
Abstract
Nonneoplastic and neoplastic lesions of the prostate are presented, with emphasis on the most common disorders. The clinical, macroscopic, and microscopic features are outlined, as well as main key points used in the differential diagnosis. Among the nonneoplastic lesions of the prostate, infectious and noninfectious etiologies are included. Topics include metaplastic and inflammatory conditions, precursors, intraductal carcinoma, prostatic adenocarcinoma and its variants, and the variety of soft tissue tumors. The classic Gleason grading system is described. Practical applications of immunohistochemistry in the different entities are offered.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Prostatitis
- Nodular hyperplasia
- Prostatic intraepithelial neoplasia
- Immunohistochemistry
- Adenocarcinoma
- Mesenchymal tumors
Inflammatory Lesions
Acute Bacterial Prostatitis
Clinical
-
♦
Sudden onset of fever, chills, pain, and irritative and obstructive symptoms
-
♦
Swollen, tender, and indurated on digital rectal examination
-
♦
E. coli infection accounts for 80% of cases
-
♦
Diagnosis confirmed by culture of midstream urine and/or prostatic secretions
-
♦
Transrectal ultrasonography useful for preoperative diagnosis
-
♦
Biopsy contraindicated
Microscopic
-
♦
Microabscess formation and heavy infiltrate of acute and chronic inflammatory cells (Fig. 38.1)
Fig. 38.1. 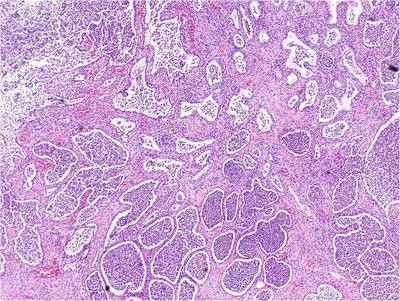
Acute prostatitis with microabscess formation.
-
♦
Acinar destruction and epithelial cell degeneration
-
♦
Stromal hemorrhage and edema
-
♦
Abscess is a rare complication, especially in immunocompromised patients

Chronic Bacterial and Nonbacterial Prostatitis
Clinical
-
♦
Chronic nonbacterial prostatitis is more common than chronic bacterial prostatitis (E. coli)
-
♦
Chlamydia trachomatis and Ureaplasma urealyticum are common etiologic agents
-
♦
Often follows an indolent clinical course with relapses and remissions
Microscopic
-
♦
Epithelial degeneration and metaplasia
-
♦
Chronic inflammation
Differential Diagnosis
-
♦
High-grade prostatic intraepithelial neoplasia (HGPIN)
-
Partial acinar involvement, nuclear stratification, and prominent nucleoli
-
Caution is urged in diagnosing prostatic intraepithelial neoplasia (PIN) in the setting of inflammation
-
Granulomatous Prostatitis
Clinical
-
♦
Prior history of urinary tract infection is common (Table 38.1)
Table 38.1. Etiology of Granulomatous Prostatitis -
♦
Suspicious for carcinoma on digital rectal examination
-
♦
Probably caused by blockage of prostatic ducts and stasis of secretion
Microscopic
-
♦
Specific etiology often cannot be determined from histologic examination
-
♦
Glandular disruption, epithelial degeneration, and metaplasia
-
♦
Granulomatous inflammation with or without necrosis
-
♦
Polymorphous chronic inflammation composed of multinucleated giant cells, histiocytes, lymphocytes, plasma cells, and neutrophils
Immunohistochemistry
-
♦
Prostate-specific antigen (PSA) negative, prostate acid phosphatase (PAP) negative, cytokeratin negative, CD68 positive, and other macrophage markers positive
Variants
-
♦
Xanthoma
-
Incidental finding in elderly men
-
Clusters and sheets of lipid-laden histiocytes in a nodular configuration (Fig. 38.2)
Fig. 38.2. 
Xanthoma .
-
CD68 positive, cytokeratin negative
-
-
♦
Xanthogranulomatous prostatitis
-
Nonspecific granulomatous prostatitis
-
Composed predominantly of sheets of epithelioid histiocytes (Fig. 38.3)
Fig. 38.3. 
Xanthogranulomatous prostatitis. Lymphocytes rim a massive monomorphous collection of macrophages with abundant clear cytoplasm. This case was initially misdiagnosed as high-grade carcinoma.
-
Polymorphous inflammatory infiltrate
-
Associated with atrophy and acinar disruption
-
-
♦
Malakoplakia
-
Due to defective intracellular lysosomal digestion of bacteria
-
Intracellular and extracellular Michaelis-Gutmann bodies are characteristic of the lesion (Fig. 38.4)
Fig. 38.4. 
Malakoplakia. Numerous Michaelis-Gutmann bodies are noted.
-
The Michaelis-Gutmann bodies represent bacterial debris within phagolysosomes, highlighted by PAS and von Kossa stains
-
-
♦
Wegener granulomatosis
-
Stellate and geographic granulomas with palisading histiocytes
-
Necrotizing vasculitis involving small- and medium-sized vessels
-
-
♦
Postsurgical granulomatous prostatitis
-
Occurs up to years following surgery
-
Central zone of fibrinoid necrosis surrounded by peripheral palisading of epithelioid histiocytes
-



Benign Lesions and Mimics of Adenocarcinoma
Benign Prostatic Hyperplasia and Other Forms of Hyperplasia
Benign Prostatic Hyperplasia
Clinical
-
♦
Occurs in 50% or more of men >50 years
-
♦
Often presents with lower urinary tract symptoms
-
♦
Develops in transition zone, resulting from stromal and epithelial proliferation
-
♦
Etiology and pathogenesis are not completely understood
-
♦
Inflammation is implicated in the pathogenesis of benign prostatic hyperplasia (BPH); patients with inflammation have larger prostates, higher serum PSA, and greater risk of urinary retention
-
♦
Hormonal regulation is mainly via dihydrotestosterone (DHT), derived from testosterone by the activity of 5-α-reductase
-
♦
Growth factors also play an important role in the development of BPH; epidermal growth factor (stimulatory) and transforming growth factor-β (inhibitory) alter prostatic growth
Macroscopic
-
♦
Yellow-gray rubbery to firm and bulging nodules in the transition zone and periurethral region (Fig. 38.5)
Fig. 38.5. 
Benign prostatic hyperplasia (BPH) , stromal variant. Bulging from the cut surface of this adenectomy specimen is a fleshy firm stromal nodule.
-
♦
For transurethral resection specimens, submit a minimum of six cassettes for the first 30 g of tissue and one cassette for every 10 g thereafter

Microscopic
-
♦
Epithelial and stromal hyperplasia in the transition zone and periurethral region (Fig. 38.6)
Fig. 38.6. 
Benign prostatic hyperplasia. This epithelium-predominant round nodule is typical.
-
♦
Stromal nodules consist of fibromuscular spindle cell proliferation with thin- or thick-walled vessels and scattered lymphocytic infiltrate (mainly T-helper cells)
-
♦
Often associated with prostatic infarct with squamous and urothelial metaplasia
-
♦
At least part of a nodule should be present for the diagnosis to be made on biopsies (uncommon)
-
♦
Multiple variants (see below) (Table 38.2)
Table 38.2. Histopathological Variants of Nodular Hyperplasia

Stromal Hyperplasia with Atypical Giant Cells
-
♦
Often occurs in the transition zone
-
♦
Benign variant of nodular hyperplasia
-
♦
Increased stromal cellularity with bizarre giant cells and nuclear degenerative changes (Fig. 38.7)
Fig. 38.7. 
Stromal hyperplasia with atypical giant cells.
-
♦
Nuclear pleomorphism, nuclear hyperchromasia, and pyknosis
-
♦
Lacks the circumscription of leiomyoma
-
♦
No mitotic figures
-
♦
Some have applied the term prostatic stromal tumor of uncertain malignant potential, but this is discouraged as it lumps stromal hyperplasia (benign) with phyllodes tumor (malignant)

Cribriform Hyperplasia
-
♦
Often occurs in the transition zone
-
♦
Variant of nodular hyperplasia
-
♦
Cribriform pattern of acinar proliferation with intact basal cell layer (Fig. 38.8)
Fig. 38.8. 
Cribriform hyperplasia. Note the variable size and collapsible nature of the luminal fenestrations. Unlike high-grade PIN and ductal adenocarcinoma, there are no cytologic abnormalities. In this preparation, the basal cell layers at the periphery of the acini are especially prominent.
-
♦
Uniform cells with clear or granular cytoplasm and inconspicuous nucleoli
-
♦
Basal cells probably contain the regenerative or stem cells of the prostate
-
♦
Occurs in 6% of biopsies and 9% of transurethral resection specimens

Basal Cell Proliferation
Basal Cell Hyperplasia
-
♦
Often occurs in the transition zone
-
♦
Variant of BPH
-
♦
Proliferation of basal cells with multiple layers (>2) (Fig. 38.9)
Fig. 38.9. 
Basal cell hyperplasia . These tight nests of basaloid cells are characteristic of BCH.
-
♦
Often eccentrically located with partial involvement of acini, retaining the overlying columnar or cuboidal secretory cells
-
♦
Basal cells have enlarged nuclei, fine powdery chromatin, and occasional nuclear grooves:
-
Nuclear “bubble” artifact or intranuclear vacuole often seen in formalin-fixed tissue but not in frozen section
-
-
♦
Often associated with chronic inflammation

Atypical Basal Cell Hyperplasia
-
♦
Same as basal cell hyperplasia BCH) but with prominent nucleoli (Fig. 38.10)
Fig. 38.10. 
Atypical basal cell hyperplasia. (A) The acini are set in a moderately fibrotic stroma. (B) The acini contain basal cells with prominent nucleoli.
-
♦
Require >10% of cells displaying prominent nucleoli for diagnosis

Basal Cell Adenoma
-
♦
Variant of BPH
-
♦
Nodule formation with BCH (Fig. 38.11)
Fig. 38.11. 
Basal cell adenoma from a transurethral resection specimen. The lesion is well circumscribed (A). Basal cells have powdery nuclei with fine chromatin (B).
-
♦
Well-circumscribed solid nests and aggregates of hyperplastic basal cells in a condensed fibrous stroma
-
♦
Plump nuclei, high nucleus-to-cytoplasmic ratio, and inconspicuous nucleoli
-
♦
High-molecular-weight cytokeratin 34βE12 positive (Table 38.3)
Table 38.3. Immunohistochemical Profiles of Benign Lesions in the Prostate -
♦
PSA and PAP are patchy positive
-
♦
S-100 protein and chromogranin are often positive

Atypical Adenomatous Hyperplasia
Clinical
-
♦
Occurs in the transition zone and is found in ~23% of prostatectomy specimens
-
♦
Multicentric in ~46% of cases
-
♦
Proposed as a putative precursor lesion, but considered by most to be benign
-
♦
The extent and zonal distribution of atypical adenomatous hyperplasia (AAH) and carcinoma share a weak but significant association
-
♦
Shares less frequent but similar allelic imbalance with prostatic adenocarcinoma
-
♦
May be associated with a subset of low-grade carcinoma arising in the transition zone
-
♦
The identification of AAH should not influence or dictate therapeutic decisions
Microscopic
-
♦
Requires most or all of the focus to be present for diagnosis of AAH on biopsy – very uncommon (Table 38.4)
Table 38.4 Atypical Adenomatous Hyperplasia vs. Well-differentiated Adenocarcinoma -
♦
Well-circumscribed nodular proliferation of small acini at the periphery of BPH; sometimes involves the entire nodule (Fig. 38.12A)
Fig. 38.12. 
Atypical adenomatous hyperplasia (AAH). This circumscribed cluster of small to intermediate acini was initially misdiagnosed as Gleason pattern 1 + 1 carcinoma (A); however, a fragmented basal cell layer was identified by immunostain for high-molecular-weight cytokeratin 34βE12 (B).
-
♦
Parent gland with larger branching lumina in the central location
-
♦
Lacks diffuse nucleolar enlargement
-
♦
May contain intraluminal mucin secretions and crystalloids
-
♦
Basal cell layer fragmented (Fig. 38.12B)
-
♦
α-Methylacyl-CoA racemase (P504S) immunostaining may be focally positive

