
Abstract
Drug combination studies are generally conducted to look for synergistic effects. In this chapter, we discuss typical study design and analysis methods for drug combination studies, with a focus on in vitro experiments. Two reference models Loewe additivity and Bliss independence are used for synergy evaluation. A new index based on Bliss independence is introduced, comparable to the interaction index based on Loewe Additivity. An example data set is used to demonstrate the implementation of these analysis methods. In the final discussion, we point out some future research areas.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
Drug combination studies are conducted in many fields. In the pharmaceutical industry, as drug research and development costs have been skyrocketing and the attrition rate has been climbing up, companies are looking to combine several compounds as a new treatment for diseases. This is especially the case in oncology and infectious disease therapeutic areas. In agriculture, scientists may seek to combine several synergistic chemicals for a more effective pesticide. In environmental sciences, environmentalists may also study whether a toxicity synergy can result from combination of chemical pollutants discharged together. Scientists are looking for therapeutic synergy in the first two scenarios and toxic synergy in the third scenario.
This chapter will focus on drug combination studies in the pharmaceutical industry. Just as mutual funds provide more investment options by combining different individual stocks, combination therapies offer scientists a discovery tool that can lead to many more treatment options. However, drug combination also poses challenges to the drug discovery and development process. For example, in addition to studying each of the combined compounds, one needs to test a factorial combination of many doses of both compounds. The first question is how to design such experiments. Another challenge is how to evaluate the combined effect. As can be seen shortly, defining synergy is based on a reference model, which has several options but no one has been convincingly established as the best. Then the same study result can lead to different conclusions using different reference models.
Drug combination studies are conducted in different phases of drug discovery and development. Early in drug discovery, after a disease target is identified, scientists screen compounds that may have a target related. There are two ways of screening. One is unguided screening, in which some compounds sampled from a library are combined and studied. In this case, scientists only have a limited understanding about the mechanism of action of these compounds to narrow down candidate compounds in the library. The other is guided screening, where the mechanism of action of a candidate is well characterized and shows some effect on the target. Then based on their knowledge of biology or disease, scientists hypothesize compounds whose mechanism of action is understood and projected to be synergistic with the compound of interest. Then combination studies of these compound pairs are designed and conducted. At this stage, drug combination studies are typically in vitro, so multiple doses, usually no less than 4, of each compound can be used in the combinations, resulting in a factorial matrix of 4 × 4 or even higher dimension. In this case, a dose response curve of each monotherapy can be well modeled and synergy can be evaluated based on either Loewe additivity (Loewe 1928) or Bliss independence (Bliss 1939), which will be introduced in a later section.
If a compound pair is found to be synergistic in vitro, it moves to in vivo testing. In this stage, only two or at most three dose levels of each can usually be studied, limited by the number of animals appropriate for such studies. Studies typically use a simple factorial design. However, it is hard to evaluate synergy using methods as those for in vitro studies. One option is the min test (Hung 2000), which tests the hypothesis that the combination is superior to both single agents. This test is also used to show the efficacy of a drug combination in clinical trials. It may be helpful to note that a drug usually means a compound that has been approved by a regulatory agency for marketing. Before approval, it is called a compound or drug candidate. However, we use compound and drug interchangeably in this chapter.
In this chapter, we will discuss experimental designs for drug combination studies and different analysis methods for study data, with a focus on in vitro studies and a passing discussion of in vivo and clinical studies. We will propose an analysis method for combinations which we recommend as good practice to interpret study results.
Before we move to the next section, we will note a brief history of drug combination studies. In a broad sense, combination therapies can be dated back thousands of years ago when the Chinese started herbal medicines which typically included a combination of several herbs. However, herbal medicines were different from modern combination therapies because the dose response of each active herb in the combination was not characterized and the dose of each herb in the combination was based on empirical knowledge and often varied from one prescriber to another. Systematic evaluation of drug synergy started in the early twentieth century when Loewe defined a reference model Loewe additivity (Loewe 1928) and Bliss defined an independence reference model (Bliss 1939). Later a wealth of literature has been developed by pharmacologists, statisticians, chemists, and biologists. Excellent reviews include Berenbaum (1989) and Greco et al. (1995).
