
Abstract
Since its introduction in 1967, the Hill repair has proven to be an effective and durable surgical intervention for the management of gastroesophageal reflux disease. In addition to the standard tenets of antireflux surgery, it incorporates three key anatomic concepts: the intra-abdominal posterior fixation of the gastroesophageal junction (GEJ), the pivotal role of the lower esophageal sphincter collar sling musculature in the proper reconstruction of the GEJ, and the importance of the gastroesophageal valve for the competence of the antireflux barrier. It has undergone two major modifications since its inception including conversion from an open to a laparoscopic procedure, and incorporation into a new operation to include a Nissen fundoplication wrap as part of the Nissen-Hill hybrid procedure. The original Hill procedure, as well as its variants, demonstrated excellent long-term outcomes in the surgical management of uncomplicated and complicated gastroesophageal reflux disease as well as paraesophageal hernias. We will discuss the history, principles, techniques, and results of the Hill Repair and Nissen-Hill hybrid antireflux operations.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Antireflux surgery
- Gastroesophageal reflux disease
- Hill repair
- Nissen-Hill hybrid
- Manometry
- Lower esophageal sphincter
- Gastroesophageal valve
- Gastroesophageal junction
Introduction
In 1967, Lucas D. Hill introduced the Hill Repair to the American Surgical Association, and it transformed the field of antireflux surgery [1]. The principles behind the Hill repair were derived from detailed anatomical dissections and incorporated the regular use of preoperative and intraoperative esophageal manometry and pH testing. The science and objective measures behind the Hill repair not only facilitated the creation of a highly effective and durable antireflux operation, but also set standards in an emerging field that continue to be utilized in present day [2, 3]. Incorporating the knowledge and technical aspects of the repair into one’s repertoire enhances the understanding of the function and anatomy of both the gastroesophageal junction (GEJ) and its modification by antireflux procedures and broadens the surgical options available for both straightforward and complex surgical repairs.
Advantages of the Hill Repair
- 1.
-
2.
Accurately reproduces normal anatomy, with inferior fixation of the gastroesophageal junction (GEJ) and complete reconstruction of the antireflux barrier without reliance on a fundoplication, thus reducing herniation and wrap slippage and enabling use following partial gastrectomy or gastric bypass [5, 6].
-
3.
Esophageal lengthening procedure generally not required, even in instances of short esophagus [7].
-
4.
Intraoperative manometric control over the final lower esophageal sphincter (LES) pressure, allowing for an individualized tailored surgical repair. Suitable for patient with ineffective esophageal motility and a very low incidence of long-term dysphagia [8].
-
5.
Maintenance of the short gastric vessels and associated low incidence of postoperative gas bloat [5].
Principles of Repair
The Hill repair incorporates three important anatomical concepts: (1) the intra-abdominal posterior fixation of the GEJ; (2) the central role of the collar sling musculature of the LES in the proper reconstruction of the GEJ; and (3) the importance of the gastroesophageal valve (GEV) for the competence of the antireflux barrier, while adhering to traditional tenets of antireflux surgery, including closure of the crura, configuring an intra-abdominal segment of distal esophagus, and reestablishing total/intra-abdominal length and pressure of the LES.
The anatomical reconstruction of the GEJ is accomplished through the Hill repair sutures, which anchor the anterior and posterior aspects of the LES collar sling musculature to the preaortic fascia just superior to the celiac trunk. A thorough understanding of the LES anatomy facilitates proper placement of the Hill sutures. As previously delineated by Liebermann-Meffert, the clasp fibers of the lesser curvature on the LES interdigitate with the collar sling musculature of the oblique gastric muscle layer, the latter of which forms a horseshoe arching over the anterior, posterior, and greater curvature (angle of His) aspects of the GEJ (Fig. 6.1) [9]. Four successively placed Hill sutures through the sling fibers allow for progressive downward tension on the sling fibers and accentuation of the angle of His. Intraoperative manometry is utilized to assess appropriate tension of the Hill sutures and allows for an individualized tailoring of the valve and antireflux barrier [10].

