Kebapci M (2006) Enhanced growth of hepatic hemangiomatosis in two adults after postmenopausal estrogen replacement therapy. Tohoku J Exp Med 210:257–261
Park DM, Zhuang Z, Chen L, Szerlip N, Maric I, Li J, Sohn T, Kim SH, Lubensky IA et al (2007) Von Hippel-Lindau disease-associated hemangioblastomas are derived from embryologic multipotent cells. PLoS Med 4:e60
Patil M, Pabla N, Huang S, Dong Z (2013) Nek1 phosphorylates Von Hippel-Lindau tumor suppressor to promote its proteasomal degradation and ciliary destabilization. Cell Cycle 12:166–171
Pavanello M, Piatelli G, Ravegnani M, Consales A, Rossi A, Nozza P, Milanaccio C et al (2007) Cystic angiomatosis of the craniocervical junction associated with Chiari I malformation: case report and review of the literature. Childs Nerv Sys 23:697–700
Pavlenishvili IV, Nemsadze KP (1978) Disseminated hemangiomatosis of the liver in a newborn infant (in Russian). Vopr Okhr Materin Det 23:85–87
Pientka FK, Hu J, Schindler SG, Brix B, Thiel A, Jöhren O, Fandrey J, Berchner-Pfannschmidt U et al (2012) Oxygen sensing by the prolyl-4-hydroxylase PHD2 within the nuclear compartment and the influence of compartmentalisation on HIF-1 signalling. J Cell Sci 125:5168–5176
Pins MR, Rosenthal DI, Springfield DS, Rosenberg AE (1993) Florid extravascular papillary endothelial hyperplasia (Masson’s pseudoangiosarcoma) presenting as a soft-tissue sarcoma. Arch Pathol Lab Med 117:259–263
Platokouki H, Aronis S, Mitsika A, Keramidas D, Harokopos E (1998) Diffuse splenic and visceral hemangiomas complicated by chronic consumption coagulopathy. Acta Paediatr Jpn 40:381–384
Poetke M, Jamil B, Muller U, Berlien HP (2002) Diffuse neonatal hemangiomatosis associated with Simpson-Golabi-Behmel syndrome: a case report. Eur J Pediatr Surg 12:59–62
Popa G, Ambarus V, Dolinescu C, Daniil C, Ungureanu E, Cosma M (1984) Diffuse hepatic hemangioma associated with secondary polycythaemia. Rev Med Chir Soc Med Nat Iasi 88:375–377
Pulido-Zamudio T, Orr W, Lertzman M (2001) Cystic angiomatosis of the bone appearing as intrathoracic lung masses. Can Respir J 8:187–190
Ramesh P, Annapureddy SR, Khan F, Sutaria PD (2004) Angioleiomyoma: a clinical, pathological and radiological review. Int J Clin Pract 58:587–591
Rankin EB, Tomaszewski JE, Haase VH (2006) Renal cyst development in mice with conditional inactivation of the von Hippel-Lindau tumor suppressor. Cancer Res 66:2576–2583
Reed CN, Cooper PH, Swerlick RA (1984) Intravascular papillary endothelial hyperplasia. Multiple lesions simulating Kaposi’s sarcoma. J Am Acad Dermatol 10:110–113
Reid AB, Reid IL, Johnson G, Hamonic MM, Major P (1989) Familial diffuse cystic angiomatosis of bone. Clin Orthop Relat Res 238:211–218
Reynoso-Roldan A, Roldan M, Cancino-Diaz JC, Rodriguez-Martinez S, Cancino-Diaz ME (2012) Vascular endothelial growth factor production is induced by histone deacetylase 1 and suppressed by von Hippel-Lindau protein in HaCaT cells. Clin Invest Med 35:E340–E350
Ribback S, Thiele A, Rosenberg C, Friesecke S, Neumann V, Tannapfel A, Dombrowski F (2011) Nodular hemangiomatosis of pleura and peritoneum. Pathol Res Pract 207:718–721
Ritchie G, Zeier FG (1956) Hemangiomatosis of the skeleton and spleen. J Bone Joint Surg 38:115
Rizza V, Coletti G, Di Cocco P, Mazzotta C, Famulari A, Pisani F (2009) Serious renal hemorrhage in Masson tumor. Transplant Proc 41:1402–1404
