
Abstract
Nurses are the largest group of health-care professionals in hospitals providing 24-h care to patients. Hence, nurses are pivotal in coordinating and communicating patient care information in the complex network of health-care professionals, services, and other care processes. Further, surveillance and timely interventions by nurses impact quality of care, reduce errors, and decrease health-care costs. Information communication technologies (ICTs) provide the capabilities to support many aspects of nursing care. However, within the context of acute nursing care, there is a lack of integrated technology solutions to support the complex interactions associated with nursing activities and thereby the delivery of high-quality and safe care. Generally, to date, the literature reports low levels of acceptance of ICT solutions by nurses. To address this, the following discussion serves to examine nurses’ acceptance of an integrated point-of-care solution for acute nursing contexts. The ICT was specifically designed to be sensitive to nurses’ needs with the expectation that this will lead to high levels of user acceptance. An evaluation of the acceptability of the proposed solution is presented using unified theory of acceptance and use of technology (UTAUT). Through the UTAUT lens, initial reactions of the participating nurses were examined. The findings provided us with feedback to redesign the solution to better fit with the dynamics and complexity of nursing care. The study has implications for theory, including using UTAUT in health-care contexts, and for practice, including recommendations for the design and development of ICT solutions suitable for nursing contexts.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
Introduction
Nurses are the largest group of health-care professionals in hospitals providing 24-h care to patients. Hence, nurses are pivotal in coordinating and communicating patient care information in the complex network of health-care professionals, services, and other care processes. Yet, despite nurses’ central role in health-care delivery, information communication technologies (ICTs) have historically rarely been designed around nurses’ operational needs. This could explain the poor integration of technologies into nursing work processes and consequent rejection by many nursing professionals (Rogers et al. 2013; Stevenson et al. 2010). The complex nature of acute care delivery in hospitals and the frequently interrupted patterns of nursing work suggest that nurses require flexible intelligent systems that can support and adapt to their variable workflow patterns. This study was designed to explore nurses’ initial reactions to a new integrated point-of-care solution for acute health-care contexts. The following reports on the first stage of a longitudinal project to use an innovative approach involving nurses in the development and refinement of this solution: from conceptualization to implementation. In this project, unified theory of acceptance and use of technology (UTAUT) was used to evaluate acceptance (Venkatesh et al. 2003).
Background
Given the advances of ICT solutions, it is reasonable to assume that it should be possible to design and develop suitable solutions to support nursing workflows in acute care contexts. It is essential that the design of such systems demonstrate high fidelity to nursing work and usability within real clinical work settings to increase the likelihood that they will be adopted by the expected end users, that is, nurses.
Information Technology Solutions and Nursing Practice
The complexities associated with the coordination, communication, and delivery of health care at the point of care present particular challenges for the design of information technology (IT) systems. In an Australia-wide qualitative study that examined nurses’ experiences of already established computerized patient information systems (CPIS), Darbyshire (2004) found that nurses often considered that these established systems made no “clinical sense” and were perceived to waste time. Overriding of the system, duplication of documentation, and a reversion to familiar systems such as paper recording have all been reported as work-around strategies used to continue delivery of safe and reliable clinical communication and care in the face of technological solutions that do not meet clinicians’ needs (Alaszewski 2005; Dowding et al. 2009; Lau et al. 2010; Viitanen et al. 2011).
Creating an ongoing collaborative process whereby nursing and IT industries both actively contribute to the development and sequential implementation of an intelligent tool for nursing work within health-care settings is proposed as a feasible, viable, and crucial solution.
Building Intelligent Systems Suited to Support Nursing Care
An intelligent system specifically designed for the discipline of nursing that can adequately and appropriately meet the requirements of nursing in terms of design and flexibility is challenging. Jennings et al. (2009) recommends that intelligent systems need to be designed to meet full epidemiological clinical and research needs of the clinical nurse. This idea is supported by suggestions that intelligent systems for nursing should encompass a set of standard elements directly related to the routine of everyday nursing practice (Yu et al. 2009; Yun-Ke et al. 2009). There is evidence that intelligent systems often address some of the needs of nursing care delivery, but fall short of supporting the full scope of nurses’ work in complex clinical settings: that is, the system doesn’t “think” like a nurse “thinks” (Yun-Ke et al. 2009).
