
Abstract
Cancer is not a modern disease but has clearly existed for many centuries. It is however a more common phenomenon nowadays than previously due to the increase of the world’s population and the relatively advanced age to which people now live, since it is a disease that is more common in elderly ages than in younger ages (World Cancer Report 2008).
The burden of cancer worldwide is continuously rising largely because of the age and growth of the world population alongside an increasing adoption of cancer-causing behaviors, particularly smoking, physical inactivity, and “westernized” lifestyle in economically developing countries. Based on the GLOBOCAN 2008 estimates, about 12.7 million cancer cases and 7.6 million cancer deaths are estimated to have occurred in 2008; of these, 56 % of the cases and 64 % of the deaths occurred in the economically developing world. Cancer is the leading cause of death in economically developed countries and the second leading cause of death in developing countries (CA Cancer J Clin 61:69–90. CV2011 American Cancer Society, Inc., 2011). Breast cancer is the most frequently diagnosed cancer and the leading cause of cancer death among females, accounting for 23 % of the total cancer cases and 14 % of the cancer deaths. Lung cancer is the leading cancer site in males, comprising 17 % of the total new cancer cases and 23 % of the total cancer deaths. Breast cancer is now also the leading cause of cancer death among females in economically developing countries, a shift from the previous decade during which the most common cause of cancer death was cervical cancer. Further, the mortality burden for lung cancer among females in developing countries is as high as the burden for cervical cancer, with each accounting for 11 % of the total female cancer deaths. Although overall cancer incidence rates in the developing world are half those seen in the developed world in both sexes, the overall cancer mortality rates are generally similar. Cancer survival tends to be poorer in developing countries, most likely because of a combination of a late stage at diagnosis and limited access to timely and standard treatment. A substantial proportion of the worldwide burden of cancer could be prevented through the application of existing cancer control knowledge and by implementing programs for tobacco control, vaccination (for liver and cervical cancers), and early detection and treatment, as well as public health campaigns promoting physical activity and a healthier dietary intake. Clinicians, public health professionals, and policy makers can play an active role in accelerating the application of such interventions globally (CA Cancer J Clin 61:69–90. CV2011 American Cancer Society, Inc., 2011) (Fig. 19.1).
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Health care costs
- Health care demands
- Oncology
- Registry
- Screening
- New cancer cases
- Strategy
- Palliative care
- UAE
Introduction
Cancer is not a modern disease but has clearly existed for many centuries. It is however a more common phenomenon nowadays than previously due to the increase of the world’s population and the relatively advanced age to which people now live, since it is a disease that is more common in elderly ages than in younger ages [1].
The burden of cancer worldwide is continuously rising largely because of the aging and growth of the world population alongside an increasing adoption of cancer-causing behaviors, particularly smoking, physical inactivity, and “westernized” lifestyle in economically developing countries. Based on the GLOBOCAN 2008 estimates, about 12.7 million cancer cases and 7.6 million cancer deaths are estimated to have occurred in 2008; of these, 56 % of the cases and 64 % of the deaths occurred in the economically developing world. Cancer is the leading cause of death in economically developed countries and the second leading cause of death in developing countries [2]. Breast cancer is the most frequently diagnosed cancer and the leading cause of cancer death among females, accounting for 23 % of the total cancer cases and 14 % of the cancer deaths. Lung cancer is the leading cancer site in males, comprising 17 % of the total new cancer cases and 23 % of the total cancer deaths. Breast cancer is now also the leading cause of cancer death among females in economically developing countries, a shift from the previous decade during which the most common cause of cancer death was cervical cancer. Further, the mortality burden for lung cancer among females in developing countries is as high as the burden for cervical cancer, with each accounting for 11 % of the total female cancer deaths. Although overall cancer incidence rates in the developing world are half those seen in the developed world in both sexes, the overall cancer mortality rates are generally similar. Cancer survival tends to be poorer in developing countries, most likely because of a combination of a late stage at diagnosis and limited access to timely and standard treatment. A substantial proportion of the worldwide burden of cancer could be prevented through the application of existing cancer control knowledge and by implementing programs for tobacco control, vaccination (for liver and cervical cancers), and early detection and treatment, as well as public health campaigns promoting physical activity and a healthier dietary intake. Clinicians, public health professionals, and policy makers can play an active role in accelerating the application of such interventions globally [2] (Fig. 19.1).

Estimated new cancer cases and deaths worldwide for leading cancer sites by level of economic development. Source: GLOBOCAN 2012
The World Health Organization (WHO) projected that by 2030, the cancer figures could increase to 26.4 million new cases and 17 million cancer-related deaths. The majority of the global cancer burden is shifting from the more developed world to economically disadvantaged countries. Nearly 70 % of cancer incidence will occur in economically disadvantaged countries, where survival rates are less than half of those in developed countries. Population growth and aging are the largest contributors to the increasing numbers of cancer cases in low- and middle-income countries. The population aged 65 and over in low- and middle-income countries is expected to increase from 247 million to 982 million between 2000 and 2050, due to increased attention and resources to combat HIV/AIDS and other infectious diseases [2].
