
Abstract
The use of improved surgical techniques, neoadjuvant therapy, and more precise imaging modalities has transformed rectal cancer treatment, improved oncologic outcomes, reduced morbidity and mortality, and enhanced patients’ quality of life. In the current era, the majority of patients are now candidates for a sphincter-saving procedure, with less than a 10 % risk of local recurrence and acceptable maintenance of sexual and bladder function postoperatively. Proctectomy has remained the cornerstone of rectal cancer treatment. In this chapter, we will review the evolution of proctectomy technique and discuss the technical details of proctectomy and histologic assessment of a rectal cancer specimen.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Proctectomy
- Total mesorectal excision
- Laparoscopy
- Robotic-assisted surgery
- Endopelvic fascia
- Mesorectum
- Superior hypogastric plexus
- Inferior hypogastric plexus
- Low anterior resection
- Abdominoperineal resection
- Extralevator abdominoperineal resection
- Intersphincteric resection
- Coloanal anastomosis
Key Concepts
-
A proper proctectomy with sharp dissection along the visceral and parietal layers of the endopelvic fascia facilitates margin-negative resection, reduces local recurrence, and limits nerve injury associated with sexual dysfunction.
-
Precise understanding of pelvic anatomy including fascial planes, autonomic nerves, and pelvic floor musculature is critical in performing a proper proctectomy.
-
The quality of mesorectal excision and the distance of the circumferential radial margin are associated with local pelvic control.
-
Proctectomy can be performed using open, laparoscopic, and robot-assisted techniques.
Background and History
At the beginning of the twentieth century, the majority of patients diagnosed with rectal cancer in Europe and the United States underwent perineal proctectomy—the preferred operation of the day. While this operation was an improvement over previous surgeries, it was highly morbid, with poor oncologic results. In 1908, William Ernest Miles of St. Mark’s Hospital in London recognized that nearly all of his patients suffering from rectal cancer died of recurrent disease within 3 years after perineal proctectomy. On autopsy, he noted that most recurrences were identified in the part of the mesorectum that had been left in place and/or within lymph nodes situated near the left common iliac artery. Miles termed these areas the “zone of upward spread.” He concluded that perineal proctectomy was inadequate because it failed to address the ultimate cause of local recurrence: incomplete excision of the mesorectum, including its lymphovascular supply.
Based on his observations, Miles devised a different procedure, which he described as abdominal perineal excision (APE) or, as it came to be called, abdominoperineal resection (APR ). APR soon became the surgical procedure of choice for treatment of carcinoma of the rectum [1]. As Miles described it, APR actually comprised two procedures performed during the same operation: an abdominal operation and a perineal operation. The abdominal part of the APR includes dissection of the rectum and mesorectum and creation of a colostomy; the perineal part includes detachment of the rectum, anus, and levator muscles from the genital/urinary organs and the ischiorectal fat . Describing the perineal approach in 1910, Miles stressed that the levator muscles should be “divided as far outwards as their origin from the white line so as to include the lateral zone of spread” [2]. Compared with perineal proctectomy, long-term outcomes following this new operation improved considerably.
Miles’ emphasis on the necessity of removing the mesorectum in its entirety would become the guiding principle of what is now known as total mesorectal excision (TME ). Today, TME remains the gold standard in rectal cancer surgery. TME entails sharp—rather than blunt—dissection of the visceral and parietal layers of the endopelvic fascia , resulting in intact removal of the rectum and mesorectum [3]. In Miles’ time, however, most surgeons continued to perform traditional blunt dissection, limiting the benefits of APR and resulting in a 25% rate of positive resection margins, with high rates of recurrence and mortality.
The absolute necessity of sharp dissection in every rectal cancer operation—i.e., meticulous removal of the entire mesorectum along the areolar plane outside of the rectal fascia propria—was reemphasized in 1982 by Bill Heald. Heald defined TME as an “optimal dissection plane around the cancer which must clear all forms of extension and circumscribe predictably uninvolved tissue,” in other words, sharp mesorectal excision along definable tissue planes. He described this as the “holy plane” of rectal cancer surgery [4]. The aims of TME are to excise the rectum and surrounding mesorectum, including its blood vessels and pararectal lymph nodes, within an intact visceral fascial “envelope”; to complete en bloc resection of the lymph nodes along the superior rectal and inferior mesenteric arteries; and to achieve clear resection margins.
Advocates of “ total mesorectal excision” have focused attention on two critical components of oncologic proctectomy: the lateral (radial) margin and the distal margin of mesorectal excision. Sharp dissection in the avascular plane surrounding the mesorectum, so as to remove the mesorectum in its fascial envelope and achieve a wide circumferential radial margin (CRM ), has been demonstrated to be essential in avoiding local recurrence of tumor in the pelvis [5–7]. Although this concept is not novel [8, 9], it has served to refocus attention on surgical technique during proctectomy, which is warranted, given the widely divergent local recurrence rates reported in the literature [10]. In 1985, Quirke and colleagues showed that pelvic relapse was the result of residual tumor at the CRM, and they were among the first to describe a systematic assessment of the CRM [7]. Since the original publication of this paper, numerous studies (including prospective trials) have confirmed that CRM involvement is a strong predictor of local recurrence, as well as distant metastasis and poor survival [11].
The second component of TME, as advocated initially by Heald et al., is the removal of the entire mesorectum distal to the tumor. However, the necessity of removing mesorectum more than 4–5 cm distal to a proximal rectal tumor is not supported by pathologic studies of lymph node involvement in the mesorectum [9, 10, 12–16]. Furthermore, it may have contributed to a high anastomotic leak rate (17%) in early series [17] and has not been shown to be of benefit in a large clinical review [18]. At present, many advocates of “ total mesorectal excision” limit mesorectal resection to 4–5 cm distal to proximal rectal tumors [6, 19–21], although some authors still refer to this technique as “total” mesorectal excision [19–22], which has caused confusion. Other groups have termed the concept of tailoring the mesorectal excision to the position of the tumor “tumor-specific mesorectal excision” [6], which may be more accurate.
In summary, for all patients with rectal cancer, it is critical that the primary tumor is removed in its entirety. In addition, mesenteric tissue at greatest risk for nodal metastases should also be resected. For patients with mid and distal rectal cancers, appropriate proctectomy technique will involve removing the entire mesorectum. For patients with proximal rectal cancers, it is important to remove the mesorectum for a distance of approximately 4–5 cm distal to the tumor, although resecting the mesorectum distal to that point does not appear to confer benefit.
Anatomy of the Mesorectum/Rectal Fascia
Chapter 1 has an in-depth look at the anatomy of the colon, rectum, and anus; however, surgical anatomy as it relates to proctectomy will be covered here. The proctectomy technique is based on an understanding of the anatomy of the rectum and the mesorectal fascia. The rectum is located at the end of the large intestine, where the taeniae coalesce to form a complete lineal muscular layer. This is surrounded by a recognizable annular envelope: the rectal fascia (or mesorectum, as it is better known to surgeons). The mesorectum contains the lymphovascular supply of the rectum and upper anal canal. It encloses the branches of the superior rectal artery and the perirectal lymph nodes , which drain in a caudal direction toward the inferior mesenteric artery. Around the rectum is an avascular plane, surgically recognizable as a cobweb of areolar tissue.
The mesorectum is asymmetrically distributed. The bulk of it sits posterior to the rectum, identified by two protruding bulges (the “mesorectal cheeks”); anteriorly and laterally, the perirectal tissue is thinner. Similarly, the mesorectal fascia is most developed on the posterior aspect. Anteriorly, the mesorectum is thinner and bordered by the recto-genital septum known as Denonvilliers’ fascia . In men, Denonvilliers’ fascia separates the rectum and mesorectum from the prostate and seminal vesicles. In women, the thinner rectovaginal fascia separates the rectum from the vagina. Ligaments below and lateral to the peritoneal reflection connect to the parietal fascia on the pelvic sidewall.
An extensive autonomic nervous system of sympathetic and parasympathetic fibers supplies the rectum and genitourinary tract , controlling continence and sexual function. The sympathetic autonomous system is responsible for urinary continence and ejaculation, whereas the parasympathetic system controls micturition , as well as genital erection and lubrication. Precise knowledge of the anatomy of this pelvic autonomic network is essential in rectal surgery, as injury to these nerves during proctectomy can lead to sexual dysfunction and incontinence. The sympathetic autonomic plexus arises from lumbar sympathetic nerves originating in the T12–L2 spinal junction , which pass anterior to the aorta and form a network in close proximity to the origin of the inferior mesenteric artery. This is known as the superior hypogastric plexus . The superior hypogastric plexus enters the pelvic cavity anterior to the sacral promontory and splits into fairly well-defined left and right hypogastric nerves (Figure 31-1). Damage to this sympathetic plexus during ligation of the inferior mesenteric artery, or damage to the hypogastric nerve trunks during mesorectal mobilization, can lead to urinary incontinence and retrograde ejaculation. The hypogastric nerves course posterolateral to the mesorectum and ultimately join parasympathetic nerves—also known as the pelvic plexus, pelvic splanchnic nerves, or nervi erigentes—to form the inferior hypogastric plexus . The parasympathetic nerves that join the sympathetic system originate from the S2–S4 sacral spinal nerve roots , lying posterolaterally along the mesorectal fascia. Preservation of the pelvic splanchnic nerves and the inferior hypogastric plexus, and careful separation of these from the rectum, is one of the most challenging aspects of proctectomy. The inferior hypogastric plexus forms an extensive network of interlocking fibers of the sympathetic left and right hypogastric nerves, and parasympathetic pelvic splanchnic nerves are situated on the pelvic sidewall. Various nerves leave the inferior hypogastric plexus to enter the rectal wall, while the remaining neurovascular bundles extend anterolaterally to the seminal vesicles, distal ureters, vasa deferentia, urinary bladder, prostate and cavernous bodies in men, and in the similar anatomic area in women, for whom the lower portion of the inferior hypogastric plexus runs along the lower lateral wall of the vagina.