Over more than 98 hours of nurses’ workflow patterns, Cornell et al. (2010a) observed that nurses often made important decisions about care delivery quickly and decisively; their workflow was often sporadic and chaotic in nature, incorporating a complex mix of patient and environmental data and clinical experience. They also discovered that the workflow patterns of nurses changed little after the introduction of technology. Indeed, the technology added an extra task (Cornell et al. 2010b).
Disparities between the clinical work of nursing and the effectiveness of intelligent systems in supporting that work are commonly reported. Issues such as responsiveness, reliability , and ease of use are often cited problems (Alaszewski 2005; Garg et al. 2005; Kawamoto et al. 2005; Yun-Ke et al. 2009). In addition, difficulties with security , maintenance, and confidentiality of patient records (Garg et al. 2005; Holden 2010; Viitanen et al. 2011; Weber et al. 2009) are often seen as barriers to the assimilation of a nursing information system into acute clinical contexts.
In pursuing the goal of a fully integrated e-health system in health care , it is useful for IT solutions to focus on nursing care as a central part of the communication and care processes that occur in acute care settings. The IT solution then needs to be sufficiently robust and flexible to be easily integrated into the multidisciplinary nature of care so that it is accepted as the “preferred” method of planning and documenting care across the health-care team (Oroviogoicoechea 2008). In the past, many IT applications have focused on aspects of nursing care delivery such as health records, medication administration, and decision-making, but few have managed to successfully integrate all of these processes into one all-encompassing system (Kowitlawakul 2011; Weber 2007). With a focus on patient-centered care, the notion of care being integrated across multidisciplinary teams has emerged as an important consideration that impacts patient safety and quality of care. Nurses are consistently the core of multidisciplinary health-care teams.
Understanding and applying a theory that is closely aligned to nursing practice and reflects the relativity of clinical application is essential to the success or failure of IT solutions (Turley 1996). Determinants such as interactional workability, relational integration, and skill set workability are clear factors in the success or failure of an intelligent nursing care system. This approach is based on the premise that if acceptance by nurses is obtained in the first instance, a “relative flow on” effect could lead to a wider acceptance by other members of the multidisciplinary health-care team.
Technology Acceptance
User adoption is a central theme in much of the information systems (IS) literature (see for example Rogers 2003; Venkatesh et al. 2003; Venkatesh et al. 2012) . This is primarily due to the fact that user adoption is used as a proxy for trying to determine a priori if a system will be successful or not. Given the amount of time and financial resources invested in so many IS/IT projects, not to mention the impact these systems have on critical service and business functions and the expectation that these projects will deliver significant benefits, it is understandable that user acceptance is an important early consideration.
Health care is now witnessing many initiatives to embrace IS/IT, including but not limited to diverse projects focused at designing and implementing various types of electronic medical records (EMRs), numerous e-health initiatives as well as the application of Web 2.0 in the form of personally controlled health-care records and patient portals. More recently, we are also observing the introduction of personal monitoring, mobile, and wireless devices. It is of particular importance in the health-care domain that such implementations are successful, first and foremost because ultimately a patient’s well-being may be at stake. In addition, health care in general is experiencing challenges regarding provision of cost-effective and high-quality services and treatments; hence, situations such as costly implementations of less than successful IS/IT solutions can have widespread detrimental effects .
To date, within the IS field, several models have been developed to examine the critical issue of user acceptance including theory of reasoned action (TRA), technology acceptance model (TAM/TAM2), theory of planned behavior (TPB), combined TAM and TPB, motivational model (MM), model of PC utilization (MPCU), social cognitive theory (SCT), and innovation and diffusion theory (IDT). However, as noted by Venkatesh et al. (2003), due to a need “…to integrate the fragmented theory and research on individual acceptance of information technology that captures the essential elements of eight previously established models,” they developed UTAUT , which we used as a conceptual model for our research .
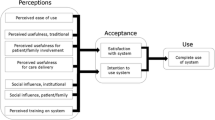
Succinctly stated, UTAUT proposes that four constructs; namely, performance expectancy (i.e., by using the technology, will this have a positive impact on performance/outcome?), effort expectancy (i.e., will using this technology require much effort on the user’s part?), social influence (i.e., is using this technology a socially acceptable activity?), and facilitating conditions (i.e., other benefits or positives that make using this technology positive) act as determinants of behavioral intentions and usage behaviors. In addition, there are four key moderator variables including: gender, age, experience, and voluntariness of use (Venkatesh et al. 2003).