The United Arab Emirates (UAE) is a rapidly developing country composed of a multinational population with varying educational backgrounds, religious beliefs, and cultural practices, which pose a challenge for population-based public health strategies. A number of public health issues significantly contribute to morbidity and mortality in the UAE.
The UAE has a highly developed health service, including a sophisticated physical infrastructure of well-equipped hospitals, specialized clinics, and primary care centers. Health care is free for all nationals, and there is a compulsory health insurance scheme in place in Abu Dhabi to cover all residents. The scheme will be extended country-wide.
Currently, there are 65 hospitals in the UAE, 15 of them federal institutions, and over 150 primary health care centers and clinics, in addition to 11 school health centers, 10 centers for mothers and children, and 110 special units for mothers and children in hospitals and primary health care centers. This is compared with 7 hospitals and 12 health centers when the Federation was established in 1971.
Nevertheless, as the population increases and health care demands burgeon, Government policies and strategies, such as Emirates Vision 2021 and the Strategy of the Government of the United Arab Emirates 2011–2013, are committed to make continuing improvements to health care, including remote areas.
UAE Demographics and Population Growth
In Abu Dhabi; one of the seven UAE emirates and the capital; every individual is entitled access to health care and health insurance is mandatory in all emirates, and many elements are being implemented to provide world-class quality health care. Population growth is the product of natural growth and net migration [2]. Migrant workers are recruited from all over the world to satisfy the manpower demands of the fast-paced economic and industrial developments in the UAE [3]. Consequently, the UAE population has increased substantially primarily due to the high inward migration of expatriate workers (4.1 million in 2005, 8.3 million in 2010) [4]. Indeed, mass recruitment of migrant workers has created an unusual population structure; with the total UAE population composed of approximately 11 % (950,000) Emiratis, and the rest are expatriates of varying nationalities [5]. Similarly, the total population of Abu Dhabi (the largest emirate in the UAE) is estimated to be 2.3 million, with over half of the population being expatriate males’ aged 20–59 years [5].
As a result of expatriate workforce recruitment for industrial projects, males outnumber females 3:1 in the overall UAE population (nationals and non-nationals); however, there are approximately equal numbers of male and female UAE nationals. Among non-nationals, the ratio of males to females is 3.7:1 due to the imbalance between the number of expatriate males employed in construction compared with migrant females working in hospitality, health care, or domestic service [2]. As such, the UAE is composed of a multinational population, with varying educational backgrounds, religious beliefs, and cultural practices, which pose a challenge for population-based public health strategies.
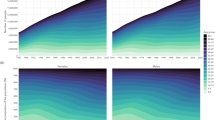
In 2013, HAAD has presented estimates of population growth in Abu Dhabi emirates for both the nationals and expatriates as seen in Fig. 19.2.

Population estimates here are based on raw insurance data; projections are rounded to the nearest 2.5 % variance between high and low, and those for expatriates at 5 %. Source: Health Statistics 2013; HAAD (Health Authority—Abu Dhabi)
Cancer Status in UAE
Cancer is the second leading cause of death worldwide and in all regions of the world. Historically, the UAE had a much lower incidence of cancer than Western countries; however, over the last 40 years, it has undergone a period of dramatic economic, social, and demographic change, resulting in increased life expectancy and prosperity. This epidemiological transition has led to significant increases in the incidence of all chronic noncommunicable diseases, including cancer, which is now the third leading cause of death in the UAE (after cardiovascular disease and injury) causing 10 % of all deaths in 2010 and 16 % of all deaths in the emirate of Abu Dhabi during the same year [6]. At present, there is no national or regional population-based cancer registry in the UAE, which means there is no reliable information available on the incidence of cancer in the UAE. However, the Ministry of Health collected some cancer registration data for the UAE, which has been submitted for inclusion in the Globocan database [7] and Gulf Cooperation Council-wide cancer registry report, “Ten Year Cancer Incidence Among Nationals of the GCC States 1998–2007,” published by the Gulf Centre for Cancer Registration [8].
The Globocan data from 2008 shows that the age-standardized rates for the incidence and mortality from all cancers in the UAE is lower compared to Western countries, such as the United States (Table 19.1). The incidence of all cancers is projected to double by 2020, primarily due to aging and also possibly due to increased exposure to risk factors for cancer. Breast cancer is the most common cancer among Emirati females, lung cancer is the most common cancer among Emirati males but is extremely rare in females, which reflects the prevalence of smoking (23.0 % vs. 0.5 %, respectively), and colorectal cancer is the second most common cancer in both sexes combined (Table 19.2) [7–9]. However, rates for all three types of cancer are much lower than most Western countries and are also lower than in Qatar, Bahrain, and Kuwait [13]. This is likely to be due to the younger age of the population, less exposure to some risk factors, lower levels of screening compared to Western countries, and possibly incomplete registration. Cancer rates are also projected to increase by the year 2030 as the UAE population ages, total fertility declines, exposure time to lifestyle risk factors increases, the prevalence of obesity and diabetes increases, and due to the long latency period between starting smoking and developing lung cancer. Population-based education and awareness campaigns are urgently required to increase screening rates for at-risk individuals and to facilitate early diagnosis and prompt treatment, thereby reducing morbidity and improving survival.