The superior hypogastric plexus splits into the right and left hypogastric nerves as it enters the pelvic cavity. Parasympathetic pelvic splanchnic nerves, also known as nervi erigentes, arise from sacral spinal nerves S2–S4 and pierce the presacral fascia on the left and right side to join the hypogastric nerves, forming the inferior hypogastric plexus (not shown). With permission from Lee-Kong et al.: Autonomic nerve preservation during rectal cancer resection. J Gastrointest Surg 2010;14:416–422. © Springer [104].
Laterally, the mesorectum is sometimes not completely covered by a layer of fascia and is penetrated by the middle rectal vessels (coming from the internal iliac vessels, present in about 10–20% of patients) and autonomic nerves from the inferior hypogastric plexus. The mesorectum is tethered inferolaterally to the inferior hypogastric plexus, necessitating a more challenging dissection that is best achieved with precise monopolar diathermy and subtle traction and countertraction, in order to draw the autonomic nerve fibers controlling urinary continence and sexual function carefully away from the surface of the mesorectum.
Posterior to the mesorectum is the presacral fascia, which follows the concavity of the sacrum. The presacral fascia is a thickened parietal fascia that covers the presacral veins and fat, extending laterally to join Denonvilliers’ fascia anteriorly. Inferiorly, between the levels of the third and fourth sacral vertebra, the mesorectum and the presacral fascia fuse. The thick connective tissue bridging these two separate fascias is also known as the rectosacral fascia or Waldeyer’s fascia. Waldeyer’s fascia is an important surgical landmark during posterior rectal mobilization, because of its close relationship to the sympathetic hypogastric nerves and the inferior hypogastric plexus . Inaccurate dissection at this level can lead anteriorly to breach of the mesorectum and posteriorly to tearing of the fascia, resulting in considerable bleeding from the presacral veins. At the most distal part of the rectum, the mesorectum thins out as a recognizable structure so that it is virtually absent over the final 1 cm of the rectum. Distal rectal cancers are thus at greater risk of invading surrounding structures than proximal rectal cancers, particularly the pelvic floor/external anal sphincter, vagina, or prostate, because of the relative paucity of mesorectum at this level.
Surgical Principles of Proctectomy for Rectal Cancer
The basic principles of proctectomy are as follows [23]:
-
1.
Sharp dissection circumferentially around the mesorectum in an avascular areolar plane between the visceral and parietal layers of the endopelvic fascia (Figure 31-2a)
Figure 31-2. 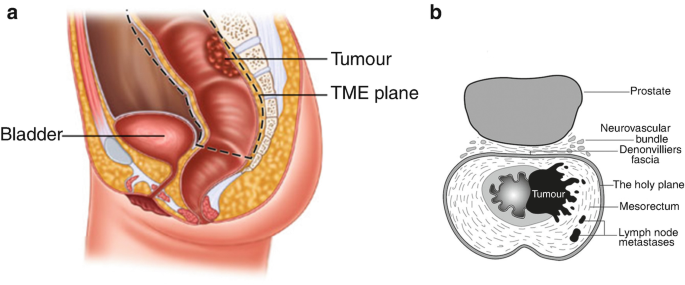
Total mesorectal excision. (a) Dissection follows the dotted line. Tumor deposits are often present within the lymphovascular tissue surrounding the rectum (mesorectum). Incomplete resection leaves residual deposits which are most likely the origin of local treatment failure. With permission from Janjua AZ, Moran B, Heald RJ. Open surgical management of rectal cancer. Patel HRH, Mould T, Joseph JV, Delaney CP. (Eds). Pelvic Cancer Surgery: Modern Breakthroughs and Future Advances. Springer, New York, 2015: pp: 531. © Springer 2015 [105]. (b) The plane of total mesorectal excision allows complete removal of regional lymph nodes while sparing the neurovascular bundles. With permission from Heald RJ et al.: Embryology and anatomy of the rectum. Semin Surg Oncol. 1998 Sep; 15(2):66–71. © John Wiley and Sons [106].
-
2.
Identification and preservation of the autonomic nerve plexus that controls bladder and sexual function (Figure 31-2b)
-
3.
Achievement of a circumferential margin that is macroscopically and microscopically clear of tumor
-
4.
Preservation of the anal sphincter complex and pelvic floor, with restoration of gastrointestinal continuity when appropriate

Pathological Assessment
In addition to assessment of proximal, distal, and CRMs, pathologists can grade the quality of the mesorectal specimen. This has been demonstrated to have prognostic significance. Quirke et al. described a grading system which classifies rectal cancer specimens according to whether the surgeon has dissected outside the mesorectal fascia, in the correct plane (the mesorectal excision plane), or has violated the mesorectum, leaving mesorectal tissue behind in the pelvis by following a plane within the mesorectum (intra-mesorectal plane) or directly on the muscularis propria (muscularis propria plane) [24]. This mesorectal grading system has been evaluated in subsequent studies and has been found to be an independent predictor of local pelvic control [25, 26]. One study reported a significant association between plane of surgery and survival—even in patients with an uninvolved CRM [27]. However, these studies also showed that the surgical plane was related to CRM positivity rates, with the lowest rates of positive CRM in surgery that achieved sharp dissection along the mesorectal plane.
Pathological analysis of the excised proctectomy specimen provides important prognostic information on the stage and biology of the tumor. It is also a means of assessing the quality of surgery, because margin status and quality of mesorectal excision can be used as surrogates for oncologic outcome assessment. The College of American Pathologists (CAP) has implemented standardized assessment of rectal cancer specimens [28]. The surgeon or pathologist should ink the non-peritonealized radial margin of the fresh resection specimen to help guide this analysis. A standardized synoptic report should include a subjective assessment of mesorectal grade and quantitative measurement of CRM in millimeters. A margin is considered positive if the primary tumor or involved lymph node extends to within 1 mm of the resection margin.
Preoperative Preparation
All patients undergoing rectal cancer surgery require preoperative preparation aimed at optimizing the technical success of the procedure and avoiding perioperative complications. Oral mechanical bowel preparation with polyethylene glycol, to reduce the bacterial load and risk of intraoperative fecal spillage, has been considered an axiom in colon and rectal surgery. However, a number of prospective trials have failed to demonstrate any benefit from mechanical bowel cleansing in preventing surgical site infections (SSIs) [29, 30]. These results were confirmed by a Cochrane systematic review of 5805 patients, in which the authors concluded that there is no statistically significant benefit from mechanical bowel preparation or the use of rectal enemas [31]. Another recent systematic review by the Agency for Healthcare Research and Quality reached similar conclusions [32]. Oral mechanical bowel preparation appeared to be protective, compared to no preparation, for peritonitis or intra-abdominal abscess, but the evidence was weak. The study could not draw any conclusion on potential harms, such as dehydration and electrolyte imbalances, related to use of oral mechanical bowel preparation.
Despite the lack of solid data regarding the impact of bowel preparation on wound infection, there are other valid reasons for preoperative cathartic bowel preparation prior to proctectomy. It is preferable to have the rectosigmoid cleared of stool, in order to accurately assess the position of the tumor intraoperatively. In addition, division of the colon and rectum is more easily accomplished if the lumen is free of stool. Lastly, if the patient is to undergo a temporary diverting proximal stoma, it is preferable to have the intervening colon free of stool, in case of anastomotic leak. Although it is theoretically possible to have patients clear stool from the rectosigmoid with preoperative enemas, in practice this is often difficult to accomplish due to the rectal tumor itself and physical disabilities associated with the advanced age of many patients. In addition, enemas do not clear the proximal colon of stool, mitigating the benefit of proximal fecal diversion if anastomosis is performed.
High-quality evidence indicates that preoperative antibiotics covering aerobic and anaerobic bacteria, delivered orally, intravenously, or both, reduce the risk of postoperative surgical wound infection by as much as 66% in elective colorectal surgery [33]. Oral neomycin- and erythromycin-based antibiotics are typically administered the day before surgery, in combination with oral mechanical bowel preparation. For patients without penicillin allergy, a second-generation cephalosporin (cefotetan or cefoxitin) is administered intravenously within 60 min of the surgical incision, with re-dosing during the procedure as required, according to the half-life of the drug and the duration of surgery. For penicillin-allergic patients, metronidazole or clindamycin combined with either ciprofloxacin or gentamicin is acceptable, as are aztreonam and fluoroquinolones [34]. Ertapenem, a long-acting carbapenem active against gram-negative anaerobe, is an accepted alternative to second-generation cephalosporins for prophylaxis. Other measures that prevent SSI include tight glucose control in diabetic patients, smoking cessation, clipping rather than shaving the skin of the abdominal wall, and maintaining normothermia and adequate oxygenation during anesthesia [35]. Patients undergoing rectal cancer surgery are also at risk of deep venous thrombosis and pulmonary embolism and should have thromboembolic prophylaxis with unfractionated heparin or low molecular weight heparin during the perioperative and postoperative period [36].
As the incidence of rectal cancer increases with age, many patients also have cardiovascular or respiratory conditions requiring medical clearance before surgery. While technical advances have made rectal cancer operations safer, optimal outcomes require special effort to ensure that the patient’s overall health is acceptable at the time of surgery. Many patients with other comorbid conditions such as diabetes, hypertension, and coronary artery disease require medical evaluation before undergoing surgery. Comorbidities can impact decision-making and affect short- and long-term outcomes. Patient’s clinical and performance status should be optimized to reduce the risk of perioperative complications. Fertility options should be discussed with all individuals of childbearing potential. In the setting of Lynch syndrome, discussion regarding oophorectomy and hysterectomy is appropriate. Patients who may require a stoma should be seen before surgery by an enterostomal therapist. Adequate marking of the stoma site improves outcomes. Preoperative teaching shortens the time required by patients to gain proficiency in managing their stoma and reduces length of hospital stay [37].