Robinson D, Hambleton G (1977) Cutaneous and hepatic haemangiomata. Arch Dis Child 52:155–157
Rojiani AM, Owen DA, Berry K, Woodhurst B, Anderson FH, Scudamore CH, Erb S (1991) Hepatic hemangioblastoma. An unusual presentation in a patient with von Hippel-Lindau disease. Am J Surg Pathol 15:81–86
Rolain G, Olive D, Marchal C, Leveau P, Hoeffel JC, Bretagne MC (1978) A radiological study of a case multiple liver and bone angiomas in an infant (in French). J Radiol Electrol Med Nucl 59:109–111
Rosso R, Paulli M (2004) Littoral cell angiosarcoma: a truly malignant tumor. Am J Surg Pathol 28:1255
Rosso R, Paulli M, Gianelli U, Boveri E, Stella G, Magrini U (1995) Littoral cell angiosarcoma of the spleen. Case report with immunohistochemical and ultrastructural analysis. Am J Surg Pathol 19:1203–1208
Rosso R, Gianelli U, Chan JK (1996) Further evidence supporting the sinus lining cell nature of splenic littoral cell angiosarcoma. Am J Surg Pathol 20:1531
Rotman M, John M, Stowe S, Inamdar S (1980) Radiation treatment of pediatric hepatic hemangiomatosis and coexisting cardiac failure. N Engl J Med 302:852
Schulze SM, Moser RL, Bhattacharyya N (2006) A rare case of diffuse neonatal hemangiomatosis. Am Surg 72:359–362
Segura-Sampedro JJ, Alamo-Martinez JM, Cañete-Gomez J, Suarez-Artacho G, Gonzalez-Canton JR et al (2012) Gallbladder leiomyoma in absence of immune system disorders: an unusual diagnosis. Rev Esp Enferm Dig 104:382–384
Sezgin S, Kotiloglu E, Kaya H, Inanli S (2005) Extravascular papillary endothelial hyperplasia of the larynx: a case report and review of the literature. Ear Nose Throat J 84:52–53
Shennan T (1914) Histologically non-malignant angioma, with numerous metastases. J Pathol Bacteriol 19:139
Shivaram GM, Pai RK, Ireland KB, Stevens KJ (2007) Temporal progression of skeletal cystic angiomatosis. Skelet Radiol 36:1199–1204
Shively SB, Falke EA, Li J, Tran MG, Thompson ER, Maxwell PH, Roessler E, Oldfield EH et al (2011) developmentally arrested structures preceding cerebellar tumors in von Hippel-Lindau disease. Mod Pathol 24:1023–1030
Soares et al. 2008 PubMed PMID 18929993
Sonobe H, Ohtsuki Y, Mizobuchi H, Toda M, Shimizu K (1996) An angiomyoma with t(X;10)(q22; q23.2). Cancer Genet Cytogenet 90:54–56
Steffen C (2003) The man behind the eponym: C.L. Pierre Masson. Am J Dermatopathol 25:71–76
Stern JK, Wolf JE, Jarratt M (1981) Benign neonatal hemangiomatosis. J Am Acad Dermatol 4:442–445
Stratte et al. 1996 PubMed PMID 8655722
Tarazov PG, Polysalov VN, Ryzhkov VK (1990) Hemangiomatosis of the liver and spleen: successful treatment with embolization and splenectomy. AJR Am J Roentgenol 155:1235–1236
Tarazov PG, Polysalov VN, Ryzhkov VK (1991) Hemangiomatosis of liver and spleen in a female patient: interventional radiologic and surgical treatment (in Russian). Vestn Rentgenol Radiol (1):71–73
Torres VM, Rodriguez FJ (1984) Kaposi’s sarcoma-like tumors due to intravascular papillary endothelial hyperplasia. Bol Assoc Med PR 76:223–226
Tsang WY, Chan JK (1993) The family of epithelioid vascular tumors. Histol Histopathol 8:187–212
Tsukagoshi H, Iwasaki Y, Toyoda M, Sato T, Takagi H, Mori M, Sasaki A, Kumakura H et al (1998) An autopsy case of systemic hemangiomatosis with honeycomb-like liver and focal splenic sarcomatous changes. Intern Med 37:847–852