Differential Diagnosis
-
♦
Verumontanum mucosal gland hyperplasia:
-
Located in the posterior wall of the distal prostatic urethra
-
Back-to-back arrangement of small acini with prominent corpora amylacea
-
Fragmented nonlamellated orange-red concretions
-
Cytoplasmic lipofuscin
-
Intact basal cell layer and intimately associated with urothelial-lined ducts
-
-
♦
Postatrophic hyperplasia
-
Lobular cluster of atrophic acini with proliferative change
-
Not intimately associated with nodular hyperplasia
-
Associated with adjacent atrophy with inflammation, stromal fibrosis, or smooth muscle atrophy
-
-
♦
Sclerosing adenosis:
-
Biphasic pattern with hyalinized periacinar stroma
-
S-100 protein and actin positive
-
-
♦
Low-grade small acinar prostatic adenocarcinoma
-
Nucleolar enlargement
-
Lacks basal cell layer
-
Postatrophic Hyperplasia
-
♦
Occurs in all zones with predilection for the peripheral zone (91% of cases)
-
♦
Found in up to 32% of radical prostatectomy specimens
-
♦
Lobular cluster of atrophic acini surrounding central dilated larger acini, often in a hyalinized stroma (Fig. 38.13)
Fig. 38.13. 
Postatrophic hyperplasia. Irregular circumscribed aggregate of markedly atrophic distorted acini set in a fibrous stroma.
-
♦
Variable acinar architectural distortion and irregularity
-
♦
Acini lined by a single layer of secretory cells with proliferative changes
-
♦
Moderate cytoplasm with luminal apocrine blebs
-
♦
Enlarged nuclei with evenly distributed fine granular chromatin and occasional enlarged nucleoli
-
♦
Fragmented or intact basal cell layer
-
♦
Often associated with adjacent inflammation
-
♦
Distinguished from carcinoma by characteristic lobular architecture, intact or fragmented basal cell layer, inconspicuous or mildly enlarged nucleoli, and adjacent acinar atrophy with stromal fibrosis or smooth muscle atrophy

Sclerosing Adenosis
Clinical
-
♦
Incidental finding in 2% of transurethral resection specimens
-
♦
An unusual variant of BPH
-
♦
Occurs in transition zone, usually solitary and microscopic
-
♦
The only prostatic lesion with myoepithelial differentiation of basal cells
-
♦
Benign
Microscopic
-
♦
Well-circumscribed proliferation of small acini in a dense myofibroblast stroma (Fig. 38.14A)
Fig. 38.14. 
Sclerosing adenosis. (A) Packed circumscribed cluster of small acini of variable size set in a densely cellular stroma. (B) Intense S-100 protein immunoreactivity in the basal cells of virtually every acinus.
-
♦
Thickened basement membrane with prominent myoepithelial cells
-
♦
Acini appear to merge with adjacent pale staining cellular stroma with abundant loose ground substance
-
♦
Compressed and distorted glands imparting a pseudoinfiltrative pattern
-
♦
Occasional nuclear and nucleolar enlargement; rare cases with prominent nucleolomegaly referred to as atypical sclerosing adenosis
-
♦
Moderate amount of clear to eosinophilic cytoplasm

Electron Microscopy
-
♦
Myoepithelial differentiation with aggregates of thin filaments
Immunohistochemistry (Table 38.3)
-
♦
High-molecular-weight cytokeratin 34βE12 and p63 positive
-
♦
Muscle-specific actin (MSA) positive
-
♦
S-100 protein positive (Fig. 38.14B)
-
♦
Negative for α-methylacyl-CoA racemase (P504S)
Differential Diagnosis
-
♦
AAH
-
Lacks densely hyalinized stroma and fragmented basal cell layer
-
MSA and S-100 protein negative
-
-
♦
Prostatic adenocarcinoma
-
Cytologic atypia with nucleomegaly and prominent nucleoli
-
Lacks hyalinized stroma
-
MSA, high-molecular-weight cytokeratin, and S-100 protein negative
-
Hyperplasia of Mesonephric Remnants (Florid Mesonephric Hyperplasia)
-
♦
Rare; occurs in all zones, mainly in the transition zone
-
♦
Lobular proliferation of small acini lined by single layer of cuboidal cells (Fig. 38.15)
Fig. 38.15. 
Mesonephric remnants.
-
♦
Two growth patterns:
-
Closely packed small round to oval tubules lined by cuboidal hobnail cells with eosinophilic cytoplasm
-
Proliferation of small acini with empty lumens or solid nests
-
-
♦
May have haphazard arrangement at periphery, imparting pseudoinfiltrative growth pattern
-
♦
Ectatic tubules with luminal colloid-like eosinophilic inclusions and micropapillary infoldings
-
♦
Uniform cells with occasional nuclear and nucleolar enlargement
-
♦
PSA and PAP negative; high-molecular-weight cytokeratin 34βE12 and p63 positive

Verumontanum Mucosal Gland Hyperplasia
-
♦
Located in the posterior wall of the midprostatic urethra
-
♦
Used as a landmark during transurethral resection of the prostate (resection is proximal)
-
♦
Recognized in 14% of radical prostatectomy specimens
-
♦
Rare in biopsies and not seen in transurethral resection specimens
-
♦
Often intimately associated with urothelium
-
♦
Multifocal lobular proliferation of closely packed small (>25) acini usually with intact basal cell layer (Fig. 38.16)
Fig. 38.16. 
Verumontanum mucosal gland hyperplasia.
-
♦
Uniform cells with basophilic cytoplasm and lack of cytologic atypia
-
♦
Numerous corpora amylacea and distinctive orange-red nonlaminated concretions that are often fragmented
-
♦
Luminal secretory cells may contain lipofuscin pigment
-
♦
Intact basal cell layer
-
♦
PSA, PAP, p63, and high-molecular-weight cytokeratin 34βE12 positive

Metaplasia (Table 38.5)
Squamous Metaplasia
-
♦
Often seen at edge of prostatic infarct and after hormonal therapy or cryotherapy (Fig. 38.17)
Fig. 38.17. 
Squamous metaplasia of benign epithelium following cryosurgery.
-
♦
Common in the region of prostatic urethra in patients with an indwelling catheter
-
♦
Syncytial aggregates of polygonal cells with abundant eosinophilic cytoplasm and hyperchromatic nuclei

Mucinous Metaplasia
-
♦
Clusters of columnar cells or goblet cells with mucin production (Fig. 38.18)
Fig. 38.18. 
Mucinous metaplasia.
-
♦
Focal or complete involvement of acini and lack of involvement of the entire lobular unit of acini
-
♦
Negative immunostaining for PSA and PAP
-
♦
High-molecular-weight cytokeratin 34βE12 positive
-
♦
Mucicarmine, PAS with diastase, and alcian blue positive

Eosinophilic Metaplasia
-
♦
May represent a form of host response related to regenerative/reparative process
-
♦
Clusters of cells with prominent eosinophilic cytoplasmic granules in apical location (Fig. 38.19)
Fig. 38.19. 
Eosinophilic metaplasia.
-
♦
Typically occur in small- to medium-sized prostatic ducts and may also occur in the acinar epithelium
-
♦
No clinical significance

Urothelial Metaplasia
-
♦
The presence of urothelium beyond the normal urothelial-columnar junction is often difficult to identify
-
♦
Stratified epithelium with streaming effect of nuclei (Fig. 38.20)
Fig. 38.20. 
Urothelial metaplasia .
-
♦
Ovoid cells with pale cytoplasm, uniform nuclei, nuclear grooves, perinuclear halos, fine granular chromatin, and inconspicuous nucleoli
-
♦
The long axis of the cells is perpendicular to the basement membrane

Nephrogenic Adenoma
-
♦
Suburethral location; composed of exophytic mass of small tubules or papillae with solid and cystic appearance (Fig. 38.21)
Fig. 38.21. 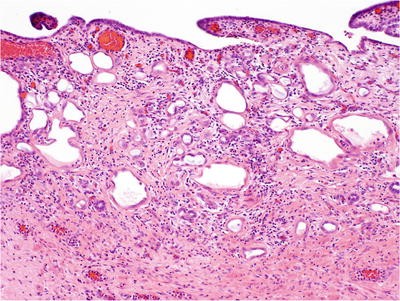
Nephrogenic adenoma (metaplasia).
-
♦
Uniform nuclei with fine granular chromatin and inconspicuous nucleoli; rare cases have focal or extensive nucleolomegaly, referred to as atypical nephrogenic metaplasia
-
♦
Edematous and often inflamed stroma without desmoplasia
-
♦
Often associated with proliferative papillary urethritis
-
♦
Negative immunoreactivity for PSA, PAP, and CEA
-
♦
High-molecular-weight cytokeratin 34βE12 positive
-
♦
Positive staining for α-methylacyl-CoA racemase (P504S) (58% of cases) creates potential for misdiagnosis as adenocarcinoma
-
♦
May be neither metaplastic nor neoplastic in nature; nephrogenic metaplasia in renal transplant recipients is apparent
-
♦
Derived from tubular cells of the transplant and is not a metaplastic proliferation of the recipient’s bladder urothelium

Atrophy
-
♦
Often located in the peripheral zone
-
♦
Lobular configuration of atrophic glands with open ectatic lumina in a sclerotic stroma
-
♦
Variable acinar architectural distortion and irregularity
-
♦
Cystic dilation of acini and ducts lined by flattened attenuated epithelial cells with scant cytoplasm, hyperchromatic nuclei, and inconspicuous nucleoli
-
♦
When associated with inflammation, the epithelium may show focal reactive proliferative changes
-
♦
The basal cell layer may be fragmented
-
♦
In the past, considered by some to be a potential precursor to adenocarcinoma, but convincing evidence is lacking and idea is largely abandoned
Seminal Vesicles and Ejaculatory Ducts
Microscopic
-
♦
Well circumscribed
-
♦
Complex papillary folds with irregular convoluted lumens (Fig. 38.22)
Fig. 38.22. 
Seminal vesicle . The epithelium contains scattered refractile golden-brown pigment, as well as moderate anisonucleosis.
-
♦
Lined by nonciliated pseudostratified columnar epithelium
-
♦
Ejaculatory ducts have large lumens with more prominent mucosal folding and prominent circumferential layer of the muscular wall
-
♦
Stromal (eosinophilic) hyaline bodies:
-
Often seen within the muscular wall, resulting from smooth muscle degeneration
-
Highlighted by Masson trichrome and PAS stain
-
-
♦
Bizarre smudged cells with granular refractile golden-yellow lipofuscin pigment
-
♦
Enlarged nuclei with nuclear hyperchromasia, coarse granular chromatin, prominent nucleoli, and occasional nuclear halos
-
♦
Multinucleated giant cells with pyknotic nuclei and a lack of mitotic figures
-
♦
DNA aneuploid in 6.7% of seminal vesicles

Immunohistochemistry
-
♦
PSA and PAP negative; high-molecular-weight cytokeratin 34βE12 and p63 positive
Differential Diagnosis
-
♦
Pigmented prostatic epithelium (melanosis):
-
Scant, finely granular, yellow-brown pigment
-
PSA and PAP positive
-
-
♦
Postatrophic hyperplasia:
-
Lobular arrangement of acini surrounding central dilated acini; proliferative change
-
Lacks lipofuscin or cytologic atypia
-
-
♦
High-grade PIN:
-
Lacks lipofuscin; displays significant nuclear pleomorphism
-
-
♦
Adenocarcinoma:
-
Lacks lipofuscin; displays nuclear degeneration; bizarre nuclei uncommon
-
PSA and PAP positive, cytokeratin 34βE12 negative
-
Senile Seminal Vesicle Amyloidosis
Clinical
-
♦
Occurs in up to 8% of men 46–60 years, 23% between ages 61 and 75 years, and 40% >75 years
-
♦
Derived from secretory protein of the epithelium
-
♦
Benign; not associated with systemic amyloidosis
Microscopic
-
♦
Linear or nodular subepithelial deposition of amorphous eosinophilic amyloid (Fig. 38.23)
Fig. 38.23. 
Senile seminal vesicle amyloidosis.
-
♦
Basement membrane thickening