Diagrammatic illustration of the collar sling musculature
Hill Repair Technique
A complete list of the equipment required for a laparoscopic Hill antireflux procedure can be found in Table 6.1.
Manometry Catheter and Bougie Dilator Placement
The manometric equipment is prepared prior to initiation of the operation. The manometry catheter is a water-perfused, single-use eight channel catheter, with four pressure ports at 0 cm from the tip, and subsequent ports at 5-cm intervals. The catheter is placed through a clear 44–48 Fr dilator with the distal pressure port 10 cm beyond the tapered tip of the dilator and secured with tape at the proximal end. The bougie and attached catheter is then passed through the esophagus to 30 cm at the beginning of the case by the surgeon or an experienced anesthesiologist, taking care that the manometric catheter remains properly oriented and is not folded upon itself. The distal channel is connected to a transducer and anesthesia monitor—at pulmonary artery catheter settings for greatest sensitivity—or to a dedicated esophageal manometry system.
Patient Positioning and Port Placement
Our standard positioning is low dorsal lithotomy with both arms out at 90°. The surgeon stands between the legs, the assistant on the patient’s left, and the camera operator or robotic arm for camera fixation on the right. Five trocars are used for the operation. It is noteworthy that a 10–11 mm assistant port is placed just below the left costal margin in the mid-clavicular line, or more medially when the costal margin is narrow. This requires placement of the surgeons’ right-hand work port more inferiorly than would be typical for a Nissen repair (Fig. 6.2a), but the assistant port location facilitates management of the Hill sutures (Fig. 6.2b). A sixth optional port for downward traction of lesser curvature fat may be added in the left lower quadrant to gain better exposure to the preaortic fascia; this exposure is critical to placement of the preaortic sutures and may be particularly helpful with obese patients. The left lobe of the liver is elevated with a 5-mm Nathanson retractor and fixed to a self-retaining table mounted system.

(a) Trochar placement for the laparoscopic Nissen and Nissen-Hill hybrid repair. (b) Trochar placement for the laparoscopic Hill repair
Hiatal Dissection and Closure
Dissection is performed with ultrasonic shears. Care is taken to dissect along the superior aspect of the phrenoesophageal fat pad (Hill’s phrenoesophageal bundle) and bring it down with the dissection, keeping it attached to the GEJ. Following dissection, the anterior and posterior fat pad/bundles are trimmed as necessary to eliminate hernia sac and redundancy, while avoiding the lesser curvature and the vagus nerves. The short gastric vessels are not routinely taken, but it is essential with a Hill repair to free the entire posterior fundus by opening the lesser sac from left gastric artery to GEJ. This is accomplished from the lesser curvature aspect and facilitated with critical exposure provided by the assistant, who lifts the posterior phrenoesophageal tissue immediately posterior to the posterior vagus nerve. The location of the celiac trunk should be roughly identified (though not dissected) and the preaortic fascia and overlying diaphragmatic muscle should be exposed down to the level of the celiac axis. (The preaortic fascia is a dense connective tissue layer that lies deep to the inferior fusion of the right and left crura and extends inferiorly to the celiac axis, where its inferior edge forms the median arcuate ligament.) Dissection is continued into the mediastinum to obtain adequate length of intra-abdominal esophagus. A Penrose drain is not routinely utilized, as it would be in the way of subsequent suture placement. Following dissection, the hiatus is closed posteriorly with 0-braided non-absorbable suture using an extracorporeal knot pusher or the Ti-Knot device. For larger hernias, some of the hiatal repair may need to be completed anteriorly, since too much angulation of the esophagus may be created from excessive posterior closure and subsequent posterior fixation of the GEJ to the preaortic fascia.