van den Bosch J, Van Damme B, Baert A, Verwilghen RL (1975) Diffuse skeletal hemangiomatosis with visceral hemangiomas (in Dutch). Ned Tijdschr Geneeskd 119:1669–1674
Vanhoenacker FM, Schepper AM, Raeve H, Berneman Z (2003) Cystic angiomatosis with splenic involvement: unusual MRI findings. Eur Radiol 13(Suppl 4):L35–L39
Vilgrain V, Boulos L, Vullierme MP, Denys A, Terris B, Menu Y (2000) Imaging of atypical hemangiomas of the liver with pathologic correlation. RadioGraphics 20:379–397
Vorse HB, Smith EI, Luckstead EF, Fraser JJ (1983) Hepatic hemangiomatosis of infancy. Am J Dis Child 137:672–673
Vortmeyer AO, Frank S, Jeong SY, Yuan K, Ikejiri B, Lee YS, Bhowmick D, Lonser RR et al (2003) Developmental arrest of angioblastic lineage initiates tumorigenesis in von Hippel-Lindau disease. Cancer Res 63:7051–7055
Waldron RL, Zeller JA (1969) Diffuse skeletal hemangiomatosis with visceral involvement. J Can Assoc Radiol 20:119–123
Wallis LA, Asch T, Maisel BW (1964) Diffuse skeletal hemangiomatosis – report of two cases and review of literature. Am J Med 37:545–563
Wananukul S, Voramethkul W, Nuchprayoon I, Seksarn P (2006) Diffuse neonatal hemangiomatosis: report of 5 cases. J Med Assoc Thai 89:1297–1303
Wang L, Xiu D, Jiang B, Ma Z, Yuan C, Li L (2013) Simultaneous laparoscopic splenectomy and right hemihepatectomy for littoral cell angiosarcoma accompanied with liver metastases. World J Surg Oncol 11:215
Welborn J, Fenner S, Parks R (2010) Angioleiomyoma: a benign tumor with karyotype aberrations. Cancer Genet Cytogenet 199:147–148
Welten CM, Keats EC, Ang LC, Khan ZA (2012) Hemangioblastoma stromal cells show committed stem cell phenotype. Can J Neurol Sci 39:821–827
Witters I, Van Damme MT, Ramaekers P, Van Assche FA, Fryns JP (2003) Benign multiple diffuse neonatal hemangiomatosis after a pregnancy complicated by polyhydramnios and a placental chorioangioma. Eur J Obstet Gynecol Reprod Biol 106:83–85
Yavas GF, Okur N, Küsbeci T, Norman E, Inan U (2013) A case of von Hippel-Lindau disease with juxtapapillary retinal capillary hemangioma and nutcracker phenomenon. Int Ophthalmol 33:309–314
Yin WH, Li J, Chan JK (2012) Sporadic haemangioblastoma of the kidney with rhabdoid features and focal CD10 expression: report of a case and literature review. Diagn Pathol 7:39
Young RS, Zalneraitis EL, Bauman ML (1981) Disseminated neonatal hemangiomatosis: successful hepatic resection with subsequent development of hydrocephalus. J Pediatr Surg 16:752–753
Zeitlin H (1942) Hemangioblastomas of the meninges and their relation to Lindau’s disease. J Neuropathol Exp Neurol 1:14–23
Zeng ZJ, Johansson E, Hayashi A, Chavali PL, Akrap N, Yoshida T, Kohno K, Izumi H et al (2012) TLX controls angiogenesis through interaction with the von Hippel-Lindau protein. Biol Open 1:527–535
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this entry
Cite this entry
Zimmermann, A. (2017). Variants of Hepatobiliary Angiomatous Tumors. In: Tumors and Tumor-Like Lesions of the Hepatobiliary Tract. Springer, Cham. https://doi.org/10.1007/978-3-319-26956-6_50
Download citation
DOI: https://doi.org/10.1007/978-3-319-26956-6_50
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-26954-2
Online ISBN: 978-3-319-26956-6
eBook Packages: MedicineReference Module Medicine