Given that our interest was to examine what drives nurses to adopt a novel technology in acute care contexts, it was important to look closely at the role of nurses as it related to technology adoption and the workflow of activities and tasks they must perform.
Consequently, we focused on the following research question: “Based on various UTAUT dimensions, what are initial reactions of nurses to the proposed solution?” We contend that by answering this question it is possible to then better understand nurses’ requirements and improve their acceptance of new ICT solutions.
Research Approach
To answer the posed research question, a mixed method design was adopted for a clinical trial to critically examine nurses’ use of a novel information system called SW in acute care contexts (both surgical and medical wards), within a single hospital service in Melbourne, Australia. The following describes the key aspects of the research setting, data collection, and data analysis.
Research Setting
SW is a new ICT solution to support nursing work. It is a sophisticated, multifunctional technology designed to support nurses in documentation of the delivery of patient care by decreasing time spent by nurses on administrative tasks to allow direct patient care, create an electronic record of patient care delivery, reduce errors, and provide a positive enhancement to nurses’ work experience.
SW was tested with nurses working in two acute care wards (medical and surgical) using a three-stage project across two hospital sites of a large Victorian public health service over an 8-week period in 2013. Temporary implementation of the SW system at 4 beds in each ward was used to evaluate fidelity of the system to nursing work as well as usability and acceptability of the SW system to nurses. The test wards included a 25-bed general surgical ward with 32 regular nursing staff at Site A and a 32-bed general medical and neurology ward with 50 regular nursing staff at Site B. In stage 1, over a 2-week period, the SW system was installed and nurses were recruited and introduced to the system prior to implementation . Baseline workflow data were also collected during stage 1. In stage 2, SW was partially integrated into nursing care processes; during this stage, all nurses were invited to familiarize themselves with the SW system and they began to adopt it into care processes for patients in the selected beds. During this stage, issues of concern related to usability and risk were identified and subsequently modified by the developers prior to stage 3. The duration of this stage was 3 weeks. In stage 3, the SW system was used exclusively for documentation of nursing care delivery for selected patients by a small number of nurse “super users.” An UTAUT-based survey was distributed during stage 1. The primary research objective was to capture initial reactions to the system by the nurses participating in the trial.
Data Collection
The UTAUT-based survey reported in this chapter was conducted during the clinical trial. The surveys collected demographic data, responses to UTAUT items , and additional questions related to the training, support, and implementation of the SW system. This chapter reports findings related to nurses’ responses to 26 items addressing the five UTAUT constructs and four key moderator variables using a 7-point Likert scale (from 1 being totally disagree to 7 being totally agree). The items included:
-
Performance expectancy (PE), n = 8
-
Effort expectancy (EE), n = 4
-
Social influence (SI), n = 5
-
Facilitating conditions (FC), n = 4
-
Behavioral intentions (BI), n = 5. As the system was in a testing stage, only intention rather than actual use was included.
Overall contextual variables included:
-
Gender
-
Age
-
Experience
-
VU voluntariness, n = 3
A brief descriptive analysis of these variables is included below with the results for the interest of readers. The intention here was not to validate the UTAUT model nor predict the nurses’ behavioral intention but to describe and examine the constructs PE, EE, SI, FC and explore the impact of these constructs on BI.
Response rates are presented in Table 19.1:
Data Analysis
The survey data were entered into an Excel 2010 file. Duplicate and invalid records were removed prior to analysis leaving 38 complete responses. Data were then cleaned and imported into SPSS v22 and Excel for statistical analysis and data visualization. The following statistical analyses were conducted:
-
Descriptive analysis techniques were employed for each individual survey construct, particularly PE, EE, SI, FC, and BI.
-
Reliability analysis was conducted using Cronbach’s alpha to examine the internal consistency of the items included in the scale for each UTAUT construct.