Immunohistochemistry
-
♦
Congo red, crystal violet, toluidine blue, and PAS positive
Cowper Glands
Microscopic
-
♦
Located within the urogenital diaphragm; seen in biopsies of the apex
-
♦
Not present in transurethral resection specimens
-
♦
Equivalent to Bartholin glands of the female genital tract
-
♦
Small paired bulbomembranous urethral glands surrounded by the skeletal muscle
-
♦
Well-circumscribed small acinar proliferation (Fig. 38.24)
Fig. 38.24. 
Cowper gland.
-
♦
Uniform cells with abundant apical mucinous cytoplasm
-
♦
Lack nuclear and nucleolar enlargement

Immunohistochemistry
-
♦
PSA negative; high-molecular-weight cytokeratin, mucicarmine, and PAS with diastase positive
Differential Diagnosis
-
♦
Mucinous metaplasia:
-
Focal involvement of a small number of acini
-
Lacks skeletal muscle
-
-
♦
Mucinous adenocarcinoma:
-
Nests and clusters of epithelial cells floating in extravasated mucin pool
-
-
♦
Well-differentiated adenocarcinoma:
-
Prominent nucleoli
-
PSA positive, high-molecular-weight cytokeratin negative
-
Paraganglia
-
♦
Located closer to the base than the apex of the prostate
-
♦
Usually associated with neurovascular structures
-
♦
Solid nests and organoid arrangement of closely packed polygonal cells with abundant clear cytoplasm (Fig. 38.25)
Fig. 38.25. 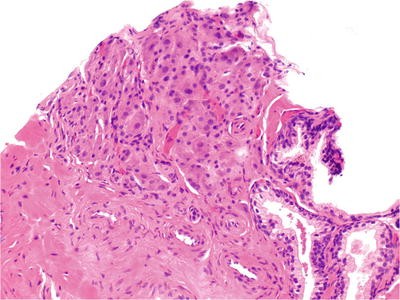
Intraprostate ganglionic tissue. In contrast with the benign acini (lower right), the ganglion cells are small, closely packed, and contain a light dusting of brown pigment. This focus was initially misdiagnosed as adenocarcinoma.
-
♦
Centrally located uniform nuclei with or without prominent nucleoli
-
♦
PSA, PAP, and cytokeratin negative; neuroendocrine markers positive

Prostatic Urethral Polyp
Proliferative Papillary Urethritis
-
♦
Papillary proliferation of the urothelium with metaplastic changes and reactive changes
-
♦
Inflammation and stromal edema
Ectopic Prostatic Tissue (Benign Polyp with Prostatic-Type Epithelium)
-
♦
Adolescents or young adults present with hematuria
-
♦
Delicate papillae with fibrovascular core and prostatic epithelial lining
Nephrogenic Adenoma
-
♦
Described elsewhere
Benign Urothelial Papilloma
-
♦
Patient <50 years with solitary lesion <2 cm in greatest dimension
-
♦
<7 cells in thickness with intact superficial (umbrella) cell layer
-
♦
No significant cytologic atypia (no more than grade 1 urothelial carcinoma)
Inverted Papilloma
-
♦
Patients present with hematuria and urinary obstructive symptoms
-
♦
Smooth contoured invaginated cords and columns of urothelial cells with intact overlying urothelium
-
♦
Peripheral palisading basaloid cells and thickened basement membrane
-
♦
Squamous metaplasia and microcystic change
-
♦
Scant stroma
-
♦
Lacks fibrovascular cores
High-Grade Prostatic Intraepithelial Neoplasia (HGPIN)
Definition
-
♦
Precancerous end of the morphologic continuum of cellular proliferations within preexisting prostatic ducts, ductules, and acini
Clinical
-
♦
Divided into low grade (formerly PIN 1) and high grade (formerly PIN 2 and 3)
-
♦
Most pathologists do not report low-grade PIN, recognizing the difficulty in separating this lesion from benign epithelium and reactive atypia
-
♦
PIN is genotypically and phenotypically linked to cancer
-
♦
Precedes the onset of carcinoma by 5–10 years
-
♦
Multifocal (63% of cases) and coexists with cancer in 86% of prostatectomy specimens
-
♦
Occurs in the nontransition zone (63% of cases) and all zones (36%)
-
♦
Present in up to 4.2% of transurethral resection specimens (2.8% without cancer, 10.2% with cancer)
-
♦
The volume of HGPIN increases with the pathologic stage, Gleason grade, and positive surgical margins in patients with prostate cancer
-
♦
More prevalent and extensive and occurs approximately a decade earlier in African American men than in Caucasian men
-
♦
Prevalence and extent of HGPIN are decreased after androgen deprivation therapy
-
♦
No influence on serum PSA concentration
-
♦
Found in approximately 9% of contemporary needle biopsies
-
♦
The diagnosis of HGPIN confers a 33% predictive value for cancer on repeat biopsy within 1 year
-
♦
Multifocal HGPIN has an even higher predicate value for cancer than unifocal HGPIN on biopsy
-
♦
Followup is suggested, but the interval may be 1 year or more according to some; there are no standards, and most agree that multifocal or extensive PIN requires earlier followup
Patterns of Growth
-
♦
Tufting (97% of specimens with HGPIN, most common) (Fig. 38.26A)
Fig. 38.26. 
Four major patterns of high-grade prostatic intraepithelial neoplasia (PIN). Tufting pattern of high-grade PIN (A). Small mounds of cells protrude into the lumen. This focus has a prominent basal cell layer at the periphery. Micropapillary pattern of high-grade PIN (B). Elongated fingerlike projections of epithelium protrude into the lumens. Flat pattern of high-grade PIN (C). Cribriform pattern of high-grade PIN (D).
-
♦
Micropapillary (66%) (Fig. 38.26B)
-
♦
Flat (21%) (Fig. 38.26C)
-
♦
Cribriform (19%) (Fig. 38.26D)
-
♦
Other rare growth patterns include signet ring cell, small cell (neuroendocrine), foamy gland (microvacuolated), hobnail (inverted), and squamous patterns

Pattern of Spread
-
♦
Replacement of normal luminal secretory cells with preservation of the basal cell layer
-
♦
Direct invasion with disruption of the basal cell layer
-
♦
Pagetoid spread (rare)
Microscopic
-
♦
Nuclear and nucleolar enlargements are the cytologic hallmark of HGPIN
-
♦
Cellular crowding, irregular spacing, nuclear stratification, and overlapping
-
♦
No significant expansion of ductules (unlike intraductal carcinoma; see below)
-
♦
Partial acinar involvement is frequent
-
♦
No necrosis
-
♦
Cells usually display cytoplasmic blebs along the luminal surface
-
♦
Disruption of the basal cell layer is highlighted by high-molecular-weight cytokeratin and p63 (Fig. 38.27) (Table 38.6)
Fig. 38.27. 
High-grade PIN, triple immunostain: Brown reaction product indicates a patchy and fragmented pattern of immunoreactivity for high-molecular-weight cytokeratin 34βE12 in basal cell cytoplasm and p63 in basal cell nuclei; red reaction product indicates immunoreactivity for alpha-methylacyl-CoA racemase (P504S) in luminal secretory cells.
Table 38.6. Immunohistochemical Profiles of Preinvasive and Malignant Lesions in the Prostate -
♦
α-Methylacyl-CoA racemase (P504S) and c-myc stain positive (Fig. 38.27)

Differential Diagnosis
-
♦
Inflammatory reactive changes
-
Metaplastic (eosinophilic) changes and inflammatory background
-
-
♦
Urothelial metaplasia
-
Lacks prominent nucleoli
-
-
♦
Seminal vesicles and ejaculatory ducts
-
Bizarre cells with lipofuscin pigment
-
Nuclear hyperchromasia, nuclear pleomorphism, and degenerative changes
-
PSA and PAP negative
-
-
♦
Cribriform hyperplasia
-
Occurs in transition zone; sieve-like pattern
-
Uniform cells with clear cytoplasm
-
Lacks nuclear and nucleolar enlargement
-
-
♦
Postatrophic hyperplasia
-
Lacks prominent nucleoli
-
-
♦
Atypical basal cell hyperplasia (ABCH)
-
Small solid nests or eccentric expansion of the basal cell layers between normal columnar secretory cells and basement membrane
-
The long axis of basal cells is usually parallel to the basement membrane
-
Enlarged nuclei with delicate stippled chromatin, occasional nuclear grooves, and nuclear “bubble” artifact
-
Often associated with inflammatory background
-
Cytokeratin 34βE12 positive
-
-
♦
Low-grade PIN
-
The epithelium lining ducts and acini are heaped up, crowded, and irregularly spaced
-
Lacks prominent nucleoli and less nuclear hyperchromasia
-
Intact basal cell layer without disruption
-
-
♦
Intraductal carcinoma
-
Cribriform or papillary growth with significant expansion of ductular size
-
Frank anaplasia
-
Usually adjacent to or associated with invasive cancer
-
-
♦
Ductal (endometrioid) prostatic adenocarcinoma
-
Lacks basal cell layer
-
-
♦
Large gland variant of Gleason pattern 3 carcinoma and cribriform variant
-
More extensive involvement, infiltrative growth pattern
-
Often associated with small acinar carcinoma
-
Lacks circumferential basal cell layer
-
Atypical Small Acinar Proliferation Suspicious for but Not Diagnostic of Malignancy (ASAP)
Clinical
-
♦
A diagnostic category encompassing a spectrum of histologic abnormalities that fall below the threshold for the diagnosis of cancer
-
Not a diagnostic entity, as it often represents undersampled cancer
-
-
♦
The incidence of atypical small acinar proliferation (ASAP) is 2.5–4% in contemporary prostate biopsies
-
♦
Predicts ~45% likelihood for cancer on repeat biopsy within 1 year
-
♦
Many ASAP foci may represent marginally sampled cancer
-
♦
99% of cancers were diagnosed on second and third biopsy, usually within 6 months after the ASAP diagnosis (73%)
-
♦
41% of cancers were detected exclusively in other sites other than that of the initial ASAP lesion
-
♦
The entire prostate should be rebiopsied due to random sampling variation
Microscopic
-
♦
Lacks the full complement of requisite architectural and cytologic features of cancer (Table 38.7)
Table 38.7. Reasons for the Diagnosis of Atypical Small Acinar Proliferation (ASAP) -
♦
Usually very small in size – invariably less than two dozen acini (Fig. 38.28A)
Fig. 38.28. 
Atypical small acinar proliferation suspicious for but not diagnostic of malignancy. (A) The aggregate of about half a dozen small acini with variable size, shape, and spacing stands in marked contrast with the adjacent benign acini. Note cholesterol clefts and intraluminal neutrophils, raising the concern for reactive changes rather than neoplasia; (B) same focus as (A), immunostained for high-molecular-weight cytokeratin 34βE12. The absence of staining in the acini of concern compounds the suspicion of malignancy. Note weak to moderate staining of basal cells in the adjacent benign acini.
-
♦
The focus often disappears on deeper levels
-
♦
Lacks unequivocal cytologic features of malignancy
-
♦
Enlarged nucleoli are often difficult to find
-
♦
Clustered growth of acini
-
♦
May represent partial sampling of AAH, sclerosing adenosis, or low-grade cancer
-
♦
Treatment-induced atypia
-
♦
Confounding acinar atrophy and prominent inflammation in the immediate vicinity of suspicious acini and poor histologic preparations
-
♦
Features that may be present include:
-
Infiltrative growth
-
Variation in acinar size
-
Nucleomegaly
-
Nucleolar enlargement
-
Microvacuolated cytoplasm
-
Intraluminal proteinaceous secretions
-
Luminal mucin
-
Crystalloids
-