The enhanced recovery after surgery (ERAS) protocols were introduced in open colorectal surgery in the 1990s, with the aim of speeding patient recovery, improving patient outcomes and satisfaction, shortening hospitalization, and reducing healthcare costs [38]. ERAS protocols span the entire perioperative period and attempt to minimize surgical stress and postoperative ileus through patient education, preoperative hydration and carbohydrate loading, goal-directed intraoperative fluid management, narcotic sparing for intraoperative and postoperative pain control, and early mobilization and oral feeding in the postoperative period. A number of prospective trials and reviews have indicated that the implementation of ERAS protocols reduces length of hospital stay, compared to conventional recovery in patients undergoing open or minimally invasive surgery for CRC [39, 40].
Operative Approaches
Optimal resection of rectal cancer according to the oncologic principles of TME can be achieved by open or minimally invasive (laparoscopic or robotic) surgical techniques. Herein, we describe methods for both open and minimally invasive approaches. General concepts such as nerve preservation are detailed in the “open” section but apply to minimally invasive approaches as well.
Open Low Anterior Resection
The patient is placed in a modified lithotomy or supine split-leg position. A variety of incisions can be utilized; however, it is important to keep the incision line away from the area of potential stoma and stoma appliance, so as to not interfere with management of the stoma postoperatively. The abdominal cavity is explored thoroughly, especially the liver and the peritoneum, to identify signs of distant metastatic disease. If unresectable distant metastatic disease is encountered, then the surgeon should carefully consider whether low pelvic anastomosis is warranted. Patients with unresectable distant metastatic spread often undergo prolonged treatment with chemotherapy, and the presence of a temporary diverting ileostomy may increase the severity of chemotherapy-induced enteritis . In addition, the added risk of colorectal or coloanal anastomotic leak may not be warranted because, if leak occurs, systemic chemotherapy may be delayed. In addition, chemotherapy must be stopped temporarily to close the ileostomy; if complications ensue from this second procedure, systemic chemotherapy may again be delayed. Lastly, the functional derangements associated with low pelvic anastomosis will only be exacerbated if the patient receives cytotoxic chemotherapy , which may produce enteritis. In sum, it may be preferable to simply perform a Hartmann’s resection for mid and distal rectal adenocarcinoma that does not invade the pelvic floor or anal sphincter, in patients with unresectable distant metastatic disease. For patients with proximal rectal cancer who may not require temporary fecal diversion and are at low risk for anastomotic complications, it is reasonable to perform anterior resection with primary anastomosis, even in the setting of unresectable distant metastatic disease (if this was the original plan).
Our preferences regarding the technical aspects of restorative proctectomy are described as follows: The small bowel is carefully packed and retracted to the right, providing access to the pelvis. The sigmoid and left colon is mobilized by dissection laterally to medially along the white line of Toldt. The sigmoid colon is retracted medially. In this loose connective tissue plane, first the gonadal vessels and then, more medially, the left ureter are encountered. Dissection is continued in this plane, and the left colon is dissected away from Gerota’s fascia. At the base of the sigmoid mesocolon, the retrorectal avascular plane is entered. While the sigmoid colon is elevated from the left lateral side, gonadal vessels, the left ureter, and the left hypogastric nerve are preserved in the embryologic avascular plane, and the mesorectal dissection plane is reached. The sigmoid is retracted in the right lateral direction. Then, from the right side, the sigmoid mesocolon is entered through a window over the surgeon’s hand at the pelvic brim. Through this window, the inferior mesenteric artery is liberated, and separate ligations of the artery and vein are performed. The superior rectal artery (just distal to the left colic artery) or inferior mesenteric artery, at its origin 1–2 cm from the aorta, is ligated and divided to preserve the sympathetic plexus. High ligation of the IMA is useful when bulky adenopathy is present at the base of the vessel or when a coloanal anastomosis is necessary and maximal length of the left colon is required. When the inferior mesenteric artery is ligated, care must be taken to preserve the marginal artery, which provides the blood supply from the middle colic vessels to the left colon and anastomosis.
The inferior mesenteric vein is ligated at the paraduodenal (ligament of Treitz) location just inferior to the pancreas and again adjacent to the ligation site of the inferior mesenteric artery. Dividing the vein at the ligament of Treitz is critical in order to accommodate full mobilization of the splenic flexure , which is then allowed to rotate into the pelvis for maximal length. Splenic flexure mobilization is performed by continuing the lateral dissection of the descending colon superiorly, retracting and dissecting the descending colon off Gerota’s fascia . Colonic attachments to the pancreas are then taken down, and care is taken to avoid aggressive retraction on the colon, which can tear the splenic capsule. Omental attachments are then taken down from the distal transverse colon to complete the mobilization.
The sigmoid mesentery is divided to the bowel wall, which is stapled and divided. The left colon is packed superiorly, facilitating visualization of the pelvis. The stapled sigmoid is retracted anteriorly, which opens the perimesorectal planes. A sharp dissection is carried out under direct vision, circumferentially around the mesorectum. The presence of the superior hypogastric plexus posteriorly must be kept in mind throughout the dissection (Figure 31-3a). Starting the dissection in the posterior and then the lateral plane, in a stepwise manner, facilitates identification of the correct mesorectal plane (Figure 31-3b). If bleeding is encountered in one area, it is reasonable to proceed to the opposite circumference, so that pressure is applied while progress continues. The key to this phase is the recognition of the areolar tissue on the back of the mesorectum, through which the dissection should proceed when the areolar tissue is on stretch. Once there is sufficient space, a St. Mark’s Pelvic Retractor is introduced behind the specimen. Traction and countertraction are critical to the pelvic dissection and are optimized by use of the retractor. The lateral dissection is carried out by extending the posterior plane of dissection anteriorly and around the sidewalls of the pelvis. At this point in the dissection, the inferior hypogastric plexuses curve around the surface of the mesorectum and are vulnerable to inadvertent injury. While retracting the divided rectosigmoid forward, the tangentially running hypogastric and pelvic parasympathetic nerves are carefully identified and dissected away from the mesorectal surface on each side (Figure 31-4a). This area of adherence between the nerves and the mesorectum is one of the most challenging and critical in proctectomy. As the lateral dissection moves deeper into the pelvis, one or two middle rectal arteries may be encountered. Middle rectal arteries are present in less than 20% of patients and, if encountered, can be easily divided with cautery. Dissection anteriorly progresses along Denonvilliers’ fascia down to the pelvic floor (Figure 31-4b). Forward retraction with the help of the St. Mark’s Retractor facilitates the development of the space anteriorly. Anterior tumors require resection of Denonvilliers’ fascia , which puts the parasympathetic nerves at risk, as they extend anteriorly toward the prostate. For posterior tumors, dissection can proceed below Denonvilliers’ fascia. Adequacy of the dissection distal to the lower edge of the tumor is examined by palpation and/or endoscopy to ensure a proper distal margin. When mesorectal mobilization down to the pelvic floor is considered complete on both anterior and posterior sides, the rectum is elevated above the pelvic floor and cross-clamped. At this point, washout of the anorectal stump can be performed with saline solution or water. Following this, the rectum is transected with a linear stapler (TA-45), and the specimen is removed. The anastomosis between the colon conduit and the rectal stump is constructed with a circular EEA™ Stapler (Figure 31-5a). The serosa and mucosa are visually evaluated for adequate vascular supply. Intraoperative anastomotic air testing of the colorectal anastomosis is performed by filling the pelvis with saline solution and insufflating the rectum with air through a sigmoidoscope. A handsewn coloanal anastomosis is shown in Figure 31-5b and is discussed separately below.

(a) The distal sigmoid/proximal rectum is elevated anteriorly, exposing the aortic bifurcation and sacral promontory, with identification of the left ureter, left iliac vein, and superior hypogastric plexus. The hypogastric nerves may appear as an obvious discrete band of tissue or as multiple smaller bands. (b) Careful dissection of the sigmoid mesentery distally results in an avascular, areolar plane separating the mesorectal fascia propria from the presacral fascia. With permission from Lee-Kong et al.: Autonomic nerve preservation during rectal cancer resection. J Gastrointest Surg 2010;14:416–422. © Springer [104].

(a) Caudal dissection in the posterior midline, while lifting the rectum “toward the ceiling” may cause the hypogastric nerves to “tent up,” as they often adhere to the mesorectal fascia. (b) Anterior dissection during TME. With permission from Lee Kong et al.: Autonomic nerve preservation during rectal cancer resection. J Gastrointest Surg 2010;14:416–422. © Springer [104].

(a) Stapled end-to-end colorectal anastomosis. (b) Handsewn end-to-end coloanal anastomosis. With permission from Wexner SD, Fleshman JW, editors. Colon and Rectal surgery: Abdominal Operations, Master Techniques in Surgery. Philadelphia: Lippincott Williams & Wilkins; 2012 [107].