In 2009, UAE’s population stood at about 5.7 million, of which approximately 21.9 % were nationals and the rest foreigners. As a consequence, UAE nationals form a minority of those who reside in the country. UAE has one of the most diverse populations in the Middle East. 23 % of the population is non-Emirati Arabs or Persians and the majority of the population, about 50 %, is from South Asia.
The population of the UAE also has a skewed sex distribution consisting of more than twice as many males as females. The 15–65 age groups have a male/female sex ratio of 2.743. The average life expectancy is 78.24 years, higher than any other Arab country. The breast cancer in UAE is considered the number one cancer among females and constitutes almost 23 % of all cancer cases and 43 % of all female cancers annually and that is similar to international ratios.
Cancer rates are set to increase at an alarming rate globally as well as locally. Cancer is set to become the fifth disease in UAE and GCC region. A difference can be made by taking action today and use the opportunity to stem this increase. Governments, health practitioners, and the general public need to take urgent action; actions as cost-effective treatment plans, provision of financial support to people, screening awareness, and tobacco cessation (see Figs. 19.3 and 19.4).

Estimated projection of new cancer cases in UAE amongst national and expatriates based on population growth and market labor needs

Projected level of cancer cases in the UAE and GCC countries showing cancer cases are increasing at an alarming rate. Source: McKinsey & Company
Age-standardized rate (W): A rate is the number of new cases or deaths per 100.000 persons per year. An age-standardized rate is the rate that a population would have, if it had a standard age structure. Standardization is necessary when comparing several populations that differ with respect to age because age has a powerful influence on the risk of cancer. Risk of getting or dying from the disease before age 75 %: The probability or risk of individuals developing dying from cancer. It is expressed as the number of new born children (out of 100) who would be expected to develop die from cancer before the age of 75. If they had cancer rates observed in the period in the absence of other causes of death.
Uptake of Oncology Drugs Costs on Selected Cancers in UAE
UAE hospitals are not unique in the struggle to coping with the existing and further increasing financial burden caused by cancer and its treatment. Worldwide, drugs associated with cancer care are estimated to cost approximately $40 billion per year. In the United States, cancer drugs represent the biggest category of overall pharmaceutical sales, in 2007 sales increased by 14 %. Seventy percent of these sales came from products introduced in the last 10 years and 30 % in the last 5 years [10]. These new drugs have improved the quality of life, delayed disease progression, and helped prolong survival for patients.
New molecular targeted agents introduced in recent years include well-known agents such as Rituximab (1997), Trastuzumab (Herceptin in 1998), Imatinib (Gleevec in 2001), and Bevacizumab (Avastin in 2004) therapies that caused excitement among the oncology community. However, such therapy comes at considerable cost, just recently new agents were released such as Regarofenib (2012) and Pertuzumab (2012) and we know that there are many other new agents under development.
It is widely recognized that the across tumor sites, mean net costs of care are highest in the initial and last year of life phases of care and lowest in the continuing phase [11, 12].
The significant increase in costs of initial cancer treatment reflects more patients receiving surgery and adjuvant therapy and rising prices for these treatments. These trends are likely to continue in the near future, although more efficient targeting of costly therapies could mitigate the overall economic impact of this trend [13].
The costs of cancer care are substantial and vary by tumor site, phase of care, stage at diagnosis, and survival.
Patterns of care have been reported to be more aggressive for younger cancer patients compared with elderly cancer patients in many health care settings. In addition, as the prevalence of comorbid conditions and levels of medical care increase with age, health care spending also typically increases with age [14].
Oncologists are in a difficult position, on the one hand, as prescribers they can be asked to be gatekeepers; on the other, they are advocates for their patients. These issues are well recognized in the oncology community and as such organizations such as ASCO through their Journal of Clinical Oncology publish many studies on economic evaluation [15].
Cancer caused 14 % of all deaths in the Emirate of Abu Dhabi in 2011. Lymphoid, hematopoietic, and related tissue cancers are the dominant cancers in Abu Dhabi. Late detection of breast cancer leads to significant increases in mortality. Female adult nationals aged 40–69 are being screened for breast cancer as part of their Thiqa insurance renewal. Education and awareness campaigns have increased screening rates for all nationalities [16].
The American Society of Clinical Oncologists (ASCO) issued a guidance statement affirming the “critical role of oncologists in addressing costs of care.” Since in the United States the high cost of cancer care can be financially devastating to patients and their families, oncologist communicate with their patients and discuss costs of their therapy and implications on the quality of care [17].
Outside of the United States, many counties use a formal process to evaluate new technologies before deciding whether they should be broadly adopted.
Published estimates for the treatment costs of breast cancer vary widely in methodology, perspective, patient populations, and time horizon.
Breast cancer represents the most drug-intensive area when it comes to treatment of solid tumors. Tamoxifen, a costly treatment launched in 1975 has established itself as the most cost-effective cancer treatment to date. Its broad indication for the treatment of advanced disease and adjuvant treatment represents a major breakthrough in the treatment of breast cancer. Newer, innovative drugs (aromatase inhibitors; anastrozole, exemestane, and letrozole) are now replacing, fully or in part, tamoxifen, both in the treatment of advanced disease but also in the adjuvant setting. In addition, anthracyclines and taxanes have established themselves as very valuable palliative and adjuvant treatments.
