
Abstract
This chapter reviews the clinical, macroscopic, and microscopic features and the differential diagnosis of the most common pancreatic lesions seen in a routine surgical pathology practice. It begins with the main congenital anomalies and metabolic disorders and then proceeds to the inflammatory conditions. The neoplasia section begins with the most common neoplasm of the pancreas, invasive ductal carcinoma. This is followed by a discussion of preinvasive ductal neoplasia and serous cystic neoplasms. The nonductal neoplasia section covers acinar, neuroendocrine, and solid pseudopapillary neoplasms and pancreatoblastoma. Finally, quick review of how to report pancreatic tumors and TNM classification of pancreatic tumors is presented.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Acinar
- Colloid
- Cystic
- Ductal
- Neuroendocrine
- IPMN
- IOPN
- PanIN
- Pancreatitis
- Pancreatoblastoma
- Serous
- Solid pseudopapillary
Congenital Anomalies
Annular Pancreas
Clinical
-
♦
Very rare embryologic abnormality
-
♦
Pancreatic parenchyma encircles the duodenum
-
♦
Main pancreatic duct follows a course different than usual
-
♦
Some associated with Down syndrome or other congenital conditions
Microscopic
-
♦
Irregularly shaped islets composed of pancreatic polypeptide (PP) cells (consistent with ventral bud origin)
-
♦
May be associated with pancreatitis
Heterotopic Pancreas
Clinical
-
♦
Occurs in a variety of organs, most common in gastrointestinal and biliary tracts
-
♦
Most are incidental
-
♦
May form macroscopic nodules
-
♦
May rarely show pancreatic pathology (pancreatitis, pancreatic neoplasia) or local complications such as ulceration and hemorrhage
Microscopic
-
♦
All or some components of the pancreas (acini, ducts, or islets)
Differential Diagnosis
-
♦
Metaplasia
-
Microscopic
-
Usually, acini only
-
Pancreas Divisum
-
♦
Failed fusion of the dorsal (Santorini) and ventral (Wirsung) ducts in embryologic life
-
♦
“Division” of drainage between the anterosuperior and posteroinferior head
-
♦
Usually clinically inconsequential
-
♦
Some patients develop pancreatitis, usually dorsally
-
♦
Diagnosis is radiologic; pathologic documentation is difficult, if not impossible
Congenital Cysts
-
♦
Intestinal duplication may present as a cystic lesion
-
♦
Foregut cysts (some with ciliated/respiratory-type epithelia)
-
♦
“Fibrocystic”-type changes may occur in a variety of congenital syndromes
Pancreas in Metabolic and other Medical Disorders
Nesidioblastosis
-
♦
Functional disorder of the β cells
-
♦
Associated with persistent hyperinsulinemic hypoglycemia (PHH) in newborns and very rarely in adults
-
♦
Etiopathogenesis not fully understood; a genetic susceptibility to develop abnormal reaction to abrupt metabolic changes (such as substantial weight loss or gastric bypass) has been implicated
-
♦
Potential susceptibility genes include SUR1 [sulfonylurea receptor gene], Kir6.2 [inwardly rectifying potassium channel], or GCK/GLUT1, ABCC8, and KCNJ11 mutations
Microscopic
-
♦
Newborn Type
-
Can be focal (in about 40% of the patients)
-
Characterized by the presence of hypertrophic insulin cells . Many islets are large, typically measuring up to several millimeters (much more pronounced in the newborns than in the adults)
-
β Cells are disproportionally higher in number
-
Clinicopathologic correlation is necessary; no good criteria for “hyperplastic” versus normal islet
-
-
♦
Adult Type
-
Pathologic findings vary greatly; in 1/3 of the cases, the pancreatic changes are minimal (not recognizable without clinical correlation)
-
The most consistent finding is the presence of cytologically conspicuous islet cells
-
All other criteria, such as a lobulated arrangement of the cells within the islets, hyperplasia, and hypertrophy of islets or an increased β-cell number, are only found in a fraction of the patients
-
The final diagnosis relies on the pathologic analysis of the pancreatic tissue specimen, which must first exclude a small insulinoma and then use the criteria given above
-
Diabetes Mellitus
-
♦
No identifiable changes in most cases
-
♦
Subtle alterations in the islets of some patients including:
-
Altered number or size (no established criteria)
-
Mild fibrosis
-
Amyloid deposition (of “amyloid islet” – amylin type, Fig. 43.1)
Fig. 43.1. 
Amyloid deposition in the islets of Langerhans.
-
Mild leukocytic infiltrates
-

Cystic Fibrosis
-
♦
Pancreatic involvement with “fibrocystic” appearance in 80–90%
-
♦
Hyperviscous mucus precipitates in the ducts resulting in duct ectasia
-
♦
Obstruction-related changes including acinar atrophy and replacement of atrophic lobules by interstitial fibrosis
Inflammatory Conditions
Acute Pancreatitis
Clinical
-
♦
Most are due to alcohol abuse; some are related to gallstones
-
♦
Pain and elevated serum enzyme levels (especially amylase)
-
♦
In some, pain is associated with nausea and vomiting
-
♦
Variety of other metabolic complications
-
♦
Local anatomic complications such as pseudocysts (see below), abscesses, hemorrhage, or thrombi
Microscopic
-
♦
Findings range from “mild edematous pancreatitis” to “severe necrotizing pancreatitis.”
-
♦
Mild edematous pancreatitis: interstitial edema and usually microscopic fat necrosis, mainly on the surface
-
♦
Severe necrotizing pancreatitis: extensive and sometimes hemorrhagic tissue necrosis involving both pancreatic parenchyma and extrapancreatic fat tissue, development of complications
-
♦
Fat necrosis (Fig. 43.2)
Fig. 43.2. 
Acute pancreatitis with fat necrosis. There is a rim of neutrophils around the necrotic focus.
-
Grossly, chalky white-yellow areas
-
Fragmented adipocytes with saponification and/or calcification and a rim of neutrophils
-

Chronic Pancreatitis
Alcohol or Obstruction Related
Clinical
-
♦
Most are related to alcohol abuse, obstruction (lithiasis or tumors), or other chemical/metabolic factors (hypercalcemia)
-
♦
Recurrent abdominal pain that is later accompanied by exocrine insufficiency and diabetes
-
♦
Increased risk of developing a pancreatic carcinoma
-
♦
Complications such as pseudocyst, persistent stenosis of the bile duct, duodenal stenosis, and fistulas
Macroscopic
-
♦
Fibrosis and effacement of pancreatic lobular architecture
-
♦
In some cases, calcifications and intraluminal stones
Microscopic
-
♦
Ductal dilatation with eosinophilic mucoprotein plugs (with/without calcifications, Fig. 43.3)
Fig. 43.3. 
Alcohol- or obstruction-related chronic pancreatitis (acinar atrophy and interstitial fibrosis) associated with lithiasis represented in this section as calcified intraluminal material.
-
♦
Remaining small ductules may appear pseudoinfiltrative
-
♦
Acinar dilatation and atrophy
-
♦
Interstitial fibrosis with variable cellularity
-
♦
Remaining islets become prominent and may appear pseudoinfiltrative or form micronodules (Fig. 43.4)
Fig. 43.4. 
“Hyperplastic islets.” Islets of Langerhans become prominent or appear proliferative in some pathologic conditions of the pancreas, in particular chronic pancreatitis.


Differential Diagnosis
-
♦
Ductal carcinoma
-
Irregularities in the number, spacing, distribution, and contours of the ducts
-
In some cases, pale, foamy, microvesicular cytoplasm and a dense chromophilic, apical condensation
-
Cytologic atypia with nuclear enlargement and contour irregularities
-
Ducts in places that they do not belong: perineurial, intravascular, and in adipose tissue (naked ducts without associated islets or acini)
-
-
Autoimmune Pancreatitis, Type 1
Clinical
-
♦
Typically seen in sixth to seventh decade, male predominance
-
♦
Slight increase in jaundice compared to autoimmune pancreatitis with granulocytic epithelial lesions
-
♦
About 25% associated with established autoimmune conditions (PSC, Sjögren, etc.)
-
♦
Some with “multifocal inflammatory fibrosclerosis” (Riedel thyroiditis, orbital pseudotumor, mediastinal and retroperitoneal fibrosis, etc.)
-
♦
Radiographically, simulates pancreatic carcinoma; sausage-like appearance of the pancreas and halo formation are characteristic
-
♦
Elevated serum IgG4 levels (usually >135 mg/dL)
-
♦
Often responds well to steroid administration
Macroscopic
-
♦
Localized region of fibrosis and effacement of pancreatic lobular architecture producing mass-like enlargement
-
♦
Scarring; adhesions to adjacent organs
Microscopic
-
♦
Dense “duct-centric” inflammation of predominantly lymphoplasmacytic cells and expansion of periductal fibrous tissue (Fig. 43.5)
Fig. 43.5. 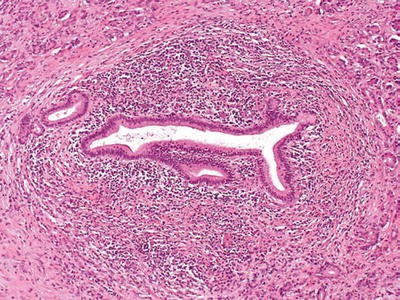
Type 1 autoimmune pancreatitis. Characteristic periductal lymphoplasmacytic inflammation, with a dense rim of inflammatory cells, and concentric bands of periductal fibrous tissue surrounding the narrowed pancreatic duct.
-
♦
Periphlebitis and obliterative venulitis are common (Fig. 43.6); frank vasculitis may be seen (not common)
Fig. 43.6. 
Type 1 autoimmune pancreatitis. Characteristic venulitis, with aggregates of lymphoid cells in the wall and undermining the epithelium. Sometimes, veins are completely obliterated and replaced by the inflammation and are recognized by their proximity to uninvolved arteries.
-
♦
Interstitial fibroblastic proliferation with storiform architecture (“inflammatory pseudotumor”-like)
-
♦
Immunohistologically, >50 IgG4+ plasma cells/HPF is considered highly specific for AIP type 1. However, an elevated IgG4+/IgG+ plasma cell ratio of >40% is more meaningful than IgG4+ plasma cell counts alone in establishing the diagnosis