Hill Sutures: Anatomical Landmarks
The Hill sutures are placed through the collar sling musculature of the GEJ (see Fig. 6.1). This lies immediately beneath the phrenoesophageal ligament (Hill’s phrenoesophageal bundles), commencing just to the patient’s left and anterior to the anterior vagus nerve, extending over the angle of His and ending just to the patient’s right and posterior to the posterior vagus nerve. Thus, the vagus nerves are important landmarks and must be identified. The anterior vagus nerve is found under tension by pulling down on the lesser curvature tissue. The posterior vagus nerve is found by lifting the posterior fat pad upward and to the patient’s right, as it consistently lies in the groove between the fundus and esophagus created by this maneuver. It is usually necessary to trim part of the anterior and posterior esophageal fat pads to delineate the appropriate anatomy.
Hill Sutures: Placement
Following hiatal closure, four Hill sutures of multicolored 48 in. 0-Ethibond are placed and left untied and clamped externally. This is the most critical part of the repair, and exact placement is important (Fig. 6.3 ). The first two sutures are introduced through the surgeon’s right-hand working port, while the third and fourth are introduced through the assistant port in the left upper quadrant. There are three separate and distinct bites of tissue with each suture, the first being placement through the anterior bundle/collar sling musculature from inferior to superior; the second being placement through the posterior bundle/collar sling musculature from superior to inferior; and the third being transverse placement through the inferior aspect of the preaortic fascia. Placement of the posterior bundle sutures may be aided by preliminarily fixing the superior aspect of the posterior fundus to the left crus and left aspect of the preaortic fascia with 1–2 sutures.

Illustration of the Hill sutures
-
Anterior Bundle : The first bite of the first suture is placed immediately to the patient’s left of the anterior vagus nerve. Grasping the bundle with the left hand and maneuvering the tissue over the needle facilitates this placement. This bite must go deeply enough to grab the collar sling musculature, and as previously discussed, it is usually necessary to trim away part of the anterior fat pad to expose this anatomy (Fig. 6.4).
Fig. 6.4 
First Hill suture, first bite: intraoperative view
-
Posterior Bundle : The second bite of the same suture is placement through the posterior bundle. The assistant exposes the posterior vagus nerve by grasping the lesser curvature tissue between the vagus nerves and retracting it anteriorly and to the left. The surgeon grasps and manipulates the posterior bundle with the left hand. Beginning just posterior to the posterior vagus, the suture is passed through the bundle in a superior to inferior direction, including the underlying collar sling musculature. To do this successfully, the needle will frequently need to be perpendicular to the tissue at the time of entry (Fig. 6.5).
Fig. 6.5 
First Hill suture , second bite: intraoperative view
-
Preaortic Fascia : The final bite is transverse placement through the preaortic fascia. The assistant retracts the GEJ to the left and inferiorly for exposure. The suture is passed through the preaortic tissue inferiorly, immediately superior to the fatty tissue overlying the celiac axis. The location of this suture determines the final length of intra-abdominal esophagus, so it is important to be sufficiently inferior. The aorta lies 5–10 mm deep and may be avoided by lifting the tissue upward with a grasper and driving the needle transversely from left to right, rather than posteriorly (Fig. 6.6 ). Finally, the suture is then retracted through the working port, taking care to brace the suture internally with a grasper to avoid excess tissue trauma. It is then clamped externally with a hemostat (Fig. 6.7).
Fig. 6.6 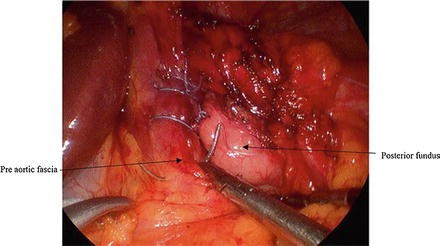
First Hill suture, third bite: intraoperative view
Fig. 6.7 
First Hill suture, completed but not tied: intraoperative view




This same process is repeated with three more sutures; the second suture also going through the surgeon’s right hand work port, while the third and fourth sutures are introduced and withdrawn through the left upper quadrant assistant port. Each suture advances 2–3 mm further up the two bundles (e.g., in the direction of the angle of His) and the preaortic fascia. With excessive advancement, the repair will be too snug, whereas with inadequate advancement the repair may be too loose. The uppermost suture should enter the anterior bundle at approximately the left lateral border of the esophagus . It should enter the posterior bundle at its upper extent without going behind the esophagus. Colors should alternate to aid in identification and prevention of tangling. Care should be given to the angle of entry of the sutures through the ports, to also prevent crossing. Three-eighths inch Teflon pledgets may be added to either end of the sutures; it has been our standard to add pledgets to the second and fourth sutures.