Trastuzumab, an HER2 receptor antibody, has become a cornerstone of treatment for patients with advanced breast cancer over-expressing HER2, in the adjuvant setting.
The lifetime treatment Estimates per-patient costs of breast cancer ranged from US$ 20,000 to US$ 100,000. (Campbell and Ramsey 2009) [18]. While disease stages I and II were emphasized, the costs of initial and terminal therapy were greater than continuing care on a per unit time basis, but continuing care accounts for the largest share of lifetime cost due to the relatively long survival of breast cancer patients.
Costs of different surgeries were relatively similar (breast-conserving surgery vs mastectomy) but, all else equal, significant costs (US$ 23,000–31,000) were observed for patients who received adjuvant chemotherapy compared with those who did not.
In the 1980s, colorectal cancer remained a therapeutic area in which medical treatment was considered to have little or no effect. Developments in diagnostic and surgical techniques were major contributors to outcome improvement. With the publication of the adjuvant data on modulated 5-fluorouracil (S-FU)-based therapy, colorectal cancer rapidly became an area of focus for further drug development. Recently, two new innovative drugs, Bevacizumab and cetuximab, have also been used for the treatment of advanced colorectal cancer; representing a more cost incurred in the treatment of the disease. Bevacizumab is an anti-angiogenesis drug with its indication in the first-line treatment of advanced colorectal cancer. Cetuximab , which interacts with the epidermal growth factor (EGF) receptor, is indicated in the second or third-line treatment of metastatic disease. The prevalence of colorectal cancer was projected by Mariatto et al. (2006) [19] to increase in the United States from 1,002,786 (0.36 %) patients to 1,522,348 (0.46 %) patients between 2000 and 2020. Their review of SEER data they project that colorectal cancer prevalence will increase more rapidly than the US population, largely due to the aging of the US population. This suggests that considerable resources will be needed in the future for initial, continuing and last year of life treatment of colorectal cancer patients unless notable breakthroughs in primary prevention occur in the future years.
Oncology drugs account for a significant proportion of drug expenditures in the clinic setting in the United States (Hoffman et al. 2012) [20].
The top 20 cancer drugs based on expenditures for chemotherapy drugs consumed in UAE in 2011 are listed in Table 19.3. Bevacizumab, Trastuzumab, and Rituximab represent the top three oncology drugs based on expenditures in 2010 (Table 19.3).
Hoffman et al. (2012) go on to describe the top ten therapeutic classes of drugs, with antineoplastic and hemostatic modifiers (such as those used in the treatment of hemophilia) being the top two, with blood growth factors (e.g., Filgrastim, Pegfilgrastim, Lenograstrim) the top four all comprising some 34 % of total expenditure (Table 19.4).
Opportunities and Challenges to Health Care Systems in UAE
The United Arab Emirates (UAE) is a rapidly developing country composed of a multinational population with varying educational backgrounds, religious beliefs, and cultural practices, which pose a challenge for population-based public health strategies.
Cancer is a cause of a comparable less burden of disease in the Middle East countries compared to Europe and the United States. However, in the Middle East, the burden of illness is expected to change from communicable diseases toward more expensive to treat noncommunicable diseases and injuries over the next decades—it is estimated that these will account for 60 % of the disease burden in 2020, compared to 45 % today, which will have consequences for health system configurations and health spending. Diagnosis and treatment of noncommunicable diseases and acute injuries are often complex and costly, which will put increased pressure on health care budgets. It is therefore increasingly important that investments are well managed and directed toward cost-effective technologies. Challenges for the health systems in these countries are to analyze what the costs and benefits of treating noncommunicable diseases are, and how to adopt the health care systems for treatment of such diseases in the optimal way [21].
The generally high standards of health care in the United Arab Emirates are a result of decades of high levels of public spending since the oil boom. There is a developing private health sector, several small private hospitals have been set up over the past few years, and however wealthy people still tend to travel abroad for medical care. Health expenditure was almost 3 % of GDP in 2004. Health care used to be free to all, but in 2001 the government introduced charges for expatriates, a move that partly sought to reduce the draw of health care on public funds, but also aimed to increase the employers’ cost of expatriate labor (which now requires health insurance) and thus encourage the employment of local staff. Since the policy was introduced, visits to government hospitals have fallen sharply, with some reports suggesting a 50 % reduction.
UAE also faces some elements that will dramatically increase health care demand in the area:
Population growth: Until 2025, the size of the population will increase at a compound annual growth rate (CAGR) of around 3.0 %, one of the highest in the world. By then, GCC population in 2025 will be almost twice the size it is today.
Hospital beds: By 2025, demand for hospital beds in UAE will be more than double, requiring almost 162,000 beds to meet this demand. Saudi Arabia and the United Arab Emirates will register the greatest percentage increase in demand for hospital beds (Fig. 19.5).