Autoimmune Pancreatitis, Type 2
Clinical
-
♦
Seen in fifth to sixth decade, almost equal male/female ratio
-
♦
Approximately 30% of the cases have associated inflammatory bowel disease, such as ulcerative colitis
-
♦
It is not associated with serum IgG4 elevation
Microscopic
-
♦
Intraepithelial neutrophils and occasionally eosinophils (“granulocytic epithelial lesions, GELs”), especially in intralobular ducts, are the hallmark
-
♦
In the cases with the most severe GELs, the acute inflammatory infiltrate extends into the ductules, acini, and interstitial spaces
-
♦
Phlebitis is not a common pattern
-
♦
Has none or very few (<10 cells/HPF) IgG4+ plasma cells
Paraduodenal Pancreatitis
Synonyms
-
♦
Cystic dystrophy of heterotopic pancreas, groove pancreatitis
Clinical
-
♦
Predominantly in 40–50-year-old males
-
♦
History of alcohol abuse is common
-
♦
Waxing and waning severe upper abdominal pain and postprandial vomiting are common
-
♦
Predominantly solid ones often mimic pancreas cancer or ampullary/periampullary tumors, radiographically
Macroscopic
-
♦
Often centered in the region of minor papilla (and the adjacent pancreas)
-
♦
Scarring of duodenal wall and/or distal common bile duct and/or the “groove” between the duodenum, CBD, and pancreas
-
♦
Trabeculation of duodenal musculature with occasional cysts (Fig. 43.7)
Fig. 43.7. 
Paraduodenal pancreatitis. In most cases, there is some degree of thickening and scarring of duodenal wall with trabeculations and associated cysts. Sometimes, one or more cysts achieve large sizes and form paraduodenal wall cyst.
-
♦
Paraduodenal wall cyst (up to 10 cm) mimicking intestinal duplication may occur

Microscopic
-
♦
Dense myoid stromal proliferation with intervening rounded lobules of pancreatic tissue (“myoadenomatosis,” Fig. 43.8)
Fig. 43.8. 
Paraduodenal pancreatitis. Myoadenomatosis-type changes, which are often associated with accessory duct abnormalities, may form a pseudotumor that can be mistaken clinically as cancer.
-
♦
Brunner gland hyperplasia
-
♦
Small cystic spaces lined by cellular stroma
-
♦
Extravasated (stromal) mucoprotein plugs surrounded by eosinophils or multinucleated giant cells
-
♦
Prominence of nerve bundles mimicking traumatic neuroma

Pseudocysts
Clinical
-
♦
Complication of pancreatitis
-
♦
Most frequently seen in alcoholic males
-
♦
Most common cystic lesion of the pancreatic region (60–70%) but rarely sampled for pathologic examination
-
♦
Occurs due to postnecrotic resorption of peripancreatic fat necrosis
Macroscopic
-
♦
1–15 cm unilocular cyst, filled with necrotic material fluid
-
♦
Peripancreatic
Microscopic
-
♦
Depends on the stage of the process
-
♦
No epithelial lining by definition
-
♦
The lumen contains necrotic adipose tissue, precipitated acinar secretions, and mucoprotein plugs
-
♦
The wall consists of dense fibrous tissue with various degrees of granulation-type changes
Differential Diagnosis
-
♦
Mucinous cystic neoplasm
-
Epithelial lining
-
Ovarian-like stroma with more wavy and layered appearance (compared to haphazard cellularity of fibroblastic reaction in pseudocysts)
-
-
♦
Other cystic lesions
-
Epithelial lining or specific characteristic features
-
Infections
-
♦
Bacterial, fungal, or parasitic infections may involve the pancreas, but none has any particular affinity for this organ
Neoplasia
Ductal Neoplasia
Invasive Ductal Adenocarcinoma
Synonyms
-
♦
Pancreatobiliary, tubular
Clinical
-
♦
>85% of all pancreatic tumors
-
♦
More common in developed countries, fourth leading cause of cancer deaths in the USA
-
♦
M/F = 1.5/1, African American/Caucasian = 2/1, mean age 63, very seldom under the age of 40
-
♦
Proposed risk factors include long-standing diabetes mellitus, smoking, and chronic pancreatitis (especially hereditary pancreatitis); a few are familial, some associated with familial atypical multiple mole/melanoma (FAMMM) syndrome (p16 related)
-
♦
Common symptoms: abdominal or back pain, weight loss, and jaundice
-
♦
Some patients develop diabetes mellitus
-
♦
80% are deemed “unresectable” due to early spread (to mesenteric vessels/retroperitoneum, liver, or peritoneum)
-
♦
Median survival: 8 months if unresectable but treated with chemo-/radiotherapy and 12 months if resected, 5-year survival <5%; very few patients are alive at 7 years
-
♦
Almost all develop metastasis (mostly to liver or peritoneum)
Macroscopic
-
♦
70% occur in the head
-
♦
Typical size = 3 cm; the tumor is widely disseminated or fatal by the time it reaches 6–7 cm
-
♦
“Scirrhous” pattern: firm, white-gray or yellow mass with ill-defined borders (Fig. 43.9)
Fig. 43.9. 
Ductal adenocarcinoma is grossly a scirrhous carcinoma, characterized by firm white mass with ill-defined irregular borders.
-
♦
Obstruction of the ducts (in particular, the common bile duct) is typical
-
♦
May ulcerate into the duodenum

Microscopic
-
♦
Infiltrating tubular units (often widely scattered with open lumina), cords, or individual cells (Fig. 43.10)
Fig. 43.10. 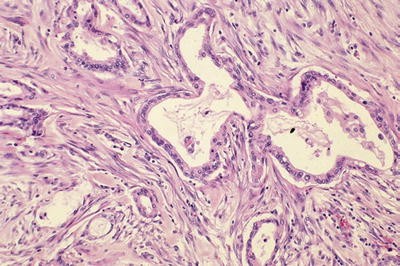
Invasive ductal carcinomas of the pancreas are characterized by infiltrating small tubular units with open lumina, surrounded by desmoplastic stroma of variable cellularity.
-
♦
Abundant desmoplastic stroma of variable cellularity
-
♦
Cuboidal to columnar cells with variable mucin and nuclear atypia
-
♦
Perineurial invasion in >75% of the cases (Fig. 43.11)
Fig. 43.11. 
Perineural invasion is common in invasive ductal carcinoma.
-
♦
Gland formation and bland cytology may be retained even in perineurial or vascular invasion
-
♦
Extension to retroperitoneal tissue, especially through the posterior uncinate region, is very common


Variants
-
♦
Foamy gland pattern (Fig. 43.12)
Fig. 43.12. 
Invasive ductal adenocarcinoma with foamy gland pattern can be deceptively benign appearing, as reflected in this focus of lymph node metastasis.
-
Abundant pale, foamy, microvesicular cytoplasm stuffed with small, evenly shaped vesicles
-
Thin, distinct band of chromophilic condensation in the apical cytoplasm forming a brush border-like zone
-
-
♦
Vacuolated cribriform pattern (Fig. 43.13)
Fig. 43.13. 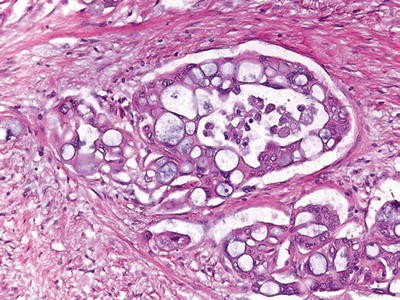
Cribriform/vacuolated pattern is not uncommon in ductal adenocarcinoma and may help recognize this tumor type in metastatic sites.
-
Multicell-sized vacuoles resembling lipocytes (or signet ring cells) and forming a cribriform architecture
-
Vacuoles contain necrotic debris and neutrophils
-
Nuclear atypia is prominent
-
-
♦
Other rare patterns: large duct pattern (mimicking intraductal neoplasia), cord-like formation (Fig. 43.14), clear cell pattern (mimicking renal cell carcinoma), signet ring, hepatoid, oncocytic, and rhabdoid patterns
Fig. 43.14. 
Invasive ductal carcinoma, cord-like pattern. Often glandular areas are admixed with less differentiated patterns such as this one mimicking mammary lobular carcinoma.
-
♦
May mimic the primary tumors at metastatic sites
-
Bronchioloalveolar pattern (“lepidic” growth) in the lung
-
Mucinous cystic pattern mimicking primary borderline tumors in the ovary
-