-
Calculation of a composite score was used to summarize items with strong correlation with each other. Pearson Correlation was used to examine the strength of relationships between BI and each of the UTAUT constructs (PE, EE, SI, and FC). The intention of this chapter was not to predict BI, hence a regression analysis was not included in analyses. As a result of reliability analysis, FC3 was removed from the FC construct. This approach to data analysis using the UTAUT framework has been followed in previous studies (Heselmans et al. 2012; Wills et al. 2008) in the context of health care.
Findings
Gender, Age, Computer Skills, and Perceived Voluntariness of Use
Most (95 %) of the nurse respondents were female; only 2 out of the 38 respondents (5 %) were male. The mean age was 38 (95 % confidence interval for mean: 34.25–41.75, range: 23–58, median = 41.5, interquartile range (IQR): 27.75–42.25). Examination of the age distribution revealed large clusters: 38.2 % (n = 13) were younger than 30 and 29.4 % (n = 10) were aged between 41 and 45 years.
Most nurse participants rated their computer skills as average (52.6 %, n = 20) and above average (26.3 %, n = 10), and over half rated themselves as being comfortable or very comfortable with computers (52.6 %, n = 20; Figs. 19.1 and 19.2).

Computer skills and comfortable with computer use
Five of the voluntariness of use (VU) items refer to nurses’ perceptions about whether the SW system should be compulsory or not (VU1), and if they should be required (VU2) or expected (VU3) to use it (Table 19.2).

Voluntariness of use (VU)
Please see Table 19.2 for IQR and Fig. 19.2 for the data shapes. The distribution of the responses to these items is slightly to moderately positively skewed, indicating that nurses tended to disagree with the suggestion that the SW system should not be compulsory.
Performance Expectancy
Eight items comprised the PE construct. The first five of these items referred to users’ perceptions about key functionality of the SW system that included patient admission (PE1.1), planning and adhering to the care plan (PE1.2), ensuring continuity of care (PE1.3), patient discharge (PE1.4), and care evaluation (PE1.5). Three remaining items for this construct refer to users’ perceptions about how the system enables them to perform their tasks more quickly (PE2), increase their productivity (PE3), and provide a chance for career advancement (PE4).
Overall, all medians were between 4 (neutral) and 5 (slightly agree), see Table 19.3 for the IQR for each of the items. Examination of the distribution of responses shows that approximately one quarter of responses were neutral across all the PE items, except for PE1.1 where fewer (18.4 %, n = 7) responding nurses were neutral. Overall, nurses’ responses to the PE items suggest they were slightly positive in their perceptions about the usefulness of the system (see Figs. 19.3 and 19.4). A small number of nurses disagreed with the system’s usefulness across almost all the PE items. A notable proportion of the respondents reported extreme negative views in response to the items that “using SW would enable me to accomplish tasks more quickly (PE2; 15.8 %, n = 6) and improve my productivity” (PE3; 18.4 %, n = 7; see Table 19.3 and Fig. 19.4 for examples).

PE1.1 and PE1.2

PE3 and PE4
Summary
Overall responses suggest nurses were generally positive about the PE construct.
Effort Expectancy
The four items that comprise the EE construct address nurses’ perceptions about their interactions with the system (EE1), ease of becoming skillful (EE2), ease of use (EE3), and ease of learning to operate (EE4).
See Table 19.4 for the descriptive statistics summary of this construct. There was no totally disagree response to EE1 and EE2. The median was 5 in EE1, EE2, and EE3 and was 4.5 in EE4. The IQR was between neutral to strongly agree.
Around one in four of the responding nurses were neutral in EE1, EE2, and EE3. Close to one in three (31.6 %, n = 12) was neutral in ease of learning to operate (EE4). Most skeptical is EE3, easy to use, as almost one in four (cumulative 24.3 %, n = 9) disagreed to some degree (Fig. 19.5).

EE1 and EE3
Summary
Most of the responses regarding EE were positive, suggesting they perceived the SW system easy to learn, while few were skeptical about how easy it would be to learn to use.
Social Influence
The five SI items referred to perceived influences on nurses to use SW by other people (SI1), by people important to them (SI2), nurses’ perceived helpfulness of senior management (SI3), perceived helpfulness of other nurses (SI4), and hospital support for the use of the SW system (SI5). Overall, responses to these items were positive indicating SIs were present.
Examination of distributions reveal that the responses were centered around neutral and “slightly/moderately agree” (median: 5, IQR: 4–6). Responses to SI4 were most positive, suggesting nurses highly valued help from other nurses. A clear minority of responses were negative (Table 19.5).
