
Abstract
Current definition of electrical storm (ES) is the occurrence of three or more episodes of sustained ventricular tachycardia (VT) or ventricular fibrillation (VF) within 24 h requiring appropriate medical intervention. The same definition applies in implantable cardioverter-defibrillator (ICD) carriers in which ES is defined by three or more appropriate and separate (at least 5 min) device interventions in 24 h, either with antitachycardia pacing (ATP) or shock [1].
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Ventricular Tachycardia
- Catheter Ablation
- Ventricular Assistance Device
- Inappropriate Therapy
- Electrical Storm
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
12.1 Focusing on the Issue
Current definition of electrical storm (ES) is the occurrence of three or more episodes of sustained ventricular tachycardia (VT) or ventricular fibrillation (VF) within 24 h requiring appropriate medical intervention. The same definition applies in implantable cardioverter-defibrillator (ICD) carriers in which ES is defined by three or more appropriate and separate (at least 5 min) device interventions in 24 h, either with antitachycardia pacing (ATP) or shock [1].
Current guidelines recommend ICD implantation for secondary prevention of sudden cardiac death (SCD) in survivors of cardiac arrest with no correctable causes and in patients with sustained symptomatic VT of different etiology. They also recommend ICD implantation for primary prevention in patients with ischemic or nonischemic dilated cardiomyopathy and ejection fraction equal or lower than 35 % after at least 3 months of optimized medical therapy [2] and in other less frequent inherited arrhythmogenic syndromes.
Considering that approximately 1–2 % of the adult population in developed countries suffer from heart failure (HF) and that at least half of these patients have a low ejection fraction [3], the number of ICD carriers is wide spreading. Moreover, the improving therapies of HF ensure a long survival of patients making them older and affected by more comorbidities. For these reasons, ES is an increasingly frequent cause of access to emergency department (ED). It is estimated that about 25 % of ICD carriers experience at least one ES episode per year follow-up [4]. ES is definitely a medical emergency requiring a multidisciplinary approach.
12.2 What Physicians Working in ED and Anesthesiologists Should Know
12.2.1 How Is an ICD Made and How Does It Work?
The ICD is a subcutaneous implantable device able to monitor cardiac rhythm and terminate potentially life-threatening arrhythmias. It consists of two main components:
-
The generator that contains the battery, all the circuits that run the device, and the operator communicating system. It is implanted in a subcutaneous pocket, usually under the left clavicle.
-
The leads that reach heart chambers through the venous system and allow the device to either monitor heart electrical activity and deliver therapies. The ICDs have a lead implanted in the right ventricle apex able both to record ventricular activity and release therapies like pacing and/or direct current shock. In adjunct some ICDs have another lead implanted in the right atrium to record atrial electrical activity, improving discrimination between supraventricular arrhythmias (SVA) and ventricular ones and to pace the atrium (ICD-DR). ICDs with cardiac resynchronization therapy (CRT-D) have a third lead that paces the left ventricle, through the coronary venous system, synchronously to the right ventricle improving contractility. Some recent devices are implanted entirely subcutaneously, leads included (subcutaneous ICD), and can deliver high-energy shocks only (without long-term pacing capabilities) without a direct contact with the heart chambers and no leads inserted in the venous system.
ICDs use mathematical algorithms defined by the manufacturer to discriminate life-threatening ventricular arrhythmias from SVA and deliver appropriate therapy. Sometimes correct recognition fails, and in this case the therapy delivered is defined inappropriate. In other cases the delivered therapy may not be able to terminate the ventricular arrhythmia, and in this case it is called ineffective:
-
The operator interfaces with the ICD through a programmer able to communicate with the device. Each manufacturer uses a different programmer, so it is imperative to know the manufacturer and use the right equipment. The programmer establishes an initial connection with the device through a head which must be positioned on the skin above the ICD. Usually green lights turn on to indicate the head is in the right place. At this point, depending on the features of the device, it may be necessary to maintain the head above the ICD throughout the query to allow communication, or, in some devices, the head can be removed since the communication continues via Wi-Fi.
The programmer allows the operator to visualize all the data stored in the device such as:
-
Arrhythmic events: the device registers all arrhythmic events recognized as such on the basis of user-defined criteria. Each event provides endocavitary (or external for subcutaneous ICDs) electrocardiogram lead recording and therapies delivered.
-
Battery status.
-
Information about lead integrity.
On the basis of stored data, the operator may decide to change some settings such as:
-
Arrhythmia recognition criteria (heart rate, time before treatment, algorithms for SVT recognition, etc.) and intervention criteria
-
Type and characteristics of therapies delivered
12.2.2 How Does the ICD Recognize and Treat Arrhythmias (Appropriate Therapies)?
VT recognition is primarily based upon tachycardia cycle length (to distinguish from normal sinus rhythm) and duration (to detect non-sustained episodes). Both of these parameters are tailored on the patient’s characteristics. Thus, ICD uses ventricular rate zones for rhythm classification. The boundaries between zones are defined by two main principles:
-
The recognition of unstable fast VT/VF must be highly sensitive even at the cost of inappropriate rapid SVA treatment.
-
The recognition of slower VT (generally better tolerated) has to be more specific to avoid inappropriate therapies even at the cost of some delay in detection.
The ICDs treat ventricular tachyarrhythmias by:
-
Antitachycardia pacing (ATP): it is a brief ventricular pacing (6–8 beats) with a cycle length slightly lower (thus at a faster rate) of the arrhythmia (usually 81–88 %), in the attempt of resetting the reentrant circuit and interrupting the arrhythmia. Sometimes the paced cycle shortens from beat to beat, and in this case it is referred as ATP ramp.
-
Direct current shock (DC shock): it is a biphasic electrical shock provided between the generator case and the coil localized on the right ventricular lead. The energy released may vary, reaching up to 40 J with the latest generation high-energy devices.
Basing on several studies [5–7], ICD programming should empirically involve the use of three rate zones:
-
A slow VT zone up to 320 ms cycle length (<188 bpm)
-
A fast VT zone from 320 to 240 ms (188–250 bpm)
-
A VF zone from 240 ms (>250 bpm)
In both VT zones, a variable number of ATP attempts precede shocks delivery. In the slow VT zone, a greater number than in fast VT zone are usually programmed (e.g., 3 ATPs followed by 3 ATP ramps), as fast arrhythmias are usually less tolerated.