Immunohistochemistry
-
♦
CK7+, CK20+/−
-
♦
Mucin positive, especially acidic sialomucin
-
♦
Mucin-related glycoproteins and oncoproteins [CA19-9, CEA, B72.3, MUC1 (Fig. 43.15), MUC5AC, DUPAN2] +
Fig. 43.15. 
MUC1 in ductal adenocarcinoma. The labeling is typically apical membranous in the glandular areas and becomes more intracytoplasmic in the less differentiated (nonglandular) component of the tumor.
-
♦
May contain scattered neuroendocrine cells
-
♦
Acinar enzymes typically lacking
-
♦
Loss of DPC4 (SMAD4), seen in approximately 50% of the cases, strongly favors of adenocarcinoma, provided that inbuilt controls are working properly
-
♦
Alterations in codon 12 of KRAS oncogene (90%), CDKN2A (p16, 95%), TP53 (50%), DPC4 (>50%), BRCA2 (7%), and STK11 (Peutz-Jeghers, 5%) genes

Differential Diagnosis
-
♦
Noninvasive ducts (benign reactive ducts or intraductal neoplasia)
-
Smooth contours
-
Lobular, organized distribution, spatially related to acini and/or islets
-
Smaller ducts tend to be in clusters; larger ones have elongated lumina
-
-
♦
Pseudotumoral pancreatitis
-
Approximately 5% of pancreatectomies performed with the clinical diagnosis of “pancreas cancer” prove to be chronic pancreatitis (see pancreatitis section)
-
-
♦
Ampullary/common bile duct carcinomas
-
May be morphologically identical
-
Location is determined by gross examination
-
Preinvasive neoplasia in the corresponding sites
-
-
♦
Nonductal tumors (acinar, neuroendocrine, solid pseudopapillary neoplasia, and pancreatoblastoma)
-
Stroma poor (no desmoplasia)
-
Cellular, nonglandular neoplasia with sheetlike or nested growth patterns
-
Relatively uniform cytology
-
-
♦
Intestinal-type adenocarcinoma (gastrointestinal or ampullary origin)
-
Basophilic appearance, columnar cells, stratification
-
Large, tubular units with relatively compressed lumina
-
CK7−, CK20+, MUC1−/+, MUC2+, MUC5AC−
-
-
♦
Ovarian adenocarcinoma
-
Cellular, tubular areas composed of long, branching units with slit-like spaces
-
Many psammoma bodies
-
Tufts and micropapillae
-
WT1+/MUC5AC−
-
Other Related Carcinomas
-
♦
Undifferentiated (sarcomatoid, Fig. 43.16): often, ordinary tubular pattern in the background
Fig. 43.16. 
This undifferentiated carcinoma is composed of large, pleomorphic cells with sarcomatoid transformation.
-
♦
Adenosquamous and squamous:
-
Also have dismal prognosis like ordinary ductal adenocarcinomas
-
Immunohistochemical stains for p63 and CK903 confirm the squamous differentiation
-

Rare Carcinomas of Presumed Ductal Origin
Colloid Carcinoma
Definition
-
♦
Invasive carcinoma composed almost exclusively of extracellular mucin pools that contain scanty, detached carcinoma cells
-
♦
Almost always associated with intestinal-type intraductal papillary mucinous neoplasm
Clinical
-
♦
Mean age = mid-60s
-
♦
Thromboembolism in some cases
-
♦
Pure examples may have a protracted clinical course
Macroscopic
-
♦
Mean size = 4.5 cm
-
♦
Relatively well demarcated
-
♦
Gelatinous
Microscopic (Fig. 43.17)
-
♦
Well-defined pools of extracellular mucin that contain scanty, detached carcinoma cells
-
♦
Cells floating in mucin may form strips, signet ring cells, glands, or stellate clusters

Colloid carcinoma. Pools of mucin, some of which contain scanty, detached malignant cells.
Differential Diagnosis
-
♦
Other invasive carcinomas (ductal, signet ring, or others)
-
Invasive carcinoma cells outside the mucin or at least attached to the stroma
-
More cells than mucin
-
Loss of DPC4
-
-
♦
In situ neoplasia (mucinous cystic neoplasm, intraductal neoplasia)
-
Epithelium continuous and well attached to the stroma
-
Mucin not abundant in histologic sections (washed off during processing)
-
Undifferentiated Carcinoma with Osteoclast-Like Giant Cells
Clinical
-
♦
Very rare
-
♦
Aggressive behavior
Macroscopic
-
♦
Average size = 10 cm
-
♦
May appear well demarcated
-
♦
Most are soft, white-yellow to tan
-
♦
Some are almost completely cystic or have intraductal growth
Microscopic (Fig. 43.18)
-
♦
Sea of ovoid to spindle-shaped, highly pleomorphic mononuclear cells, in which a variable number of osteoclast-like giant cells are suspended
-
♦
Malignant cells are those smaller spindle-shaped, highly pleomorphic mononuclear cells, while the osteoclast-like giant cells are benign
-
♦
There is usually a conventional ductal adenocarcinoma pattern in the background
-
♦
Heterologous elements such as bone and cartilage can be seen
Immunohistochemistry
-
♦
Sarcomatoid and tubular elements show ductal differentiation (Table 43.1)
-
♦
Giant cells are of macrophagic nature; CD45+, CD68+

Undifferentiated carcinoma with abundant osteoclast-like giant cells.
Medullary Carcinoma
-
♦
Very rare
-
♦
Similar to the medullary carcinomas of the breast and colon
-
♦
Has protracted clinical course
-
♦
Some have synchronous and metachronous colon carcinomas, and some of these have hereditary nonpolyposis colorectal cancer (HNPCC) syndrome
Microscopic
-
♦
Pushing border-type infiltration
-
♦
Syncytial growth pattern
-
♦
Lymphoplasmacytic infiltrates
Immunohistochemistry
-
♦
Associated with microsatellite instability (loss of MLH1 and/or MSH2 expression)
Differential Diagnosis
-
♦
Metastatic carcinomas
-
♦
Acinar cell carcinoma
-
Trypsin+, MLH1, and MLSH2+ (not lost)
-
-
♦
Poorly differentiated ductal carcinoma
-
Scirrhous (scar-like) pattern
-
Small unit infiltration (tubules or cords)
-
Desmoplasia
-
Preinvasive Ductal Neoplasia
Pancreatic Intraepithelial Neoplasia
Definition and Classification
-
♦
Microscopic/incidental forms of preinvasive neoplasia in the ducts
-
♦
Encompasses a spectrum of changes from those previously called mucinous hypertrophy/metaplasia to frank CIS
-
♦
Spectrum graded as low-grade PanIN and high-grade PanIN (CIS) (per Baltimore consensus, December 2015)
-
♦
Presumed precursors of ductal adenocarcinoma
-
♦
Low-grade PanIN is a common, incidental finding even in normal pancreata
-
♦
High-grade PanIN is very common in pancreata with invasive ductal carcinoma and is exceedingly uncommon otherwise
Microscopic
-
♦
Not grossly detectable
-
♦
Atypical proliferative changes in the native ducts
-
♦
Ducts involved are typically <0.5 cm
-
♦
Low-grade PanIN: Simple, columnar, mucin-filled, perfectly polarized cells with small nuclei (previously PanIN-1A) or these changes + mild folding of the epithelium and early (basal) stratification (previously PanIN-1B; Fig. 43.19) or pseudostratification of nuclei; nuclear enlargement, more prominent folding (papillae); some cytologic atypia (previously PanIN-2; Fig. 43.20)
Fig. 43.19. 
Low-grade PanIN (Previously PanIN-1). In the background of columnar, mucin-filled, polarized cells (previously PanIN-1A), the mucosal folds at the center show mild stratification of cells (Previously PanIN-1B).
Fig. 43.20. 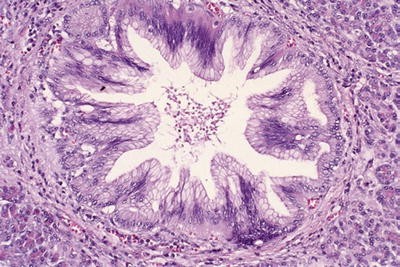
Another example of low-grade PanIN (Previously PanIN-2). This duct shows papillary folds with stratification of mildly irregular cells. Some of the nuclei are depolarized.
-
♦
High-grade PanIN: loss of polarity, irregular stratification, tufting, necrosis, mitosis, cytologic atypia (nuclear enlargement, pleomorphism, nuclear irregularities; Fig. 43.21)
Fig. 43.21. 
High-grade PanIN (Previously PanIN-3 or carcinoma in situ). There is loss of polarity, and tuft formation is evident. There are necrotic cells detached into the lumen of the duct. The nuclei are hyperchromatic and irregular.
-
♦
Clinical significance and rate of progression to invasive carcinoma undetermined