Immunohistochemistry
-
♦
High-molecular-weight cytokeratin (34βE12) and p63 negative or equivocal (Fig. 38.28B)
-
♦
α-Methylacyl-CoA racemase (P504S) and c-myc are usually negative, weak, or equivocal
Differential Diagnosis (See “Prostatic Adenocarcinoma”)
-
♦
Prostatic adenocarcinoma:
-
Usually requires a minimum of three malignant acini for the diagnosis, unless:
-
•
Prominent cytologic anaplasia was present
-
•
No confounding inflammation
-
•
Persistence of cancer on serial sections
-
•
The possibility of seminal vesicle/ejaculatory ducts and other mimics has been excluded
-
•
-
-
♦
HGPIN
-
Frequently coexists with ASAP
-
-
♦
Atrophy and postatrophic hyperplasia
-
♦
Sclerosing adenosis
-
♦
Basal cell hyperplasia
-
♦
AAH
Malignant Tumors
Intraductal Carcinoma
Clinical
-
♦
No specific findings; usually an incidental finding in association with typical adenocarcinoma
-
♦
On biopsies, may be observed in isolation (very rare in isolation in prostatectomies)
-
♦
Previously referred to as noninvasive ductal carcinoma
-
♦
Considered to be clinically aggressive, but no consensus exists regarding optimal response when found in isolation on biopsy (some believe that this finding warrants immediate definitive treatment; others disagree)
Microscopic
-
♦
Marked expansion of ductal space by a proliferation of frankly malignant cells
-
♦
Nucleomegaly with frank nuclear anaplasia
-
♦
Dense near-solid (rigid) cribriform growth or partial solid growth
-
♦
Duct space enlargement to greater than two times the diameter of the largest adjacent benign spaces
-
♦
Comedonecrosis
-
♦
Intact or partially intact basal cell layer at the periphery of the proliferation
-
♦
Almost always associated with invasive carcinoma; this may not be apparent in a biopsy
-
♦
There is still a high level of interobserver disagreement
Immunohistochemistry
-
♦
Basal cell-specific cytoplasmic high-molecular-weight cytokeratin (34βE12) positive at the periphery, similar to high-grade PIN
-
♦
PTEN and ERG immunoreactivity in majority of cases, unlike PIN that is usually negative
Differential Diagnosis (See “Prostatic Adenocarcinoma”)
-
♦
Prostatic adenocarcinoma, especially ductal carcinoma:
-
Lacks basal cell layer
-
-
♦
Large gland variant of Gleason pattern 3 carcinoma and cribriform variant:
-
More extensive involvement, infiltrative growth pattern
-
Often associated with small acinar carcinoma
-
Lacks circumferential basal cell layer
-
-
♦
High-grade prostatic intraepithelial neoplasia:
-
Smaller ducts and ductules without massive enlargement
-
No frank anaplasia
-
Cribriform pattern is loose and “collapsible” without solid growth
-
No comedonecrosis
-
Immunohistochemistry for PTEN and ERG recommended in borderline cases
-
Prostatic Adenocarcinoma
Clinical
-
♦
Most common non-skin cancer in American men
-
♦
Accounted for 220,800 newly diagnosed cancers and 27,540 cancer deaths in 2015
-
♦
One in six men will develop clinically evident prostate cancer during his life
-
♦
Prevalence increases from 10–20% at age 50 years to ~80% at age 80 years
-
♦
Proposed risk factors include age, family history, race, dietary fat, heavy metal exposure (cadmium, zinc), vasectomy, obesity, alcohol, and HGPIN or ASAP on biopsy
-
♦
The American Cancer Society recommends:
-
Starting at age 50, men should talk to a doctor about the pros and cons of PSA testing to decide if testing is the right choice for them
-
If they are African American or have a father or brother who had prostate cancer before age 65, men should have this talk with a doctor starting at age 45
-
-
♦
An abnormal serum PSA concentration is commonly defined as a value >2.5 ng/ml
-
♦
Up to 15% of men with cancer have normal serum PSA (<2.5 ng/ml)
-
♦
Serum PSA half-life is 2–3 days
-
♦
70–80% of prostate cancers arise in the peripheral zone (often referred to as the posterior lobe in the older literature), 15–25% in the transition zone, and 10% in the central zone
-
♦
Prostatic carcinoma in the transition zone is usually well differentiated
-
♦
Fusions of the 5′ untranslated end of the androgen-responsive transmembrane serene protease gene TMPRSS2 and the ETS transcription factor family members, particularly ERG, are key molecular events during initiation and progression of prostate cancer
-
♦
TMPRSS2-ERG gene fusion is present in approximately 50% of prostate cancer
-
♦
Prostate cancer with TMPRSS2-ERG fusion may behave more aggressively than fusion-negative tumors
-
♦
Detection of TMPRSS2-ERG gene fusion may be useful for predicting cancer progression when isolated high-grade PIN is identified in needle biopsies
Macroscopic
-
♦
Yellow-white mass with a firm consistency in the peripheral zone
-
♦
Many are grossly inapparent
Gleason Grading
-
♦
Based on the degree of architectural differentiation (Figs. 38.29 and 38.30)
Fig. 38.29. 
Original Gleason grading diagram for prostate cancer.
Fig. 38.30. 
Gleason grading of prostati c adenocarcinoma. (A): Gleason 1 + 1 = 2 adenocarcinoma on transurethral resection. At this magnification, BPH cannot be excluded. However, the acini throughout displayed enlarged nuclei and prominent nucleoli; further, the acini were negative for high-molecular-weight cytokeratin 34βE12; (B) Gleason pattern 2 + 2 = 4 adenocarcinoma. There is only mild to moderate variation in acinar size and shape, and the acinar contours are chiefly round and smoothly sculpted. (C) Gleason pattern 3 + 3 = 6 adenocarcinoma. There is greater variation in size, shape, and spacing of acini than in patterns 1 and 2. Note prominent nucleolomegaly; (D) Gleason pattern 4 + 4 = 8 adenocarcinoma. The malignant acini display fusion and are lined by cells with enlarged nuclei and prominent nucleoli; (E) Gleason 5 + 5 = 10 adenocarcinoma. There are sheets of cells with nuclear and nucleolar enlargement; (F) Gleason 5 + 5 = 10 adenocarcinoma. There are distorted solid nests and cords of cells with only rare abortive lumens. Note abnormal mitotic figure centrally.
-
♦
The predominant grade is recorded as the primary grade, and the nondominant grade is assigned as the secondary grade
-
♦
When only one pattern exists (frequently encountered on biopsies), then double the grade
-
♦
Gleason score = primary grade + secondary grade
-
♦
Needle biopsy underestimates tumor grade in 33–45% of cases and overestimates grade in 4–32% of cases


Reporting
-
♦
Biopsy specimens
-
Biopsy site
-
Histopathologic type of carcinoma
-
Gleason score
-
Tertiary pattern
-
Extent of cancer
-
•
Percent of length of specimens involved
-
•
Number of cores involved and total number of cores sampled
-
•
-
Perineural invasion
-
Extraprostatic extension (rare in biopsies)
-
Associated conditions (e.g., HGPIN, postatrophic hyperplasia)
-
Ancillary studies, as needed (e.g., immunohistochemistry)
-
-
♦
Transurethral resection specimens
-
12 g, embed totally; >12 g, a minimum of six cassettes for the first 12 g and thereafter one cassette for every 10 g; if cancer involves <5% of the tissue submitted, all remaining tissue should be examined
-
-
♦
Histopathologic type of carcinoma
-
Gleason score
-
Extent of cancer (% of specimen)
-
HGPIN and/or ASAP
-
-
♦
Radical prostatectomy specimens
-
Weight and size of the prostate
-
Histopathologic type of carcinoma
-
Gleason score
-
Location of cancer
-
•
Bilateral versus unilateral (left or right)
-
•
Anterior versus posterior
-
•
Peripheral zone versus transition zone
-
•
-
Estimated cancer volume (% of specimen)
-
Extraprostatic extension (EPE) (Fig. 38.31)
Fig. 38.31. 
Extraprostatic extension. (A) Cancer in the adipose tissue, (B) cancer in the perineural space of large neurovascular bundle, and (C) cancer in the anterior skeletal muscle.
-
•
Location and extent
-
•
Definition of EPE
-
•
-
Cancer in adipose tissue (Fig. 38.31A)
-
Cancer in perineural spaces of the neurovascular bundles outside the prostate (Fig. 38.31B)
-
Cancer in the anterior muscle beyond the rounded interface between the fibromuscular stroma and skeletal muscle (Fig. 38.31C)
-
Seminal vesicle invasion (Fig. 38.32)
Fig. 38.32. 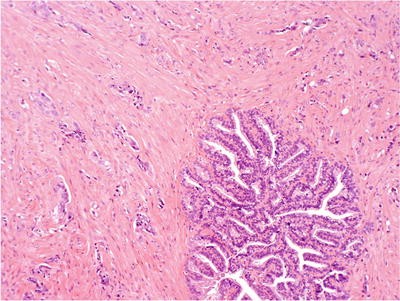
Seminal vesical invasion by prostatic adenocarcinoma. Lymphovascular invasion is also present.
-
•
Cancer in the adventitia but not in the muscular wall of the seminal vesicle does not qualify for seminal vesicle invasion
-
•
-
Surgical margin status
-
•
Positive margins are defined as cancer cells at the inked surface
-
•
Record sites and extent of margins involved are used
-
•
-
Vascular/lymphatic invasion
-
HGPIN and/or ASAP
-
Associated conditions (e.g., nodular hyperplasia)
-
Lymph node status:
-
•
Anatomic sites
-
•
Number of positive nodes
-
•
Size of nodal metastasis
-
•
Extranodal extension (we exclude this because of recent data)
-
•
-
-
♦
Ancillary studies, as needed (e.g., immunohistochemistry)
-
♦
Pathologic stage (state which TNM classification is used)


Microscopic
-
♦
The diagnosis of cancer is made in the presence of >3 malignant acini in most cases
-
♦
Angulated and distorted acini with an irregular haphazard arrangement and infiltrative growth pattern
-
♦
Acini vary in size, shape, and spacing and lack a basal cell layer
-
♦
Enlarged nuclei with large eccentrically located prominent nucleoli (>1 μm)
-
♦
The presence of multiple nucleoli is strong evidence of malignancy
-
♦
Vacuolated or microvacuolated cytoplasm
-
♦
Collagenous micronodules are a specific finding of prostatic adenocarcinoma, correlated with mucin production by the tumor (0.6% of biopsies and 12.7% of prostatectomies)
-
♦
Extraprostatic extension and lymphovascular invasion are rare in needle biopsies and are diagnostic of prostatic adenocarcinoma
-
♦
Perineural invasion is of diagnostic value, but has no apparent clinical significance in most studies
-
♦
Complete circumferential perineural growth and intraneural and/or ganglion invasion are usually diagnostic for cancer
-
♦
Intraluminal crystalloids and amorphous wispy basophilic acid mucin secretions are helpful, but not specific findings of cancer
-
♦
Neuroendocrine cells with large eosinophilic granules are seen focally in 10% of cases, but have no diagnostic or prognostic significance
-
♦
Necrotic debris within lumina indicates Gleason pattern 5 cancer
Immunohistochemistry (Table 38.6)
-
♦
PSA (located in endoplasmic reticulum, vesicle vacuoles, luminal cells) positive
-
♦
PAP (lysosome) positive
-
♦
Basal cell-specific cytoplasmic high-molecular-weight cytokeratin (34βE12) positive (Fig. 38.33)
Fig. 38.33. 
Prostatic adenocarcinoma . (A) Gleason 3 + 3 = 6 adenocarcinoma, consisting of less than a dozen acini with hyperchromatic nuclei. (B) Triple immunostain reveals brown reaction product in benign acini but not the cancer acini (high-molecular-weight cytokeratin 34βE12 in basal cell cytoplasm and p63 in basal cell nuclei) and red reaction product for racemase in luminal secretory cells. (C) Another case of Gleason 3 + 3 = 6 adenocarcinoma (large acinar pattern) with immunophenotype diagnostic of malignancy (note benign acinus in top left of image for comparison).
-
♦
Basal cell-specific nuclear p63 positive (Fig. 38.33)
-
♦
α-Methylacyl-CoA racemase (P504S) positive in a granular distribution along the luminal surfaces of the neoplastic secretory cells (Fig. 38.33)
-
♦
Positive c-myc nuclear staining for HGPIN and cancer