Laparoscopic Low Anterior Resection
The patient is placed in a modified lithotomy position. A 5-trocar technique is generally utilized, with an umbilical camera port, two left-sided and two right-sided working (Figure 31-6). This allows the surgeon and second assistant to stand on the patient’s right, with the first assistant standing on the left. The dissection is performed in a medial-to-lateral fashion, first dissecting the vessels, followed by takedown of the splenic flexure, and then the lateral colonic attachments before entering the pelvis for rectal resection. With the patient in head-down and right-sided tilt, enabling the surgeon to move the small bowel mesentery out of the pelvis and away from the colonic mesentery, dissection begins at the sacral promontory. The superior rectal vessels are lifted ventrally, and a plane is developed beneath the sigmoid mesentery. Dissection is carried out just beneath the vessels, in order to sweep the sympathetic nerves toward the retroperitoneum. Dissection proceeds medial to lateral beneath the mesentery and along Toldt’s fascia, preserving the ureter and gonadal vessels. The root of the IMA is exposed by creating an additional window on the superior border of the IMA. The IMA is ligated, taking care not to injure the aortic nerve plexus, either just below the left colic branch or at the origin of the vessel. The IMV is subsequently divided along with the sigmoid mesentery. The left mesocolon is further mobilized along with the splenic flexure. The IMV is divided adjacent to the pancreas to allow full mobilization and rotation of the left colon, so as to reach the pelvis for a tension-free anastomosis. Again, in a medial-to-lateral fashion, dissection continues along the ventral plane of the pancreas, with entry into the lesser sac. Often, the lateral attachments of the splenic flexure can be divided in a medial approach, exposing the spleen. The transverse colon is then retracted caudally, and the omentum is dissected off the transverse colon, meeting the prior dissection place. Lastly, the remaining lateral and splenic attachments are divided by retracting the colon medially.

Preferred port placement for laparoscopic LAR with TME.
For pelvic dissection, it may be necessary to position the patient in a more head-down position, often with less rotation to the right. The rectum is retracted anteriorly and the retrorectal space is identified. Sharp dissection is carried out posteriorly along the areolar plane that defines the junction of the visceral and parietal layers of the endopelvic fascia. Care must be taken to sweep the hypogastric nerves laterally, and dissection proceeds posteriorly along the mesorectum. Once posterior mobilization is completed, dissection continues in the same perimesorectal plane on the lateral sides of the pelvis. The rectum is mobilized circumferentially, applying standard open TME surgical principles. Dissection can be performed with cautery, ultrasonic dissector, or vessel-sealing devices. After TME dissection is completed, the level of rectal transection is confirmed with digital rectal and endoscopic examinations. The rectum is irrigated and then stapled and divided with endoscopic staplers. The specimen is extracted via a wound protector at the umbilical camera port or the future diverting ileostomy site. The proximal sigmoid/left colon is divided, and the anvil is secured for laparoscopic circular anastomosis. An air leak test confirms the integrity of the anastomosis, and a diverting ileostomy is fashioned selectively.
In patients with a narrow pelvis or elevated body mass index, pelvic dissection can be challenging. In such cases, a lower midline or Pfannenstiel incision may be utilized to allow open pelvic dissection, rectal division, and restoration of intestinal continuity. A combination of laparoscopic and open surgery in this manner is often referred to as a “hybrid” approach .
Robotic Low Anterior Resection
Robotics has emerged as a useful technology in pelvic dissection and may have advantages for the surgeon with respect to manual dexterity, versus standard laparoscopy . The straight laparoscopic instruments make dissection within the confines of the narrow, bony pelvis difficult and subject the surgeon to ergonomic stress. The robotic platform allows for stable retraction; enhanced three-dimensional (3D), high-definition visualization; and articulating instruments. There is some indication that use of the robot has been associated with a reduced rate of conversion to laparotomy during proctectomy as compared to standard laparoscopic surgery (although many of the studies on this topic are plagued by selection bias) [41].
A single-docking technique using the da Vinci® Si™ robot is first described. This entails single docking of the robot for the entire procedure, from colon mobilization to pelvic dissection. The patient is placed in a modified lithotomy position. Pneumoperitoneum is established with a Hasson technique through a supraumbilical incision . The abdominal cavity is examined using the robotic camera. Four additional robotic ports are inserted, along with an assistant port, as shown in Figure 31-7a. The greater omentum and the small bowel are retracted out of the pelvis. The patient is placed in Trendelenburg position, with right-side down. The robotic cart is brought to the left lower quadrant. The robotic arms are first docked, with robot arm 1 in the right lower quadrant using monopolar curved scissors or vessel sealer, robot arm 2 in the right upper abdomen using a fenestrated bipolar forceps, and robot arm 3 in the left mid-abdomen using a ProGrasp™ or Cadiere forceps for retraction. Arm 3 begins on the left side of the robot, on the same side as arm 1. Dissection proceeds in a medial-to-lateral fashion, as in standard laparoscopic dissection. Following division of the IMA and IMV, splenic flexure mobilization, and division of the left colic mesentery, robot arm 3 is repositioned (Figure 31-7b). The robot does not need to be moved, and patient position can be maintained. On occasion, a slightly more accentuated head-down and minimal tilt is utilized for the pelvic dissection, in order to keep the small bowel out of the pelvis. This configuration ensures that all instruments can reach the pelvic floor without conflict. Proctectomy proceeds, as described above for standard laparoscopy, but with a few exceptions. Care is taken to maintain dissection along the mesorectal plane laterally and avoid dissection into the pelvic sidewall. This is facilitated by early anterior dissection, which is easily visualized with the camera setup, as described, and use of articulating instruments. We often use a tie around the rectum (such as thin vaginal packing) to facilitate rectal retraction. During pelvic dissection, the bedside assistant utilizes the lateral assistant port and the right upper quadrant robotic port (which was used for pedicle ligation and flexure takedown). Intraoperative endoscopy, with picture-in-picture technology, allows the operating surgeon to visualize the rectal tumor at the robotic console and optimize the distal resection margin. We use cautery and the Vessel Sealer, along with the robotic stapler (EndoWrist® Stapler 45), to achieve low pelvic stapling. Superior visualization and retraction, along with articulating instruments, greatly facilitates deep pelvic dissection along the prostate and in the intersphincteric groove for coloanal anastomosis. When the distal rectum has been divided, the robot is undocked, and the rectum is extracted via a wound protector at the umbilical port or future stoma site. The descending colon is divided, the anvil secured, and the laparoscopic anastomosis performed.

Trocar placement for robotic LAR using the da Vinci® Si™ robot with the two separate phases of the operation: (a) pedicle ligation, splenic flexure mobilization; (b) pelvic dissection.
A similar setup is utilized with the da Vinci® Xi™ robot. This system has more flexibility, as the camera is 8 mm and can be used in any port. This is referred to as “port hopping” and is useful if dissection becomes difficult and a new vantage point is needed. The da Vinci® Xi™ robot instruments are longer, eliminating problems related to reaching the splenic flexure and the deep pelvis. Port setup is shown in Figure 31-8a, b.

Trocar placement for a robotic LAR using the da Vinci® Xi™ robot. (a) Configuration used for pedicle ligation, splenic flexure mobilization. (b) Configuration used for pelvic dissection.
Abdominoperineal Resection
APR is necessary for very low rectal tumors that invade the external sphincter or the levator muscles . The relative indications for APR include external sphincter involvement at any time in the patient’s workup. Relative indications include patients with poor preoperative baseline bowel function who are not candidates for a Hartmann resection . Furthermore, care should be taken when planning surgery in patients with bulky low tumors that show minimal response or progression on neoadjuvant chemoradiation . This portends aggressive tumor biology with extension along lymphovascular and perineural spaces, making complete margin-negative resection more challenging. Wide resection, including APR, should be considered in such cases.
During APR, left colon/splenic flexure mobilization is not required. Dissection is generally taken down to the pelvic floor, and then the perineal phase is begun. Perineal dissection can be performed in lithotomy or prone position. Some assert that the prone dissection is more comfortable for the surgeon and facilitates anterior dissection but requires abdominal closure and stoma maturation prior to repositioning the patient facedown. When beginning the perineal phase, additional Betadine® preparation is utilized, and the anus is sutured to reduce contamination. A wide elliptical incision is created to encompass the sphincter complex, and dissection proceeds into the ischiorectal space. Care is taken to dissect just superior to the coccyx, where the pelvic floor is divided and the perineal dissection meets the anterior dissection. The lateral pelvic floor musculature is divided widely, and the anterior dissection is then performed, carefully avoiding injury to the vagina or membranous portion of the urethra. Following specimen removal and pelvic irrigation, the perineum is closed in multiple layers to eliminate the dead space. Pelvic drains are used liberally to reduce fluid buildup in the contaminated pelvis.
Extralevator or “Cylindrical ” APR
In recent years, several authors have shown that oncologic outcomes after APR have not improved to the same degree as those seen after low anterior resection (LAR) . In fact, compared with patients undergoing LAR during the same time period, patients undergoing APR have higher rates of local recurrence and poorer survival [42, 43]. The difference in oncologic outcomes may be explained to a substantial degree by the increased risk of tumor-involved margins (CRM) and inadvertent bowel perforations associated with APR, as both of these factors are significantly related to local control and survival. It is important to keep in mind that the distal rectum is devoid of surrounding mesorectum; therefore, tumor extension beyond the muscularis propria can invade surrounding tissues, resulting in positive CRM with standard resection. Higher rates of CRM were highlighted in a 2005 study from the UK and subsequently verified in a joint study of specimens from the Dutch trial [42, 44]. In the latter study, Nagtegaal and colleagues assessed 846 LAR and 373 APR specimens. They found that the plane of resection was within the sphincteric muscle, the submucosa, or lumen in more than one-third of the APR cases, resulting in a positive CRM rate of 30.4% in APR versus 10.7% in LAR and a perforation rate of 13.7% versus 2.5%, respectively. Others have reported improved outcomes with wide anatomic resection [45, 46].