Immunohistochemistry
-
♦
Mucin of usually acidic sialomucin type
-
♦
Molecular alterations of ductal carcinogenesis increasing from 1A to 3 (see ductal adenocarcinoma section)
Differential Diagnosis
-
♦
Intraductal papillary mucinous neoplasms
-
Mass-forming neoplasia (clinically/grossly detectable papillary or cystic changes)
-
Size typically >1 cm
-
Many clinically symptomatic
-
Tall papillae, some with intestinal phenotype
-
MUC2 and CDX2 expression, common
-
-
♦
Invasive ductal carcinoma
-
Contour irregularities
-
Irregular clustering and haphazard distribution
-
Intraductal Papillary Mucinous Neoplasms (Table 43.2)
Definition
-
♦
Intraductal proliferation of mucinous cells of variable papillae formation and cystic change in the ducts
Clinical
-
♦
Increasing frequency due to detection of small cystic “incidentalomas.”
-
♦
Elderly (mean age 68), slightly more common in men, some with history of pancreatitis
-
♦
30% have coexisting tumors of other organs
-
♦
Endoscopic: mucin extrusion from ampulla of Vater
-
♦
Radiologic: dilatation of the ductal system
-
♦
Graded as IPMN, low-grade and IPMN, high-grade (CIS) based on the cytoarchitectural atypia (per Baltimore consensus, December 2015)
-
♦
Grade seems to correlate with clinical outcome, but unexpected clinical course has been noted in some, attributed to missed foci of invasive cancer that are either unresected because of unrecognized multifocality or undiagnosed during pathologic examination
-
♦
Presence of associated invasive carcinoma and the size of the invasive component are the most important prognostic factors
-
♦
“Branch duct” type tends to be smaller and more cystic and often proves to have only low-grade dysplasia, thus amenable for “watchful waiting.”
-
♦
“Main duct” type is often more complex, more diffuse, and prone to harbor carcinoma
-
♦
Overall 5-year survival >70%; the ones WITHOUT associated invasive carcinoma have a much better prognosis than the ones with associated invasive carcinoma
Macroscopic
-
♦
Dilatation of the main duct or one of its branches, sometimes multilocular cysts
-
♦
Tan, friable papillary nodules filling the ducts in some cases
Microscopic
-
♦
Intraductal proliferation of mucinous cells
-
♦
In cystic areas, tall columnar cells with abundant apical mucin
-
♦
Papillary areas have more atypia
-
♦
Papillae may have intestinal (Fig. 43.22), pancreatobiliary (Fig. 43.23), gastric (Fig. 43.24), or oncocytic (arborizing papillae with oncocytic cells – abundant, granular, acidophilic cytoplasm – and intracytoplasmic lumina, Fig. 43.25)
Fig. 43.22. 
In intestinal-type IPMNs, the papillae are morphologically similar to colonic villous adenomas.
Fig. 43.23. 
The lining epithelium of gastric-type IPMN resembles gastric foveolar epithelium.
Fig. 43.24. 
Pancreatobiliary-type IPMN reveals complex architecture and cuboidal cells with less mucinous cytoplasm and enlarged nuclei.
Fig. 43.25. 
Oncocytic-type IPMNs are characterized by complex branching papillae, oncocytic cells, and intraepithelial lumina formation.




Classification/Grading
-
♦
Pathologic classification and grading are valid only if the tumor is thoroughly examined
-
♦
IPMN with low-grade dysplasia: tall columnar mucinous cells with abundant apical mucin and well-polarized, uniform small nuclei without atypia or with mild/moderate atypia
-
♦
IPMN with high-grade dysplasia/carcinoma in situ: severe cytologic or architectural atypia (florid papillary nodules) with cuboidal nuclei, prominent nucleoli, mitotic figures, tufts, and necrosis
Immunohistochemistry
-
♦
The immunoprofile of different cell types parallels their lineage markers
-
♦
Intestinal-type IPMNs express intestinal lineage markers CDX2 and MUC2
-
♦
MUC1 expression is very common in pancreatobiliary type, seldom identified in gastric or intestinal types
-
♦
MUC6 is mostly seen in oncocytic and, to a lesser degree, in pancreatobiliary types
Differential Diagnosis
-
♦
Mucinous cystic neoplasms
-
Perimenopausal females
-
Tail of the pancreas
-
Thick-walled cyst
-
No communication with the ducts
-
Ovarian-type stroma (most helpful)
-
-
♦
Intraductal oncocytic papillary neoplasms
-
Complex papillae, intraepithelial lumina, oncocytic cells
-
-
♦
Invasive ductal carcinoma
-
Irregular clustering and haphazard distribution
-
Contour irregularities
-
Small units with round, open lumina
-
Perineurial invasion
-
-
♦
Pancreatic intraepithelial neoplasia
-
Microscopic/incidental (not mass forming)
-
Simple mucosal folds or at most, short papillae
-
Lack MUC2
-
Intraductal Tubulopapillary Neoplasms
Definition and Classification
-
♦
Cystic epithelial neoplasm that grows within the pancreatic ducts and is composed of back-to-back tubular units
-
♦
Common expression of MUC6, in the absence of MUC5AC, raises the possibility of pyloric differentiation
-
♦
Many show marked atypia, high mitotic count, and necrosis and classified as intraductal tubular neoplasm with high-grade dysplasia
-
♦
Data on the prognosis is limited in the literature: Despite the histologic indicators of a high-grade malignancy (atypia, mitosis, and necrosis), overall outcome appears relatively favorable if lacking an invasive component
-
♦
Approximately one third have foci of invasion ranging from microscopic to larger foci
Mucinous Cystic Neoplasms (Table 43.2 )
Clinical
-
♦
Almost exclusively in perimenopausal females (mean age 48, 97% females)
-
♦
Graded as MCN, low-grade and MCN, high-grade (CIS) based on the cytoarchitectural atypia (per Baltimore consensus, December 2015)
-
♦
Recent studies confirm that grade accurately predicts the outcome, but (only) if the tumor is sampled/examined thoroughly
Macroscopic
-
♦
Large (average size = 7–10 cm), multilocular, thick-walled cyst (Fig. 43.26)
Fig. 43.26. 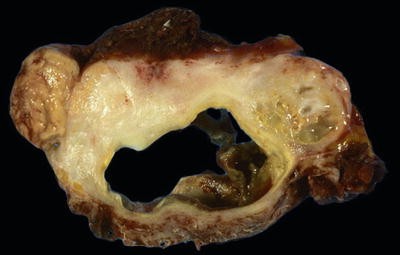
Mucinous cystic neoplasm typically forms a thick-walled, multilocular cyst in the tail of the pancreas.
-
♦
Typically in the body or tail
-
♦
Do not communicate with the ducts
-
♦
Thick mucinous content
-
♦
May become purulent
-
♦
Areas of carcinoma often not evident macroscopically

Microscopic
-
♦
Ovarian-type stroma is diagnostic, specific, and almost a prerequisite (Fig. 43.27)
Fig. 43.27. 
Ovarian-type stroma is pathognomonic for mucinous cystic neoplasms.
-
Identical to ovarian stroma morphologically and immunophenotypically
-
May contain sclerotic foci, hypervascularity, and rarely even luteal cells
-
-
♦
Mucinous or nonmucinous lining with varying degrees of atypia (see below)
-
♦
Abrupt transition from areas with low-grade dysplasia to frank high-grade dysplasia (CIS) is common (Fig. 43.28)
Fig. 43.28. 
Mucinous cystic neoplasm with high-grade dysplasia. The epithelium shows abrupt transition from areas of low-grade dysplasia to those with frank high-grade dysplasia (carcinoma in situ).
-
♦
Scattered goblet and neuroendocrine cells
-
♦
Papillae may be seen, forming large nodules in some cases


Classification/Grading
-
♦
The neoplasm is graded based on the highest degree of dysplasia identified, not the average
-
♦
Grading is valid only if the tumor is thoroughly examined
-
♦
Low-grade dysplasia: tall columnar mucinous cells with abundant apical mucin and well-polarized, uniform small nuclei without atypia or with mild/moderate atypia
-
♦
High-grade dysplasia (carcinoma in situ): severe cytologic or architectural atypia (florid papillary nodules) with cuboidal nuclei, prominent nucleoli, mitotic figures, tufts, and necrosis
-
♦
Invasive carcinoma arising in association with MCN is seen in 16% and tends to occur more commonly in larger tumors (>4 cm) and complex and large intracystic papillary nodules
-
♦
Invasive carcinoma is almost exclusively of tubular type with all the morphologic features of invasive ductal adenocarcinoma (see section on ductal adenocarcinoma)
Immunohistochemistry
-
♦
Ductal lineage markers, positive (Table 43.1)
-
♦
Progesterone receptors + in ovarian-type stroma
Differential Diagnosis
-
♦
Intraductal papillary mucinous neoplasms
-
Intraductal (communication with the native ducts demonstrable radiologically or on gross examination)
-
Intestinal-type papillae may be seen
-
More common in the head
-
More common in elderly males
-
-
♦
Intraductal oncocytic papillary neoplasms
-
Complex papillae, intraepithelial lumina, oncocytic cells
-
-
♦
Pseudocyst
-
No epithelial lining
-
Granulation-type tissue (but not ovarian-type stroma)
-
Fat necrosis
-
Serous Cystic Neoplasms
Synonyms
-
♦
Glycogen-rich adenoma, microcystic serous cystadenoma
Clinical
-
♦
More common in females (M/F = 1/3, mean age 58)
-
♦
Present with nonspecific symptoms or detected incidentally
-
♦
Have well-established association with von Hippel-Lindau (VHL) syndrome
-
♦
Cyst fluid analysis does not show oncoproteins seen in mucinous tumors (CEA, CA19-9, and others)
-
♦
Almost exclusively benign, very rare (questionable) examples of a malignant counterpart
Macroscopic (Fig. 43.29)
-
♦
Mean size = 4 cm (may become very large, up to 30 cm)
-
♦
Well-demarcated, spongelike appearance is diagnostic
-
♦
Central stellate scar is common
-
♦
Characteristic microcystic pattern with innumerable small cysts, each measuring a few millimeters
Microscopic (Fig. 43.30)
-
♦
Conglomerate of innumerable tubules and cysts
-
♦
Simple cuboidal epithelium
-
♦
Clear (glycogen-rich) cells with distinct cytoplasmic borders
-
♦
Small, round nuclei with dense, homogenous chromatin
-
♦
The tumor cells are intimately admixed with prominent capillary network akin to other clear cell tumors also associated with VHL syndrome

Serous cystadenoma. Microcystic pattern (innumerable small cysts most of which are smaller than a few millimeters) creating a spongelike appearance is diagnostic. A stellate scar is commonly present. These tumors may become very large.