Projected level of hospital beds in UAE and GCC countries showing an increase in the required number of beds to meet the local population needs. Source: McKinsey & Company
Oncology Division: Cancer Center
Tawam Hospital has been established as a Regional Center of Excellence for Cancer Care in Al-Ain since 1980. The center is a dedicated facility providing a range of Medical Oncology and Hematology services for all forms of cancers and blood disorders, with a dedicated team of Certified Hematologists/Oncologists. In addition to traditional cancer treatment options of Surgery, Chemotherapy, Radiotherapy, and Palliative care, the Center is continuously offering new therapies, which are creating exciting new treatment possibilities. The oncology program spans from prophylactic check-ups in patients with an increased hereditary risk of developing cancer through to adjuvant treatment for metastatic diseases and palliative treatment.
The Division of Oncology offers highly specialized treatments with antibodies and tyrosine kinase inhibitors, chemotherapy and endocrine therapy for both inpatients and outpatients.
The oncology team consists of highly experienced and trained professionals who treat all kinds of cancers in breast cancer, colorectal tumors, lung cancers, as well as other types.
Health Care Demand in UAE and the World Comparison
Over the past several decades, discoveries in molecular biology have significantly improved cancer care. Biomarkers based on mutation status or over-expression of specific genes is now commonly used to guide treatment, and drugs targeting these biomarkers have helped extend the lives of many patients.
Considerable debate has therefore arisen over the affordability of cancer care, especially in light of the efforts many countries are making to control or reduce health care spending. In fact, cancer is now becoming the most expensive disease. In the European Union alone, insurance companies will spend about €49 billion annually on health services for cancer patients, and it is estimated that total health care spending in the region will reach US$ 60 billion in 2025, up from US$ 12 billion today.
The United Arab Emirates—part of GCC region, will face an unparalleled and unprecedented rise in demand for health care over the course of the next two decades. No other region in the world faces such rapid growth in demand with the simultaneous need to realign its health care systems to be able to treat the disorders of affluence.
The UAE faces some elements that will dramatically increase health care demand in the area:
Population growth: Until 2025, the size of the population will increase at a compound annual growth rate (CAGR) of around 3.0 %, one of the highest in the world. By then, GCC population in 2025 will be almost twice the size it is today. Furthermore, there is demand for more clinical staff; government can help make jobs more attractive to students by creating professionally and financially rewarding career paths for them to stay in the region. Better salaries, substantial investments in professional training and development (such as residencies), and more flexible careers made possible by a greater degree of private-sector participation in the health care system should all help to attract nationals and keep expatriates. Cancer rates are set to increase at an alarming rate globally as well as locally [22].
Screening
Screening is the process of looking for cancer in people who have no symptoms of the disease. Regular screening for some types of cancer can detect changes in cells before they become cancerous. Screening in UAE is currently available for breast, cervical, prostate, and colorectal cancer.
Despite breast-screening services being widely available under health insurance in the UAE, with many facilities offering free checks, many women do not get checked; much still needs to be done in terms of affordability to public as the cost of screenings can often be a constraint for individuals who wish to screen themselves for cancer risk. On average, a mammogram costs about Dh300 and a PAP test to check for cervical cancer costs Dh100. Colonoscopies to test for colorectal cancer cost between Dhs. 2000 to Dhs. 3000, but a fecal exam can also be used as an alternative, and this costs about Dhs. 100 [23].
The fight to raise awareness of this disease is ongoing here in the UAE. Breast cancer accounts for 13.7 % of all cancer deaths in women across the globe and is the most common cause of cancer in women in the UAE. Furthermore, studies have shown that women in the Gulf region are more likely to develop breast cancer at least a decade earlier than their counterparts in Western countries. There is as well the fact that the majority of women in the UAE comprise expatriates on lower incomes—such as maids and nannies—which makes the tests unaffordable to them and this where governments support comes in, by providing and/or bearing the costs of breast screening for all women residing in UAE to help combat the disease locally and globally and also to provide breast cancer education to public to raise awareness to a higher level among people by promoting workshops, seminars, and exhibitions.
There is the psychological factor as well in some Arabic countries, for example, there is a belief that once a woman is diagnosed with breast cancer, she may be divorced by her husband and possibly rejected by the community, or that following a breast cancer diagnosis her breast will be cut off and she will die. As a result of such misconceptions and unfounded beliefs, women may tend to hide their breast cancer symptoms at the early stages when treatment is most likely to be effective.
To further decrease the number of deaths from breast cancer in UAE for instance, there is an extreme need to reemphasize the facts that women must begin screening at age 40 years and continue annually. Health systems as well as insurance plans have to be developed to increase the proportion of the population receiving high-quality screening and treatment when needed, support programs to improve and standardize the quality of screening.
A remarkable milestone in the process of developing health care services in the UAE is the establishment of the National Breast Screening Program (NBSP) in 1995, operated by central department of maternal and child health, a division of the health policy affairs sector at the Ministry of health in UAE. The program’s mission is to reduce mortality from breast cancer by delivering high-quality breast-screening service to UAE women as part of the overall spectrum of women’s health. The program has been accredited by the WHO and the Nottingham Breast Institute in the United Kingdom in 2005 [24].