In the VF zone, the hemodynamic instability of the arrhythmia and its high life-threatening potential require an immediate shock delivery (usually at the maximum energy from the beginning). In modern devices an ATP during capacitor charging (usually requiring less than 10 s) is delivered, avoiding the shock in the case of arrhythmic interruption.
VT/VF detection not only is based upon ventricular rate but also requires a programmable duration of the arrhythmia to avoid detection of non-sustained episodes. Usually a VT/VF is detected when a certain percentage of ventricular sensed beats meets cycle length criteria. The type of counting used varies between detection zones and among manufacturers. In order to improve sensibility, according to some manufacturers, the arrhythmia is detected when a certain percentage of beats (not necessarily consecutive) falls in VF zone, while consecutive interval counting is required in the VT zone, increasing specificity. The time to detection in the VT zone should be longer enough to allow spontaneous termination of non-sustained episodes [6, 8].
12.2.3 Inappropriate Therapies
Inappropriate therapies (especially shocks) are one of the main issues to be avoided as they cause patient discomfort, are potentially proarrhythmic, and reduce battery life.
The two main causes of inappropriate shock are failure in discriminating SVA and signal misinterpretation.
Frequently SVA is associated with a fast ventricular response leading ventricular rate to fall into VT/VF detection zone causing inappropriate therapy release. This problem occurs more frequently with single-chamber ICDs that do not have atrial sensing capabilities. Dual-chamber devices can compare atrial and ventricular rates to set the origin of the. ICDs use a variety of algorithms to discriminate SVA from VT; major ones are listed below:
-
Atrioventricular rate comparison: applies only in dual-chamber ICDs; when the ventricular rate is faster, the diagnosis is VT. When atrial and ventricular rates are equal, additional criteria are required for discrimination.
-
Onset: useful for discrimination of gradually accelerating sinus tachycardia from sudden-onset VT. It applies when the RR interval shortens by a programmed percentage if compared with the average number of preceding beats. May fail in case of VT occurring during sinus tachycardia.
-
Stability: useful for discrimination of fast response AF. It evaluates RR variability; when greater than a programmed percentage (e.g., 20 %), AF is supposed. It may fail in the case of very fast AF in which there is a pseudo-regularization of ventricular rate, in atrial flutter or in irregular VT.
-
Morphology: it compares endocavitary electrocardiograms recorded during sinus rhythm and during VT. It is useful in single-chamber ICDs lacking of atrial information but may fail in intraventricular conduction delays and in rate-dependent conduction delays.
-
Rate duration: it is an extreme lifesaving measure. It results in shock delivery after a programmable time interval even if the episode is classified as SVA; this algorithm is usually activated when there is a high risk of undertreatment of VT erroneously recognized as SVA, but it increases the risk of overtreatment.
Signal misinterpretation is the other big deal leading to inappropriate shocks. It may depend on some programmed variables; easily editable, external, and far-field interferences; or device/lead failure that usually requires an interventional approach. Main causes of signal misinterpretation are listed below:
-
T wave oversensing: it happens when a high amplitude T wave is erroneously recognized as an R wave. It may happen because of the low ventricular sensing threshold necessary to recognize even low-amplitude VF. This problem can be solved by increasing sensing threshold, lengthening refractory period, or changing sensing decay parameters to suppress T wave detection.
-
Electromagnetic external interference: external electromagnetic fields can be mistaken for intracardiac signals resulting in inappropriate arrhythmic detection and therapy. Common household appliances are not generally a problem, but some high-intensity fields such as high-voltage power lines, electric motors, magnetic resonance imaging, TENS units, electrocautery during surgery, neurostimulators, and radiotherapy should be avoided.
-
Myopotentials: far-field myopotential recording may lead to inappropriate arrhythmic detection. This problem occurred in the past with unipolar leads using large sensing fields (from the lead tip to the generator case) and is now largely avoided with the modern bipolar leads, recording more localized signals only.
-
Lead failure: lead fracture or insulation loss of continuity may cause external noise recording and inappropriate detection. In these cases lead extraction and/or new lead insertion is the only choice. Modern devices usually provide alerts for lead integrity.
12.2.4 Electrical Storm
12.2.4.1 Incidence and Clinical Predictors
Several studies examined the incidence of ES in ICD recipients, although ES definition was not standardized and the inclusion criteria and follow-up period were not homogeneous. Considering current definition, the incidence varies from 4 to 28 % in a follow-up period between 1 and 3 years [9]. In the sub-analysis of the AVID trial [10], including 499 patients treated for secondary prevention, the rate of ES was 20 % at 3-year follow-up. Of note, the incidence of ES in primary prevention trials appears lower (4 % in MADIT II), and in our experience [11], after a mean 2-year follow-up, only 13 patients (2 %) experienced an ICD treatment configuring an ES.
A recent meta-analysis [9] evaluated the real weight of ES as a risk factor and its clinical predictors. On the basis of 13 studies, a trend toward an increased prevalence of ES was associated with advanced age and male gender. Other factors related to ES in ICD carriers were heart failure-related clinical variables (as lower ejection fraction), an ICD implant for secondary prevention, the presence of monomorphic VT as triggering arrhythmias instead of polymorphic VTs and VF, and the treatment with class I antiarrhythmic drugs but not with amiodarone and beta-blockers. On the contrary, no significant differences between patients with ischemic or nonischemic dilated cardiomyopathy were reported. After meta-regression analysis, no significant interaction between any of the examined clinical variables and the increased risk of ES was confirmed.
The main clinical characteristics and clinical predictors of ES in the group of patients treated with a CRT-D have been considered in a multicenter experience including 631 patients, with a mean follow-up of 19 ± 11 months. In this study VT or VF episodes were detected and treated in 141 patients (22 %), and ES occurred in 45 (7 %). At univariate analysis, the only predictors of ES were the nonischemic etiology of cardiomyopathy and secondary prevention indication, while other common variables such as age, male gender, ejection fraction lower than 25 %, and advanced NYHA class did not correlate.