2 Study Design
Studies at different stages use different designs. For in vitro studies, several designs have been proposed. One is the fixed ratio (ray) design, in which one can select a dose D 1 of drug 1 and a dose D 2 of drug 2 (e.g., their EC50s), and a fraction c, to obtain a combination dose D = c D 1 + (1-c) D 2 . Then a series of concentrations or dilutions of this combination forms a ray as in Fig. 13.1. The combination fraction c can take different values, resulting in other rays. For a detailed discussion of this design, see Tallarida (2000) and Straetemans et al. (2005). For its optimal version, see Donev and Tobias (2011).

A ray or fixed ratio design for two drugs in combination studies
This design is typically used in industry for in-vitro studies. A third design (Tan et al. 2009) is an optimal one based on a uniform measure that meets some power requirement for testing departure from Loewe additivity.
For in vivo studies, the number of doses is limited to typically two per compound to avoid using an excessive number of animals. Therefore, usually a factorial design is used.
3 Analysis Methods
3.1 In Vitro Studies
In Vitro studies typically use a 96-well plate with a number of doses of each monotherapy and their combinations. The experiment can be replicated on, for example, three plates. A factorial/checkerboard design is often used in the industry. Here we illustrate the study with an example from Harbron (2010) and the data is reproduced in Table 13.1. Nine doses were tested for each monotherapy with three-fold spacing, of which the six lowest doses were tested in combination based on a factorial design. The test was replicated on three plates, resulting in three growth inhibition values. We use the three-parameter logistic model to model the monotherapy dose response curves.
where y is the drug response at dose d, E the maximum drug response (tumor inhibition), m the slope parameter, and EC 50 the dose that produces 50 % of the maximum drug response. Note that another parameter can be added to represent the minimum drug response, which we assume to be 0. The model was fit to monotherapy data of drug 1 and drug 2 in Table 13.1 and displayed in Fig. 13.2.

Three parameter logistic model fitting for monotherapy data of drug 1 and drug 2
For the data in Table 13.1, the question of interest is, “Are these two drugs synergistic?”
This turns out to be a question that has been extensively explored for almost a century and will continue to be researched. The difficulty can be illustrated with the following example. Suppose two people A and B need to plant and water a given number of trees in a park. A and B can finish planting and watering in 10 h and 6 h respectively by oneself. Now suppose they work together. If each still does his/her own planting and watering, then together you can expect they will finish in 1/(1/10 + 1/6) = 3.75 h. However, if they finish in a shorter time, say, 3.5 h, then we will say there is synergy from their teamwork. On the other hand, if they finish in a longer time, say, 5 h, then there is antagonism from their teamwork. In this case the expected or reference teamwork time is 3.75 h. Now consider another case where person A is better at planting and person B is better at watering. Let us assume it takes person A to plant all trees in 3 h and person B to water all trees in 3 h. Then they can finish planting and watering in 3 hours. So in this case, 3 h is the reference teamwork time. If together they finish in less than (or more than) 3 h, then their teamwork is synergistic (or antagonistic). For example, if they finish in 3.5 h, then there is antagonism from their combination work. Therefore, evaluation of synergy depends on a reference value which in turn is dependent on the way these two people work.
3.1.1 Reference Models
We will see that evaluation of the synergy of a drug combination also needs a reference model. There are different choices of reference model that may lead to different conclusions for the same drug combination data. Some suggest that choice of reference model be determined by the compounds’ mechanism of action (Greco et al. 1995). Even if this is the case, sometimes we know the mechanism of action of both compounds, but other times we do not know. In the above example, if we do not know about these two people’s working efficiency, but only know they together finish in 3.5 h, then we cannot tell whether or not there is synergy. In the following we discuss reference models for drug combinations, their relationship and how/when to apply them.