An approach to reduce CRM involvement and specimen perforation, proposed by the Karolinska Institute in Stockholm and termed extralevator or “cylindrical” APR, involves wide resection of the levator muscles en bloc with the sphincter muscles, anal canal, and mesorectum. The abdominal component of the procedure terminates higher in the pelvis, and the levator ani muscle is divided along its attachments to the sidewall to avoid a “waist” in the specimen (Figure 31-9). The perineal phase widely resects the ischiorectal space and completes the dissection. In a report comparing cylindrical to conventional APR specimens, Holm and colleagues demonstrated a marked reduction in CRM involvement and perforation with cylindrical APR [47]; however, flap closure is usually required, and perineal wound complications, as well as chronic pain, were significantly increased in the extralevator group [48, 49]. Many advocate “selective extralevator dissection” in areas of tumor, stressing the need for accurate preoperative imaging and examination [50]. Prone positioning for the perineal phase is not mandatory, and minimally invasive approaches are feasible [51–53]. Appropriate patient selection, methods of closing the pelvic floor to reduce wound complications and perineal hernias, and an optimal approach (open versus laparoscopic or robotic) are pertinent issues warranting further investigation in extralevator APR.

Abdominoperineal resection specimens. Dissections from above and below meet above the anal canal. (a) APR specimen with a waist. Courtesy of Eric K Johnson, MD. (b) Specimen with a cylindrical resection and no waist (intact mesorectum). Courtesy of Conor Delaney, MD.
Special Considerations
Rectal Washout
It has been suggested that implantation of exfoliated malignant cells is a possible mechanism of luminal tumor recurrence in colorectal anastomoses. Intraoperative rectal washout with saline solution or water theoretically decreases the amount and viability of these cells. A study from Sweden reported a reduction in local recurrence from 10.2% with no washout to 6% with washout. However, there is no conclusive evidence regarding the effect of rectal washout on local recurrence after rectal cancer surgery. Although it may be merely a surrogate marker for attention to detail, we routinely use intraoperative rectal washout. It is a simple procedure, with minimal morbidity and with potential benefits [54].
Distal Margin
The distal resection margin is an important consideration in rectal cancer surgery. Although lymphatic drainage of the rectum generally occurs in a cephalad direction toward the major lymph node stations, pathological studies have shown distal mesorectal spread as far as 2–3 cm below the lower palpable edge of the tumor. Thus, for upper rectal cancers, mesorectal resection should include mesorectum at least 4–5 cm distal to the lower edge of the tumor, and the mesorectum is divided perpendicular to the longitudinal access of the rectum for a tumor-specific mesorectal excision. It is critical not to “cone in” and leave mesorectum behind when performing this maneuver. For mid to low rectal cancers, dissection 4–5 cm below the tumor generally ends at the pelvic floor. Thus, as long as the entire mesorectum can be removed and negative margins of resection obtained for the primary tumor, it is reasonable to consider restorative proctectomy with coloanal anastomosis for patients with distal cancers [55–58]. The exact distance that constitutes an adequate distal mural margin in this situation is the subject of debate, but an attempt to achieve 1 cm seems reasonable.
Coloanal Anastomosis
In carefully selected cases in the setting of an ultra-low rectal cancer, continued dissection along the intersphincteric plane (which is an extension of the muscularis propria of the rectum) may facilitate sphincter preservation. A handsewn anastomosis is commonly performed, with good oncologic outcomes, especially in patients with a significant response to preoperative chemoradiotherapy [53, 58]. Patient selection and counseling are critical, as patients with coloanal anastomosis have worse bowel function and potentially poorer quality of life than those with a standard stapled colorectal anastomosis [59].
Options for Reconstruction of the Gastrointestinal Tract
Following rectal resection, patients often describe frequent bowel movements, incomplete evacuation, clustering, urgency, and, at times, incontinence. In order to mitigate these symptoms, which are collectively known as LAR syndrome, various techniques have been attempted to recreate the reservoir function of the resected rectum. These are known as colonic neorectal reservoirs and include the colonic J-pouch and the end-to-side (or “Baker-type”) anastomosis.
A colonic J-pouch is constructed in similar fashion to an ileal J-pouch; however, the colonic J-pouch is much smaller, about 6–8 cm in length. Randomized trials, a meta-analysis, and Cochrane review have all concluded that a colonic J-pouch results in improvement of symptoms (decreased frequency, urgency, and nocturnal bowel movements) and a better quality of life for at least 1 year after surgery, compared to an end-to-end anastomosis [60–62]. Coloplasty, longitudinal colotomy closed transversely, was proposed for patients with a narrow pelvis for whom J-pouch was not technically feasible; however, this has not been shown to be an improvement over straight anastomosis. The additional suture line has a risk of leak that can be difficult to treat, and generally coloplasty has fallen out of favor. It is difficult to interpret the results of some trials, given the variation in surgical technique: specifically, the use of either sigmoid colon or descending colon for construction of the neorectum. The use of the sigmoid colon for construction of the neorectum in patients with significant muscular hypertrophy or diverticular disease may negatively impact postoperative function.
An end-to-side or Baker anastomosis, first described in 1950, has recently been revisited as another option for improving postoperative bowel function. This side-to-end anastomosis appears to confer many of the functional advantages of the colonic J-pouch. Compared to a straight anastomosis, it is associated with significantly fewer anastomotic leaks, and overall it is safe, easier, and faster to create than the colonic J-pouch. A 2008 Cochrane review of four randomized trials comparing colonic J-pouch to the side-to-end anastomosis, as well as a more recent meta-analysis of six randomized trials, found similar functional outcomes between the two groups [63]. In many instances, there is insufficient bowel length, or the pelvis is too narrow to permit creation of a reservoir. Ensuring sufficient length of the bowel to adequately sacralize in the pelvis is crucial to healing and function. Some experts prefer to avoid the multiple staple lines associated with reservoirs and the risk of anastomotic leaks, which are difficult to remedy.
Fecal Diversion
Anastomotic leakage following proctectomy occurs in up to one-quarter of patients. Creation of a defunctioning stoma following restorative proctectomy may decrease the sequelae of anastomotic leak and pelvic sepsis. However, the value of a protective stoma has been a subject of controversy for many years. A randomized controlled trial in 2009 reported a reduction in leak rate from 28% without to 10% with a stoma [64]. A 2009 meta-analysis comparing defunctioning stoma to no stoma after rectal resection concluded that the defunctioning stoma resulted in lower rates of leak and reoperation [65]. This meta-analysis included data from four randomized controlled trials and 21 non-randomized studies, involving 11,429 patients in total. A recent meta-analysis of 13 studies published between 2004 and 2014, pooling data on 8002 patients, reported similar conclusions [66]. However, diversion does require a second operation, may result in dehydration, entails an increased risk of bowel obstruction, and is not popular with patients. Therefore, most centers divert selectively, based on anastomotic height, patient-related factors such as diabetes and previous pelvic radiation, and the results of intraoperative leak test.
Extended Resection
Up to 10% of patients with rectal cancer present with tumor invading adjacent structures, necessitating en bloc resection of the affected organ(s) [67]. En bloc resection of adjacent pelvic organs has been associated with good oncologic outcomes when pathologically negative microscopic (R0) margins can be achieved [68, 69].
Involvement of the uterus and vagina in women is best treated with en bloc resection of the rectum with the uterus and the posterior vaginal wall, in order to achieve R0 resection. Closure can be done easily after partial vaginectomy by flap reconstruction or primary closure, preserving sexual function.
Involvement of the seminal vesicles on one or both sides in men can be managed by dissection anterior to the vesicles, removing them en bloc with the rectum. The neurovascular bundles arising from the inferior hypogastric plexus, which control urinary and sexual function, are at risk during this dissection—as are the distal ureters, which should be identified and preserved. Involvement of the prostate by rectal cancer usually requires urologic consultation and is usually treated either with a partial prostatectomy or a pelvic exenteration, depending on the extent of tumor invasion. It should be noted that en bloc resection of the seminal vesicles only, with preservation of the bladder and prostate, is a challenging operation, often much more difficult than pelvic exenteration.
Involvement of the distal ureters by a locally advanced rectal tumor is rare. However, if encountered, it is best managed with en bloc resection of the ureter, with primary ureteric anastomosis over a stent or a psoas hitch, depending on the length of the ureteric defect. Rectal cancers that adhere to the urinary bladder require partial or total cystectomy, especially when the trigone is involved.
Lateral pelvic sidewall lymph node involvement has been reported in up to 20% of T3/T4 rectal cancer cases [70]. In general, pelvic sidewall lymph node involvement is associated with low-lying tumors and worse prognosis [71]. In Japanese studies, selective use of lateral pelvic lymphadenectomy has reportedly led to good outcomes. A meta-analysis of 20 studies demonstrated no improvement in survival or local recurrence when an extended lymphadenectomy was performed compared to standard proctectomy [72]. However, in selected cases where lymphatic spread is suspected clinically or radiographically, an extended lymphadenectomy is warranted in order to obtain an R0 resection.
Intraoperative Radiation Therapy
Intraoperative radiation therapy (IORT ) has been used in patients with locally advanced primary rectal cancer and an involved or threatened CRM following surgical resection. The goal of IORT is to sterilize any microscopic foci of tumor, thus decreasing the risk of local recurrence. During IORT, the radiosensitive bladder and bowel can be excluded from the radiation field, allowing a higher dose to be delivered to the tumor bed. In the United States, IORT is most commonly administered by two different techniques: intraoperative electron-beam radiation therapy (IOERT) or high-dose-rate (HDR) brachytherapy. IOERT is delivered by means of a linear accelerator over the course of a few minutes; it can be used in any operating room because electrons do not penetrate the tissue as deeply as conventional radiation. The radiation is delivered through a cone, usually toward the tumor bed. HDR treatment, however, can be administered only in adequately shielded rooms. It is delivered through parallel catheters in a flexible plastic flap, which can be cut to fit the region at risk and packed onto the curving pelvic surface. HDR brachytherapy may take up to an hour.