Differential Diagnosis
-
♦
Inflammatory reactive changes
-
Associated with inflammation and metaplasia
-
Lacks nucleolar enlargement
-
High-molecular-weight cytokeratin (34βE12) positive
-
-
♦
Xanthoma and xanthogranulomatous prostatitis
-
Sheets of foamy histiocytes
-
PSA/PAP negative, cytokeratin negative, and macrophage markers (CD68) positive
-
-
♦
Postatrophic hyperplasia (PAH)
-
Lobular clusters of atrophic acini with epithelial proliferative changes
-
Central large dilated atrophic acini or ducts
-
Moderate cytoplasm with occasional apical cytoplasmic blebs
-
Lacks diffuse nucleolar enlargement
-
Background of inflammation, atrophy, and stromal fibrosis
-
Intact or fragmented basal cell layer
-
-
♦
ABCH
-
Proliferation of basal cells between normal columnar secretory cells and basement membrane
-
Eccentric expansion of multiple basal cell layers
-
The long axis of basal cells is often oriented parallel to the luminal surface
-
Clear cytoplasm
-
Enlarged nuclei with fine powdery chromatin, occasional nuclear grooves, and nuclear “bubble” artifact
-
Often associated with inflammation
-
High-molecular-weight cytokeratin (34βE12) and p63 positive
-
-
♦
AAH
-
Lobular architecture maintained with fragmented basal cell layer
-
Closely packed small acini
-
Lacks cytologic features of malignancy
-
Intimately associated with nodular hyperplasia with similar cytologic findings
-
-
♦
Seminal vesicles and ejaculatory ducts
-
Circumscribed, pushing border rather than haphazard arrangement
-
Bizarre cells with golden-yellow lipofuscin pigment
-
Nuclear hyperchromasia, nuclear pleomorphism, and degenerative changes
-
Negative immunoreactivity for PSA or PAP
-
-
♦
Paraganglia
-
Closely associated with nerves or blood vessels
-
Lobular cluster of polygonal cells with abundant clear cytoplasm
-
Centrally located nuclei with prominent nucleoli
-
PSA, PAP, and broad-spectrum cytokeratin negative; neuroendocrine markers positive
-
-
♦
Lesion with clear cell changes
-
AAH
-
Cribriform hyperplasia
-
Basal cell hyperplasia
-
Cowper glands
-
Mucinous metaplasia
-
Paraganglion
-
Xanthoma and xanthogranulomatous prostatitis
-
Metabolic storage disease
-
Sclerosing adenosis
-
-
♦
Basal cell layer disruption
-
HGPIN
-
Inflammatory atypia
-
AAH
-
Atrophy and postatrophic hyperplasia (PAH)
-
-
♦
Sclerosing adenosis
-
Compressed and distorted acini in cellular fibrous stroma
-
Lobular pattern is retained and lacks cytologic atypia
-
High-molecular-weight cytokeratin (34βE12), p63, S-100 protein, and muscle-specific antigen (MSA) positive
-
Negative for α-methylacyl-CoA racemase (P504S)
-
-
♦
Hyperplasia of mesonephric remnants
-
Lobular arrangement of small tubular acini
-
Often contains intraluminal eosinophilic colloid-like material
-
-
♦
Nephrogenic metaplasia
-
Polypoid proliferation of small tubules and papillae lined by hobnail cells
-
Thickened basement membrane and intraluminal eosinophilic secretions
-
Edematous stroma and cystic dilation of some tubules
-
Associated with adjacent urothelium-lined ducts
-
Positive α-methylacyl-CoA racemase (P504S) staining may cause diagnostic confusion with cancer
-
-
♦
Urothelial carcinoma
-
Often coexisting urothelial dysplasia and carcinoma in situ
-
May have history of bladder carcinoma
-
Nuclear pleomorphism, eosinophilic cytoplasm
-
Often associated with heavy inflammation
-
PSA/PAP negative, high-molecular-weight cytokeratin (34βE12) and p63 positive
-
Prostatic Adenocarcinoma Variants (Table 38.8)
Ductal (Endometrioid) Adenocarcinoma
Clinical
-
♦
Accounts for 0.8% of prostatic adenocarcinomas
-
♦
Similar clinical presentation and prognosis as conventional acinar carcinoma
-
♦
Typically occurs in elderly men with urinary obstructive symptoms
-
♦
Most cases have concurrent invasive acinar carcinoma
-
♦
Serum PSA concentration is often normal, probably due to secretion of PSA directly into the prostatic urethra by tumor cells
Macroscopic
-
♦
Polypoid tumor located in the urethra at or near the verumontanum is classic; however, most cases are within large cystic spaces within the peripheral zone
Microscopic
-
♦
Considered Gleason pattern 4 (no necrosis) or 5 (with necrosis) cancer
-
♦
Cribriform and papillary proliferation of medium- to large-sized acini (Fig. 38.34)
Fig. 38.34. 
Ductal adenocarcinoma. This papillary proliferation filled the large periurethral prostatic ducts and protruded into the urethra.
-
♦
Acini lined by stratified tall columnar cells with cytologic atypia
-
♦
May have prominent central necrosis and frequent mitotic figures

Immunohistochemistry
-
♦
PSA, PAP, α-methylacyl-CoA racemase (P504S), CEA (focal), and c-myc positive
Differential Diagnosis
-
♦
Cribriform hyperplasia
-
Lacks cytologic atypia, α-methylacyl-CoA racemase (P504S) positive
-
-
♦
HGPIN (cribriform pattern)
-
Less extensive; lacks infiltrative growth
-
-
♦
Intraductal carcinoma (noninvasive ductal carcinoma):
-
Intact basal cell layer
-
-
♦
Urothelial carcinoma
-
Dysplasia and carcinoma in situ of adjacent urothelium
-
PSA negative
-
-
♦
Large gland variant of Gleason pattern 3 adenocarcinoma
-
♦
Ectopic prostatic tissue (prostatic urethral polyp)
-
Lacks significant cytologic atypia
-
-
♦
Proliferative papillary urethritis
-
Lacks cytologic atypia
-
PSA negative
-
Mucinous Adenocarcinoma
Clinical
-
♦
Accounts for 0.04% of prostate carcinoma (pure mucinous pattern)
-
♦
Similar clinical presentation to typical acinar carcinoma
-
♦
Aggressive, may not respond well to radiotherapy or androgen deprivation
-
♦
Elevated serum PSA concentration and bone metastasis
Macroscopic
-
♦
Often located in peripheral zone
Microscopic
-
♦
Usually considered Gleason pattern 4 adenocarcinoma
-
♦
Requires 25% of tumor to contain extracellular mucin, excluding nondilated glands with mucin for diagnosis
-
♦
The presence of epithelial nests or glands in mucin pools is diagnostic (Fig. 38.35)
Fig. 38.35. 
Mucinous (colloid) carcinoma, with pools of mucin punctuated by floating islands and trabeculae of cancer cells.
-
♦
May present with acinar or cribriform carcinoma with luminal distention
-
♦
Collagenous micronodules are often seen

Immunohistochemistry
-
♦
PSA, PAP, c-myc, and α-methylacyl-CoA racemase (P504S) positive
Differential Diagnosis
-
♦
Metastatic or contiguous spread of mucinous adenocarcinoma (e.g., colon cancer)
-
PSA and PAP negative
-
-
♦
Cowper glands
-
Circumscribed lobules of closely packed small uniform acini
-
Embedded in skeletal muscle
-
Uniform cells with mucinous cytoplasm and basally located small nuclei
-
PSA negative; high-molecular-weight cytokeratin and p63 positive
-
Small Cell Carcinoma (High-Grade Neuroendocrine Carcinoma)
Clinical
-
♦
Highly aggressive; most patients die within 2 years
-
♦
May present with paraneoplastic syndromes
-
♦
May develop after radiation therapy and hormonal therapy for acinar adenocarcinoma
-
♦
Serum PSA varies according to cancer volume and stage
Microscopic
-
♦
Considered Gleason pattern 5 adenocarcinoma (Fig. 38.36)
Fig. 38.36. 
Small cell carcinoma of the prostate.
-
♦
Infiltrating cords and sheets of small cells with high N/C ratio and crush artifact
-
♦
Nuclear hyperchromasia, nuclear molding, and inconspicuous nucleoli
-
♦
Mixed with typical adenocarcinoma in about half of cases

Immunohistochemistry
-
♦
Neuroendocrine markers (chromogranin A, synaptophysin, serotonin) are positive, PSA is usually positive, and PAP may be positive
Adenocarcinoma with Neuroendocrine Differentiation
-
♦
All adenocarcinomas have scattered cells with neuroendocrine features
-
♦
No prognostic significance for number of neuroendocrine cells other than pure small cell carcinoma (Fig. 38.37)
Fig. 38.37. 
Prostatic adenocarcinoma with neuroendocrine differentiation. These were previously designated as a “Paneth cell-like change” (PCLC).
-
♦
Rare cancers have neuroendocrine cells with large eosinophilic granules (formerly referred to as Paneth cell-like change)

Low-Grade Neuroendocrine Carcinoma (Carcinoid)
-
Clinical
-
♦
Very rare; fewer than ten pure cases reported
-
♦
Probably indolent, but too few cases to be definitive
-
♦
-
Microscopic
-
♦
Typical features of carcinoid tumor at other sites (e.g., insular, trabecular, nested patterns, etc.)
-
♦
Mixed with typical adenocarcinoma in more than half of reported cases
-
♦
-
Immunohistochemistry
-
♦
Neuroendocrine markers (chromogranin a, synaptophysin, serotonin) are positive, PSA is usually positive, and PAP may be positive
-
♦
Signet Ring Cell Carcinoma
Clinical
-
♦
Similar clinical presentation as typical acinar carcinoma
-
♦
High stage presentation with unfavorable prognosis
Microscopic
-
♦
Considered Gleason pattern 5 adenocarcinoma
-
♦
Requires 25% tumor with signet ring cells for diagnosis (Fig. 38.38)
Fig. 38.38. 
Signet ring cell carcinoma.

Immunohistochemistry
-
♦
PSA and PAP positive; CEA, mucin, and oil red O are usually positive
Differential Diagnosis
-
♦
Paraganglion
-
Organoid nests of polygonal cells with centrally located nuclei
-
-
♦
Vacuolated smooth muscle cells or lymphocytes
-
PSA and PAP negative
-
Squamous Cell and Adenosquamous Carcinoma
Clinical
-
♦
Extremely rare in the prostate
-
♦
Account for <0.5% of cases of prostatic carcinoma
-
♦
Similar clinical presentation as typical acinar carcinoma
-
♦
Patients often have a prior history of hormonal or radiation therapy
-
♦
May be associated with schistosomiasis
-
♦
Aggressive; patients often present with osteolytic bone metastasis and are refractory to hormonal therapy
-
♦
Serum PSA may be normal even in the presence of metastasis
Macroscopic
-
♦
Often located in the periurethral region
Microscopic
-
♦
Usually high grade
-
♦
Nests and cords of malignant cells with squamous differentiation (Fig. 38.39)
Fig. 38.39. 
Squamous cell carcinoma in the prostate arising 10 years after radiation and hormonal therapy for high-grade adenocarcinoma.
-
♦
Requires the absence of acinar carcinoma and bladder involvement for diagnosis of pure squamous cell carcinoma

Immunohistochemistry
-
♦
PSA and PAP may be negative; high-molecular-weight cytokeratin is often positive
Differential Diagnosis
-
♦
Squamous metaplasia
-
Lacks significant nuclear pleomorphism
-
-
♦
Metastatic squamous cell carcinoma
-
PSA and PAP negative
-
Sarcomatoid Carcinoma (Carcinosarcoma)
Clinical
-
♦
Often occurs in elderly patients with urinary obstructive symptoms
-
♦
Patients often have prior history of hormonal or radiation therapy
-
♦
Highly aggressive, with median survival of 12 months
-
♦
No differences in outcome for those with or without heterologous elements
Microscopic
-
♦
Considered Gleason pattern 5 adenocarcinoma (Fig. 38.40)
Fig. 38.40. 
Sarcomatoid carcinoma of the prostate.
-
♦
Spindle cell proliferation with epithelial differentiation
-
♦
Nuclear pleomorphism and numerous mitotic figures
-
♦
Heterologous components variable, including osteosarcoma, leiomyosarcoma, etc

Immunohistochemistry
-
♦
PSA and PAP are sometimes positive; broad-spectrum cytokeratin is positive
Differential Diagnosis
-
♦
Postoperative spindle cell nodule
-
Clinical history of prior surgery
-
Lacks significant nuclear pleomorphism
-
-
♦
Sarcoma
-
Lacks evidence of epithelial differentiation
-
Lymphoepithelioma-Like Carcinoma
-
♦
Histologic features: islands of closely packed glands set in a dense lymphocytic stroma (Fig. 38.41)
Fig. 38.41. 
Lymphoepithelioma-like carcinoma of the prostate.
-
♦
Very rare; unknown prognostic significance
-
♦
No association with Epstein-Barr virus

Cribriform Adenocarcinoma
-
♦
Collapsible fenestrations indicate Gleason pattern 3 cancer; near-solid rigid openings indicate Gleason pattern 4 cancer
-
♦
Main differential diagnostic consideration: extensive high-grade PIN
-
♦
Used as a descriptive term – not a specific entity
Adenocarcinoma with Glomeruloid Features
-
♦
Unique Gleason grade 3 pattern consisting of a tightly cohesive tuft of cancer cells within a larger malignant acinus reminiscent of a glomerulus (Fig. 38.42)
Fig. 38.42. 
Adenocarcinoma with glomeruloid features.

