
Abstract
In this chapter we present in vivo experiments with a new minimally invasive method of monitoring intracranial pressure (ICP). Strain gauge deformation sensors are externally glued onto the exposed skull. The signal from these sensors is amplified, filtered, and sent to a computer with appropriate software for analysis and data storage. Saline infusions into the spinal channel of rats were performed to produce ICP changes, and minimally invasive ICP and direct Codman intraparenchymal ICP were simultaneously acquired in six animals. The similarity between the invasive and minimally invasive methods in response to ICP increase was assessed using Pearson’s correlation coefficient. It demonstrated good agreement between the two measures < r > = 0.8 ± 0.2, with a range of 0.31–0.99.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
Introduction
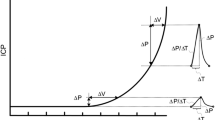
Intracranial pressure (ICP) is the result of cerebral blood and cerebrospinal fluid circulatory dynamics and can be altered in the course of many diseases of the central nervous system [2, 4]. Monitoring of ICP is essential for the detection of various neurological disorders. In cases of medium severity with a Glasgow Coma Scale score of between 9 and 12, computed tomography may not show changes. It is therefore essential to measure ICP, because in 20 % of cases neurological deterioration may occur during the first 24–48 h [1].
Conventional ICP monitoring methods require catheter insertion through the skull and the dura mater. This procedure may include risks of intracranial hemorrhage and infection [7], mainly when monitoring is performed outside the intensive care environment. Taking these disadvantages into consideration, the need to monitor ICP without complications caused by skull invasion is of utmost clinical importance.
A minimally invasive ICP monitoring method can be defined as a technique capable of measuring ICP without penetrating the skull, thereby minimizing the risks to the patient. In acute cases where direct ICP measurement is impossible, methods such as that described herein could represent an interesting alternative. Cerebral malaria, for instance, is one of the most common nontraumatic encephalopathies in the world [3], and despite the need to monitor ICP, in most cases this is not carried out because the invasive methods put the patient at risk. Nevertheless, ICP monitoring confirmed that children who were deeply unconscious with cerebral malaria had increased ICP, and those children who developed severe intracranial hypertension either died or survived with severe neurological sequelae [6].
The most likely cause of increased ICP in cerebral malaria is an increase in cerebral blood volume, particularly during the initial stages and in those patients with moderate degrees of intracranial hypertension [6]. Therefore, a method that could eliminate such complications would be of relevant clinical importance in these circumstances and make the difference between a good and a poor outcome.
We report in this work the validation of the previously proposed new minimally invasive method of ICP monitoring (ICPmi) [5] by comparing it directly with the simultaneous use of an invasive technique (ICPi) as the gold standard. In this study we aim to measure the correlation coefficient between invasive and minimally invasive measurements of ICP in rats. The system basically consists of a strain gauge sensor capable of capturing the bone deformities arising from changes in ICP. An electronic data acquisition system with an analog-to-digital module is used to digitize the signal and send it to a computer for data viewing and recording.
Materials and Methods
The ICPi (Codman®) and ICPmi (Braincare, patent pending) systems were used for simultaneous comparisons in male adult Wistar rats (n = 6, 300–350 g). Animals were anesthetized with a combination of ketamine (95 mg/kg) and xylazine (12 mg/kg). Once anesthetized, the animals underwent surgery for installation of the two sensors on opposite sides of the parietal bone. To induce dynamic changes for direct comparison of the time series response for the two methods, 0.9 % saline infusions into the spinal channel were administered using an automatic pump with a rate of 0.1 mL/min, over at least 10 min each, up to a total of volume of 1 mL. The number of infusions for each animal is shown in (Table 1). Time series were obtained with an acquisition rate of 200 Hz, data smoothing was implemented with a 10-s moving average window, and data analysis was performed using ICM+ (Cambridge Enterprises) and MatLab® software.
Results
To measure the similarity in the responses of the invasive and minimally invasive methods to ICP increase, Pearson’s correlation coefficients (r) were calculated. Figures 1 and 2 present typical time series for the two methods. The correlation coefficient values are shown in Table 1. Mean r values showed good agreement between the two methods,<r > =0.8 ± 0.2 with a range of 0.31–0.99. The values of the minimally invasive measure (mV) are related to those of the invasive measure (mmHg) according to the slopes and intercepts of regression lines between ICPi and ICPmi. The values obtained ranged from 83 to 754 (mmHg/mV; Table 1), showing some variability due to the installation of the strain gauge sensor. Regarding infusion procedures, because of variable experimental conditions among the animals (mainly movement artifacts due to the short anesthesia time), it was not possible to perform the same infusion protocol in all experiments. The last column of Table 1 shows the number of infusions for each animal.