The Health Authority Abu Dhabi (HAAD) works with public, private, and community partners to create and implement strategies to help people in the Emirate of Abu Dhabi who live with, though, and beyond cancer. HAAD Cancer Control Plan aims at reducing the risk, incidence, and deaths from cancer, as well as enhancing the quality of life for cancer survivors. They have also issued recommendation for cancer screening and have initiated a 3-year-plan for cancer control in Abu Dhabi emirate (Fig. 19.6; Table 19.5) [25].

The main cancer control strategies of HAAD, Abu Dhabi; 2012
The main cancer control strategies are:
-
Establish evidence-based cancer prevention programs
-
Improve quality of cancer care: screening, diagnosis, treatment, and palliative care
-
Promote healthy living and early detection on priority cancers: breast, colorectal, lung, and cervical
-
Enhance community support services and increase access to screening services
-
Strengthen cancer surveillance
HAAD Cancer Control plan is a comprehensive approach that addresses all aspects of cancer care: prevention, early detection, diagnosis and treatment, and palliative care (Fig. 19.7).

Summary of the 3-year plan for cancer control in Abu Dhabi
Hematopoietic Stem Cell Transplant Program
Hematopoietic stem cell transplant (HSCT) is a new but rapidly expanding field in medicine since the first successful HSCT was performed in 1968. The procedure is utilized to treat medical conditions, previously lacking any treatment options, such as leukemia, myeloma, lymphomas, immune disorders, and some solid tumors.
The government of Abu Dhabi has requested Abu Dhabi Health Services Authority (SEHA) and Tawam Hospital to submit proposals to host an HSCT program.
At this point in time, there are only a few established HSCT programs in the Middle East region, principally in the Kingdom of Saudi Arabia. Patients residing in the UAE have little option but to seek treatment abroad. The cost of this treatment is very high, compounded by the associated travel, accommodation, and family member expenses.
The number of UAE-based patients sent abroad for treatment is difficult to establish, as there are several means of sponsoring their treatment. Costs are covered by nationwide organizations such as Defense and Police, local government within each Emirate, philanthropic individuals, and charitable organizations as well as self-pay.
There must be no doubt that to establish a successful program significant up-front and ongoing operational investment will be required. Tawam and SEHA have developed a comprehensive Financial Model for the HSCT program.
HSCT is a program that is associated with very high treatment mortality. However, an HSCT program can be successful and can generate significant revenue, provided that the hospital can develop a good reputation. In order to achieve this, many patients must be successfully treated. There should be no limit in the initial years on access to care restricted by insurance; otherwise, the necessary volume required to gain experience will not be available.
To date, SEHA are in the final planning stages having sought input from experienced external advisors.
Palliative Care
Palliative care—treating the pain, symptoms, and stress of serious illness—is vital for patients, but it is still misunderstood among health professionals, cancer sufferers, and the public at large. This type of treatment is also still not recognized as an essential component of health care and is not just for patients who have terminal illnesses.
Tawam Hospital has the distinction of being the only hospital in UAE with an established Palliative Care Program. Palliative care was started as a consultation service in 2007 and was developed into a complete division within oncology providing outpatient clinics and inpatient consultations with a dedicated inpatient unit. The number of outpatient visits and inpatient consultations in Palliative Care are increasing at a steady rate.
Palliative care is an important component of comprehensive cancer care in the developed world. The patients with advance terminal cancer are provided with efficient pain and symptom management with the aim to improve their quality of life. This is achieved by multidisciplinary approach with the involvement of various support staff such as social workers, psychiatrists, dieticians, physiotherapists, speech and language therapists, clinical pharmacists, home health care nurses and physicians, and pain management physicians. This multidisciplinary approach reduces the physical psychological and social suffering of the cancer patients and their families.
The Palliative Care Unit in Radiotherapy building was specially designed for easy access to the families of the terminal patient and is close to green lawns, where patients can go out and view the scenery outside the hospital bedroom. Many patients reach the stage of palliation due to the late presentation and diagnosis of cancer in this region. The Palliative Care Division is proud to have such service in the UAE serving the people of Emirates as well as the other GCC Countries.
While progress has been made in cancer diagnosis and treatment, much remains to be done to improve palliative care, which has emerged as an important subspecialty in high-income countries [26]. The expanding need for palliative care is now recognized, both medically and geographically, with the Worldwide Palliative Care Alliance recommending that governments integrate palliative care into each country’s health care system [27].
Approximately 80 % of patients requiring palliative care live in low- and middle-income countries; 96 % are adults, the remainder children. Although childhood cancers are not among the six leading causes for palliative care, 98 % of all children needing palliative and end-of-life care belong to low- and middle-income groups. The highest rates for children needing palliative care for cancer are in eastern Mediterranean countries (WHO-EMRO region) [28].
While relative overall cancer survival rates are greater than 60 %, in less developed countries it is only 30–50 % [29]. The International Agency for Research on Cancer reported that the percentage of patients dying of cancer in 2012 varied between developed countries (40.4 %) and developing countries (66.4 %) [30]. Palliative care needs of a population can be estimated by number of deaths, a valuable reference for service planning and development [31].