Hill Sutures: Fixation and Manometric Measurements
With all repair sutures placed but not tied, the 48 Fr dilator/manometry catheter is carefully advanced and positioned across the GEJ, and the top 2 sutures, i.e., those through the left assistant port, are tied sequentially with a single half-hitch and clamped internally just above the knots with needle holders. The left hand instrument clamps the most superior suture, while the right-hand instrument clamps the second inferior suture. These two sutures are highest on the collar sling musculature and will therefore have the greatest impact on lower esophageal sphincter pressure.
Manometric measurements are taken by withdrawing the dilator/catheter system until the pressure port is 5 cm below the repair. A relative baseline intragastric pressure of zero should be established by raising or lowering the transducer, and fixing it at that point, the catheter is then slowly withdrawn at a rate of 1 cm/s. This should be done more slowly if an arterial monitor is used, especially during crossing of the high-pressure zone, in order to capture the highest peak. The ideal pressure is 30–40 mmHg. The first increase in pressure encountered during pull-through is the repair, whereas an additional spike representing the diaphragm may be seen just proximal to this.
The manometric pressure of the GEJ may then be adjusted by tightening or loosening the Hill sutures as needed. If the pressure is clearly too low, an additional superior suture may be placed as deemed appropriate. When satisfactory pressure has been obtained, the dilator is again positioned across the GEJ and all sutures are extracorporally tied at the established tension before taking a final manometric reading. Figure 6.8 shows the completed Hill repair.

Completed Hill repair: intraoperative view
The Hill repair may be performed over a 40–45 Fr bougie without the use of intraoperative manometrics, as many of Hill’s former students have done. In our experience, intraoperative manometrics has altered the operation approximately 30 % of the time [10].
Completion of the Repair
The anterior hiatus is often reinforced with one or two sutures to prevent further attenuation and as a preferred alternative to excess posterior closure. Mesh may be used at the discretion of the surgeon, but excess posterior bulk should be avoided. The fundus is sutured to the anterior rim of the hiatus along both right and left crura, to prevent herniation and accentuate the valve.
Postoperative Care
Postoperative care is standard. Nasogastric suction is not routinely utilized. The patient is kept on full liquids for 2 weeks, and then advanced slowly to a normal diet by 6 weeks.
Results of the Hill Repair
The Hill repair is highly effective and durable. The durability of the Hill repair was shown in a large multi-institution study of 1184 patients with long-term follow-up (2–25 years, mean follow-up of 10 years), demonstrating a 93 % long-term clinical success rate and only a 1.9 % reoperation rate [2]. The Hill repair has been successfully translated into laparoscopic technique, with over 2500 laparoscopic repairs having been performed. Clinical results have been nearly identical to the open repair [3]. The effectiveness and safety of the Hill repair has also been demonstrated for patients with diminished esophageal peristalsis [8], and for those with para-esophageal hernia and short esophagus, without the need for an esophageal lengthening procedure [7].
The Hill repair has also been compared to the standard Nissen fundoplication. In a recent multi-institution randomized controlled trial comparing the laparoscopic Nissen and Hill repairs, the Hill was equivalent to the Nissen in every parameter of clinical success and repair failure, including symptomatic and physiologic control of reflux, except that, in contrast to the Nissen repair it did not raise lower esophageal sphincter pressure significantly above baseline. This may be an advantage in cases of ineffective esophageal motility. There was also a trend toward less gas bloating [3]. The results of this updated study supersede the only other randomized comparison of the two operations, done in the 1970s [11] in which the Nissen was deemed superior; however, the sample size and description of the Hill technique in that study raises concern about the standardization and quality of the Hill repair that was performed.