Serous cystadenoma is characterized by innumerable, tightly packed tubular elements that are lined by glycogen-rich cells that show distinct cytoplasmic borders and small, round, uniform nuclei with dense, homogenous chromatin.
Variants
-
♦
Oligocystic variant
-
Smaller number of larger cysts
-
No apparent biologic differences form the microcystic type
-
-
♦
Solid variant
-
Packed with small gland-like units without cystic transformation
-
Very uncommon
-
Immunohistochemistry
-
♦
Epithelial differentiation markers +
-
♦
Virtually the only ductal tumor that does not show the “pancreatic ductal” differentiation markers (mucins, mucin-related oncoproteins, KRAS mutation)
-
♦
Clear cell tumorigenesis markers including glucose uptake and transporter-1 (GLUT1), HIF1A, carbonic anhydrase IX (CAIX), and vascular endothelial growth factor (VEGF) +
-
♦
Diffuse and strong positivity for AE1/AE3, inhibin–, and GLUT-1 is fairly distinctive, especially on core biopsies and fine-needle aspirates
-
♦
Chromosome 10q and VHL gene alterations in a subset (40%)
Differential Diagnosis
-
♦
Polycystic disease and VHL
-
Individual cysts indistinguishable from serous tumors
-
More widely spread in the pancreas
-
Often multifocal
-
Association with cysts in other organs
-
-
♦
Megacystic tumors (for the rare oligocystic variant)
-
Corresponding patterns in the epithelial lining (see corresponding sections in ductal neoplasia and miscellaneous cysts sections)
-
Acinar Cell Neoplasia
Acinar Cell Carcinoma
Clinical
-
♦
Uncommon, <1% of pancreatic neoplasia
-
♦
Mean age 60
-
♦
Rarely in children
-
♦
Lipase hypersecretion syndrome (subcutaneous fat necrosis, polyarthralgia, and polyarthritis) in 10%
-
♦
50% with metastasis (usually to liver) at diagnosis
-
♦
5-year survival, 30%; recent studies suggesting better overall prognosis
Macroscopic
-
♦
Typically large (>5 cm)
-
♦
Well-delineated, nodular, fleshy (soft yellow-tan) mass with fibrous bands and frequent necrosis
-
♦
Focal degenerative cystic changes may occur
Microscopic (Fig. 43.31)
-
♦
Sheetlike, stroma-poor growth pattern
-
♦
Overall basophilia
-
♦
Round nuclei with prominent nucleoli
-
♦
May contain cytoplasmic granules (sometimes acidophilic)
-
♦
Rosette-like acinar formations may be seen
-
♦
If trabecular pattern, the cells palisade on the adjacent fibrovascular stroma
-
♦
Variable amounts of neuroendocrine elements are quite common. If the neuroendocrine component is larger than 25% of the tumor, by convention, the case is classified as “mixed”
-
♦
Ultrastructurally, electron dense large granules typical of zymogenic granules
Histochemistry/Immunohistochemistry (Tables 43.1 and 43.3)
-
♦
PAS-positive diastase-resistant granules
-
♦
Immunoreactivity with epithelial and enzymatic markers (trypsin most reliable, but also chymotrypsin and lipases)
-
♦
Lack of ductal differentiation markers (mucin and mucin-related oncoproteins)

Acinar cell carcinomas form sheets of round cells with prominent nucleoli. In some cases such as this one, abortive acinar formations resembling rosettes may be seen.
Variants
-
♦
Rare intraductal and cystic variants
-
♦
Mixed acinar-neuroendocrine carcinomas
Differential Diagnosis
-
♦
Neuroendocrine neoplasia
-
Nested or trabecular pattern
-
Lack of overall basophilia
-
Neuroendocrine chromatin, nucleoli not too prominent
-
Diffuse and strong reactivity for the neuroendocrine markers (chromogranin and synaptophysin)
-
-
♦
Solid pseudopapillary neoplasm
-
Almost exclusively in young females (mean age 30)
-
Solid and pseudopapillary patterns, may have myoid stroma
-
Round to ovoid bland-appearing nuclei with small (if at all visible) nucleoli, nuclear grooves
-
Degenerative changes including zones of macrophages and hyaline globules
-
Lack of specific acinar markers (trypsin, chymotrypsin)
-
-
♦
Pancreatoblastoma
-
Ductal and neuroendocrine components (in addition to acinar, which is most common)
-
Squamoid corpuscles
-
-
♦
Ductal adenocarcinoma
-
Scirrhous pattern (firm, ill-defined, scar-like appearance)
-
Often primary tumor is <5 cm at the time of diagnosis
-
Tubular units within desmoplastic stroma
-
Acinar Cell Cystadenoma
-
♦
Also called “acinar cystic transformation”
-
♦
Very uncommon
-
♦
Usually microscopic, rarely becomes several centimeters
Neuroendocrine Neoplasia
Classification
-
♦
The current grading scheme employed by the WHO 2010 is based on two calculations:
-
(1)
Ki67 labeling index (using the MIB1 antibody) and (2) mitotic count:
-
•
G1 neuroendocrine tumors are defined as having a Ki67 labeling index of <3% and <2 mitoses/10 high-power fields (HPF) or 2 mm2
-
•
G2 neuroendocrine tumors are defined as having a Ki67 labeling index of 3–20% or 2–20 mitoses/10 HPFs
-
•
G3 neuroendocrine carcinomas are defined as having a Ki67 labeling index of >20% and >20 mitoses/10 HPFs
-
(1)
Well-Differentiated Pancreatic Neuroendocrine Tumors (PanNETs)
♦ May be WHO G1, G2, or G3 (preliminary data suggest that if it is G3, Ki67 labeling index is usually <50%)
Clinical
-
♦
May be functional (50%) or present as a mass without hormone activity (nonfunctioning)
-
♦
Some are associated with MEN1 or other syndromes
-
♦
MEN-associated examples tend to be multiple and less aggressive
-
♦
Most insulinomas follow a benign course, possibly because they are typically functional from the beginning, and are detected and removed when very small
Macroscopic
-
♦
Generally well delineated with partial to complete encapsulation
-
♦
Fleshy (tan, soft, homogenous)
Microscopic (Fig. 43.32)
-
♦
Nested, gyriform (trabecular), acinar, and even gland-like or solid-appearing patterns
-
♦
Uniform cells with fair amount of acidophilic cytoplasm
-
♦
Round, centrally located nuclei with distinctive stippled (“salt and pepper”) chromatin
-
♦
Nucleoli may be present but not prominent
-
♦
Scattered atypical cells (“neuroendocrine atypia”) may be seen
-
♦
Ultrastructurally, membrane-bound neurosecretory granules are typical; some hormones, especially insulin, have distinctive appearance

Well-differentiated pancreatic neuroendocrine tumors are characterized by sheets of round, uniform cells forming nests that are separated by delicate fibrovascular stroma.
Immunohistochemistry (Tables 43.1 and 43.3)
-
♦
Epithelial markers+, neuroendocrine markers [chromogranin, synaptophysin, CD56] +
-
♦
Hormone markers (insulin, glucagon, somatostatin, gastrin, vasoactive intestinal polypeptide, and pancreatic polypeptide) may be positive
-
♦
However, hormone immunochemistry in the tumor does not correlate with the “functionality” status
Variants
-
♦
Cystic: 5% of PanNETs result from a degenerative process
-
♦
Clear cell may mimic renal cell carcinomas, often associated with von Hippel-Lindau
-
♦
Pleomorphic, degenerative neuroendocrine atypia is more pronounced than usual in which many of the nuclei are enlarged and have smudgy, dense chromatin and irregular contours
-
♦
Lipid-rich, microvesicular, foamy cytoplasm creates a picture indistinguishable from adrenocortical cells
-
♦
Signet ringlike or rhabdoid, homogenous cytoplasmic contents that push the nucleus to the periphery of the cell
-
♦
Paraganglioma-like, nested pattern in which cells form smaller clusters surrounded by stromal cells resembling sustentacular cells
Differential Diagnosis
-
♦
“Hyperplastic islets” (nonneoplastic islets in chronic pancreatitis)
-
Cord-like pseudoinfiltrative pattern or micronodules
-
In the background of other pathologic changes
-
Hormone immunohistoprofile is similar to that of normal islets (the presence of multiple hormones and their spatial distribution)
-
-
♦
Acinar cell carcinoma
-
Overall basophilia, prominence of nucleoli, nesting not prominent
-
Immunoreactivity with enzymes (trypsin), hromogranin
-
-
♦
Solid pseudopapillary neoplasm
-
More ovoid cells with overlapping of nuclei; nesting is vague
-
Pseudopapillary pattern, nuclear grooves, hyaline globules, and zones of macrophages
-
Chromogranin and keratin may be focal or weak
-
Poorly Differentiated Neuroendocrine (Small Cell or Large Cell Type) Carcinoma
-
♦
By definition, WHO 2010 G3 (preliminary data suggest that Ki67 labeling index is usually >50%)
-
♦
Most poorly differentiated neuroendocrine carcinomas in the pancreas are metastasis from other organs
-
♦
Primary poorly differentiated neuroendocrine carcinomas are exceedingly uncommon
-
♦
Usually present with metastasis to liver
-
♦
Rapidly fatal
-
♦
Pathologically similar to their pulmonary counterparts and could be small cell (Fig. 43.33) or large cell type
Fig. 43.33. 
Poorly differentiated neuroendocrine carcinoma, small cell type, of the pancreas.
-
♦
Necrosis, abundant mitotic activity, and high (usually >50%) Ki67 labeling index are characteristic