Our experience included 62 patients (mean age 66 years, 90 % male) admitted for ES during the period 2006–2012. The mean interval from implant to ES was 47 months. Ischemic heart disease was present in 30, nonischemic cardiomyopathy in 11, and other etiologies in 14, and 60 % of patients had been treated with ICD for secondary prevention. Mean ejection fraction was 35 %. In 23 patients the arrhythmia at admittance was incessant VT, while the remaining 39 experienced several VT/VF episodes, with a mean number of 6 shocks per patient. In more than half of patients (31), there wasn’t a clear trigger and the ES rises from a primitive electrical instability. In the remaining the most frequent triggers were worsening heart failure, electrolyte imbalances, myocardial ischemia, and proarrhythmic drug side effects.
12.2.4.2 Prognosis
The majority of papers evaluating the role of ES as a mortality risk factor showed that it was associated with a threefold risk of death. ES maintained a significant value as risk factor even when compared with unclustered sustained VT/VF [9]. For the composite end point of all cause mortality, heart transplantation and hospitalization for heart failure ES was associated with a 3.39-fold increased risk.
The reported mortality among large series [12] of patients with ES treated by catheter ablation appeared extremely variable between 15 and 29 % during a follow-up ranging from 1 to 2.5 years. In our series, including patients treated not exclusively by catheter ablation, the overall survival of patients experiencing their first ES episode was 60 %, 50 %, and 44 % after 1, 2, and 3 years, respectively.
Considering that ES is associated with increased SCD and non-sudden cardiac mortality, Guerra et al. evaluated the association between ES and heart failure in patients with chronic heart failure and ICD. They reported that during 5-year follow-up, the survival estimates were not significantly different between patients with ES and HF worsening (36.4 vs. 38.5 months), while it was significantly lower in comparison to survival of patients with unclustered VT/VF episodes (49.2 months). The primary mortality cause in ES group was refractory heart failure (59 %), followed by noncardiac conditions and by SCD in only two patients. Even hospitalization-free rate was lower in both ES and HF worsening groups in comparison to patients with unclustered VT/VF episodes (15.4 vs. 20.1 vs. 36.1 months), while the hospitalization rates were not significantly different between ES and HF worsening groups. The conclusions of the authors were that heart failure patients admitted for ES show important outcome analogies with patients admitted for acute heart failure and that ES should be identified as an important clinical consequence of heart failure decompensation.
12.3 What the Cardiologist Should Know
ES is a medical emergency potentially leading to acute cardiac failure and cardiogenic shock and requiring a multidisciplinary approach.
Initial diagnostic workup includes physical examination, electrocardiogram (ECG), chest X-ray, echocardiogram, blood gas analysis, electrolytes, serum creatinine evaluation, and ICD interrogation.
The first issue to assess in a patient with multiple ICD shocks is to seek ICD intervention causes.
In case of appropriate therapies due to VT/VF, it is necessary first of all to rule out reversible causes of ES including electrolyte imbalances, acute ischemia, worsening heart failure, infective state, hyperthyroidism, and proarrhythmic drugs. In a large series reversible causes of ES account for no more than 10 % of cases referred to EP labs [4].
Following initial evaluation, an accurate patient’s risk stratification should be made according to hemodynamic tolerance of the clinical VT and comorbidities [13]. Hemodynamic decompensation defined as sustained hypotension (i.e., systolic blood pressure <80–90 mmHg) despite increasing doses of vasopressors and requiring mechanical hemodynamic support (i.e., intra-aortic balloon pump, left ventricular assist devices, or extracorporeal membrane oxygenation) [14] makes the patient at high risk by itself and in some cases even at the temporary restoration of sinus rhythm. In case of hemodynamically tolerated VT, the presence of at least one comorbidity such as left ventricular ejection fraction less than 30 %, serum creatinine level >1.5 mg/dl, chronic occlusion of left anterior descending coronary artery, and severe chronic lung disease makes the patient particularly high risk [13]. All high-risk patients should be admitted to intensive care unit (ICU) and, if necessary, undergo circulatory and/or ventilatory support and/or hemodialysis.
All the efforts should be made to reduce VT/VF episodes to avoid further shocks considering even in combination of a complex strategic approach including antiarrhythmic drug therapy, device reprogramming, deep sedation/mechanical assistance, and catheter ablation.
12.3.1 Antiarrhythmic Drugs
Initial treatment of ES usually involves the use of antiarrhythmic drugs, weighing their proarrhythmic risk and negative inotropic effect, to prevent arrhythmic recurrences.
The cornerstone of antiarrhythmic therapy still remains sympathetic blockade with beta-blockers to suppress the adrenergic drive to VT recurrence [15]. Although all beta-blockers are able to reduce susceptibility to VT/VF as class action, most of the studies analyzed propranolol. In patients with HF, propranolol resulted to be more effective than metoprolol in reducing sympathetic tone due to its capability of blocking both β1 and β2 receptors and to its lipophilic nature that enables penetration within the central nervous system blocking also presynaptic adrenergic receptors [16, 17]. Sympathetic blockade is able not only to suppress ES [18] but also to improve short-term survival more than the combined antiarrhythmic therapy with lidocaine, procainamide, and bretylium [15]. In severely compromised patients, intravenous short-acting drugs like esmolol should be preferred [19]. The first-choice antiarrhythmic drug should be amiodarone, even in combination with propranolol that effectively controlled ES and improved survival [15, 18]. When amiodarone is administered intravenously, it reduces adrenergic tone, blocks sodium and L-calcium channels without prolonging ventricular refractoriness, and, when administered, orally prolongs ventricular refractory period [20, 21]. When ineffective alone or in combination with beta-blockers, amiodarone may be helpful even in adjunct to other agents [22]. Even patients who previously keep amiodarone may beneficiate from a reloading dose/therapy adjustment if serum levels of amiodarone/desethil-amiodarone are under therapeutic levels. The acute administration is relatively safe even in patients with depressed ejection fraction due to its low inotropic negative effect. It can increase the defibrillation threshold, making potentially ineffective ICD therapy; consequently ICD defibrillation energy should be re-tested or re-evaluated. Long-term amiodarone assumption is burdened by several side effects like thyroid, liver, and lung toxicity, sometimes forcing to therapy discontinuation. In case of amiodarone failure, other additionally drugs may be considered such as procainamide both orally or intravenously. The use of multiple antiarrhythmic drugs makes the drug-to-drug interaction unpredictable, potentially increasing the side effect occurrence. The use of lidocaine is limited by its relatively incapacity to terminate scar-related VT [23]. Lidocaine is a sodium rapid channel blocker that binds to channels in a use-dependent way. During ischemic VT, the altered membrane potential as the pH reduction [24] increases the rate of drug binding, making lidocaine effective in terminating arrhythmias. The pharmacodynamic proprieties make lidocaine not so effective in settings different from ischemic arrhythmias, maintaining a role only for the treatment of polymorphic VT associated with ischemia (IIb recommendation according to the American College of Cardiology/American Heart Association guidelines [25]).