A failure of the Hill repair is clinically apparent with the return of reflux symptoms in the setting of positive pH testing, with or without evidence of a recurrent hiatal hernia on an upper gastrointestinal series (Figs. 6.9 and 6.10). The initial failure is believed to result from loosening and attenuation of the anterior bundle repair sutures, as a result of radial forces, which decreases the fixation and strength of the GEJ. As with any reoperative procedure, the technical difficulty is greater than that of the primary repair, principally as a result of the increased difficulty of dissection [12]. Careful attention to dissection of the posterior bundle sutures and fundus from the preaortic fascia is required. Barring any contraindications, such as significant esophageal dysmotility, we have managed recurrent disease with conversion of the Hill Repair to the Nissen-Hill Hybrid Repair.

Barium swallow : Hill failure without hiatal hernia recurrence

Barium swallow: Hill failure with hiatal hernia recurrence
The Nissen-Hill Hybrid Repair
The Nissen-Hill hybrid has become our preferred repair for reoperations, paraesophageal hernias, and in cases of short esophagus . As previously discussed, the most common failure of the Hill repair is from loosening and attenuation of the anterior bundle sutures, with herniation of the GEJ being relatively uncommon [3]. Contrarily, the most common failure of the Nissen fundoplication is mediastinal herniation of the wrap ; the second most common failure is a slipped Nissen, resulting from cephalad herniation of the GEJ and cardia through the wrap, with the wrap remaining intra-abdominal [3, 13]. Both of these failures reflect inadequate fixation of the GEJ within the abdomen. In a recent randomized trial comparing 46 Nissen fundoplications to 56 Hill repairs, there were two reoperations in the Nissen group, both for mediastinal herniation of the wrap; and there were two reoperations in the Hill group, both for loosening of the repair [3].
The Nissen-Hill hybrid repair incorporates the structural features of both repairs, offsetting the weakness of one repair with the integrity of the other. Two Hill sutures securely anchor the GEJ within the abdomen to maintain axial integrity , while a full 360° Nissen wrap maintains radial integrity. It is not simply an anchored Nissen wrap, in that it is the GEJ, rather than the wrap, which is anchored, resulting in complementary merger of the two repairs.
Nissen-Hill Hybrid Technique
Positioning and dissection are as described for the Hill repair, except that the port placement is as it is for a Nissen repair, with the surgeon’s right-hand work port higher beneath the left costal margin and the 5 mm assistant port placed left lateral, just below the costal margin (see Fig. 6.2a). The dissection is similar except that the short gastric vessels are routinely taken and a Penrose drain is placed around the GEJ for downward traction during mediastinal dissection and construction of the Nissen wrap. The gastroesophageal fat pad and associated hernia sac are routinely removed except along the lesser curvature, taking care to protect both vagus nerves . The hiatus is closed posteriorly with 0-braided non-absorbable suture.
Following hiatal closure, there are four components to the Nissen-Hill hybrid repair:
Nissen Configuration
A marking suture is placed on the posterior fundus by traveling 6 cm below the GE junction along the greater curvature and one third of the distance from greater to lesser curvature. A mirror-image mark is made on the anterior fundus with a marking pen. The posterior fundus is brought behind the esophagus and a “shoe-shine” maneuver is then performed to ensure full mobility of the fundus and a 1:1 relationship between anterior and posterior fundus. No fundoplication sutures are placed at this time.
Placement of Hill Sutures
The two lower of the four standard Hill sutures are then placed through the collar sling musculature and preaortic fascia as previously described (Fig. 6.1) [5]. The ends of each suture are brought out through the trocar, clipped together, and returned into the abdomen and placed inferiorly and laterally out of the field until the Nissen is completed.