Time series obtained with an invasive (ICPi) and noninvasive (ICPni) methods during the infusion procedure for animal MI02. The pattern of oscillation possibly occurs as a result of the leakage of liquid after a certain pressure is reached

Time series values obtained with ICPi and minimally invasive (ICPmi) methods during the infusion procedure for animal MI04. The pattern of oscillation possibly occurs as a result of the leakage of liquid after a certain pressure is reached
Discussion
Variations in the skull dimensions could be associated with changes in ICP using ICPmi in this work, which allows this new method to be employed in the development of equipment for minimally invasive ICP monitoring, although calibration methodology for minimally invasive ICP measurement still needs to be developed in further studies.
The needle was introduced into the spinal canal without externalizing the animal spine; thus, adequate control of the dural puncture was not feasible and leakage of liquid possibly occurred after a certain pressure was reached. The appearance of the plateau in the signals of the two methods shows the exact moment when the pressure caused the balance between the volume of fluid infused and the fluid that was seeping through the puncture hole. The studies will continue and a new infusion technique for the rat will be tested.
Our main conclusion is that our proposed minimally invasive method can be safely used as a simple and cost-effective alternative tool for ICP monitoring. These results open up new perspectives in the fields of ICP monitoring, neurology, and neurosurgery, mainly in clinical scenarios in which this has previously been impossible because of complications caused by the invasiveness. Moreover, the method can also be used in areas in which ICP is still unexplored, such as pharmacology, endocrinology, and pathology, among others. The use of this system in universities and research centers can expand the horizons of knowledge, thereby making novel contributions to science. In further work to be published in the future, we have implemented the method in a variety of significant applications in neurosurgery and the neurosciences, such as hydrocephalus, epilepsy, and trauma.
References
Alperin NJ, Lee SH, Loth F, Raskin PB, Lichtor T (2000) Intracranial pressure: a method to measure intracranial elastance and pressure invasively by means of MR imaging: baboon and human study. Radiology 217:877–885
Czosnyka M, Pickard JD (2004) Monitoring and interpretation of intracranial pressure. J Neurol Neurosurg Psychiatry 75(6):813–821
Idro R, Marsh K, John CC, Newton CRJ (2010) Cerebral malaria; mechanisms of brain injury and strategies for improved neuro-cognitive outcome. Pediatr Res 68:267–274
Machado ABM (2004) Neuroanatomia funcional, 2nd edn. Editora Atheneu, São Paulo
Mascarenhas S, Vilela GHF, Carlotti C, Damiano LEG, Seluque W, Colli BO, Tanaka K (2012) New ICP minimally invasive method shows Monro-Kellie doctrine not valid. Acta Neurochir 114:117–120
Newton CRCJ, Hien TT, White N (2000) Cerebral malaria. J Neurol Neurosurg Psychiatry 69:433–441
Pitlyk PJ, Piantanida TP, Ploeger DW (1985) Noninvasive intracranial pressure monitoring. Neurosurgery 17:581–584
Acknowledgments
Conselho Nacional de Desenvolvimento e Pesquisa (CNPq), Fundação de Amparo a Pesquisa do Estado de São Paulo (FAPESP), Brazilian Ministry of Health Pan American Health Organization – World Health Organization (PAHO-WHO), and Sapra for financial support.
Conflict of Interest
ICM+ is a software program for brain monitoring in clinical/experimental neurosciences, licensed by Cambridge Enterprise Ltd (www.neurosurg.cam.ac.uk/icmplus). MC has an interest in part of the licensing fee. The remaining authors declare that they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Vilela, G.H.F. et al. (2016). Validation of a New Minimally Invasive Intracranial Pressure Monitoring Method by Direct Comparison with an Invasive Technique. In: Ang, BT. (eds) Intracranial Pressure and Brain Monitoring XV. Acta Neurochirurgica Supplement, vol 122. Springer, Cham. https://doi.org/10.1007/978-3-319-22533-3_19
Download citation
DOI: https://doi.org/10.1007/978-3-319-22533-3_19
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-22532-6
Online ISBN: 978-3-319-22533-3
eBook Packages: MedicineMedicine (R0)