Palliative care needs to be integrated into the health care system and added to the curriculum of medical schools through the means of a proper national educational program.
Cancer Registry in UAE
Tawam Cancer Registry (TCR) is a cancer information system for the collection and analysis of information on all cancer patients diagnosed and treated at the hospital. Tawam Hospital Cancer Registry is committed to decreasing the morbidity and mortality caused by cancer, through accurate and complete data collection that can be used to monitor, analyze, and report cancer incidence, treatment, and survival. The Registry covers about 80 % of the country, including all of Abu Dhabi. Its data is still published every year, but is less useful than a complete, UAE-wide record.
Tawam Cancer Registry is the oldest registry in the country, with cases dating back to 1998 and was the first and the only Cancer Registry in the United Arab Emirates which aims to follow Commission on Cancer (CoC) “Facility Oncology Data Standards” for cancer data recording and cancer care at a facility.
Within Tawam Hospital, TCR is considered to be an integral part of the hospital’s cancer program which serves the needs of the hospital administration, the hospital’s cancer program, and above all the individual patient by maintaining their follow-up in a passive manner. TCR plays an important role in measuring cancer care delivery and supports quality improvement studies at Tawam. No other facility across the country has established a systemized and comprehensive approach to monitor and evaluate cancer care.
In 2012, a total of 1500 new cancer cases were registered at Tawam Hospital. Out of this, 43 % of the cases were diagnosed with breast cancer and 20 % were colorectal (Fig. 19.8).

Newly registered/diagnosed cancer cases at Tawam hospital in 2012 showing breast cancer amongst the top ten diagnosed cases (43 %) followed by CRC (12 %)
Recommendations
Cancer Care in the Emirate of Abu Dhabi is facing a significant increase of new cases per year and to meet future demand, additional capacities for cancer treatments have to be established. The growth in demand for health care services associated with the prevention and treatment of cancer, cardiovascular disease, diabetes, respiratory conditions, emergency medicine, and neuropsychiatric conditions is expected to be particularly high in the coming years as the population ages. Health care particularly in Abu Dhabi faces growing demand for services arising from an expanding population. The current population is young and has a rate of chronic diseases that is set to increase as it ages. The need for additional capacities is getting more evident as cancer incidents is expected to increase significantly due to changing demographics and morbidity patterns. With a yearly growth of 4.7–7.1 %, the number of new cancer cases is expected to be more than double in the near future.
Bed Capacity
Significant additional capacity is required to meet growth in demand for health care services as the population grows and ages. In existing developed areas, the emphasis is on growing existing facilities to facilitate specialization and scale. Future development plans should be focused on the areas where there is new residential and commercial development and planned population growth.
Cancer Centers
HAAD has recommended the establishment of an optimized delivery model for oncology patients which is based on international standards of cancer care to increase capacities and balance the access to service providers within the Emirate. And based on the expected caseload in 2030 and approved minimum maximum patient volumes for efficient cancer centers, a demand for two integrated cancer centers have been derived and is underway.
Clinical staff: Government can help make nursing and other medical professions more attractive to local students by creating professionally and financially rewarding career paths for clinicians who stay in the region. Better salaries, substantial investments in professional training and development (such as residencies), and more flexible careers made possible by a greater degree of private-sector participation in the health care system should all help to attract nationals and keep expatriates.
Screening
It plays an increasingly important role in determining outcomes in many forms of cancer. However, the high cost of the new tests is not affordable by many patients and although the improved outcomes may not be seen for several years. In some cases (e.g., bladder cancer), evidence is emerging that new diagnostic methods may reduce recurrence rates and lower long-term treatment costs. Methods should be planned and implemented where access to screening for all groups is available and affordable, and to ensure referring doctors have access to tools for training, information, and inclusion in screening programs.
References
World Cancer Report 2008.
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. Article first published online: 4 Feb 2011; doi:10.3322/caac.20107.
Blair I, Sharif AA. Population structure and the burden of disease in the United Arab Emirates. J Epidemiol Global Health. 2012;2:61–71.
Loney T, Cooling RF, Aw TC. Lost in translation? Challenges and opportunities for raising health and safety awareness among a multinational workforce in the United Arab Emirates. Saf Health Work. 2012;3:298–304. doi:10.5491/SHAW.2012.3.4.298.
United Arab Emirates National Bureau of Statistics. United Arab Emirates: United Arab Emirates National Bureau of Statistics; 2011. National population by emirate and sex (2010 mid-year estimates). http://www.uaestatistics.gov.ae/ReportDetailsEnglish/tabid/121/Default.aspx?ItemId=1914&PTID=104&MenuId=1 [cited 15 November 2012].
Statistical Yearbook of Abu Dhabi. United Arab Emirates: Abu Dhabi Statistics Centre. 2011. http://www.scad.ae/en/Pages/StatisticalYearBook.aspx. [cited 15 November 2012].
International Agency of Research on Cancer, GLOBOCAN. Incidence and mortality date for the United Arab Emirates; 2008.
Statistics Centre Abu Dhabi. Health statistics 2010. http://www.scad.ae/SCAD%20Publications/Health%20English.pdf.