3.1.1.1 Loewe Additivity
This reference model dates back to the early twentieth century (Loewe 1928). Suppose drug 1 and drug 2 have monotherapy dose response curves, respectively,\( {y}_i={f}_i\left({d}_i\right),\,i=1,\,2 \), as defined in (13.1), where d i is the dose of drug i. If a combination of the two drugs with doses d 1 and d 2 produces a response y, and,
where \( {D}_i(y)={f_i}^{-1}(y),\kern0.7em i=1,\kern0.5em 2 \) is the dose for monotherapy drug i to generate the same response y, then we say the two drugs are synergistic (additive, antagonistic) when τ < 1(=1, >1) at combination d 1 and d 2. Several comments are in order for this definition. First, τ is also called interaction index (Berenbaum 1989). Second, the effect of drug combination is evaluated locally. In other words, τ depends on d 1 and d 2. It is very likely that two drugs are synergistic at one combination, but additive or antagonistic in other combinations. Third, when τ =1, we can re-write the equation as,
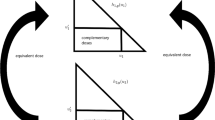
where \( \rho (y)={D}_1(y)/{D}_2(y) \) is called relative potency between drug 1 and drug 2 at response y. Then amount of drug 2, d 2, can be considered as equivalent to \( \left({D}_1(y)-{d}_1\right) \) in terms of drug 1, with consideration of their relative potency, to produce a response y. If ρ(y) does not depend on y, we say these two drugs have a constant relative potency. So this definition of additivity applies both when relative potency is constant and when it is not constant. In the latter case, remember to use the relative potency at response y from the combination, which is often misunderstood. For example, Perterson and Novick (2007, pp. 131–132) argue that this definition produces contradicting results when relative potency is not constant, but they did not use the relative potency at the response y produced by the combination d 1 and d 2. Instead, they used relative potency at f 1(d 1) in one derivation and f 2(d 2) in the other derivation. A detailed explanation of Loewe additivity with varying relative potency can be found in Plummer and Short (1990). Finally, the definition can be presented graphically with an isobologram as in Fig. 13.3. The response used in the figure is y = 50 %. If a combination of the two drugs at doses (d 1, d 2) also produces a response y = 50 %, then the two drugs are synergistic (additive, antagonistic) at these two doses if the point (d 1, d 2) falls below (on, above) the line in Fig. 13.3.

Isobologram at 50 % inhibition. The two drugs are synergistic (antagonistic) at any combination of (d 1, d 2) below (above) the line and producing 50 % inhibition
There are two types of synergy evaluation methods based on Loewe additivity. One is to estimate the interaction index and find its confidence interval (Greco et al. 1995; Lee and Kong 2009; Harbron 2010). Instead of estimating the index at each combination, Zhao et al. (2012) constructed an interaction index surface with a confidence band for the drug combination region (\( a<{d}_1<b \), \( c<{d}_2<d \)), which provides synergy information for tested or untested combinations in this region in a continuum. The other type is a response surface approach and a parameter(s) in the response model measures the departure from additivity (Plummer and Short 1990; Greco et al. 1995; Kong and Lee 2006). Although these two types are in essence equivalent, the former gives the interaction index more explicitly. In this chapter we will take the first method since it is consistent with use of isobolograms, with which most scientists are familiar.
3.1.2 Bliss Independence
This reference model was proposed by Bliss (1939). Assuming two drugs act on the same target independently, the Bliss independence model can be presented as follows,
where p 12, p 1, and p 2 are observed inhibition of combining drug 1 and drug 2 at doses (d 1, d 2), monotherapy drug 1 at dose d 1, and monotherapy drug 2 at dose d 2, respectively. For example, in Table 13.1, drug 1 had average inhibition p 1 = 60.4% at d 1 = 9, drug 2 had average inhibition p 2 = 15.4 % at dose d 2 = 3, and a combination of drug 1 and drug 2 at (9, 3) resulted in an average inhibition of p 12 = 76.6 %, which was larger than \( {p}_1+{p}_2-{p}_1\ast {p}_2 \) = 66.5 %, the two drug are synergistic at combination (9, 3).