Solid Pseudopapillary Neoplasm
Clinical
-
♦
Uncommon, 1–2% of pancreatic tumors
-
♦
Origin undetermined
-
♦
Almost exclusively in young females (mean age 33); other tumors, in particular neuroendocrine neoplasia, to be ruled out if in a male
-
♦
Indolent (low-grade) neoplasm
-
Complete removal = 85% cure rate
-
Metastasis, if occurs, is usually to the liver or peritoneum and is often present at the time of diagnosis
-
Even patients with metastases may have a protracted clinical course
-
Almost never fatal
-
-
♦
No reliable criteria to distinguish metastatic cases
Macroscopic
-
♦
Round and deceptively well demarcated (satellites and projections are common under microscopy)
-
♦
Commonly cystic and hemorrhagic with scattered fleshy tan foci of viable tumor
-
♦
Average size = 7 cm
Microscopic (Fig. 43.34)
-
♦
Solid areas with sheets of neoplastic cells punctuated by fibrotic and/or myoid stroma
-
♦
Calcifications and psammoma bodies may be seen
-
♦
Ependymoma-like pseudopapillary pattern, presumably related to the alterations in cell adhesion molecules such as E-cadherin, culminating in distinctive dyscohesiveness of the cells away from the microvasculature
-
♦
Round to ovoid, cytologically bland nuclei with small (if at all visible) nucleoli, overlapping of nuclei, nuclear grooves
-
♦
Hyaline globules and zones of foamy macrophages in the more degenerated areas
-
♦
Satellites and projections to adjacent pancreas; entrapped pancreatic elements within the main lesion

Solid pseudopapillary neoplasm. Ependymoma-like pseudopapillary pattern is characteristic. The nuclei are round to ovoid.
Variants
-
♦
Some have spindle cell areas resembling hemangiopericytomas
-
♦
Scattered or clusters of pleomorphic giant cells might be present
Immunohistochemistry (Tables 43.1 and 43.3)
-
♦
Diffuse and consistent immunoreactivity for β-catenin (abnormal cytoplasmic and/or nuclear), progesterone receptors, and CD10
-
♦
So-called neuroendocrine markers NSE, synaptophysin, and CD56 are consistently positive; however, chromogranin is mostly negative or very focal/weak positive
-
♦
Inhibin and estrogen receptors are less consistent; keratins may be focal or weak
-
♦
Wnt signaling pathway alterations with abnormal nuclear accumulation of β-catenin, overexpression of cyclin D1, and loss of E-cadherin membranous expression with/without relocalization to nucleus
Differential Diagnosis
-
♦
Pseudocyst
-
No epithelial lining (may require extensive sampling to prove)
-
-
♦
Pancreatic neuroendocrine tumors
-
♦
Nested pattern prominent; neuroendocrine chromatin; more uniform, round cells; less overlapping; keratin and chromogranin+, β-catenin NOT abnormal
-
♦
Acinar cell carcinoma
-
Overall basophilia, prominent nucleoli, PAS+ acidophilic granules
-
Immunoreactivity for acinar enzymes
-
-
♦
Pancreatoblastoma
-
Squamoid corpuscles
-
Ductal, neuroendocrine, and acinar differentiation (Table 43.1)
-
Childhood tumor
-
Pancreatoblastoma
Clinical
-
♦
Extremely rare
-
♦
Early childhood tumor (mean age 4), second peak in 30s
-
♦
Two-thirds described in Asians
-
♦
Elevated alpha-fetoprotein in some cases
-
♦
Occasionally seen in Beckwith-Wiedemann and FAP syndromes
-
♦
5-year survival, 25%
Macroscopic
-
♦
Well-demarcated, solitary, solid, multilobulated, encapsulated tumor; yellow-tan cut surface
-
♦
Typical size = 7–18 cm
Microscopic (Fig. 43.35)
-
♦
Cellular, stroma-poor neoplasm
-
♦
Multiphenotypic differentiation with a mixture of acinar (most consistent), ductal, and neuroendocrine elements
-
♦
Typically, round nondescript cells with moderate amount of cytoplasm predominate
-
♦
Squamoid corpuscles (small, distinct “morule”-like formations with meningothelial appearance, including nuclear pseudoinclusions)
-
♦
Necrosis may be seen

Pancreatoblastoma. Diffuse sheets of relatively uniform cells with distinct foci of ductal, acinar, and endocrine differentiation. Morule-like formations referred to as squamoid corpuscles are diagnostic.
Immunohistochemistry (Tables 43.1 and 43.3)
-
♦
Acinar, ductal, and neuroendocrine components show corresponding staining patterns
-
♦
APC/β-catenin pathway and chromosome 11p alterations
-
♦
Abnormal (nuclear/cytoplasmic) immunolabeling for β-catenin and overexpression of cyclin D1, more strikingly in squamoid corpuscles
Differential Diagnosis
-
♦
Acinar cell carcinoma
-
Absence of squamoid corpuscles
-
-
♦
Neuroendocrine neoplasia
-
Adults
-
Absence of squamoid corpuscles and other lineage elements
-
-
♦
Solid pseudopapillary neoplasm
-
Pseudopapillary (ependymoma-like) pattern, zones of macrophages, hyaline globules
-
Nuclear grooves
-
Absence of squamoid corpuscles
-
Mixed Carcinomas (Mixed Acinar-Neuroendocrine and Mixed Acinar-Ductal)
-
♦
Extremely uncommon
-
♦
Arbitrarily defined as carcinomas with a second component constituting >30% of the tumor
-
♦
Pitfall: scattered neuroendocrine cells are common in other neoplasia
-
♦
Behavior along the more aggressive component (see the corresponding sections)
Miscellaneous Cystic Lesions
Lymphoepithelial Cyst
Clinical
-
♦
Peripancreatic
-
♦
Adult men (M/F = 3/1, mean age 52)
-
♦
No association with any syndromes
-
♦
No association with malignancy
Microscopic (Fig. 43.36)
-
♦
Epidermal-lined cyst with variable keratinization
-
♦
Some with transitional or attenuated lining
-
♦
Rarely, goblet cells or scanty sebaceous elements
-
♦
A distinct band of lymphoid tissue composed of mature T lymphocytes surrounds the epithelium
-
♦
Lymphoid tissue may have lymph node architecture (germinal centers, sinusoids, capsule, and subcapsular sinus)
-
♦
Granulomas, cholesterol clefts, and solid epithelial cell nests may be seen