Procainamide (not available in all countries) is another IC class antiarrhythmic drug commonly used as second- or third- line therapy in refractory VTs. Procainamide acts as fast sodium channel blocker, while its active metabolite N-acetylprocainamide blocks potassium channels and accounts for much of the antiarrhythmic effect in vivo as well as side effects like QT interval prolongation. Care must be taken in administering the drug in patients with low ejection fraction due to the high risk of hypotension.
12.3.2 Device Reprogramming
Several studies demonstrated that repeated ICD shocks are associated with increased mortality as well as with a reduction of quality of life [10]. For these reasons optimization of ICD programming in order to avoid unnecessary shock is mandatory in patients experiencing ES. As stated above, arrhythmic detection and treatment by ICD is a step process including several variables such as heart rate threshold, number of intervals to detect, discrimination of SVA, and type and number of therapies released. Each of these steps can be tailored upon patient characteristics to avoid unnecessary treatment.
12.3.2.1 Higher Heart Rate Threshold
Usually patients treated with ICD for primary prevention tend to develop fast VT, while patients treated for secondary prevention usually have slower VT with a wider overlap with SVA [26]. On this basis, the first may benefit from higher rate detection zones, while the latter needs slower rate detection zones and improved SVA discriminating algorithms. Even better, rate detection zones can be tailored upon patient’s clinical history when previous arrhythmia episodes occurred. In three trials (PREPARE, MADIT-RIT, and PROVIDE), higher rate detection zones demonstrated reduce ICD shocks without increasing both syncope and death risk.
12.3.2.2 Longer Detection Period
The effect of prolonging arrhythmic detection time is well studied especially in the primary prevention setting with lower data available in the setting of secondary prevention.
The REVELANT study showed that a higher number of intervals for arrhythmic detection (30/40 vs. 12/16) significantly reduced the incidence of ICD intervention without increasing syncope or death in patients with ICD for primary prevention and nonischemic cardiomyopathy. MADIT-RIT trial showed a reduction of both inappropriate therapy and all-cause mortality with a 60-s delay at 170–199 bpm, a 12-s delay at 200–249 bpm, and a 2.5-s delay at ≥250 bpm vs. conventional programming. These results were recently confirmed by ADVANCE III trial [27] in which the combination of a higher number of intervals to detection (30/40 vs. 18/24) with ATP therapy during charge significantly reduced either appropriate or inappropriate therapies regardless of ICD type and indication. Even in the PROVIDE trial, multi-parametric programming including higher detection rate, longer detection intervals, and optimized SVA discriminating algorithms was associated with better overall survival and reduction of ICD shocks without increasing arrhythmic syncope risk, and the PainFree SST trial confirmed that longer detection intervals are safe in terms of risk of syncope. Of all these studies, only ADVANCE III and the PainFree SST included patients with both primary and secondary preventions for ICD, while the remaining trials focused only on patients treated for primary prevention.
12.3.2.3 Improving ATP Programming
ATP therapy demonstrated to be highly effective in terminating VTs, reducing unnecessary shocks and consequently improving survival, quality of life, and generator life. In several studies 85–90 % of “slow” VTs (<188–200 bpm) [28] and 54–72 % of “fast” VTs (188–250 bpm) [29, 27] were terminated by ATP. As stated before, ATP therapy can be administered as bursts or ramps on the basis of the pacing cycle length variations. Bursts and ramps proved similar efficacy in treating slower VTs [28], while fast VTs (>200 bpm) were best treated by bursts that also showed a lower risk of arrhythmic acceleration than ramps. Due to less efficacy of ATP in terminating fast VTs (>200 bpm) and the negative hemodynamic consequences of such arrhythmias, usually in the fast VT and VF zone, ATP is delivered during capacitor charge to avoid any delay in shock therapy. The majority of VTs were effectively interrupted by one or two ATP attempts with only a minority of patients responsive to more than three attempts [30, 31], and for this reason programming more than three ATP attempts should be discouraged. In CRT-D recipients, biventricular ATP should be preferred to right ventricular ATP due to its higher efficacy and safety [32, 33]. The last key point in ATP programming is burst cycle length that can be empirically programmed at 85–90 % of the arrhythmic cycle length for fast VTs and at 70–80 % for slower ones. When ATP appears ineffective in VT termination, the analysis of the post pacing interval can allow tailoring ATP programming upon patient characteristics, for example, by shortening drive cycle length or by increasing the number of paced beats [34].
Accordingly to all these data, the increase of detection time and threshold rate in patients experiencing ES helps to prevent both inappropriate and unnecessary shocks, making ICD reprogramming a mandatory step in the clinical workup of ES.
In case of inappropriate therapies, specific measures must be taken: e.g., change ICD detection parameters, enhance drug therapy, or consider catheter ablation in case of SVA; temporarily turn off the device before lead replacement in case of lead fracture/failure.