IORT has been used in locally advanced rectal cancer for more than 30 years, yet there is no convincing evidence that it decreases local recurrence or improves survival. The only multicenter randomized trial to date included 142 patients with locally advanced rectal cancer, who had received preoperative chemoradiation and were randomly assigned to either surgical resection alone or surgery plus IORT [73]. After a 5-year follow-up, the trial did not demonstrate any significant improvement in local recurrence or disease-free survival. Observational studies have reported conflicting results with respect to the efficacy of IORT. A recent systematic review of 15 individual studies, including the previously mentioned randomized trial, with 1929 patients in the IORT group and 2343 in the non-IORT group, concluded that IORT resulted in no definite improvement in overall survival or rate of recurrence for patients with R0 resections or for the total group (including R0, R1, and R2 resections) [74]. In the setting of locally advanced primary rectal cancers, we recommend having IORT available for patients if a close or threatened CRM is highly suspected, based on preoperative imaging. IORT is more commonly utilized in resection of recurrent rectal cancer if tissue planes have been previously disrupted, and discontinued foci of tumor may be present.
Flap Closure Following APR
Special attention to perineal closure is required after APR. The bony confines of the pelvis prevent tissue collapse, leading to significant dead space. Pelvic infection requiring opening of the perineum, prolonged wound healing, and chronic perineal sinuses are not uncommon. Multilayered closure to reduce dead space and liberal use of drains are common. However, in some cases rotating a well-vascularized omentum [75] or a mucocutaneous flap [76] into the pelvis should be considered, in order to reduce dead space and facilitate perineal healing after APR, especially in patients who have received pelvic radiation. A properly designed omental pedicle graft can be easily devised by dividing the gastrocolic omental attachments, detaching the left omentum from the spleen, and ligating the left gastroepiploic pedicle and the short gastric vessels. Care is taken to avoid injury to the right gastroepiploic, which allows the bulk of well-vascularized left omentum to rotate into and fill the pelvis. Rotation of the right omentum, based on the left gastroepiploic, is also feasible. In cases of exenteration, sacrectomy, extensive perineal skin loss, or requirement of vaginal reconstruction, a myocutaneous (vertical rectus abdominus myocutaneous, gracilis, or gluteal) flap is utilized.
Functional Outcomes
High rates of postoperative sexual and urinary dysfunction were a well-known phenomenon in the early years of rectal cancer surgery, ranging from 20 to 40% [77]. For example, registry data from Norway demonstrate that less than 50% of sexually active male were able to achieve erection 2 years after rectal resection. The rate fell to less than 20% in the cohort undergoing pelvic radiation and surgery [78].
Along with the advent of sharp dissection and precise technique emphasized in TME came the goal of identifying and preserving the autonomic pelvic nerves. As an integral part of the procedure, autonomic nerve preservation resulted in improved functional outcomes.
In an early study of 42 men undergoing sphincter-preserving operations for treatment of rectal cancer, Enker and colleagues reported high rates of potency (87%) and normal ejaculation (88%) after nerve-preserving proctectomy [79]. In a comprehensive study assessing sexual and urinary function in both women and men, through retrospective questionnaires, Havenga and colleagues reported the results of 136 patients undergoing nerve-sparing proctectomy [80]. They found that the ability to engage in intercourse was maintained by 86% of patients younger than 60 years and by 67% of patients 60 years and older. Eighty-seven percent of men maintained the ability to achieve orgasm. Type of surgery (APR compared to LAR) and age greater than 60 years were significantly associated with male sexual dysfunction. Women had similarly good results: 85% were able to experience arousal with vaginal lubrication, and 91% could achieve orgasm. The majority of patients had few or no complaints related to urinary function . Serious urinary dysfunction, such as neurogenic bladder, was not encountered.
The importance of autonomic nerve identification and preservation during proctectomy is also highlighted in a study by Shirouzou and colleagues, who assessed outcomes in 403 patients undergoing proctectomy, with or without autonomic nerve preservation, over a 20-year period [81]. In male patients who had proctectomy with nerve preservation, urinary function was preserved in greater than 80%, erection was preserved in 79%, and ejaculation in 65%; when proctectomy was performed without nerve preservation, urinary disorders were found in more than 90% and sexual dysfunction in virtually all patients, even those younger than age 60.
However, in patients with extensive pelvic disease, autonomic nerve preservation may not be feasible or oncologically sound. Involvement of the autonomic nerves by tumor, or lymphadenopathy in the pelvic sidewall, generally requires a resection that will affect nerve function permanently.
Despite suffering micturition and defecation problems, quality of life has consistently been shown to be better following an LAR compared an APR. This has been confirmed by comparative studies and in a meta-analysis of several studies [82–84]. Body image is consistently higher in patients undergoing an LAR versus APR, which may contribute to the inferior sexual function associated with APR.
In patients who undergo LAR, poor bowel function has been associated with the level of the anastomosis and the administration of pelvic radiotherapy. Low anastomoses (<3 cm) and coloanal anastomoses are associated with more incontinence of gas and solid stools compared to higher anastomoses [85]. Neoadjuvant radiation therapy causes fibrosis, leading to reduced compliance of the rectum and damage to the myenteric (Auerbach’s) plexus, and has been associated with higher rates of urgency, frequency, and fecal incontinence [86]. Some of the most telling data emanates from the prospective Dutch rectal cancer study, in which patients were randomized to proctectomy or neoadjuvant short-course radiotherapy plus proctectomy. Daytime incontinence was noted in 38% of patients in the surgery alone group and 62% of patients in the surgery plus radiotherapy group. Of even more concern is the finding that bowel dysfunction increased over time (studied at 2 years and 5 years after proctectomy) in the radiation cohort [87].
Oncologic Outcomes
Attention to detail during proctectomy, especially with regard to appropriate mesorectal excision , has been associated with improved local control and survival rates. Local pelvic failure rates following proctectomy at centers of excellence are now in the single digits [19, 21, 22, 88–91]. This is a substantial improvement compared to the local pelvic failure rates following proctectomy in the past, which were 3–5 times higher.
The importance of proper proctectomy technique is also reflected in a study from the Karolinska Institute reporting that in more than half of local recurrences in Sweden, evidence of residual mesorectal fat was identified on cross-sectional imaging, suggesting that incomplete mesorectal excision was the principal cause of local recurrence [92]. The same study claimed that extra-mesorectal lateral lymph node involvement accounted for only 6% of all locoregional recurrences.
The impact of training in proper proctectomy technique has been well documented. Surgical TME educational programs in Sweden, Norway, and the Netherlands have been shown to markedly reduce local recurrence, improve survival, and reduce the rate of permanent stomas [93–96]. In an observational national cohort study of 3319 patients in Norway, implementation of TME resulted in a decrease in local recurrence from 12 to 6% [96]. Survival rates were 73% after TME and 60% after conventional surgery—an overall improvement of 10–14%. In the Netherlands, the widespread adoption of TME led to a reduction in local recurrence of 16–9% [93]. In Sweden, implementation of specialized proctectomy training, utilization of neoadjuvant short-course radiotherapy , and referral of patients with rectal cancer to specialists has led to a fall in local recurrence rates: from 15% in the control group of the Stockholm I trial, and 14% in the Stockholm II trial, to 6% [97]. Cancer-related deaths fell from 15% to 16–9%. During the same period, the proportion of APR procedures performed in Sweden decreased by more than 50%. Along with participation in workshops and the increase in surgeons’ expertise, case volume directly influenced patient outcomes; when surgeons with high operative volume were compared to those with low volume, local recurrence was additionally reduced (from 10 to 4%), and there were fewer deaths from rectal cancer (18% vs. 11%) [94].
Another factor associated with oncologic outcome is the training and experience of the operating surgeon. Studies have shown that subspecialty training, surgeon experience, volume of cases, and treatment in high-volume tertiary care centers influence and enhance patient outcomes with respect to postoperative morbidity and mortality, local recurrence, and long-term survival [98–100].
Multidisciplinary Rectal Cancer Care
There is increasing evidence that multidisciplinary team management is associated with improved clinical decision-making, superior outcomes, and better patient experience in several types of cancer, including rectal cancer [101]. Cancer centers of excellence have been successfully established in several European countries over the past decade to address variability and disparity in the quality of rectal cancer care. Similar efforts in standardizing care to improve outcome have begun in the United States. The OSTRiCh (Optimizing the Surgical Treatment of Rectal Cancer) Consortium, founded in 2011, comprises a group of healthcare institutions across the United States, dedicated to improving delivery of rectal cancer care by relying on evidence-based and standardized care [102].
Variability in care was recently demonstrated in a study analyzing data from the National Cancer Data Base, which examined adherence to neoadjuvant chemoradiotherapy in 30,994 patients with clinical stage II and III rectal cancers [103]. The use of neoadjuvant radiation therapy and chemotherapy varied significantly by type of cancer center, with the highest rates of adherence observed in high-volume centers compared with low-volume centers (78% vs. 69%; adjusted odds ratio = 1.46; P < 0.001). This variation was mirrored by hospital geographic location, with little improvement observed over the last 5 years. These results further support the implementation of standardized care pathways for patients with rectal cancer.
Conclusion
The impact of optimal proctectomy technique in reducing the incidence of recurrence and improving long-term survival in rectal cancer is well established. The associated improvement in disease-free, recurrence-free, and overall survival, and increased improvement in bowel, bladder, and sexual function postoperatively, make proctectomy—with appropriate mesorectal excision and autonomic nerve preservation—the standard of care and a required part of colorectal surgical training. Complete surgical resection of the tumor and draining lymph nodes using sharp dissection are the basic principles of TME. Attention to preservation of the autonomic nerves can reduce the morbidity of this operation, improve functional outcomes, and provide a more acceptable quality of life. The use of multidisciplinary disease management teams, and implementation of centralization for the treatment of rectal cancer, has a strong potential to provide efficient delivery of evidence-based care.