Summary
Nurses were generally positive about SI and the helpfulness of other nurses (SI4) was most positively perceived by the respondents (Fig. 19.6).

SI2 and SI4
Facilitating Conditions
The four items used to examine facilitating conditions (FC) examined nurses’ perception about resources (FC1) and knowledge (FC2) necessary to use SW, whether SW is compatible with other systems (FC3), and the availability of assistance (FC4).

FC2 and FC4
Examination of the distribution shows that a clear minority of responses to FC1, FC2, and FC4 items were positive (see Table 19.6 and Fig. 19.7). Responses about the system’s compatibility with other systems in their hospital (FC3) was less positive (see mean, median, and IQR of this item in Table 19.6).
Summary
Nurses were generally positive about their knowledge, resources, and assistance to use the SW system. However, some were slightly skeptical that the system would be compatible with other systems in their hospital.
Behavioral Intentions
The five items that comprise the construct behavioral intentions (BI) refer to nurses’ intentions (BI1), prediction (BI2), planning (BI3) to use SW when it is introduced as well as perception about whether SW will help them reduce record-keeping time (BI4) and spend more time with patients (BI5) (Table 19.7, Fig. 19.8).

BI1 and BI4
Distribution of responses to BI1, BI2, and BI3 were skewed toward positive answers (5, 6, and 7). All their medians and modes were 6– showing half of the responses moderately or strongly agreed, and the most frequent responses were “moderately agree”. In comparison to BI1, BI2, and BI3, the responding nurses were found to be slightly less positive in regard to BI4 and BI5. Medians and modes were 5– “slightly agree”.
Summary
Overall, the responding nurses were moderately positive that they intend, predict, and plan to use the SW system when it is introduced to the hospital, whereas they were less positive in perceiving that the system would reduce their documentation time and enable them to have more time with patients.
Reliability of the Subscale Constructs
Despite the small sample, the Cronbach’s alpha coefficient was greater than 0.8 (over the acceptable level .07) indicating a high level of internal consistency between items within each construct (Table 19.8).
Correlations Between the Constructs (PE, EE, SI, and FC) and BI
Correlations between the construct subscales were examined revealing moderately positive and significant correlations between each of the constructs (PE, EE, SI, and FCFootnote 1) and BI (Table 19.9).
Hypotheses under examination include:
-
H1: There is no significant correlation between PE and BI.
-
H2: There is no significant correlation between EE and BI.
-
H3: There is no significant correlation between SI and BI.
-
H4: There is no significant correlation between FC and BI.
All p-value < 0.01; hence we can reject all the above hypotheses (that there is no significant correlation between each of the construct PE, EE, SI, and FC and BI). Hence, at the 0.01 significant level, there is statistical evidence for positive correlation between each of the constructs and BI.
While the above analysis suggests a positive correlation between each of the constructs and BI, this analysis does not predict the nurses’ BI based on the UTAUT constructs nor did it test the moderators (Fig. 19.9).

Scatter plots
Discussion and Conclusion
Nurses’ initial reactions to a novel technology, SW, were examined through the UTAUT lens . Overall, the nurses had slightly positive perceptions about PE, EE, and SI and moderately positive perception toward FC. These findings indicate that nurses intend, predict, and plan to use the SW system when it is introduced to the hospital. They reported slightly positive perceptions that the SW would reduce their documentation time and enable them to spend more time with patients.
The findings confirm positive correlations between each of the constructs (PE, EE, SI, FC) and BI as described in UTAUT (Venkatesh et al. 2003). The findings also support the use of the UTAUT tool to explore and plan nurse user requirements and evaluate their acceptance of innovative technology solutions and feedback to design. A subsequent analysis is underway to test whether age, gender, VU, and years of experience moderate the relationships between each of the independent variables (PE, EE, SI, FC) and the dependent variable BI.
The findings suggested redesigning the solution and developing an implementation plan to fit in with the dynamic and complex nursing care. Firstly, while nurses were found to be moderately positive in their intention to use the proposed system, they were less positive in perceiving the system’s usability. This suggests the importance of improving the system’s usability. Secondly, nurses perceived more strongly about peer support (other nurses being helpful—SI4) and were slightly/moderately positive with SI/FC respectively. This suggests the importance of peer support, training, and technical support during implementation and training.