Lymphoepithelial cyst is characterized by epidermal-lined cyst surrounded by a distinct band of lymphoid tissue.
Squamoid Cyst of Pancreatic Ducts
-
♦
Small, unilocular cysts (median size = 1.5 cm)
-
♦
Some are large and might undergo resection with the clinical impression of being an IPMN
-
♦
Have variable lining ranging from attenuated, nonstratified squamous to transitional to stratified squamous epithelium
-
♦
Contain distinctive mucoproteinaceous acidophilic acinar secretions forming concretions
-
♦
The wall is composed of a thin band of fibrous tissue devoid of any lymphoid tissue
-
♦
Nuclear p63 expression confirms the squamous/transitional nature of the epithelial lining
Epidermoid Cyst within Intrapancreatic Accessory Spleen
-
♦
Very rare
-
♦
Young patients (mean age 37)
-
♦
Typically in the tail of the pancreas
-
♦
Attenuated keratinizing squamous epithelium, surrounded by unremarkable splenic tissue
Lymphangioma
-
♦
Young females (M/F = 1/3, mean age 29)
-
♦
Endothelial-lined cysts (CD31, CD34, factor VIII+)
-
♦
Lymphoid tissue
Miscellaneous Tumors
Secondary Tumors
-
♦
Direct spread from ampullary, duodenal, and biliary tumors
-
May be morphologically identical
-
Location is determined by gross examination
-
Preinvasive neoplasia in the corresponding sites
-
-
♦
Metastasis to pancreas is rare
-
Lung and GI tumors are the most common at autopsy
-
Renal cell carcinomas and melanomas may be mistaken clinically as a primary
-
Should be considered in the differential diagnosis if a pattern not described for the primary tumors is encountered
-
Mesenchymal Tumors
-
♦
Most are secondary from neighboring sites (GISTs or retroperitoneal tumors)
-
♦
Primary ones are very rare
-
♦
Some, especially schwannomas, may be cystic
-
♦
Small blue cell tumors of childhood including primitive neuroectodermal tumors and desmoplastic small round cell tumors may also occur in the pancreas
Hematopoietic Tumors
-
♦
Very uncommon
-
♦
Virtually every hematopoietic tumor type may present as a primary mass in the pancreas including B cell, T cell, Hodgkin, and myeloma
Reporting of Pancreatic Neoplasia
-
♦
Contents of the specimen
-
♦
Type of operation
-
Pancreatoduodenectomy is the preferred term over Whipple (since most current operations are not the original Whipple operation)
-
Distal pancreatectomy (with or without splenectomy)
-
-
♦
Origin/location of the tumor (mostly based on gross examination and clinical findings)
-
Pancreatic vs. periampullary (nonspecific), ampullary, common bile duct, duodenal, or peripancreatic
-
-
♦
Type of the tumor
-
Pancreatobiliary vs. adenosquamous, colloid, medullary, intestinal, etc
-
Invasive and preinvasive (noninvasive) components reported separately
-
Generic diagnoses such as “mucinous carcinoma” should be further specified
-
-
♦
Size of the tumor
-
Size of invasive and noninvasive components reported separately
-
An estimated size, based on the correlation of gross and microscopic findings, is necessary in many cases
-
-
♦
Distribution of the tumor
-
Specify involvement of organs (ampulla, CBD, duodenum, etc.)
-
-
♦
Preinvasive neoplasia
-
Even if associated with invasive carcinoma, the features of intraductal neoplasia, mucinous cystic neoplasia, etc., should be duly noted
-
-
♦
Vascular and perineurial invasion
-
Some authors use perineurial invasion as an additional “soft” criteria for inclusion into radiotherapy protocols
-
-
♦
Lymph nodes
-
An average of 12 lymph nodes is identifiable in a typical pancreatoduodenectomy specimen; most are embedded on the surfaces of the pancreatic head and pancreatoduodenal groove
-
-
♦
Margins
-
In a right-sided (pancreatoduodenectomy) specimen:
-
Retroperitoneal (uncinate, posterior/inferior), pancreatic duct (neck), common bile duct, and gastrointestinal mucosal margins
-
Retroperitoneal (uncinate, posterior/inferior) margin is the most important. If sampled like the prostatic apex (removed as a 3–4 mm slice, serially sectioned, and submitted entirely as perpendicular margin), this margin proves positive in 50–85% of the cases with ductal carcinoma. This area also contains lymph nodes
-
Posterior and anterior free surfaces are reported separately as “surfaces” by some and as “margins” by others
-
-
In a left-sided (distal) pancreatectomy:
-
Pancreatic ductal margin, anterior surface, posterior surface, and perisplenic soft tissue surface
-
-
-
♦
Uninvolved segments of organs
-
Uninvolved pancreas (for PanINs, other precursor lesions, pancreatitis, etc.), as well as uninvolved CBD, gastrointestinal, gallbladder, and spleen
-
-
♦
Surgical hardware, especially stents
TNM Classification of Pancreatic Tumors (AJCC 2010)
♦ Primary Tumor (T)
-
TX Primary tumor cannot be assessed
-
T0 No evidence of primary tumor
-
Tis Carcinoma in situFootnote 1
-
T1 Tumor limited to the pancreas, ≤2 cm in greatest dimension
-
T2 Tumor limited to the pancreas, >2 cm in greatest dimension
-
T3 Tumor extends beyond the pancreas but without involvement of the celiac axis or the superior mesenteric artery
-
T4 Tumor involves the celiac axis or the superior mesenteric artery (unresectable primary tumor)
♦ Regional Lymph Nodes (N)
-
NX Regional lymph nodes cannot be assessed
-
N0 No regional lymph node metastasis
-
N1 Regional lymph node metastasis
♦ Distant Metastasis (M)
-
MX Distant metastasis cannot be assessed
-
M0 No distant metastasis
-
M1 Distant metastasis
Notes
- 1.
This also includes PanIN III classification
Suggested Reading
Adsay NV. The “new kid on the block”: intraductal papillary mucinous neoplasms of the pancreas: current concepts and controversies. Surgery. 2003;133:459–63.
Adsay NV. Cystic lesions of the pancreas. Mod Pathol. 2007;20:71–93.
Adsay NV, Zamboni G. Paraduodenal pancreatitis: a clinico-pathologically distinct entity unifying “cystic dystrophy of heterotopic pancreas”, “para-duodenal wall cyst”, and “groove pancreatitis”. Semin Diagn Pathol. 2004;21:247–54.
Adsay NV, Adair CF, Heffess CS, et al. Intraductal oncocytic papillary neoplasms of the pancreas. Am J Surg Pathol. 1996;20:980–94.
Adsay NV, Longnecker DS, Klimstra DS. Pancreatic tumors with cystic dilatation of the ducts: intraductal papillary mucinous neoplasms and intraductal oncocytic papillary neoplasms. Semin Diagn Pathol. 2000;17:16–30.
Adsay NV, Pierson C, Sarkar F, et al. Colloid (mucinous noncystic) carcinoma of the pancreas. Am J Surg Pathol. 2001;25:26–42.
Adsay NV, Hasteh F, Cheng JD, et al. Lymphoepithelial cysts of the pancreas: a report of 12 cases and a review of the literature. Mod Pathol. 2002;15:492–501.
Adsay V, Andea A, Kilinc N, et al. Secondary tumors of the pancreas: an analysis of a large surgical and autopsy database and review of the literature. Virchows Arch. 2004a;444:527–35.
Adsay NV, Merati K, Basturk O, et al. Pathologically and biologically distinct types of epithelium in intraductal papillary mucinous neoplasms: delineation of an “intestinal” pathway of carcinogenesis in the pancreas. Am J Surg Pathol. 2004b;28:839–48.
Adsay NV, Basturk O, Klimstra DS, et al. Pancreatic Pseudotumors: non-neoplastic solid lesions of the pancreas that clinically mimic pancreas cancer. Semin Diagn Pathol. 2004c;21:260–7.
Adsay NV, Basturk O, Thirabanjasak D. Diagnostic features and differential diagnosis of autoimmune pancreatitis. Semin Diagn Pathol. 2005;22:309–17.
Adsay NV, Basturk O, Saka B, et al. Whipple made simple for surgical pathologists: orientation, dissection, and sampling of pancreaticoduodenectomy specimens for a more practical and accurate evaluation of pancreatic, distal common bile duct, and ampullary tumors. Am J Surg Pathol. 2014;38:480–93.
Adsay V, Mari Mino-Kenudson M, Furukawa T, et al. Pathologic evaluation and reporting of intraductal papillary mucinous neoplasms (IPMNS) of the pancreas and other tumoral intraepithelial neoplasms of pancreatobiliary tract: recommendations of Verona Consensus Meeting. Ann Surg. 2015 (Epub ahead of print).
Andea A, Sarkar F, Adsay VN. Clinicopathological correlates of pancreatic intraepithelial neoplasia: a comparative analysis of 82 cases with and 152 cases without pancreatic ductal adenocarcinoma. Mod Pathol. 2003;16:996–1006.
Basturk O, Adsay NV. Pancreas pathology. In: Lefkowitch J, editor. Lefkowitch’s anatomic pathology board review. 2nd ed. Elsevier; 2015.
Basturk O, Yang Z, Tang LH, et al. The high-grade (WHO G3) pancreatic neuroendocrine tumor category is morphologically and biologically heterogenous and includes both well differentiated and poorly differentiated neoplasms. Am J Surg Pathol. 2015;39:683–90.
Basturk O, Zamboni G, Klimstra D, et al. Intraductal and papillary variants of acinar cell carcinomas: a new addition to the challenging differential diagnosis of intraductal neoplasms. Am J Surg Pathol. 2007;31:363–70.
Basturk O, Coban I, Adsay NV. Cystic neoplasms of the pancreas. Arch Pathol Lab Med. 2009;133:423–38.
Basturk O, Tang L, Hruban RH, et al. Poorly differentiated neuroendocrine carcinomas of the pancreas: a clinicopathologic analysis of 44 cases. Am J Surg Pathol. 2014;38:437–47.
Basturk O, Hong SM, Wood LD, et al. A revised classification system and recommendations from the Baltimore Consensus Meeting for Neoplastic Precursor Lesions in the Pancreas. Am J Surg Pathol. 2015;39:1730–41.