Note that
is the probability statement for a union of two independent events (Casella and Berger 2002). It can be interpreted as: the expected chance, under the assumption of Bliss independence, of a disease target being affected by a combination of drug 1 at dose d 1 and drug 2 at dose d 2 is equal to the sum of chances of the disease target being affected by monotherapies drug 1 and drug 2 at the same doses, respectively, minus the chance of the disease target being affected by both drugs simultaneously. In fact, these p’s are the same as “y” in Eq. (13.1). We use p here for its connection to probabilities.
At the time of writing, there is no index defined based on Bliss independence in the literature. In the following we introduce a new index. Equation (13.4) can be rewritten as,
Similar to the interaction index based on Loewe additivity, we define the independence index as,
and
To implement the independence index, we suggest using log-transformation for a better model fitting.
or \( \frac{ \log \left(1-{p}_{12}\right)}{ \log \left(1-{p}_1\right)+ \log \left(1-{p}_2\right)}=\eta \), and now
since \( 0<1-{p}_{12}<1 \), and \( \log \left(1-{p}_{12}\right)<0 \). With introduction of this new index, analysis methods based on Loewe additivity and Bliss independence can be conducted in a similar fashion and both results can be presented as an index.
3.1.3 Analysis of an Example
Here we use the data in Table 13.1 to demonstrate analysis methods based on the two reference models discussed in the last two subsections. For the Loewe additivity reference model, we recommend Harbron’s unified approach (Harbron 2010). It can model an overall interaction index for the whole experimental dose space of the two drugs, interaction indices for each dose level of drug 1 or drug 2, or interaction indices at each combination of two drugs. Since these models are hierarchical, one can do model selection by testing extra residual reduction as in typical regression methods. The model does not only give a point estimate of the interaction indices, but also provides a p-value or interval estimate. A core R program for the model fitting is available in the appendix of that paper.
First we fitted model (13.2) with dose response model in (13.1). The result was \( \widehat{\uptau}=0.605 \) with a p-value <0.0001. Therefore, overall the two drugs were statistically significantly synergistic.
Next we fitted a model with an interaction index at each combination. The model is given in Eq. (13.5).
The results are shown in Fig. 13.4, where indices in color were statistically significant (at significance level 0.05). This figure revealed that the two drugs were significantly synergistic at high doses of drug 1.

Estimates of interaction index at each combination. Statistically significant synergistic effects are shown in blue. (Note these estimates differ slightly from the figure in Harbron’s (2010) paper)
Other index pattern can be modeled, for example, for each dose level. An interaction index surface can also be constructed, as in Zhao et al. (2012).
Next we analyze the same data based on the Bliss independence reference model. We first use an approach that is simple and often used by scientists. Since at each dose combination there were three replicates, we can obtain three values of the difference on the left hand side of (13.3). A t-test can be used to test whether the difference is significantly different from zero with the three values. The mean difference at each combination is depicted in Fig. 13.5, with numbers in bold, italic, and color font statistically significantly larger than zero (at significance level 0.05). These numbers represent synergistic dose combinations. If a mean difference is statistically significantly smaller than zero, then corresponding dose combination is antagonistic. There is no such combination based on Table 13.1. Similar to Fig. 13.4, Fig. 13.5 also revealed that the two drugs were synergistic at higher dose levels of drug 1. However, there were more significantly synergistic dose combinations based on Loewe Additivity than those based on Bliss independence.

Observed minus expected mean difference at each combination. Statistically significant synergistic effects are shown in blue
In this analysis, a t-test was conducted at each drug combination. Since there were only three replicates, the power is obviously limited. One may use another significance level instead of 0.05. A better approach is to analyze all the data in one model. One way to do this was achieved in Zhao et al. (2014).
Finally we analyze this data set with the independence index. This can also use Harbron’s framework and determine an overall independence index and an independence index at each dose combination. The Overall independece index was estimated to be \( \widehat{\upeta}=1.52 \) with a p-value <0.0001, indicating two drugs were statistically significantly synergistic. Independence indices at all dose combinations are shown at Fig. 13.6, revealing almost the same synergy results as the interaction index method.