Atrophic Adenocarcinoma
-
♦
Occurs in up to 2% of contemporary needle biopsies
-
♦
Not considered to be a specific clinicopathologic entity
-
♦
Cancer consisting of acini with dilated lumens that may be mistaken for atrophy at low power (cancer mimicking atrophy) (Fig. 38.43)
Fig. 38.43. 
Atrophic adenocarcinoma. (A) Large acini lined by flattened epithelium reminiscent of atrophy. (B) Same focus as (A) immunostained for high-molecular-weight cytokeratin 34βE12. The absence of staining in the acini of concern confirms the diagnosis of malignancy. Note benign acini in the upper left acting as positive internal control for the staining reaction.
-
♦
Similar prognosis as conventional prostatic adenocarcinoma

Adenocarcinoma with Microvacuolated Cytoplasm (Foamy Gland Carcinoma)
-
♦
Abundant microvacuolated cytoplasm, often with small shrunken nuclei and nucleoli (Fig. 38.44)
Fig. 38.44. 
Microvacuolated (foamy gland) adenocarcinoma. The nuclei are often basally located and hyperchromatic, creating diagnostic difficulty.
-
♦
May be more aggressive (unconfirmed)
-
♦
May be difficult to diagnose due to similarity to mucinous metaplasia
-
♦
Usually mixed with typical acinar adenocarcinoma

Pseudohyperplastic Adenocarcinoma
-
♦
Resembles nodular hyperplasia (Fig. 38.45)
Fig. 38.45. 
Pseudohyperplastic adenocarcinoma. At low magnification, this focus could easily be misinterpreted as BPH. However, cytologic features and immunophenotype were diagnostic of malignancy. This focus is considered Gleason 1 + 1 = 2 adenocarcinoma.
-
♦
Negative for basal cell markers (high-molecular-weight cytokeratin [34βE12] and p63)
-
♦
Positive for α-methylacyl-CoA racemase (P504S)
-
♦
Uncommon, used as a descriptive term – not a specific entity

Adenoid Cystic/Basal Cell Carcinoma
Clinical
-
♦
Similar clinical presentation as typical acinar carcinoma
-
♦
Considered cancer of low malignant potential
-
♦
Serum PSA concentration not elevated
Microscopic
-
♦
Irregular and infiltrating nests of basal cells in a myxoid stroma (Fig. 38.46)
Fig. 38.46. 
Adenoid cystic/basal cell carcinoma.
-
♦
Predilection for perineural invasion
-
♦
Often coexistence of adenoid cystic pattern with rounded fenestrations and basaloid pattern with cell nests and peripheral palisading
-
♦
Elongated cells with crowding, stippled chromatin, and inconspicuous nucleoli
-
♦
May be associated with squamous differentiation and keratin production
-
♦
Two cell populations: peripheral basaloid cells and inner columnar ductal cells

Immunohistochemistry
-
♦
PSA and PAP may be positive; high-molecular-weight cytokeratin and p63 are positive
Differential Diagnosis
-
♦
Basal cell hyperplasia/adenoma
-
Solitary, well-circumscribed nodules associated with BPH
-
Uniformly distributed solid nests of hyperplastic basal cells
-
Condensed stroma at the periphery of nodules
-
Urothelial Carcinoma
Clinical
-
♦
Accounts for <1% of prostate cancers
-
♦
Patients present with hematuria and urinary obstructive symptoms
-
♦
Poor prognosis, with osteolytic bone metastasis; most die within 2 years of diagnosis
-
♦
Refractory to hormonal therapy
-
♦
Serum PSA concentration is normal
Microscopic
-
♦
Marked cytologic atypia with nuclear pleomorphism and high mitotic figures (Fig. 38.47)
Fig. 38.47. 
Urothelial (transitional cell) carcinoma of the prostate.
-
♦
Often associated with prominent stromal response and inflammatory background
-
♦
Dysplasia and carcinoma in situ common in adjacent urothelium
-
♦
Usually coexistent bladder cancer

Immunohistochemistry
-
♦
CEA is positive, PSA and PAP negative, high-molecular-weight cytokeratin (34βE12) positive, and cytokeratin 20 often positive
Differential Diagnosis
-
♦
Prostatic adenocarcinoma
-
Acinar differentiation with less nuclear pleomorphism
-
PSA and PAP positive, high-molecular-weight cytokeratin negative
-
-
♦
Inverted papilloma
-
Complex arborizing invagination with peripheral palisading
-
Lacks fibrovascular core
-
-
♦
HGPIN
-
PSA and PAP positive
-
Soft Tissue Tumors (Table 38.9)
Rhabdomyosarcoma
-
♦
Very rare, occurs mainly in children
-
♦
Embryonal) rhabdomyosarcoma is the most frequent type
-
♦
Sheets of immature spindle cells and occasional rhabdomyoblasts in myxoid stroma (Fig. 38.48)
Fig. 38.48. 
Rhabdomyosarcoma with an abundance of malignant rhabdomyoblasts.
-
♦
Myoglobin, MSA, and desmin positive; PSA and PAP negative

Leiomyosarcoma
Clinical
-
♦
Most common prostatic sarcoma in adults; accounts for 26% of all prostatic sarcomas
-
♦
Aggressive; usually recurs and results in death
Microscopic
-
♦
Similar to leiomyosarcoma of other sites
-
♦
Interlacing fascicles of spindle cells with eosinophilic cytoplasm and fusiform nuclei (Fig. 38.49)
Fig. 38.49. 
Leiomyosarcoma of the prostate.
-
♦
Necrosis, cytologic atypia, and increased number of mitotic figures

Immunohistochemistry
-
♦
Smooth muscle-specific actin and desmin positive
Differential Diagnosis
-
♦
Symplastic leiomyoma
-
Multinuclear giant cells and bizarre cells with nuclear degeneration
-
Mitotic figures inconspicuous
-
-
♦
Stromal hyperplasia with atypical giant cells
-
Bizarre hyperchromatic nuclei with inconspicuous nucleoli, rarely vacuolated
-
No mitotic figures or necrosis
-
-
♦
Postoperative spindle cell nodule
-
Small size of lesion
-
Fascicles of relative uniform spindle cells in a myxoid stroma
-
Cells with abundant cytoplasm
-
Enlarged nuclei with fine granular chromatin and prominent nucleoli
-
Mitotic figures may be frequent
-
Lacks atypical mitotic figures and nuclear pleomorphism
-
Prominent vasculature and associated with inflammation
-
-
♦
Blue nevi
-
Pigmented dendritic bipolar cells in fibrous stroma
-
Phyllodes Tumor
Clinical
-
♦
Patients usually present with urinary obstructive symptoms
-
♦
Potentially aggressive and often recurrent
-
♦
May dedifferentiate after recurrence (stromal overgrowth)
-
♦
Histogenesis is uncertain
Macroscopic
-
♦
Cystic and spongy tumor with prostatic enlargement, similar to BPH
Microscopic
-
♦
Biphasic growth of stromal and epithelial components
-
♦
Interlacing fascicles of spindle cells with leaflike projections into duct-like spaces (Fig. 38.50)
Fig. 38.50. 
Phyllodes tumor. Leaflike projections with a benign proliferation of epithelium and stroma.
-
♦
Increased stromal cellularity and overgrowth with compressed, elongated channels
-
♦
Uniform nuclei with inconspicuous nucleoli
-
♦
Grading is not reliable for predicting recurrence
-
♦
May undergo sarcomatous transformation after recurrence (stromal overgrowth)

Immunohistochemistry
-
♦
Stroma: actin and vimentin positive, desmin and S-100 protein negative
-
♦
Luminal epithelial cells: PSA, PAP, and keratin positive
Differential Diagnosis
-
♦
Stromal hyperplasia with atypical giant cells
-
Increased stromal cellularity and nuclear atypia
-
Bizarre cells with nuclear degenerative change
-
Associated with BPH
-
-
♦
Nodular hyperplasia with fibroadenoma-like areas
-
Cystically dilated acini associated with hyperplastic epithelium
-
-
♦
Multilocular prostatic cystadenoma
-
Epithelial cell-lined cyst in a fibrous stroma
-
Lacks stromal cellularity
-
-
♦
Leiomyosarcoma
-
Lacks biphasic growth pattern of phyllodes tumor
-
-
♦
Seminal vesicle cyst (lateral location) and Müllerian duct cyst (midline location)
-
Unilocular cyst
-
No stromal cellularity
-
PSA and PAP negative
-
Lymphoma
Clinical
-
♦
Occurs in elderly patients presenting with urinary obstructive symptoms
-
♦
Secondary involvement more common than primary involvement (55% vs. 35%)
-
♦
Poor prognosis (median survival = 23–28 months) regardless of age, histologic type, treatment, clinical stage at presentation, or type of involvement (primary vs. secondary)
-
♦
Criteria for the diagnosis of primary lymphoma
-
Absence of hematopoietic involvement (spleen, lymph nodes, peripheral blood, or liver) within 1 month prior to diagnosis
-
Limited to the prostate and adjacent soft tissue
-
Macroscopic
-
♦
Diffusely enlarged with firm to rubbery consistency
Microscopic
-
♦
Diffuse large cell and small lymphocytic lymphoma are the two most common types
-
♦
Diffuse irregular infiltrates of monotonous lymphocytes (Fig. 38.51)
Fig. 38.51. 
Small lymphocytic lymphoma involving the prostate.
-
♦
Preservation of acini

Differential Diagnosis
-
♦
Granulomatous prostatitis
-
Acinar destruction with polymorphous inflammatory infiltrate
-
Treatment Effects
Androgen Deprivation Therapy
Benign
-
♦
Acinar atrophy and distortion
-
♦
Decreased ratio of acini to stroma, with stromal fibrosis and hyalinization (Fig. 38.52)
Fig. 38.52. 
After hormonal treatment, benign prostatic tissue shows acinar destruction, stromal fibrosis, mucin pools, and calcifications.
-
♦
ABCH, squamous metaplasia, and urothelial metaplasia
-
♦
Acinar rupture with preservation of basal cell layer
-
♦
Cytoplasmic vacuolization and nuclear shrinkage

Cancer
-
♦
Linear arrays and ragged infiltrate of malignant acini with cytoplasmic vacuolization, nuclear pyknosis, and hyperchromasia (Fig. 38.53)
Fig. 38.53. 
Androgen deprivation therapy -treated adenocarcinoma. (A) Needle biopsy contains numerous minute nests of malignant cells with small nuclei and abundant clear cytoplasm. These nests stand in contrast with the large adjacent atrophic acini. (B) Brown staining indicated PSA immunoreactivity in the cytoplasm of most of the malignant cells, confirming prostatic epithelial origin. (C) Immunostain for high-molecular-weight cytokeratin 34βE12 reveals an absence of staining in the malignant acini. Benign acini are positive.
-
♦
Nucleoli may be inconspicuous
-
♦
Malignant glands are often dilated, with atrophic features and a hemangiopericytoma-like pattern
-
♦
Lacks basal cell layer
-
♦
Reduced incidence and extent of HGPIN