Gulf Centre for Cancer Control and Prevention. Saudi Arabia: Riyadh; Ten-year cancer incidence among national of the GCC states, 1998–2007.
Gavel S. The oncology pipeline: maturing, competitive, and growing. Oncol Business Rev. 2008;9:14–6.
Yabroff R, Lamont E, Mariotto A, et al. Costs of care for elderly cancer patients in the United States. J Natl Cancer Inst. 2008;100:630–41.
Oliviera C, Bremner K, Pataky R, et al. Understanding the costs of cancer care before and after diagnosis for the 21 most common cancers in Ontaria: a population-based descriptive study. CMAJ Open. 2013. doi:10.9778/cmajo.20120013.
Warren J, Yabroff R, Meekins A, et al. Evaluation of trends in the cost of initial cancer treatment. J Natl Cancer Inst. 2008;100:888–97.
Mariotto A, Yabroff R, Shao Y, Feuer E, Brown M. Projections of the cost of cancer care in the United States: 2010–2020. J Natl Cancer Inst. 2011;103:117–28.
Levine M, Ganz PA, Haller D. Economic evaluation in the journal of clinical oncology: past, present, and future. J Clin Oncol. 2007;25:614–6.
HAAD Statistics 2001. http://www.haad.ae/HAAD/LinkClick.aspx?fileticket=JY0sMXQXrOU%3d&tabid=1243. Accessed 10 April 2013.
Meropol NJ, Schrag D, Smith TJ, et al. American Society of Clinical Oncology guidance statement: the cost of cancer care. J Clin Oncol. 2009;27:3868–74.
Campbell J, Ramsey S. The costs of treating breast cancer in the US: a synthesis of published evidence. Pharmacoeconomics. 2009;27:199–209.
Mariotto B, Yabroff R, Feuer J, et al. Projecting the number of patients with colorectal carcinoma by phases of care in the US; 2000–2020. Cancer Causes Control. 2006;17:1215–26.
Hoffman J, Li E, Doloresco F, et al. Projecting future drug expenditure-2012. Am J Health Syst Pharm. 2012;69:405–21.
Patient access to cancer drugs in nine countries in the Middle East; Frida Kasteng; Nils Wilking; Bengt Jonsson.
Altekruse SF, Kosary CL, Krapcho M, et al, eds. Surveillance, Epidemiology, and End Results Cancer Statistics Review, 1975–2007. Bethesda, MD: National Cancer Institute; 2010. http://seer.cancer.gov/csr/1975_2007/, based on November 2009 SEER data submission, posted to the SEER Web site, 2010.
http://gulfnews.com/news/gulf/uae/health/free-cancer-screenings-in-abu-dhabi-1.1237981.
Shaheen R. An overview on breast cancer in Abu Dhabi and United Arab Emirates: barriers & opportunities; 2013.
Silbermann M, Fink RM, Min S-J, Mancuso MP, Brant J, Hajjar R, Al-Alfi N, Baider L, Turker I, ElShamy K, Ghrayeb I, Al-Jadiry M, Khader K, Kav S, Charalambous H, Uslu R, Kebudi R, Barsela G, Kuruku N, Mutafoglu K, Ozalp-Senel G, Oberman A, Kislev L, Khleif M, Keoppi N, Nestoros S, Abdalla RF, Rassouli M, Morag A, Sabar R, Nimri O, Al-Qadire M, Al-Khalaileh M, Tayyem M, Doumit M, Punjwani R, Rasheed O, Fallatah F, Can G, Ahmed J, Strode D. Evaluating palliative in middle eastern care needs countries. J Palliat Med. 2015;18(1):18–25. doi:10.1089/jpm.2014.0194.
Palliative care: a peaceful, humane global campaign is needed. Lancet 2014;383:487.
Connor SR, Bermedeo MCS (eds). Global atlas of palliative care at the end-of-life. London: Worldwide Palliative Care Alliance, 2014. http://www.Global-atlas-identifies-unmet-need-for-palliative-care/. Accessed 13 May 2014.
Silbermann M, Epner D, Charalmbous H, et al. Promoting new approaches for cancer care in the Middle East. Ann Oncol. 2013;23:5–10.
International Agency for Research on Cancer: GLOBOCAN 2012: Estimated cancer incidence, mortality, and prevalence worldwide in 2012. http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx. Accessed 13 May 2014.
Hligginson IJ. Health care needs assessment: palliative care and terminal care. In: Stevens A, Raftery J, editors. Health care needs assessment. Oxford: Oxford Radcliffe Medical; 1997. p. 1–28.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Jaloudi, M., Kanbar, J., James, D.M., El-Salhat, H. (2016). An Overview of Cancer Care in Societies in Transition: Global Perspectives—UAE Experience. In: Silbermann, M. (eds) Cancer Care in Countries and Societies in Transition. Springer, Cham. https://doi.org/10.1007/978-3-319-22912-6_19
Download citation
DOI: https://doi.org/10.1007/978-3-319-22912-6_19
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-22911-9
Online ISBN: 978-3-319-22912-6
eBook Packages: MedicineMedicine (R0)