Estimates of independence index η at each combination. Statistically significant synergistic effects are shown in blue
3.1.4 Relationship Between Loewe Additivity and Bliss Independence
Obviously for a given data set, using different reference models can give different synergy result. Which one should a scientist take? If the mechanism of action (MoA) is ascertained, then a choice can be made: if the two drugs have the same MoA, then the Loewe additivity model should be used; on the other hand, if the two drugs have independent MoAs, then the Bliss independence model should be used. However, in most situations, the MoA of two drugs is usually not ascertained. So it is interesting to know the relationship between these two reference models, irrespective of MoA of the two drugs.
Berenbaum (1989) showed that the two reference models were equivalent if the dose response of two drugs follows an exponential model. Drescher and Boedeker (1995) extended this comparison to other models, including probit, logit and Weibull models. However, for these models, Loewe additivity and Bliss independence may or may not give the same conclusion (synergistic or not).
We suggest one should analyze the same data set with both reference models. Then depending on the context of the analysis, one can choose a conservative result. The context could be to look for a therapeutic effect. For example, in most drug discovery settings, scientists want to find drug combinations that show synergy. In this case, one should choose dose combinations only if both reference models show a synergistic result. The other context could be to look for a toxic effect. For example, in interaction test for toxic pollutants, one wants to avoid dose combinations showing synergy. In this situation, one should conclude synergy as long as one reference model result demonstrates so.
3.2 Min Test for In Vivo or Clinical Studies
For in vivo studies or clinical trials, a factorial design is usually used. Since there are only a few dose levels per drug, it is hard to characterize a dose response curve for monotherapies. Therefore, a min testis often used for data analysis which tests whether the effect of a dose combination, say (d 1, d 2), is significantly larger than the effect of drug 1 at d 1 AND drug 2 at d 2. Therefore analysis for such studies does not require a reference model. However, multiplicity adjustment may be needed to control the overall type I error rate since this test is conducted at multiple combinations. For details on this test and analysis methods for such studies, refer to Hung (2000) and references therein.
4 Discussions and Conclusions
The challenge of how to evaluate synergy of drug combinations has a long history. Synergy evaluation requires a reference model that is usually based on the monotherapy drug dose response relationship and describes the expected effect of two drug combinations when there is no interaction between them. Loewe additivity and Bliss independence, albeit criticized frequently from one perspective or another, have been the two central competing reference models, as Greco et al. (1995) reviewed. In this chapter, we defined these two reference models and introduced some analysis methods based on them. We also introduced a new independence index based on Bliss independence that can be modeled similarly to the interaction index based on Loewe additivity.
There is still no “standard” method to evaluate synergy. In fact, Greco (2010) recently asked some experts in this field to evaluate the same two data sets, and without surprise conclusions differed. Readers are strongly encouraged to go through the articles to appreciate analysis methods other than those discussed in this chapter. A method of particular interest is nonlinear blending, proposed by Perterson and Novick (2007). This method takes a mixture experimental design by fixing the total amount of two drugs and uses the idea of min test with a response surface model to evaluate synergy. A combination is synergistic if its response is higher than both monotherapy responses. So this method does not define a reference model such as Loewe additivity and Bliss independence. A problem with this approach is that when the potency of the two drugs is dramatically different, it is difficult to study a fixed amount of both drugs. For example, in their example (Fig. 9 on Page 141) combining FLG and AZT, the former has an EC50 of about 7.2 and the latter has an EC50 of 0.04. It may be difficult to even increase the dose of AZT to the level of 7.2. A remedy may be to use doses scaled by EC50.
There are significantly fewer articles in the literature using Bliss independence reference models. One reason may be that its simplicity does not warrant any publication. Another reason is that there is not an index for this reference model. However, this method is more often used by scientists, especially in Oncology, for the same reason of simplicity. More statistical rigor should be brought into analysis methods using this model, instead of making decisions based on the difference in Eq. (13.3). Zhao et al. (2014) is such an attempt. In this chapter, we introduced the independence index that provides a similar framework for synergy evaluation as the interaction index.