Immunohistochemistry
-
♦
PSA positive, PAP positive, high-molecular-weight cytokeratin (34βE12) and p63 negative, racemase (P504S) positive (cancer) (Fig. 38.53)
Differential Diagnosis
-
♦
Clear cell change may be seen in the following lesions
-
AAH
-
Cribriform hyperplasia
-
Basal cell hyperplasia
-
Cowper glands
-
Mucinous metaplasia
-
Paraganglion
-
Xanthoma and xanthogranulomatous prostatitis
-
Metabolic storage disease
-
Sclerosing adenosis
-
Radiation Therapy
Benign
-
♦
Lobular and acinar atrophy, decreased acini to stroma ratio, stromal edema, and fibrosis
-
♦
ABCH (Fig. 38.54), squamous and transitional cell metaplasia
Fig. 38.54. 
Radiation change of the benign prostatic epithelium initially misdiagnosed as adenocarcinoma. There are marked nuclear abnormalities, including variation in size and shape and hyperchromasia.
-
♦
Acinar rupture with extravasation, dystrophic calcification
-
♦
Vascular myointimal proliferation
-
♦
Cytoplasmic clearing with nuclear pyknosis

Cancer
-
♦
Linear arrays and ragged infiltrate of malignant acini with cytoplasmic vacuolization, nuclear pyknosis, and hyperchromasia (Fig. 38.55)
Fig. 38.55. 
Prostatic adenocarcinoma after radiation therapy (A and B). Individual cancer cells may be difficult to distinguish from atypical basal cells. Immunostaining for PIN4 were helpful for the diagnosis; high-molecular-weight cytokeratin 34βE12 (brown, cytoplasmic), P504/racemase (red), and p63 (brown, nuclear).
-
♦
Nucleoli may be inconspicuous
-
♦
Lacks basal cell layer
-
♦
Reduced incidence and extent of HGPIN
-
♦
Grading of salvage prostatectomy specimens is predictive of survival