Our study appears to indicate, then, that while the participating nurses expressed a generally positive view to the use of the SW technology in their nursing context, this may not translate directly into strong acceptance of the specific solution. Clearly, this was not the finding we were expecting; however, on closer examination, we note this is reflective of the general trend in practice with health care and technology use (Lau et al. 2010; Mills et al. 2013). Currently, we are witnessing a plethora of IS/IT solutions being adopted into health-care organizations, but these solutions all show poor user acceptance and oftentimes even have to be terminated (e.g., most notably the NHS Connecting for Health project). To address this issue, we recommend follow-up analyses and studies that include a mixed method approach and use qualitative techniques to assist in the uncovering of why acceptance might be low.
There are three key limitations in this study worthy of consideration. First, this was not an empirical validation of UTAUT (Venkatesh et al. 2003). Second, due to the complex nature of acute care wards and patient safety requirements, only a small number of nurses participated in the software trial. All these resulted in a small sample size of the acceptance surveys. Third, survey research by nature does not reveal a deep understanding of how and why behind the findings. A good response rate indicates a good level of interest in the participating nurses.
This chapter contributes to theory in a very important way. It suggests that conceptual models such as UTAUT need further extension of IS theory to facilitate a deeper understanding of the complex and dynamic nature of health care and the how and why of acceptance of specific solutions despite appearance of a general acceptance that IS/IT. For practice, the message is even stronger: user needs and requirements must be carefully considered when developing IS/IT solutions for health-care contexts. More research into how to better meet the demands of a multiple heterogeneous user system such as the dynamic and complex health-care environment is definitely needed.
Notes
- 1.
FC* was calculated without FC3.
References
Alaszewski, A. (2005). Risk, safety and organizational change in health care? Health, Risk & Safety, 7(4), 315–318.
Cornell, P., Herrin-Griffith, D., Keim, C., Petschonek, S., Sanders, A. M., D’Mello, S., Golden, T. W., & Shepherd, G. (2010a). Transforming nursing workflow, part 1: The chaotic nature of nurse activities. Journal of Nursing Administration, 40(9), 366–373. doi:310.1097/NNA.1090b1013e3181ee4261.
Cornell, P., Riordan, M., & Herrin-Griffith, D. (2010b). Transforming nursing workflow, part 2: The impact of technology on nurse activities. Journal of Nursing Administration, 40(10), 432–439. doi:410.1097/NNA.1090b1013e3181f1092eb1093f.
Darbyshire, P. (2004). ‘Rage against the machine?’: Nurses’ and midwives’ experiences of using computerized patient information systems for clinical information. Journal of Clinical Nursing, 13(1), 17–25.
Dowding, D., Mitchell, N., Randell, R., Foster, R., Lattimer, V., & Thompson, C. (2009). Nurses’ use of computerised clinical decision support systems: A case site analysis. Journal of Clinical Nursing, 18(8), 1159–1167. doi:10.1111/j.1365-2702.2008.02607.x.
Garg, A. X., Adhikari, N. K. J., McDonald, H., Rosas-Arellano, M. P., Devereaux, P. J., Beyene, J., Sam, J., & Haynes, R. B. (2005). Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: A systematic review. Journal of the American Medical Association, 293(10), 1223–1238.
Heselmans, A., Aertgeerts, B. P. D., Geens, S., Van de Velde, S., & Ramaekers, D. (2012). Family physicians’ perceptions and use of electronic clinical decision support during the first year of implementation. Journal of Medical Systems, 36(6), 3677–3684. doi:10.1007/s10916-012-9841-3.
Holden, R. J. (2010). Physicians beliefs about using EMR and CPOE: In pursuit of a contextualized understanding of health IT use behavior. International Journal of Medical Informatics, 79(2), 71–80. doi:10.1016/j.ijmedinf.2009.12.003.
Jennings, J. M., Stover, J. A., Bair-Merritt, M. H., Fichtenber, C., Munoz, M. G., Maziad, R., Ketemepi, S. J., & Zenilman, J. (2009). Identifying challenges to the integration of computer-Based surveillance information systems in large city health department: A case study. Public Health Reports, 124(2), 39–48.