References
Miles WE. A method of performing abdomino-perineal excision for carcinoma of the rectum and of the terminal portion of the pelvic colon. Lancet. 1908;2:1812–3.
Miles WE. The radical abdomino-perineal operation for cancer of the pelvic colon. BMJ. 1910;11:941–3.
Abel AL. The modern treatment of cancer of the rectum. Milwaukee Proc. March 3–5 1931; pp. 296–300.
Heald RJ. The ‘Holy Plane’ of rectal surgery. J R Soc Med. 1988;81(9):503–8.
Heald RJ, Ryall RD. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet. 1986;1:1479–82.
Zaheer S, Pemberton JH, Farouk R, Dozois RR, Wolff BG, Ilstrup D. Surgical treatment of adenocarcinoma of the rectum. Ann Surg Oncol. 1998;227:800–11.
Quirke P, et al. Local recurrence of rectal adenocarcinoma due to inadequate surgical resection. Histopathological study of lateral tumour spread and surgical excision. Lancet. 1986;2(8514):996–9.
Wilson SM, Beahrs OH. The curative treatment of carcinoma of the sigmoid, rectosigmoid, and rectum. Ann Surg. 1976;183:556–65.
Dukes C. The surgical pathology of rectal cancer. Proc R Soc Med. 1943;37:131.
McCall J, Cox MR, Wattchow DA. Analysis of local recurrence rates after surgery alone for rectal cancer. Int J Colorectal Dis. 1955;10:126–32.
Nagtegaal ID, Quirke P. What is the role for the circumferential margin in the modern treatment of rectal cancer? J Clin Oncol. 2008;26(2):303–12.
Quer EA, Dahlin DC, Mayo CW. Retrograde intramural spread of carcinoma of the rectum and rectosigmoid. Surg Gynecol Obstet. 1953;96:24–30.
Grinnel RS. Distal intramural spread of rectal carcinoma. Surg Gynecol Obstet. 1954;99:421–30.
Black WA, Waugh JM. The intramural extension of carcinoma of the descending colon, sigmoid and rectosigmoid. A pathological study. Surg Gynecol Obstet. 1948;1948:457–64.
Scott N, Jackson P, Al-Jaberi T, Dixon MF, Quirke P, Finan PJ. Total mesorectal excision and local recurrence: a study of tumour spread in the mesorectum distal to rectal cancer. Br J Surg. 1995;82:1031–3.
Williams NS, Dixon MF, Johnston D. Reappraisal of the 5 centimetre rule of distal excision for carcinoma of the rectum: a study of distal intramural spread and of patients’ survival. Br J Surg. 1983;70:150–4.
Karanjia ND, Corder AP, Bearn P, Heald RJ. Leakage from stapled low anastomosis after total mesorectal excision for carcinoma of the rectum. Br J Surg. 1994;81:1224–6.
Bokey EL, Öjerskog B, Chapuis PH, Dent OF, Newland RC, Sinclair G. Local recurrence after curative excision of the rectum for cancer without adjuvant therapy: role of total anatomical dissection. Br J Surg. 1999;86:1164–70.
Heald RJ, et al. Rectal cancer: the Basingstoke experience of total mesorectal excision, 1978–1997. Arch Surg. 1998;133(8):894–9.
Arenas RB, Fichera A, Mhoon D, Michelassi F. Total mesorectal excision in the surgical treatment of rectal cancer: a prospective study. Arch Surg. 1998;133:608–11.
Hainsworth PJ, Egan MJ, Cunliffe WJ. Evaluation of a policy of total mesorectal excision for rectal and rectosigmoid cancers. Br J Surg. 1997;84(5):652–6.
Arbman G, et al. Local recurrence following total mesorectal excision for rectal cancer. Br J Surg. 1996;83(3):375–9.
Moran B, Heald RJ. Manual of total mesorectal excision. London: CRC; 2013.
Quirke P, Dixon MF. The prediction of local recurrence in rectal adenocarcinoma by histopathological examination. Int J Colorectal Dis. 1988;3(2):127–31.
Maslekar S, et al. Mesorectal grades predict recurrences after curative resection for rectal cancer. Dis Colon Rectum. 2007;50(2):168–75.
Quirke P, et al. Effect of the plane of surgery achieved on local recurrence in patients with operable rectal cancer: a prospective study using data from the MRC CR07 and NCIC-CTG CO16 randomised clinical trial. Lancet. 2009;373(9666):821–8.
Nagtegaal ID, et al. Macroscopic evaluation of rectal cancer resection specimen: clinical significance of the pathologist in quality control. J Clin Oncol. 2002;20(7):1729–34.
College of American Pathologists. Protocol for the examination of specimens from patients with primary carcinoma of the colon and rectum. 2013 [cited 2015 July 17]. http://www.cap.org/ShowProperty?nodePath=/UCMCon/Contribution%20Folders/WebContent/pdf/colon-13protocol-3300.pdf.
Contant CM, et al. Mechanical bowel preparation for elective colorectal surgery: a multicentre randomised trial. Lancet. 2007;370(9605):2112–7.
Jung B, et al. Multicentre randomized clinical trial of mechanical bowel preparation in elective colonic resection. Br J Surg. 2007;94(6):689–95.
Guenaga KF, Matos D, Wille-Jorgensen P. Mechanical bowel preparation for elective colorectal surgery. Cochrane Database Syst Rev. 2011(9):p. CD001544.
Dahabreh IJ, Steele DW, Shah N, Trikalinos TA (2014) Agency for healthcare research and quality. Comparative effectiveness review. Number 128. Oral Mechanical Bowel Preparation for Colorectal Surgery. 2014 [cited 2015 July 17]. http://effectivehealthcare.ahrq.gov/ehc/products/458/1900/colorectal-surgery-preparation-report-140428.pdf.
Nelson RL, Gladman E, Barbateskovic M. Antimicrobial prophylaxis for colorectal surgery. Cochrane Database Syst Rev. 2014;5: p. CD001181.
Bratzler DW, et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Am J Health Syst Pharm. 2013;70(3):195–283.
Poggio JL. Perioperative strategies to prevent surgical-site infection. Clin Colon Rectal Surg. 2013;26(3):168–73.
Kakkos SK, et al. Combined intermittent pneumatic leg compression and pharmacological prophylaxis for prevention of venous thromboembolism in high-risk patients. Cochrane Database Syst Rev. 2008(4): p. CD005258.
Danielsen AK, Burcharth J, Rosenberg J. Patient education has a positive effect in patients with a stoma: a systematic review. Colorectal Dis. 2013;15(6):e276–83.
Bardram L, et al. Recovery after laparoscopic colonic surgery with epidural analgesia, and early oral nutrition and mobilisation. Lancet. 1995;345(8952):763–4.
Serclova Z, et al. Fast-track in open intestinal surgery: prospective randomized study (Clinical Trials Gov Identifier no. NCT00123456). Clin Nutr. 2009;28(6):618–24.
Spanjersberg WR, et al. Fast track surgery versus conventional recovery strategies for colorectal surgery. Cochrane Database Syst Rev. 2011(2): p. CD007635.
Lin S, et al. Meta-analysis of robotic and laparoscopic surgery for treatment of rectal cancer. World J Gastroenterol. 2011;17(47):5214–20.
Marr R, et al. The modern abdominoperineal excision: the next challenge after total mesorectal excision. Ann Surg. 2005;242(1):74–82.
den Dulk M, et al. The abdominoperineal resection itself is associated with an adverse outcome: the European experience based on a pooled analysis of five European randomised clinical trials on rectal cancer. Eur J Cancer. 2009;45(7):1175–83.
Nagtegaal ID, et al. Low rectal cancer: a call for a change of approach in abdominoperineal resection. J Clin Oncol. 2005;23(36):9257–64.
Enker WE, Levi GS. Macroscopic assessment of mesorectal excision. Cancer. 2009;115(21):4890–4.
Enker WE, et al. Abdominoperineal resection via total mesorectal excision and autonomic nerve preservation for low rectal cancer. World J Surg. 1997;21(7):715–20.
Holm T, et al. Extended abdominoperineal resection with gluteus maximus flap reconstruction of the pelvic floor for rectal cancer. Br J Surg. 2007;94(2):232–8.
West NP, et al. Multicentre experience with extralevator abdominoperineal excision for low rectal cancer. Br J Surg. 2010;97(4):588–99.
Han JG, et al. A prospective multicenter clinical study of extralevator abdominoperineal resection for locally advanced low rectal cancer. Dis Colon Rectum. 2014;57(12):1333–40.
Prytz M, et al. Extralevator abdominoperineal excision (ELAPE) for rectal cancer—short-term results from the Swedish Colorectal Cancer Registry. Selective use of ELAPE warranted. Int J Colorectal Dis. 2014;29(8):981–7.
Kang CY, et al. Robotic-assisted extralevator abdominoperineal resection in the lithotomy position: technique and early outcomes. Am Surg. 2012;78(10):1033–7.
Marecik SJ, et al. Robotic cylindrical abdominoperineal resection with transabdominal levator transection. Dis Colon Rectum. 2011;54(10):1320–5.
Weiser MR, et al. Sphincter preservation in low rectal cancer is facilitated by preoperative chemoradiation and intersphincteric dissection. Ann Surg. 2009;249(2):236–42.
Kodeda K, et al. Rectal washout and local recurrence of cancer after anterior resection. Br J Surg. 2010;97(10):1589–97.
Karanjia ND, et al. ‘Close shave’ in anterior resection. Br J Surg. 1990;77(5):510–2.