Immunohistochemistry
-
♦
PSA positive, PAP positive, high-molecular-weight cytokeratin (34βE12) and p63 negative, racemase (P504S) positive (cancer) (Fig. 38.55)
TNM Classification of Prostate Cancer (2010 Revision)
-
♦
Primary Tumor (T)
-
Clinical
-
TX: Primary tumor cannot be assessed
-
T0: No evidence of primary tumor
-
T1: Clinically inapparent tumor neither palpable nor visible by imaging
-
T1a: Tumor incidental histologic finding in 5% or less of tissue resected
-
T1b: Tumor incidental histologic finding in more than 5% of tissue resected
-
T1c: Tumor identified by needle biopsy (e.g., because of elevated PSA)
-
T2: Tumor confined within prostate*
-
T2a: Tumor involves one-half of lobe or less
-
T2b: Tumor involves more than one-half of one lobe, but not both lobes
-
T2c: Tumor involves both lobes
-
T3: Tumor extends through the prostate capsule**
-
T3a: Extracapsular extension (unilateral or bilateral)
-
T3b: Tumor invades seminal vesicle(s)
-
T4: Tumor is fixed or invades adjacent structures other than seminal vesicles; such as external sphincter, rectum, bladder, levator muscles, and/or pelvic wall
-
-
Pathologic
-
•
pT2: Organ confined
-
•
pT2a: Unilateral, one-half of one side or less
-
•
pT2b: Unilateral, involving more than one-half of side but not both sides
-
•
pT2c: Bilateral disease
-
•
pT3a: Extraprostatic extension or microscopic invasion of bladder neck***
-
•
pT3b: Seminal vesicle invasion
-
•
pT4: Invasion of rectum, levator muscle, and/or pelvic wall
-
•
-
-
♦
Regional Lymph Nodes (N)
-
Clinical
-
•
NX: Regional lymph nodes were not assessed
-
•
N0: No regional lymph node metastasis
-
•
N1: Metastasis in regional lymph node(s)
-
Pathologic
-
•
pNX: Regional nodes not sampled
-
•
pN0: No positive regional nodes
-
•
pN1: Metastases in regional node(s)
-
-
♦
Distant Metastasis (M)****
-
M0: No distant metastasis
-
M1: Distant metastasis
-
M1a: Nonregional lymph node(s)
-
M1b: Bone(s)
-
M1c: Other site(s) with or without bone disease
-
Stage Groupings (Combining TNM with Serum PSA and Gleason Grade)
-
♦
Stage I
-
T1, N0, M0, Gleason grade 6 or less, PSA less than 10
-
T2a, N0, M0, Gleason grade 6 or less, PSA less than 10
-
-
♦
Stage IIA
-
T1, N0, M0, Gleason grade of 7, PSA less than 20
-
T1, N0, M0, Gleason grade of 6 or less, PSA at least 10 but less than 20
-
T2a or T2b, N0, M0, Gleason grade of 7 or less, PSA less than 20
-
-
♦
Stage IIB
-
T2c, N0, M0, any Gleason grade, any PSA
-
T1 or T2, N0, M0, any Gleason grade, PSA of 20 or more
-
T1 or T2, N0, M0, Gleason grade of 8 or higher, any PSA
-
-
♦
Stage III
-
T3, N0, M0, any Gleason grade, any PSA
-
-
♦
Stage IV
-
T4, N0, M0, any Gleason grade, any PSA
-
Any T, N1, M0, any Gleason grade, any PSA
-
Any T, any N, M1, any Gleason grade, any PSA
-
Suggested Reading
Agarwala SS. An update on pegylated IFN-alpha2b for the adjuvant treatment of melanoma. Expert Rev Anticancer Ther. 2012;12:1449–59.
Alexander RE, Sung MT, Cheng L. Lymphadenectomy in urologic oncology: pathologic considerations. Urol Clin North Am. 2011;38:483–95.
Arora R, Koch MO, Eble JN, et al. Heterogeneity of Gleason grade in multifocal adenocarcinoma of the prostate. Cancer. 2004;100:362–2366.
Attard G, Parker C, Eeles RA, et al. Prostate cancer. Lancet. 2015.
Biermann K, Montironi R, Lopez-Beltran A, Zhang S, Cheng L. Histopathological findings after treatment of prostate cancer using high-intensity focused ultrasound (HIFU). Prostate. 2010;70:1196–200.
Bock BJ, Bostwick DG. Does prostatic ductal adenocarcinoma exist? Am J Surg Pathol. 1999;23:781–5.
Bostrom PJ, Bjartell AS, Catto JW, et al. Genomic predictors of outcome in prostate cancer. Eur Urol. 2015;68:1033–44.
Bostwick DG. Prospective origins of prostate carcinoma: prostatic intraepithelial neoplasia and atypical adenomatous neoplasia. Cancer. 1996;78:330–6.
Bostwick DG. Evaluating prostate needle biopsy: therapeutic and prognostic importance. CA Cancer J Clin. 1997;47:297–319.
Bostwick DG, Cheng L. Overdiagnosis of prostatic adenocarcinoma. Semin Urol Oncol. 1999;17:199–205.
Bostwick DG, Cheng L. Precursors of prostate cancer. Histopathology. 2012;60:4–27.
Bostwick DG, Cheng L. Urologic surgical pathology. 3rd ed. Philadelphia, PA: Elsevier/Saunders; 2014.
Bostwick DG, Ma J. Over-diagnosis of high grade prostatic intraepithelial neoplasia: a prospective study of 251 cases. BJU Int. 2007;100:1036–9.
Bostwick DG, Meiers I. Diagnosis of prostatic carcinoma after therapy. Arch Pathol Lab Med. 2007;131:360–71.
Bostwick DG, Shan A, Qian J, et al. Independent origin of multiple foci of prostatic intraepithelial neoplasia (PIN): comparison with matched foci of prostate cancer. Cancer. 1998;83:1995–2002.
Bostwick DG, Qian J, Ma J, et al. Mesonephric remnants of the prostate: incidence and histologic spectrum. Mod Pathol. 2003;16:630–5.
Bostwick DG, Hossain D, Qian J, et al. Phyllodes tumor of the prostate: long-term followup study of 23 cases. J Urol. 2004;172:894–9.
Cheng L, Bostwick DG. Atypical sclerosing adenosis of the prostate: a rare mimic of adenocarcinoma. Histopathology. 2010;56:627–31.
Cheng L, Bergstralh E, Cheville JC, et al. Cancer volume of lymph node metastases predicts progression in prostate cancer. Am J Surg Pathol. 1998a;22:1491–500.
Cheng L, Neumann RM, Blute ML, et al. Long-term follow-up of untreated stage T1a prostate cancer. J Natl Cancer Inst. 1998b;90:1105–7.
Cheng L, Sebo TJ, Slezak J, et al. Predictors of survival in prostate cancer patients treated with salvage prostatectomy after radiation therapy. Cancer. 1998c;83:2164–71.
Cheng L, Shan A, Cheville JC, et al. Atypical adenomatous hyperplasia of the prostate: a premalignant lesion? Cancer Res. 1998d;58:389–91.
Cheng L, Song SY, Pretlow TG, et al. Evidence of independent origin of multiple tumors from prostate cancer patients. J Natl Cancer Inst. 1998e;90:233–7.
Cheng L, Bergstralh EJ, Schere BG, et al. Predictors of cancer progression in T1a prostate adenocarcinoma. Cancer. 1999a;85:1300–4.
Cheng L, Bergstralh EJ, Slezak J, et al. Dedifferentiation in metastatic progression of prostate cancer. Cancer. 1999b;86:657–63.
Cheng L, Bostwick DG, Guang L, et al. Allelic imbalance in the clonal evolution of prostate cancer. Cancer. 1999c;85:2017–22.
Cheng L, Cheville JC, Bostwick DG. Diagnosis of prostate cancer in needle biopsies after radiation therapy. Am J Surg Pathol. 1999d;23:1173–83.
Cheng L, Cheville JC, Pisansky TM, et al. Prevalence and distribution of prostatic intraepithelial neoplasia in salvage radical prostatectomy specimens after radiation therapy. Am J Surg Pathol. 1999e;23:803–8.
Cheng L, Darson MF, Bergstralh EJ, et al. Correlation of margin status and extraprostatic extension with progression of prostate carcinoma. Cancer. 1999f;86:1775–82.
Cheng L, Pisansky TM, Ramnani DM, et al. Extranodal extension in lymph node-positive prostate cancer. Mod Pathol. 2000a;13:113–8.
Cheng L, Slezak J, Bergstralh EJ, et al. Preoperative prediction of surgical margin status in prostate cancer patients treated by radical prostatectomy. J Clin Oncol. 2000b;18:2862–8.
Cheng L, Zincke H, Blute ML, Bergstralh EJ, Scherer B, Bostwick DG. Risk of prostate carcinoma death in patients with lymph node metastasis. Cancer. 2001a;91:66–73.
Cheng L, Zincke H, Blute ML, et al. Risk of prostate cancer death in patients with lymph node metastasis. Cancer. 2001b;91:66–73.
Cheng L, Jones TD, Lin H, et al. Lymphovascular invasion is an independent prognostic factor in prostatic adenocarcinoma. J Urol. 2005a;174:2181–5.
Cheng L, Jones TD, Pan CX, Barbarin A, Eble JN, Koch MO. Anatomic distribution and pathologic characterization of small-volume prostate cancer (<0.5 ml) in whole-mount prostatectomy specimens. Mod Pathol. 2005b;18:1022–6.
Cheng L, Koch MO, Juliar BE, et al. The combined percentage of Gleason patterns 4 and 5 is the best predictor of cancer progression after radical prostatectomy. J Clin Oncol. 2005c;23:2911–7.
Cheng L, Poulos CK, Pan CX, et al. Preoperative prediction of small volume cancer (less than 0.5-ml) in radical prostatectomy specimens. J Urol. 2005d;174:898–902.
Cheng L, Davidson DD, Lin H, Koch MO. Percentage of Gleason pattern 4 and 5 predicts survival after radical prostatectomy. Cancer. 2007;110:1967–72.
Cheng L, MacLennan GT, Abdul-Karim FW, et al. Eosinophilic metaplasia of the prostate: a newly described lesion distinct from other eosinophilic changes in prostatic epithelium. Anal Quant Cytol Histol. 2008;30:226–30.
Cheng L, Montironi R, Bostwick DG, Lopez-Beltran A, Berney DM. Staging of prostate cancer. Histopathology. 2012;60:87–117.
Cheng L, Davidson DD, Maclennan GT, et al. Atypical adenomatous hyperplasia of prostate lacks TMPRSS2-ERG gene fusion. Am J Surg Pathol. 2013;37:1550–4.
Edge SB, American Joint Committee on Cancer. AJCC cancer staging manual. 7th ed. New York: Springer; 2010.
Eichelberger LE, Cheng L. Does pT2b prostate carcinoma exist? Critical appraisal of the 2002 TNM classification of prostate carcinoma. Cancer. 2004;100:2573–6.
Eichelberger LE, Koch MO, Eble JN, Ulbright TM, Juliar BE, Cheng L. Maximum tumor diameter is an independent predictor of prostate-specific antigen recurrence in prostate cancer. Mod Pathol. 2005;18:886–90.
Emerson RE, Koch MO, Daggy JK, Cheng L. Closest distance between tumor and resection margin in radical prostatectomy specimens: lack of prognostic significance. Am J Surg Pathol. 2005;29:225–9.
Epstein JI, Allsbrook Jr WC, Amin MB, Egevad LL. The 2005 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason grading of prostatic carcinoma. Am J Surg Pathol. 2005;29:1228–42.
Epstein JI, Amin MB, Beltran H, et al. Proposed morphologic classification of prostate cancer with neuroendocrine differentiation. Am J Surg Pathol. 2014a;38:756–67.
Epstein JI, Egevad L, Amin MB, et al. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System. Am J Surg Pathol. 2015.
Epstein JI, Egevad L, Humphrey PA, Montironi R. Members of the IIiDUPG. Best practices recommendations in the application of immunohistochemistry in the prostate: report from the International Society of Urologic Pathology consensus conference. Am J Surg Pathol. 2014c;38:e6–19.
Fisher KW, Montironi R, Lopez Beltran A, et al. Molecular foundations for personalized therapy in prostate cancer. Curr Drug Targets. 2015;16:103–14.
Galosi AB, Mazzucchelli R, Scarpelli M, et al. Solitary fibrous tumour of the prostate identified on needle biopsy. Eur Urol. 2009;56:564–7.
Halat S, Eble JN, Grignon DJ, et al. Ectopic prostatic tissue: histogenesis and histopathological characteristics. Histopathology. 2011;58:750–8.
Hattab EM, Koch MO, Eble JN, Lin H, Cheng L. Tertiary Gleason pattern 5 is a powerful predictor of biochemical relapse in patients with Gleason score 7 prostatic adenocarcinoma. J Urol. 2006;175:1695–9.
Hong H, Koch MO, Foster RS, et al. Anatomic distribution of periprostatic adipose tissue: a mapping study of 100 radical prostatectomy specimens. Cancer. 2003;97:1639–43.
Hossain D, Meiers I, Qian J, MacLennan GT, Bostwick DG. Prostatic stromal hyperplasia with atypia: follow-up study of 18 cases. Arch Pathol Lab Med. 2008;132:1729–33.
Iczkowski KA, Egevad L, Ma J, et al. Intraductal carcinoma of the prostate: interobserver reproducibility survey of 39 urologic pathologists. Ann Diagn Pathol. 2014;18:333–42.
Lopez-Beltran A, Cheng L, Prieto R, Bianca A, Montironi R. Lymphoepithelioma-like carcinoma of the prostate. Hum Pathol. 2009;40:982–7.
Marks RA, Koch MO, Lopez-Beltran A, Montironi R, Juliar BE, Cheng L. Relationship between the extent of surgical margin positivity and prostate-specific antigen recurrence in radical prostatectomy specimens. Hum Pathol. 2007a;38:1207–11.
Marks RA, Lin H, Koch MO, Cheng L. Positive-block ratio in radical prostatectomy specimens is an independent predictor of prostate-specific antigen recurrence. Am J Surg Pathol. 2007b;31:311–8.
Mazzucchelli R, Lopez-Beltran A, Cheng L, et al. Rare and unusual histological variants of prostatic carcinoma: clinical significance. BJU Int. 2009a;102:1369–74.
Mazzucchelli R, Morichetti D, Lopez-Beltran A, et al. Neuroendocrine tumours of the urinary system and male genital organs: clinical significance. BJU Int. 2009b;103:1464–70.
Mazzucchelli R, Lopez-Beltran A, Galosi AB, et al. Prostate changes related to therapy: with special reference to hormone therapy. Future Oncol. 2014;10:1873–86.
Moch H, Humphrey PA, Ulbright TM, Reuter VE. Classification of tumours of the urinary system and male genital organs. Lyon: International Agency for Research on Cancer (IARC) Press; 2016.
Montironi R, Scattoni V, Mazzucchelli R, et al. Atypical foci suspicious but not diagnostic of malignancy in prostate needle biopsies (also referred to as “atypical small acinar proliferation suspicious for but not diagnostic of malignancy”). Eur Urol. 2006;50:666–74.
Montironi R, Cheng L, Scarpelli M, et al. Pathological reflection on European Urology: extended, saturation, and systematic prostate biopsies. Eur Urol. 2008;53:1111–4.
Montironi R, Cheng L, Lopez-Beltran A, et al. Stage pT0 in radical prostatectomy with no residual carcinoma and with a previous positive biopsy conveys a wrong message to clinicians and patients: why is cancer not present in the radical prostatectomy specimen? Eur Urol. 2009a;56:272–4.
Montironi R, Cheng L, Lopez-Beltran A, et al. Joint appraisal of the radical prostatectomy specimens by the urologist and uropathologist. Eur Urol. 2009b;56:951–5.
Montironi R, Cheng L, Mazzucchelli R, et al. Critical pathological evaluation of the prostate from cystoprostatectomies for bladder cancer: insights from a complete sampling with the whole mount technique. Eur Urol. 2009c;55:1305–9.
Montironi R, Cheng L, Lopez-Beltran A, et al. Original Gleason System versus 2005 ISUP Modified Gleason System. Eur Urol. 2010;58:369–73.
Montironi R, Scarpelli M, Cheng L, Lopez-Beltran A, Zhou M, Montorsi F. Do not misinterpret intraductal carcinoma of the prostate as high-grade prostatic intraepithelial neoplasia! Eur Urol. 2012a;62:518–22.
Montironi R, Scarpelli M, Mazzucchelli R, Cheng L, Lopez-Beltran A, Montorsi F. Extent of cancer of less than 50% in any prostate needle biopsy core: how many millimeters are there? Eur Urol. 2012b;61:751–6.
Montironi R, Lopez-Beltran A, Cheng L, Montorsi F, Scarpelli M. Central prostate pathology review: should it be mandatory? Eur Urol. 2013;64:199–201.
Montironi R, Lopez-Beltran A, Cheng L, Galosi AB, Montorsi F, Scarpelli M. Seminal vesicle intraepithelial neoplasia versus basal cell hyperplasia in a seminal vesicle. Eur Urol. 2014;66:623–7.
Montironi R, Cheng L, Lopez-Beltran A, Scarpelli M, Montorsi F. A better understating of the morphological features and molecular characteristics of intraductal carcinoma helps clinicians further explain prostate cancer aggressiveness. Eur Urol. 2015;67:504–7.
Netto GJ, Cheng L. Emerging critical role of molecular testing in diagnostic genitourinary pathology. Arch Pathol Lab Med. 2012;136:372–90.
Ng JC, Koch MO, Daggy JK, Cheng L. Perineural invasion in radical prostatectomy specimens: lack of prognostic significance. J Urol. 2004;172:2249–51.
Poulos CK, Daggy JK, Cheng L. Prostate needle biopsies: multiple variables are predictive of final tumor volume in radical prostatectomy specimens. Cancer. 2004a;101:527–32.
Poulos CK, Koch MO, Eble JN, Daggy JK, Cheng L. Bladder neck invasion is an independent predictor of prostate-specific antigen recurrence. Cancer. 2004b;101:1563–8.
Poulos CK, Daggy JK, Cheng L. Preoperative prediction of Gleason grade in radical prostatectomy specimens: the influence of different Gleason grades from multiple positive biopsy sites. Mod Pathol. 2005;18:228–34.
Santoni M, Piva F, Scarpelli M, et al. The origin of prostate metastases: emerging insights. Cancer Metastasis Rev. 2015a;34:765–73.
Santoni M, Scarpelli M, Mazzucchelli R, et al. Current histopathologic and molecular characterisations of prostate cancer: towards individualised prognosis and therapies. Eur Urol. 2015.
Seipel AH, Delahunt B, Samaratunga H, et al. Diagnostic criteria for ductal adenocarcinoma of the prostate: interobserver variability among 20 expert uropathologists. Histopathology. 2014;65:216–27.
Shah RB, Li J, Cheng L, et al. Diagnosis of Gleason pattern 5 prostate adenocarcinoma on core needle biopsy: an interobserver reproducibility study among urologic pathologists. Am J Surg Pathol. 2015;39:1242–9.
Simper NB, Jones CL, MacLennan GT, et al. Basal cell carcinoma of the prostate is an aggressive tumor with frequent loss of PTEN expression and overexpression of EGFR. Hum Pathol. 2015;46:805–12.
Srigley JR, Amin MB, Epstein JI, et al. Updated protocol for the examination of specimens from patients with carcinomas of the prostate gland. Arch Pathol Lab Med. 2006;130:936–46.
Sung MT, Cheng L. Contemporary approaches for processing and handling of radical prostatectomy specimens. Histol Histopathol. 2010;25:259–65.
Sung MT, Eble JN, Cheng L. Invasion of fat justifies assignment of stage pT3a in prostatic adenocarcinoma. Pathology. 2006;38:309–11.
Sung MT, Lin H, Koch MO, Davidson DD, Cheng L. Radial distance of extraprostatic extension measured by ocular micrometer is an independent predictor of prostate-specific antigen recurrence: a new proposal for the substaging of pT3a prostate cancer. Am J Surg Pathol. 2007;31:311–8.
Van der Kwast TH, Evans A, Lockwood G, et al. Variability in diagnostic opinion among pathologists for single small atypical foci in prostate biopsies. Am J Surg Pathol. 2010;34:169–77.
Wang L, Davidson DD, Montironi R, et al. Small cell carcinoma of the prostate: molecular basis and clinical implications. Histol Histopathol. 2015;30:413–24.
Wilkerson ML, Lin F, Liu H, Cheng L. The application of immunohistochemical biomarkers in urologic surgical pathology. Arch Pathol Lab Med. 2014;138:1643–65.
Williamson SR, Cheng L. Prostate cancer: effects of tertiary Gleason pattern 5 on oncological outcome. Nat Rev Urol. 2015;12:188–9.
Williamson SR, Zhang S, Yao JL, et al. ERG-TMPRSS2 rearrangement is shared by concurrent prostatic adenocarcinoma and prostatic small cell carcinoma and absent in small cell carcinoma of the urinary bladder: evidence supporting monoclonal origin. Mod Pathol. 2011;24:1120–7.
Zhang C, Montironi R, MacLennan GT, et al. Is atypical adenomatous hyperplasia of the prostate a precursor lesion? Prostate. 2011;71:1746–51.
Zhou M, Li J, Cheng L, et al. Diagnosis of “Poorly Formed Glands” Gleason Pattern 4 Prostatic Adenocarcinoma on Needle Biopsy: An Interobserver Reproducibility Study Among Urologic Pathologists With Recommendations. Am J Surg Pathol. 2015;39:1331–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Bostwick, D.G., Cheng, L. (2016). Prostate. In: Cheng, L., Bostwick, D. (eds) Essentials of Anatomic Pathology. Springer, Cham. https://doi.org/10.1007/978-3-319-23380-2_38
Download citation
DOI: https://doi.org/10.1007/978-3-319-23380-2_38
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-23379-6
Online ISBN: 978-3-319-23380-2
eBook Packages: MedicineMedicine (R0)