12.3.3 Sedation, General Anesthesia/Mechanical Ventilation, and Mechanical Hemodynamic Support
The sympathetic adrenergic activation in patients experiencing multiple shocks due to ES may perpetuate VT/VF [35] and render the arrhythmias life threatening and refractory to several maneuvers. Therefore, some patients with ES should be sedated or even undergo general anesthesia to reduce sympathetic tone and suppress ventricular electrical instability. Propofol has been reported to suppress ES [36, 37], but this beneficial effect may be offset by the inotropic negative effect. In this regard, only few data are available in literature about the effect of deep sedation/general anesthesia on the prognosis of ES patients, and most of them are extrapolated from patients undergoing catheter ablation to treat ES. Drugs inducing general anesthesia should be considered with attention because they can exacerbate hypotension and depress cardiac function [14]. Deep sedation with remifentanil even in association with a benzodiazepine like midazolam should be preferred as it is able to reduce sympathetic hypertone and provide analgesia avoiding dangerous negative inotropic effects [38–40]. A valuable alternative may be dexmedetomidine [41], an α2 presynaptic adrenergic receptor agonist able to markedly reduce sympathetic tone by both enhancing central vagal tone [42] and inhibiting presynaptical adrenaline release [43]. However, it has important side effects like hypotension and bradycardia [44] that should be rigorously monitored during its usage.
General anesthesia and mechanical ventilation should be reserved only to patients with hemodynamically non-tolerated arrhythmias refractory to all therapies. Such patients may benefit from hemodynamic mechanical support like intra-aortic-balloon pump (IABP), left ventricular assistance devices such as the Impella (Abiomed Inc., Danvers, MA) [45–47], and even extracorporeal membrane oxygenation (ECMO) [48, 49]. These devices can not only suppress ischemic VTs by increasing coronary perfusion but can be effective in suppressing ES reducing LV afterload and wall tension [50] as well as prevent multiple organ failure sustaining organ perfusion. Last but not least, they have a key role in mapping and ablating unstable VTs. Some patients experiencing refractory unstable arrhythmias should also be carefully evaluated for urgent check for cardiac transplantation.
12.3.4 Neuraxial Modulation (Thoracic Epidural Anesthesia, Cardiac Sympathetic Denervation)
Given the importance of the autonomic nervous system in triggering and maintaining ventricular arrhythmias, sympathetic neuromodulation through thoracic epidural anesthesia [51], cardiac sympathetic denervation (CSD), and spinal cord stimulation may help in reducing arrhythmic burden in selected patient with ES refractory to multiple antiarrhythmic drugs and catheter ablation. CSD is usually performed via video-assisted thoracic surgery and consists of removal the lower third of the stellate ganglia (to avoid Claude-Bernard-Horner syndrome) as well as T2–T4 thoracic ganglia. The resection is usually performed on the left side, reserving bilateral CSD for selected cases. The procedure should be performed in referral centers only, due to special anesthesiology skills required such as selective bronchus intubation management. Most of what we know about the results of the procedure results from case reports [52, 51, 53], but in a prospective study of 41 patients with ES refractory to medical therapy and catheter ablation, CDS demonstrated to be effective in prolonging ICD shock-free survival at 1-year follow-up with greater effect of bilateral CDS compared to left CDS only [54].
12.3.5 Catheter Ablation
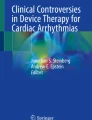
Currently, radiofrequency catheter (RF) ablation represents the mainstay treatment of recurrent VTs and even of ES. Several studies demonstrated how catheter ablation may prevent VT recurrence as well as improve survival of ES patients with a growing effectiveness due to technological improvement and deeper knowledge of arrhythmogenic substrate [14]. In the past, RF ablation was considered as the last chance treatment in patients refractory to multiple antiarrhythmic drugs, but in the last decade there has been a growing evidence for early referral to RF ablation in case of recurrent ICD therapies or even prophylactically [55–57]. RF ablation showed to be highly effective in suppressing refractory VTs in the acute management of ES, reaching an acute success rate of 80 % in the largest series [40, 12, 58, 59], especially when the end point of non-inducibility of all clinical VTs was reached [12]. As stated before, patients with unstable hemodynamic VTs should be referred for mechanical assistance in order to allow mapping and ablation but also those with apparently stable arrhythmia may develop acute hemodynamic decompensation during RF ablation procedure. In a preliminary study, a simple score named PAINESD taking in account patient’s baseline comorbidities (Pulmonary chronic obstructive disease, Age older than 60, Ischemic cardiomyopathy, NYHA class III or IV, Ejection fraction lower than 25 %, Storm at presentation, and Diabetes mellitus) was tested to predict acute decompensation during VT catheter ablation in order to select patients who may benefit prophylactic mechanical support [14] (Fig. 12.1).

A suggested algorithm/pathway for diagnosis and treatment of ES
12.4 Indication for Follow-Up and Referral
All patients who experienced an ES episode remain at high risk of recurrences even if effectively treated with catheter ablation and multiple antiarrhythmic drug prophylaxis. Often ES is the expression of worsening of the underling heart disease. For these reasons all patients who developed at least one episode of ES should be referred both to a heart failure specialist and proper electrophysiological management in order to optimize the heart failure therapy and evaluate indication to heart transplantation or left ventricular assistance devices both as a bridge to transplant and as destination therapy. Arrhythmic follow-up may be best done with home monitoring of the ICD that allows a prompt evaluation of arrhythmic events.
References
Pedersen CT, Kay GN, Kalman J, Borggrefe M, Della-Bella P, Dickfeld T, Dorian P, Huikuri H, Kim Y-H, Knight B, Marchlinski F, Ross D, Sacher F, Sapp J, Shivkumar K, Soejima K, Tada H, Alexander ME, Triedman JK, Yamada T, Kirchhof P, Lip GYH, Kuck KH, Mont L, Haines D, Indik J, Dimarco J, Exner D, Iesaka Y, Savelieva I, EP-Europace, UK. EHRA/HRS/APHRS expert consensus on ventricular arrhythmias. Heart Rhythm. 2014;11:e166–96.