Modified Hybrid Repair
In elderly patients or those with poor esophageal motility, Hill suture bites through the anterior collar sling may be omitted, using only bites through the posterior collar sling and the preaortic fascia. This still provides competent posterior intra-abdominal fixation of the GE junction, but without the aggressiveness of the anterior collar sling sutures.
Nissen Construction
The Nissen repair is then completed in a standardized fashion [14, 15] over a 58 Fr dilator utilizing a horizontal mattress 2-0 double-armed prolene suture with double-mounted 5/8″ Teflon pledgets on either side, suturing anterior to posterior fundus and incorporating the wall of the esophagus along its lesser curvature aspect (9:00 position) (Fig. 6.11). The sutures are tied using a Ti-Knot device. Two additional fundus-to-fundus sutures are then placed and tied, 5 mm above and 5 mm below the horizontal mattress suture, to create a 2–2.5 cm “floppy” Nissen wrap (Fig. 6.12).

Illustration of the Nissen-Hill hybrid sutures in place (untied)

Illustration of a completed Nissen-Hill hybrid repair (tied)
Completion of the Hill Sutures and EGD
With the dilator in place, the Hill sutures are retrieved in reverse order, redundant tissue along the lesser curvature is retracted inferiorly, and the sutures are tied down with the Tie-knot. Intraoperative manometry is not done as the repair is performed over a large dilator. The laxity of the anterior hiatus is assessed before and after removing the dilator and is typically reinforced and/or further closed with one or more sutures to prevent subsequent widening and herniation. Biologic absorbable mesh is used routinely in cases of para-esophageal hernia. This should be low-profile material so as not to create excess bulk behind the esophagus. The corresponding intraoperative pictures of the Hybrid repair, with the Nissen already in place, and placement of mesh toward the end can be seen in Figs. 6.13, 6.14, and 6.15.

Nissen wrap completed , hybrid sutures in place: intraoperative view

Completed hybrid repair: intraoperative view

Mesh placement in cases of para-esophageal hernia: intraoperative view
We routinely perform flexible upper endoscopy to assess calibration of the repair and the valve configuration. This is a helpful tool to aid the surgeon in refining technique and will occasionally prevent a disastrous outcome.
Results of the Hybrid Repair
With short-term follow-up in over 150 hybrid repairs, the results continue to exceed our initial expectations. After an initial feasibility and safety trial on patients with para-esophageal hernia and Barrett’s metaplasia [16], the procedure has now been extended to patients with uncomplicated reflux. Gratifyingly, there has been no noticeable increase in complications or short to mid-term side effects, and the recurrence rate has been lower than predicted with traditional repair. In the first 50 patients with para-esophageal hernia undergoing hybrid repair, there was only one clinical recurrence at 13-month follow-up; there were three small asymptomatic fundic herniations with the GE junction intact and no reflux on pH testing; only two patients had resumed antisecretory medication, and preoperative symptoms were controlled in 98 %. There were significant improvements in all parameters of quality of life metrics, including dysphagia [17]. Similar success has been achieved in a smaller group of patients with Barrett’s metaplasia.
A recent mid-term cohort analysis of 153 patients who underwent Hybrid, Nissen, or Hill repair for uncomplicated GERD demonstrated an equivalent improvement in quality of life between the three repairs, but significantly reduced dysphagia rate and a trend toward reduced recurrences in those who had a Hybrid repair compared to a standard Nissen or Hill repair [18].
Summary
The Hill repair is at least equivalent in short-term clinical outcomes to the Nissen fundoplication in the surgical management of uncomplicated gastroesophageal reflux, and it may have advantages in the management of short esophagus and ineffective esophageal motility. In addition, as it is based on different anatomic and functional concepts than the Nissen, it gives additional insight into the multi-modality and critical aspects of a successful antireflux operation.
The open repair has been shown to be highly durable with up to 25-year follow-up, and the operation has been successfully translated into a laparoscopic approach, with clinical results that match the open approach. Its technical performance is well within the scope of any qualified esophageal surgeon, and the technical details of manometric calibration and precise suture placement have been standardized and simplified.