Pollett WG, Nicholls RJ. The relationship between the extent of distal clearance and survival and local recurrence rates after curative anterior resection for carcinoma of the rectum. Ann Surg. 1983;198(2):159–63.
Vernava III AM, et al. A prospective evaluation of distal margins in carcinoma of the rectum. Surg Gynecol Obstet. 1992;175(4):333–6.
Paty PB, et al. Treatment of rectal cancer by low anterior resection with coloanal anastomosis. Ann Surg. 1994;219(4):365–73.
Paty PB, et al. Long-term functional results of coloanal anastomosis for rectal cancer. Am J Surg. 1994;167(1):90–4. discussion 94-5.
Brown CJ, Fenech DS, McLeod RS. Reconstructive techniques after rectal resection for rectal cancer. Cochrane Database Syst Rev. 2008(2): p. CD006040.
Hallbook O, et al. Randomized comparison of straight and colonic J pouch anastomosis after low anterior resection. Ann Surg. 1996;224(1):58–65.
Heriot AG, et al. Meta-analysis of colonic reservoirs versus straight coloanal anastomosis after anterior resection. Br J Surg. 2006;93(1):19–32.
Si C, Zhang Y, Sun P. Colonic J-pouch versus Baker type for rectal reconstruction after anterior resection of rectal cancer. Scand J Gastroenterol. 2013;48(12):1428–35.
Matthiessen P, et al. Defunctioning stoma reduces symptomatic anastomotic leakage after low anterior resection of the rectum for cancer: a randomized multicenter trial. Ann Surg. 2007;246(2):207–14.
Tan WS, et al. Meta-analysis of defunctioning stomas in low anterior resection for rectal cancer. Br J Surg. 2009;96(5):462–72.
Gu WL, Wu SW. Meta-analysis of defunctioning stoma in low anterior resection with total mesorectal excision for rectal cancer: evidence based on thirteen studies. World J Surg Oncol. 2015;13(1):9.
Gunderson LL, et al. Revised TN categorization for colon cancer based on national survival outcomes data. J Clin Oncol. 2010;28(2):264–71.
Derici H, et al. Multivisceral resections for locally advanced rectal cancer. Colorectal Dis. 2008;10(5):453–9.
Smith JD, et al. Multivisceral resections for rectal cancer. Br J Surg. 2012;99(8):1137–43.
Sugihara K, et al. Indication and benefit of pelvic sidewall dissection for rectal cancer. Dis Colon Rectum. 2006;49(11):1663–72.
Yano H, Moran BJ. The incidence of lateral pelvic side-wall nodal involvement in low rectal cancer may be similar in Japan and the West. Br J Surg. 2008;95(1):33–49.
Georgiou P, et al. Extended lymphadenectomy versus conventional surgery for rectal cancer: a meta-analysis. Lancet Oncol. 2009;10(11):1053–62.
Dubois JB, et al. Intra-operative radiotherapy of rectal cancer: results of the French multi-institutional randomized study. Radiother Oncol. 2011;98(3):298–303.
Wiig JN, Giercksky KE, Tveit KM. Intraoperative radiotherapy for locally advanced or locally recurrent rectal cancer: does it work at all? Acta Oncol. 2014;53(7):865–76.
Killeen S, Devaney A, Mannion M, Martin ST, Winter DC. Omental pedicle flaps following proctectomy: a systematic review. Colorectal Dis. 2013;15(11):e634–45.
Chessin DB, Hartley J, Cohen AM, Mazumdar M, Cordeiro P, Disa J, Mehrara B, Minsky BD, Paty P, Weiser M, Wong WD, Guillem JG. Rectus flap reconstruction decreases perineal wound complications after pelvic chemoradiation and surgery: a cohort study. Ann Surg Oncol. 2005;12(2):104–10.
Camilleri-Brennan J, Steele RJ. Quality of life after treatment for rectal cancer. Br J Surg. 1998;85(8):1036–43.
Bruheim K, et al. Late side effects and quality of life after radiotherapy for rectal cancer. Int J Radiat Oncol Biol Phys. 2010;76(4):1005–11.
Enker WE. Potency, cure, and local control in the operative treatment of rectal cancer. Arch Surg. 1992;127(12):1396–401. discussion 1402.
Havenga K, et al. Male and female sexual and urinary function after total mesorectal excision with autonomic nerve preservation for carcinoma of the rectum. J Am Coll Surg. 1996;182(6):495–502.
Shirouzu K, Ogata Y, Araki Y. Oncologic and functional results of total mesorectal excision and autonomic nerve-preserving operation for advanced lower rectal cancer. Dis Colon Rectum. 2004;47(9):1442–7.
Cornish JA, et al. A meta-analysis of quality of life for abdominoperineal excision of rectum versus anterior resection for rectal cancer. Ann Surg Oncol. 2007;14(7):2056–68.
Engel J, et al. Quality of life in rectal cancer patients: a four-year prospective study. Ann Surg. 2003;238(2):203–13.
Kasparek MS, et al. Quality of life after coloanal anastomosis and abdominoperineal resection for distal rectal cancers: sphincter preservation vs quality of life. Colorectal Dis. 2011;13(8):872–7.
Guren MG, et al. Quality of life and functional outcome following anterior or abdominoperineal resection for rectal cancer. Eur J Surg Oncol. 2005;31(7):735–42.
Birgisson H, et al. Late adverse effects of radiation therapy for rectal cancer—a systematic overview. Acta Oncol. 2007;46(4):504–16.
Lange MM, et al. Risk factors for faecal incontinence after rectal cancer treatment. Br J Surg. 2007;94(10):1278–84.
MacFarlane JK, Ryall RD, Heald RJ. Mesorectal excision for rectal cancer. Lancet. 1993;341(8843):457–60.
Enker WE, et al. Total mesorectal excision in the operative treatment of carcinoma of the rectum. J Am Coll Surg. 1995;181(4):335–46.
Bjerkeset T, Edna TH. Rectal cancer: the influence of type of operation on local recurrence and survival. Eur J Surg. 1996;162(8):643–8.
Kockerling F, et al. Influence of surgery on metachronous distant metastases and survival in rectal cancer. J Clin Oncol. 1998;16(1):324–9.
Syk E, et al. Local recurrence in rectal cancer: anatomic localization and effect on radiation target. Int J Radiat Oncol Biol Phys. 2008;72(3):658–64.
Kapiteijn E, Putter H, van de Velde CJ. Impact of the introduction and training of total mesorectal excision on recurrence and survival in rectal cancer in The Netherlands. Br J Surg. 2002;89(9):1142–9.
Martling A, et al. The surgeon as a prognostic factor after the introduction of total mesorectal excision in the treatment of rectal cancer. Br J Surg. 2002;89(8):1008–13.
Wibe A, et al. Total mesorectal excision for rectal cancer—what can be achieved by a national audit? Colorectal Dis. 2003;5(5):471–7.
Wibe A, et al. A national strategic change in treatment policy for rectal cancer—implementation of total mesorectal excision as routine treatment in Norway. A national audit. Dis Colon Rectum. 2002;45(7):857–66.
Martling AL, et al. Effect of a surgical training programme on outcome of rectal cancer in the County of Stockholm. Stockholm Colorectal Cancer Study Group, Basingstoke Bowel Cancer Research Project. Lancet. 2000;356(9224):93–6.
Helsper JT. Impact of the surgeon on cancer management outcomes. J Surg Oncol. 2003;82(1):1–2.
Luna-Perez P, et al. The surgeon as prognostic factor for local recurrence and survival in the anal sphincter preservation for mid-rectal cancer. Rev Invest Clin. 1999;51(4):205–13.
Renzulli P, Laffer UT. Learning curve: the surgeon as a prognostic factor in colorectal cancer surgery. Recent Results Cancer Res. 2005;165:86–104.
Dietz DW. Multidisciplinary management of rectal cancer: the OSTRICH. J Gastrointest Surg. 2013;17(10):1863–8.
The Consortium for Optimizing the Treatment of Rectal Cancer (OSTRiCh). 2014 [cited 2015 July 17]. http://www.ostrichconsortium.org/index.html.
Monson JR, et al. Failure of evidence-based cancer care in the United States: the association between rectal cancer treatment, cancer center volume, and geography. Ann Surg. 2014;260(4):625–31. discussion 631-2.
Guillem JG, Lee-Kong SA. Autonomic nerve preservation during rectal cancer resection. J Gastrointest Surg. 2010;14:416–22.
Janjua AZ, Moran B, Heald RJ. Open surgical management of rectal cancer. In: Patel HRH, Mould T, Joseph JV, Delaney CP, editors. Pelvic cancer surgery: modern breakthroughs and future advances. New York: Springer; 2015. p. 531.
Heald RJ, et al. Embryology and anatomy of the rectum. Semin Surg Oncol. 1998;15(2):66–71.
Hockel M. Laterally extended endopelvic resection for the treatment of locally advanced and recurrent cervical cancer. In: Patel HRH, Mould T, Joseph JV, Delaney CP, editors. Pelvic cancer surgery: modern breakthroughs and future advances. New York: Springer; 2005.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 ASCRS (American Society of Colon and Rectal Surgeons)
About this chapter
Cite this chapter
Pappou, E.P., Weiser, M.R. (2016). Proctectomy. In: Steele, S.R., Hull, T.L., Read, T.E., Saclarides, T.J., Senagore, A.J., Whitlow, C.B. (eds) The ASCRS Textbook of Colon and Rectal Surgery. Springer, Cham. https://doi.org/10.1007/978-3-319-25970-3_31
Download citation
DOI: https://doi.org/10.1007/978-3-319-25970-3_31
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-25968-0
Online ISBN: 978-3-319-25970-3
eBook Packages: MedicineMedicine (R0)