McMurray JJV, Adamopoulos S, Anker SD, Auricchio A, Böhm M, Dickstein K, Falk V, Filippatos G, Fonseca C, Gomez-Sanchez MA, Jaarsma T, Køber L, Lip GYH, Maggioni AP, Parkhomenko A, Pieske BM, Popescu BA, Rønnevik PK, Rutten FH, Schwitter J, Seferovic P, Stepinska J, Trindade PT, Voors AA, Zannad F, Zeiher A, ESC Committee for Practice Guidelines. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2012;33:1787–847.
Mosterd A, Hoes AW. Clinical epidemiology of heart failure. Heart. 2007;93:1137–46.
Hohnloser SH, Al-Khalidi HR, Pratt CM, Brum JM, Tatla DS, Tchou P, Dorian P, SHock Inhibition Evaluation with AzimiLiDe (SHIELD) Investigators. Electrical storm in patients with an implantable defibrillator: incidence, features, and preventive therapy: insights from a randomized trial. Eur Heart J. 2006;27:3027–32.
Wathen MS. Prospective randomized multicenter trial of empirical antitachycardia pacing versus shocks for spontaneous rapid ventricular tachycardia in patients with implantable cardioverter-defibrillators: Pacing Fast Ventricular Tachycardia Reduces Shock Therapies (PainFREE Rx II) trial results. Circulation. 2004;110:2591–6.
Wilkoff BL, Williamson BD, Stern RS, Moore SL, Lu F, Lee SW, Birgersdotter-Green UM, Wathen MS, Van Gelder IC, Heubner BM, Brown ML, Holloman KK. Strategic programming of detection and therapy parameters in implantable cardioverter-defibrillators reduces shocks in primary prevention patients. J Am Coll Cardiol. 2008;52:541–50.
Wilkoff BL, Ousdigian KT, Sterns LD, Wang ZJ, Wilson RD, Morgan JM. A comparison of empiric to physician-tailored programming of implantable cardioverter-defibrillators. J Am Coll Cardiol. 2006;48:330–9.
Gunderson BD, Abeyratne AI, Olson WH, Swerdlow CD. Effect of programmed number of intervals to detect ventricular fibrillation on implantable cardioverter-defibrillator aborted and unnecessary shocks. Pacing Clin Electrophysiol. 2007;30:157–65.
Guerra F, Shkoza M, Scappini L, Flori M, Capucci A. Role of electrical storm as a mortality and morbidity risk factor and its clinical predictors: a meta-analysis. Europace. 2014;16:347–53.
Tan VH, Wilton SB, Kuriachan V, Sumner GL, Exner DV. Impact of programming strategies aimed at reducing nonessential implantable cardioverter defibrillator therapies on mortality: a systematic review and meta-analysis. Circ Arrhythm Electrophysiol. 2014;7:164–70.
Proclemer A, Muser D, Campana A, Zoni-Berisso M, Zecchin M, Locatelli A, Brieda M, Gramegna L, Santarone M, Chiodi L, Mazzone P, Rebellato L, Facchin D. Indication to cardioverter-defibrillator therapy and outcome in real world primary prevention. Data from the IRIDE [Italian registry of prophylactic implantation of defibrillators] study. Int J Cardiol. 2013;168:1416–21.
Carbucicchio C, Santamaria M, Trevisi N, Maccabelli G, Giraldi F, Fassini G, Riva S, Moltrasio M, Cireddu M, Veglia F, Della Bella P. Catheter ablation for the treatment of electrical storm in patients with implantable cardioverter-defibrillators: short- and long-term outcomes in a prospective single-center study. Circulation. 2008;117:462–9.
Bella PD, Baratto F, Tsiachris D, Trevisi N, Vergara P, Bisceglia C, Petracca F, Carbucicchio C, Benussi S, Maisano F, Alfieri O, Pappalardo F, Zangrillo A, Maccabelli G. Management of ventricular tachycardia in the setting of a dedicated unit for the treatment of complex ventricular arrhythmias: long-term outcome after ablation. Circulation. 2013;127:1359–68.
Santangeli P, Muser D, Zado ES, Magnani S, Khetpal S, Hutchinson MD, Supple G, Frankel DS, Garcia FC, Bala R, Riley MP, Lin D, Rame JE, Schaller R, Dixit S, Marchlinski FE, Callans DJ. Acute hemodynamic decompensation during catheter ablation of scar-related VT: incidence, predictors and impact on mortality. Circ Arrhythm Electrophysiol. 2015;8:68–75.
Nademanee K, Taylor R, Bailey WE, Rieders DE, Kosar EM. Treating electrical storm: sympathetic blockade versus advanced cardiac life support-guided therapy. Circulation. 2000;102:742–7.
Bristow MR, Ginsburg R, Umans V, Fowler M, Minobe W, Rasmussen R, Zera P, Menlove R, Shah P, Jamieson S. Beta 1-and beta 2-adrenergic-receptor subpopulations in nonfailing and failing human ventricular myocardium: coupling of both receptor subtypes to muscle contraction and selective beta 1-receptor down-regulation in heart failure. Circ Res. 1986;59:297–309.
Billman GE, Castillo LC, Hensley J, Hohl CM, Altschuld RA. Beta2-adrenergic receptor antagonists protect against ventricular fibrillation: in vivo and in vitro evidence for enhanced sensitivity to beta2-adrenergic stimulation in animals susceptible to sudden death. Circulation. 1997;96:1914–22.
Tsagalou EP, Kanakakis J, Rokas S, Anastasiou-Nana MI. Suppression by propranolol and amiodarone of an electrical storm refractory to metoprolol and amiodarone. Int J Cardiol. 2005;99:341–2.
Brodine WN, Tung RT, Lee JK, Hockstad ES, Moss AJ, Zareba W, Hall WJ, Andrews M, McNitt S, Daubert JP. Effects of beta-blockers on implantable cardioverter defibrillator therapy and survival in the patients with ischemic cardiomyopathy (from the Multicenter Automatic Defibrillator Implantation Trial-II). Am J Cardiol. 2005;96:691–5.
Kodama I, Kamiya K, Honjo H, Toyama J. Acute and chronic effects of amiodarone on mammalian ventricular cells. Jpn Heart J. 1996;37:719–30.
Du XJ, Esler MD, Dart AM. Sympatholytic action of intravenous amiodarone in the rat heart. Circulation. 1995;91:462–70.