The Nissen-Hill hybrid repair incorporates features of each of the individual repairs and acts in a synergistic manner, offsetting the weakness of one with the advantages of the other. Like the Hill repair, it is also particularly useful in cases of short esophagus, as it anchors the GE junction intra-abdominally and obviates the need for an esophageal lengthening procedure. Short- and mid-term results suggest that this approach may be superior to either the Nissen or the Hill in cases of para-esophageal hernia or short esophagus, without an increase in side effects or complications.
References
Hill LD. An effective operation for hiatal hernia: an eight year appraisal. Ann Surg. 1967;166(4):681–92.
Aye RW, et al. The Hill antireflux repair at 5 institutions over 25 years. Am J Surg. 2011;201(5):599–604.
Aye RW, et al. A randomized multi institution comparison of the laparoscopic Nissen and Hill repairs. Ann Thorac Surg. 2012;94(3):951–8.
Low DE, et al. Fifteen- to twenty-year results after the Hill antireflux operation. J Thorac Cardiovasc Surg. 1989;98(3):444–9. discussion 449–50.
Aye R. The Hill procedure for gastroesophageal reflux [AU1]. 1st ed. Philadelphia: Harcourt Health Sciences; 2001.
Aye R, Gupta A. Antireflux surgery: the Hill antireflux operations repair and its variants. New York: Springer; 2014.
Jobe BA, et al. Laparoscopic management of giant type III hiatal hernia and short esophagus. Objective follow-up at three years. J Gastrointest Surg. 2002;6(2):181–8. discussion 188.
Aye RW, Mazza DE, Hill LD. Laparoscopic Hill repair in patients with abnormal motility. Am J Surg. 1997;173(5):379–82.
Korn O, et al. Gastroesophageal sphincter: a model. Dis Esophagus. 1997;10(2):105–9.
Schneider A, Aye R. Impact of intraoperative manometry on the Hill repair. Abstract presented at North Pacific Surgical Association, 14–15 Nov 2014. 2014.
Demeester TR, Johnson LF, Kent AH. Evaluation of current operations for the prevention of gastroesophageal reflux. Ann Surg. 1974;180(4):511–25.
Pennathur A, et al. Minimally invasive redo antireflux surgery: lessons learned. Ann Thorac Surg. 2010;89(6):S2174–9.
Horgan S, et al. Failed antireflux surgery: what have we learned from reoperations? Arch Surg. 1999;134(8):809–15. discussion 815–7.
DeMeester TR, Bonavina L, Albertucci M. Nissen fundoplication for gastroesophageal reflux disease. Evaluation of primary repair in 100 consecutive patients. Ann Surg. 1986;204(1):9–20.
Attwood SE, et al. Standardization of surgical technique in antireflux surgery: the LOTUS trial experience. World J Surg. 2008;32(6):995–8.
Qureshi AP, et al. The laparoscopic Nissen-Hill hybrid: pilot study or a combined antireflux procedure. Surg Endosc. 2013;27(6):1945–52.
Aye RW, et al. Laparoscopic Nissen-Hill hybrid: a promising solution for Type III paraesophageal hernia. Abstract Poster presentation at Digestive Disease Week, 20 May, 2013. 2013.
Schneider AM et al. Does the Nissen-Hill hybrid repair reduce recurrence rates for uncomplicated GERD? Abstract Poster presentation at Society of American Gastrointestinal and Endoscopic Surgeons 16–17 Apr 2015. 2015.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Warren, H., Aye, R.W. (2016). Alternatives to Nissen Fundoplication: The Hill Repair and the Nissen-Hill Hybrid. In: Aye, R., Hunter, J. (eds) Fundoplication Surgery. Springer, Cham. https://doi.org/10.1007/978-3-319-25094-6_6
Download citation
DOI: https://doi.org/10.1007/978-3-319-25094-6_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-25092-2
Online ISBN: 978-3-319-25094-6
eBook Packages: MedicineMedicine (R0)