Another research area is to further study the relationship between these two reference models. Berenbaum (1989) and Drescher and Boedeker (1995) have identified some situations in which the relationship between these two reference models can be established. The relationship depends on the dose response models used. More work is needed to study the relationship between the interaction index and the independence index and to further understand how to interpret such a relationship in the context of synergy evaluation.
Ideally, there should be some “standard” practice for synergy evaluation. We mentioned some principles along this line, such as choosing a reference model based on mechanism of action (MoA) if the MoA is clear, or analyzing data with both reference models and making decisions based on therapeutic or toxic context.
References
Berenbaum MC (1989) What is synergy? Pharmacol Rev 41:93–141
Bliss CI (1939) The toxicity of poisons applied jointly. Ann Appl Biol 26:585–615
Casella G, Berger RL (2002) Statistical inference (second edition) Duxbury/Thomson Learning, Pacific Grove, CA
Donev AN, Tobias RD (2011) Optimal serial dilutions designs for drug discovery experiments. J Biopharm Stat 21:484–497
Drescher K, Boedeker W (1995) Assessment of the combined effects of substances: the relationship between concentration addition and independent action. Biometrics 51:716–730
Greco WR (2010) Concentration-effect modeling of single agents and combinations of agents. Frontier Biosci, preface
Greco WR, Bravo G, Parsons JC (1995) The search for synergy: a critical review from a response surface perspective. Pharmacol Rev 47:331–385
Harbron C (2010) A flexible unified approach to the analysis of pre-clinical combination studies. Stat Med 29:1746–1756
Hung HMJ (2000) Evaluation of a combination drug with multiple doses in unbalanced factorial design clinical trials. Stat Med 19:2079–2087
Kong M, Lee JJ (2006) A generalized response surface model with varying relative potency for assessing drug interaction. Biometrics 62:986–995
Lee JJ, Kong M (2009) Confidence intervals of interaction index for assessing multiple drug interaction. Stat Biopharm Res 1:4–17
Loewe S (1928) Die quantitation probleme der pharmakologie. Ergeb Physiol Biol Chem Exp Pharmkol 27:47–187
Perterson JJ, Novick SJ (2007) Nonlinear blending: a useful general concept for the assessment of combination drug synergy. J Receptor Sig Transduct 27:125–146
Plummer JL, Short TG (1990) Statistical modeling of the effects of drug combinations. J Pharmacol Methods 23:297–309
Straetemans R, O’Brien T, Wouters L, Van Dun J, Janicot M, Bijnens L, Burzykowski T, Aerts M (2005) Design and analysis of drug combination experiments. Biom J 47:299–308
Tallarida RJ (2000) Drug synergy and dose-effect data analysis. Chapman and Hall/CRC, Boca Raton, FL
Tan MT, Fang H, Tian G (2009) Dose and sample size determination for multi-drug combination studies. Stat Biopharma Res 1:301–316
Zhao W, Zhang L, Zeng L, Yang H (2012) A two-stage response surface approach to modeling drug interaction. Stat Biopham Res 4:375–383
Zhao W, Sachsenmeier K, Zhang L, Sult E, Hollingsworth RE, Yang H (2014) A new Bliss independence model to analyze drug combination data. J Biomol Screen 19:817–821
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Zhang, L., Yang, H. (2016). Design and Evaluation of Drug Combination Studies. In: Zhang, L. (eds) Nonclinical Statistics for Pharmaceutical and Biotechnology Industries. Statistics for Biology and Health. Springer, Cham. https://doi.org/10.1007/978-3-319-23558-5_13
Download citation
DOI: https://doi.org/10.1007/978-3-319-23558-5_13
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-23557-8
Online ISBN: 978-3-319-23558-5
eBook Packages: Mathematics and StatisticsMathematics and Statistics (R0)