Vassallo P, Trohman RG. Prescribing amiodarone: an evidence-based review of clinical indications. JAMA. 2007;298:1312–22.
Guidelines 2000 for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Part 6: advanced cardiovascular life support: section 5: pharmacology I: agents for arrhythmias. The American Heart Association in collaboration with the International Liaison Committee on Resuscitation. Circulation. 2000;102:I112–28.
Nasir N, Taylor A, Doyle TK, Pacifico A. Evaluation of intravenous lidocaine for the termination of sustained monomorphic ventricular tachycardia in patients with coronary artery disease with or without healed myocardial infarction. Am J Cardiol. 1994;74:1183–6.
American College of Cardiology, American Heart Association Task Force, European Society of Cardiology Committee for Practice Guidelines, European Heart Rhythm Association, Heart Rhythm Society, Zipes DP, Camm AJ, Borggrefe M, Buxton AE, Chaitman B, Fromer M, Gregoratos G, Klein G, Moss AJ, Myerburg RJ, Priori SG, Quinones MA, Roden DM, Silka MJ, Tracy C, Smith SC, Jacobs AK, Adams CD, Antman EM, Anderson JL, Hunt SA, Halperin JL, Nishimura R, Ornato JP, Page RL, Riegel B, Priori SG, Blanc J-J, Budaj A, Camm AJ, Dean V, Deckers JW, Despres C, Dickstein K, Lekakis J, McGregor K, Metra M, Morais J, Osterspey A, Tamargo JL, Zamorano JL. ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: a report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (writing committee to develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death). J Am Coll Cardiol. 2006;48:e247–346.
Wilkoff BL, Hess M, Young J, Abraham WT. Differences in tachyarrhythmia detection and implantable cardioverter defibrillator therapy by primary or secondary prevention indication in cardiac resynchronization therapy patients. J Cardiovasc Electrophysiol. 2004;15:1002–9.
Gasparini M, Proclemer A, Klersy C, Kloppe A, Lunati M, Ferrer JBM, Hersi A, Gulaj M, Wijfels MCEF, Santi E, Manotta L, Arenal A. Effect of long-detection interval vs standard-detection interval for implantable cardioverter-defibrillators on antitachycardia pacing and shock delivery: the ADVANCE III randomized clinical trial. JAMA. 2013;309:1903–11.
Sweeney MO. Antitachycardia pacing for ventricular tachycardia using implantable cardioverter defibrillators. Pacing Clin Electrophysiol. 2004;27:1292–305.
Wathen MS, DeGroot PJ, Sweeney MO, Stark AJ, Otterness MF, Adkisson WO, Canby RC, Khalighi K, Machado C, Rubenstein DS, Volosin KJ, PainFREE Rx II Investigators. Prospective randomized multicenter trial of empirical antitachycardia pacing versus shocks for spontaneous rapid ventricular tachycardia in patients with implantable cardioverter-defibrillators: Pacing Fast Ventricular Tachycardia Reduces Shock Therapies (PainFREE Rx II) trial results. Circulation. 2004;110:2591–6.
Martins RP, Blangy H, Muresan L, Freysz L, Groben L, Zinzius P-Y, Schwartz J, Sellal J-M, Aliot E, Sadoul N. Safety and efficacy of programming a high number of antitachycardia pacing attempts for fast ventricular tachycardia: a prospective study. Europace. 2012;14:1457–64.
Anguera I, Dallaglio P, Sabaté X, Nuñez E, Gracida M, Di Marco A, Sugrañes G, Cequier A. The benefit of a second burst antitachycardia sequence for fast ventricular tachycardia in patients with implantable cardioverter defibrillators. Pacing Clin Electrophysiol. 2014;37:486–94.
Haghjoo M, Hajahmadi M, Fazelifar AF, Sadr-Ameli MA. Efficacy and safety of different antitachycardia pacing sites in the termination of ventricular tachycardia in patients with biventricular implantable cardioverter-defibrillator. Europace. 2011;13:509–13.
Gasparini M, Anselme F, Clementy J, Santini M, Martínez-Ferrer J, De Santo T, Santi E, Schwab JO, ADVANCE CRT-D Investigators. BIVentricular versus right ventricular antitachycardia pacing to terminate ventricular tachyarrhythmias in patients receiving cardiac resynchronization therapy: the ADVANCE CRT-D Trial. Am Heart J. 2010;159:1116–1123.e2.
Madhavan M, Friedman PA. Optimal programming of implantable cardiac-defibrillators. Circulation. 2013;128:659–72.
Zipes DP, Barber MJ, Takahashi N, Gilmour RF. Influence of the autonomic nervous system on the genesis of cardiac arrhythmias. Pacing Clin Electrophysiol. 1983;6:1210–20.
Mulpuru SK, Patel DV, Wilbur SL, Vasavada BC, Furqan T. Electrical storm and termination with propofol therapy: a case report. Int J Cardiol. 2008;128:e6–8.
Burjorjee JE, Milne B. Propofol for electrical storm; a case report of cardioversion and suppression of ventricular tachycardia by propofol. Can J Anaesth. 2002;49:973–7.
Ogletree ML, Sprung J, Moravec CS. Effects of remifentanil on the contractility of failing human heart muscle. J Cardiothorac Vasc Anesth. 2005;19:763–7.
Mandel JE, Hutchinson MD, Marchlinski FE. Remifentanil-midazolam sedation provides hemodynamic stability and comfort during epicardial ablation of ventricular tachycardia. J Cardiovasc Electrophysiol. 2011;22:464–6.
Brugada J, Berruezo A, Cuesta A, Osca J, Chueca E, Fosch X, Wayar L, Mont L. Nonsurgical transthoracic epicardial radiofrequency ablation: an alternative in incessant ventricular tachycardia. J Am Coll Cardiol. 2003;41:2036–43.
Tarvainen MP, Georgiadis S, Laitio T, Lipponen JA, Karjalainen PA, Kaskinoro K, Scheinin H. Heart rate variability dynamics during low-dose propofol and dexmedetomidine anesthesia. Ann Biomed Eng. 2012;40:1802–13.