Kawamoto, K., Houlihan, C. A., Balas, E. A., & Lobach, D. F. (2005). Improving clinical practice using clinical decision support systems: A systematic review of trials to identify features critical to success. BMJ, 330(7494), 765. doi:10.1136/bmj.38398.500764.8F.
Kowitlawakul, Y. (2011). The technology acceptance model: Predicting nurses’ intention to use telemedicine technology (eICU). Computers Informatics Nursing, 29(7), 411–418. doi:410.1097/NCN.1090b1013e3181f1099dd1094a.
Lau, F., Kuziemsky, C., Price, M., & Gardner, J. (2010). A review on systematic reviews of health information system studies. Journal of the American Medical Informatics Association, 17(6), 637–645. doi:10.1136/jamia.2010.004838.
Mills, J., Chamberlain-Salaun, J., Henry, R., Sando, J., & Summers, G. (2013). Nurses in Australian acute care settings: Experiences with and outcomes of e-health. An integrative review. International Journal of Management & Information Technology, 2(2), 1–8.
Rogers, E. (2003). Diffusion of innovations (5th ed.). New York: Free Press.
Rogers, M. L., Sockolow, P. S., Bowles, K. H., Hand, K. E., & George, J. (2013). Use of a human factors approach to uncover informatics needs of nurses in documentation of care. International Journal of Medical Informatics, 82(11), 1068–1074.
Stevenson, J., Nilsson, G., Petersson, G., & Johanssson, P. (2010). Nurses’ experience of using electronic patient records in everyday practice in acute/inpatient ward settings: A literature review. Health Informatics Journal, 16(1), 63–72.
Turley, J. P. (1996). Toward a model for nursing informatics. Journal of Nursing Scholarship, 28(4), 309–313.
Venkatesh, V., Morris, M. G., Gordon, B. D., & Davis, F. D. (2003). User acceptance of information technology: Toward a unified view. MIS Quarterly, 27(3), 425–478.
Venkatesh, V., Thong, J. Y. L., & Xin, X. (2012). Consumer acceptance and use of information technology: Extending the unified theory of acceptance and use of technology. MIS Quarterly, 36(1), 157–178.
Viitanen, J., Hypponen, H., Laaveri, T., Vanska, J., Reponen, J., & Winblad, I. (2011). National questionnaire study on clinical ICT systems proofs: Physicians suffer from poor usability. International Journal of Medical Informatics, 80(10), 708–725.
Weber, S. (2007). A qualitative analysis of how advanced practice nurses use clinical decision support systems. Journal of the American Academy of Nurse Practitioners, 19(12), 652–667. doi:10.1111/j.1745-7599.2007.00266.x.
Weber, S., Crago, E. A., Sherwood, P. R., & Smith, T. (2009). Practitioner approaches to the integration of clinical decision support system technology in critical care. Journal of Nursing Administration, 39(11), 465–469. doi:10.1097/NNA.0b013e3181bd5fc2.
Wills, M. J., El-Gayar, O. F., & Bennett, D. (2008). Examining health care professionals’ acceptance of electronic medical records using UTAUT. Issues in Information Systems, 9(2), 396–401.
Yu, P., Li, H., & Gagnon, M.-P. (2009). Health IT acceptance factors in long-term care facilities: A cross-sectional survey. International Journal of Medical Informatics, 78(4), 219–229. doi:10.1016/j.ijmedinf.2008.07.006.
Yun-Ke, C., Khoo, C., Nourbakhsh, A., & Gan, A. (26–27 Sept 2009). Requirement analysis for a nursing decision support system. Paper presented at the Science and Technology for Humanity (TIC-STH), 2009 IEEE Toronto International Conference.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Nguyen, L. et al. (2016). The Acceptance of Nursing Information Systems: An Analysis Using UTAUT. In: Wickramasinghe, N., Troshani, I., Tan, J. (eds) Contemporary Consumer Health Informatics. Healthcare Delivery in the Information Age. Springer, Cham. https://doi.org/10.1007/978-3-319-25973-4_19
Download citation
DOI: https://doi.org/10.1007/978-3-319-25973-4_19
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-25971-0
Online ISBN: 978-3-319-25973-4
eBook Packages: MedicineMedicine (R0)