Chetty R, Serra S. Membrane loss and aberrant nuclear localization of E-cadherin are consistent features of solid pseudopapillary tumour of the pancreas. An immunohistochemical study using two antibodies recognizing different domains of the E-cadherin molecule. Histopathology. 2008;52:325–30.
Chetty R, Serra S, Asa SL. Loss of membrane localization and aberrant nuclear E-cadherin expression correlates with invasion in pancreatic endocrine tumors. Am J Surg Pathol. 2008;32:413–9.
Compton CC. Serous cystic tumors of the pancreas. Semin Diagn Pathol. 2000;17:43–56.
Deshpande V, Fernandez-del Castillo C, Muzikansky A, et al. Cytokeratin 19 is a powerful predictor of survival in pancreatic endocrine tumors. Am J Surg Pathol. 2004;28:1145–53.
Deshpande V, Mino-Kenudson M, Brugge W, et al. Autoimmune pancreatitis: more than just a pancreatic disease? A contemporary review of its pathology. Arch Pathol Lab Med. 2005;129:1148–54.
Estrella JS, Li L, Rashid A, et al. Solid pseudopapillary neoplasm of the pancreas: clinicopathologic and survival analyses of 64 cases from a single institution. Am J Surg Pathol. 2014;38:147–57.
Goossens A, Gepts W, Saudubray JM, et al. Diffuse and focal nesidioblastosis. A clinicopathological study of 24 patients with persistent neonatal hyperinsulinemic hypoglycemia. Am J Surg Pathol. 1989;13:766–75.
Hochwald SN, Zee S, Conlon KC, et al. Prognostic factors in pancreatic endocrine neoplasms: an analysis of 136 cases with a proposal for low grade and intermediate-grade groups. J Clin Oncol. 2002;20:2633–42.
Holen KD, Klimstra DS, Hummer A, et al. Clinical characteristics and outcomes from an institutional series of acinar cell carcinoma of the pancreas and related tumors. J Clin Oncol. 2002;20:4673–8.
Hruban RH, Adsay NV. Molecular classification of neoplasms of the pancreas. Hum Pathol. 2009;40:612–23.
Hruban RH, Adsay NV, Albores-Saavedra J, et al. Pancreatic intraepithelial neoplasia: a new nomenclature and classification system for pancreatic duct lesions. Am J Surg Pathol. 2001;25:579–86.
Hruban RH, Takaori K, Klimstra DS, et al. An illustrated consensus on the classification of pancreatic intraepithelial neoplasia and intraductal papillary mucinous neoplasms. Am J Surg Pathol. 2004;28:977–87.
Hruban RH, Pitman MB, Klimstra DS. Tumors of the pancreas. In: AFIP atlas of tumor pathology series. Washington, DC; 2007.
Jang KT, Park SM, Basturk O, et al. Clinicopathologic characteristics of 29 invasive carcinomas arising in 178 pancreatic mucinous cystic neoplasms with ovarian-type stroma: implications for management and prognosis. Am J Surg Pathol. 2015;39:179–87.
Kardon DE, Thompson LD, Przygodzki RM, et al. Adenosquamous carcinoma of the pancreas: a clinicopathologic series of 25 cases. Mod Pathol. 2001;14:443–51.
Kim MJ, Jang SJ, Yu E. Loss of E-cadherin and cytoplasmic-nuclear expression of beta-catenin are the most useful immunoprofiles in the diagnosis of solid-pseudopapillary neoplasm of the pancreas. Hum Pathol. 2008;39:251–8.
Klimstra DS. Nonductal neoplasms of the pancreas. Mod Pathol. 2007;20:S94–112.
Klimstra DS, Adsay NV. Lymphoplasmacytic sclerosing (autoimmune) pancreatitis. Semin Diagn Pathol. 2004;21:237–46.
Klimstra DS, Heffess CS, Oertel JE, et al. Acinar cell carcinoma of the pancreas. A clinicopathologic study of 28 cases. Am J Surg Pathol. 1992;16:815–37.
Klimstra DS, Rosai J, Heffess CS. Mixed acinar-endocrine carcinomas of the pancreas. Am J Surg Pathol. 1994;18:765–78.
Klimstra DS, Wenig BM, Adair CF, et al. Pancreatoblastoma. A clinicopathologic study and review of the literature. Am J Surg Pathol. 1995;19:1371–89.
Klimstra DS, Wenig BM, Heffess CS. Solid-pseudopapillary tumor of the pancreas: a typically cystic tumor of low malignant potential. Semin Diagn Pathol. 2000;17:66–81.
Klimstra DS, Adsay NV, Dhall D, et al. Intraductal tubular carcinoma of the pancreas: clinicopathologic and immunohistochemical analysis of 18 cases (abstract). Mod Pathol. 2007;20:285A.
Klimstra DS, Adsay NV. Tumors of the pancreas. In: Odze RD, Goldblum JR, editors. Surgical pathology of the GI tract, liver, biliary tract, and pancreas. 3rd ed. Elsevier; 2014.
Klöppel G. Pseudocysts and other non-neoplastic cysts of the pancreas. Semin Diagn Pathol. 2000;17:1–7.
Klöppel G, Adsay NV. Chronic pancreatitis and the differential diagnosis versus pancreatic cancer. Arch Pathol Lab Med. 2009;133:382–7.
Klöppel G, Heitz PU. Pancreatic endocrine tumors. Pathol Res Pract. 1988;183:155–68.
Klöppel G, Lüttges J. WHO-classification 2000: exocrine pancreatic tumors. Verh Dtsch Ges Pathol. 2001;85:219–28.
Klöppel G, Lüttges J, Sipos B, et al. Autoimmune pancreatitis: pathological findings. JOP. 2005;6:97–101.
Klöppel G, Sipos B, Zamboni G, et al. Autoimmune pancreatitis: histo- and immunopathological features. J Gastroenterol. 2007;42:28–31.
Klöppel G, Basturk O, Schlitter AM, et al. Intraductal neoplasms of the pancreas. Semin Diagn Pathol. 2014;31:452–66.
La Rosa S, Adsay V, Albarello L, et al. Clinicopathologic study of 62 acinar cell carcinomas of the pancreas: insights into the morphology and immunophenotype and search for prognostic markers. Am J Surg Pathol. 2012;36:1782–95.
Longnecker DS, Adsay NV, Fernandez-del Castillo C, et al. Histopathological diagnosis of pancreatic intraepithelial neoplasia and intraductal papillary-mucinous neoplasms: interobserver agreement. Pancreas. 2005;31:344–9.
Ohike N, Kosmahl M, Klöppel G. Mixed acinar-endocrine carcinoma of the pancreas. A clinicopathological study and comparison with acinar-cell carcinoma. Virchows Arch. 2004;445:231–5.
Othman M, Basturk O, Groisman G, et al. Squamoid cyst of pancreatic ducts: a distinct type of cystic lesion in the pancreas. Am J Surg Pathol. 2007;31:291–7.
Paal E, Thompson LD, Heffess CS. A clinicopathologic and immunohistochemical study of ten pancreatic lymphangiomas and a review of the literature. Cancer. 1998;82:2150–8.
Paal E, Thompson LD, Frommelt RA, et al. A clinicopathologic and immunohistochemical study of 35 anaplastic carcinomas of the pancreas with a review of the literature. Ann Diagn Pathol. 2001;5:129–40.
Reid MD, Choi H, Memis B, et al. Serous neoplasms of the pancreas: a clinicopathologic analysis of 232 cases and literature review with new insights on oligocystic and solid variants and critical reappraisal of so-called “serous cystadenocarcinoma”. Am J Surg Pathol. 2015;39:1597–610.
Reid MD, Choi H, Balci S, et al. Serous cystic neoplasms of the pancreas: clinicopathologic and molecular characteristics. Semin Diagn Pathol. 2014;31:475–83.
Reid MD, Bagci P, Ohike N, et al. Calculation of the Ki67 index in pancreatic neuroendocrine tumors: a comparative analysis of four counting methodologies. Mod Pathol. 2015b;28:686–94.
Schmitt AM, Anlauf M, Rousson V, et al. WHO 2004 criteria and CK19 are reliable prognostic markers in pancreatic endocrine tumors. Am J Surg Pathol. 2007;31:1677–82.
Serra S, Chetty R. Revision 2: an immunohistochemical approach and evaluation of solid pseudopapillary tumour of the pancreas. J Clin Pathol. 2008;61:1153–9.
Singhi AD, Norwood S, Liu TC, et al. Acinar cell cystadenoma of the pancreas: a benign neoplasm or non-neoplastic ballooning of acinar and ductal epithelium? Am J Surg Pathol. 2013;37:1329–35.
Tanaka M, Chari S, Adsay V, et al. International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology. 2006;6:17–32.
Thompson LDR, Basturk O, Adsay V. Pancreas. In: Mills SE, editor. Sternberg’s diagnostic surgical pathology. 6th ed. Wolters Kluwer Health; 2015.
Thompson LDR, Becker RC, Pryzgodski RM, et al. Mucinous cystic neoplasm (mucinous cystadenocarcinoma of low malignant potential) of the pancreas: a clinicopathologic study of 130 cases. Am J Surg Pathol. 1999;23:1–16.
Tiemann K, Kosmahl M, Ohlendorf J, Krams M, Kloppel G. Solid pseudopapillary neoplasms of the pancreas are associated with FLI-1 expression, but not with EWS/FLI-1 translocation. Mod Pathol. 2006;19:1409–13.
Tiemann K, Heitling U, Kosmahl M, et al. Solid pseudopapillary neoplasms of the pancreas show an interruption of the Wnt-signaling pathway and express gene products of 11q. Mod Pathol. 2007;20:955–60.
Vege SS, Gardner TB, Chari ST, et al. Low mortality and high morbidity in severe acute pancreatitis without organ failure: a case for revising the Atlanta classification to include “moderately severe acute pancreatitis”. Am J Gastroenterol. 2009;104:710–5.
Zamboni G, Scarpa A, Bogina G, et al. Mucinous cystic tumors of the pancreas: clinicopathological features, prognosis, and relationship to other mucinous cystic tumors. Am J Surg Pathol. 1999;23:410–22.
Zamboni G, Terris B, Scarpa A, et al. Acinar cell cystadenoma of the pancreas: a new entity? Am J Surg Pathol. 2002;26:698–704.
Zamboni G, Lüttges J, Capelli P, et al. Histopathological features of diagnostic and clinical relevance in autoimmune pancreatitis: a study on 53 resection specimens and 9 biopsy specimens. Virchows Arch. 2004;445:552–63.
Zhang L, Notohara K, Levy MJ, et al. IgG4-positive plasma cell infiltration in the diagnosis of autoimmune pancreatitis. Mod Pathol. 2007;20:23–8.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Basturk, O., Volkan Adsay, N. (2016). Pancreas. In: Cheng, L., Bostwick, D. (eds) Essentials of Anatomic Pathology. Springer, Cham. https://doi.org/10.1007/978-3-319-23380-2_43
Download citation
DOI: https://doi.org/10.1007/978-3-319-23380-2_43
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-23379-6
Online ISBN: 978-3-319-23380-2
eBook Packages: MedicineMedicine (R0)