Kamibayashi T, Hayashi Y, Mammoto T, Yamatodani A, Sumikawa K, Yoshiya I. Role of the vagus nerve in the antidysrhythmic effect of dexmedetomidine on halothane/epinephrine dysrhythmias in dogs. Anesthesiology. 1995;83:992–9.
Hayashi Y, Sumikawa K, Maze M, Yamatodani A, Kamibayashi T, Kuro M, Yoshiya I. Dexmedetomidine prevents epinephrine-induced arrhythmias through stimulation of central alpha 2 adrenoceptors in halothane-anesthetized dogs. Anesthesiology. 1991;75:113–7.
Gerlach AT, Murphy CV. Dexmedetomidine-associated bradycardia progressing to pulseless electrical activity: case report and review of the literature. Pharmacotherapy. 2009;29:1492.
Miller MA, Dukkipati SR, Mittnacht AJ, Chinitz JS, Belliveau L, Koruth JS, Gomes JA, d’ Avila A, Reddy VY. Activation and entrainment mapping of hemodynamically unstable ventricular tachycardia using a percutaneous left ventricular assist device. J Am Coll Cardiol. 2011;58:1363–71.
Abuissa H, Roshan J, Lim B, Asirvatham SJ. Use of the Impella microaxial blood pump for ablation of hemodynamically unstable ventricular tachycardia. J Cardiovasc Electrophysiol. 2010;21:458–61.
Miller MA, Dukkipati SR, Chinitz JS, Koruth JS, Mittnacht AJ, Napolitano C, d’ Avila A, Reddy VY. Percutaneous hemodynamic support with Impella 2.5 during scar-related ventricular tachycardia ablation (PERMIT 1). Circ Arrhythm Electrophysiol. 2013;6:151–9.
Ücer E, Fredersdorf S, Jungbauer C, Debl K, Philipp A, Amann M, Holzamer A, Keyser A, Hilker M, Luchner A, Schmid C, Riegger G, Endemann D. A unique access for the ablation catheter to treat electrical storm in a patient with extracorporeal life support. Europace. 2014;16:299–302.
Lü F, Eckman PM, Liao KK, Apostolidou I, John R, Chen T, Das GS, Francis GS, Lei H, Trohman RG, Benditt DG. Catheter ablation of hemodynamically unstable ventricular tachycardia with mechanical circulatory support. Int J Cardiol. 2013;168:3859–65.
Franz MR, Burkhoff D, Yue DT, Sagawa K. Mechanically induced action potential changes and arrhythmia in isolated and in situ canine hearts. Cardiovasc Res. 1989;23:213–23.
Bourke T, Vaseghi M, Michowitz Y, Sankhla V, Shah M, Swapna N, Boyle NG, Mahajan A, Narasimhan C, Lokhandwala Y, Shivkumar K. Neuraxial modulation for refractory ventricular arrhythmias: value of thoracic epidural anesthesia and surgical left cardiac sympathetic denervation. Circulation. 2010;121:2255–62.
Ajijola OA, Lellouche N, Bourke T, Tung R, Ahn S, Mahajan A, Shivkumar K. Bilateral cardiac sympathetic denervation for the management of electrical storm. J Am Coll Cardiol. 2012;59:91–2.
Estes EH, Izlar HL. Recurrent ventricular tachycardia. A case successfully treated by bilateral cardiac sympathectomy. Am J Med. 1961;31:493–7.
Vaseghi M, Gima J, Kanaan C, Ajijola OA, Marmureanu A, Mahajan A, Shivkumar K. Cardiac sympathetic denervation in patients with refractory ventricular arrhythmias or electrical storm: intermediate and long-term follow-up. Heart Rhythm. 2014;11:360–6.
Stevenson WG, Wilber DJ, Natale A, Jackman WM, Marchlinski FE, Talbert T, Gonzalez MD, Worley SJ, Daoud EG, Hwang C, Schuger C, Bump TE, Jazayeri M, Tomassoni GF, Kopelman HA, Soejima K, Nakagawa H, Multicenter Thermocool VT Ablation Trial Investigators. Irrigated radiofrequency catheter ablation guided by electroanatomic mapping for recurrent ventricular tachycardia after myocardial infarction: the multicenter thermocool ventricular tachycardia ablation trial. Circulation. 2008;118:2773–82.
Reddy VY, Reynolds MR, Neuzil P, Richardson AW, Taborsky M, Jongnarangsin K, Kralovec S, Sediva L, Ruskin JN, Josephson ME. Prophylactic catheter ablation for the prevention of defibrillator therapy. N Engl J Med. 2007;357:2657–65.
Kuck K-H, Schaumann A, Eckardt L, Willems S, Ventura R, Delacrétaz E, Pitschner H-F, Kautzner J, Schumacher B, Hansen PS, VTACH study group. Catheter ablation of stable ventricular tachycardia before defibrillator implantation in patients with coronary heart disease (VTACH): a multicentre randomised controlled trial. Lancet. 2010;375:31–40.
Silva RMFL, Mont L, Nava S, Rojel U, Matas M, Brugada J. Radiofrequency catheter ablation for arrhythmic storm in patients with an implantable cardioverter defibrillator. Pacing Clin Electrophysiol. 2004;27:971–5.
Strickberger SA, Man KC, Daoud EG, Goyal R, Brinkman K, Hasse C, Bogun F, Knight BP, Weiss R, Bahu M, Morady F. A prospective evaluation of catheter ablation of ventricular tachycardia as adjuvant therapy in patients with coronary artery disease and an implantable cardioverter-defibrillator. Circulation. 1997;96:1525–31.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Muser, D., Facchin, D., Rebellato, L., Proclemer, A. (2016). Management of the Electrical Storm in Patients with ICD. In: Zecchin, M., Sinagra, G. (eds) The Arrhythmic Patient in the Emergency Department. Springer, Cham. https://doi.org/10.1007/978-3-319-24328-3_12
Download citation
DOI: https://doi.org/10.1007/978-3-319-24328-3_12
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-24326-9
Online ISBN: 978-3-319-24328-3
eBook Packages: MedicineMedicine (R0)