
Abstract
This chapter will detail the cytopathology of a spectrum of risk-modifying, precancerous, and cancerous lesions of the cervix classified based on the 2014 Bethesda System. Included are the following categories: atypical squamous cells of undetermined significance (ASC-US), atypical squamous cells-cannot exclude HSIL (ASC-H), low-grade squamous intraepithelial lesion (LSIL), high-grade squamous intraepithelial lesion (HSIL), squamous cell carcinoma, atypical glandular cells-not otherwise specified (AGC-NOS), atypical glandular cells-endocervical (AGC-EC), atypical glandular cells-endometrial (AGC-EM), endocervical adenocarcinoma in situ (AIS), adenocarcinoma (endocervical, endometrial, not otherwise specified), and other malignant neoplasms.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
Introduction
Cervical cytology screening (Papanicolaou [Pap] test ) has markedly reduced mortality from cervical cancer, especially squamous cell carcinoma, which comprises the majority of cervical cancers (up to 90 %) [1, 2]. This cervical cancer mortality reduction is not only due to an increase in the detection of early stage invasive cervical cancer which has a 5-year survival rate of 92 % but also the detection and treatment of precancerous lesions [1, 2]. In the USA, more than 50 % of women with invasive cervical cancer either have never had cervical cytology tests or have not been screened periodically [3, 4].
The Pap test was invented by and named after Dr. Papanicolaou to detect potentially precancerous/cancerous cells sampled from transformation zone, the junction of the ectocervix and endocervix [5]. Conventional Pap test involves plating cervical samples obtained by brush and spatula on a microscope slide and then preserving samples with fixative solution. In liquid-based cytology, samples from the brush and spatula are transferred into a liquid fixative solution, and then cells are trapped onto a filter and plated onto a glass slide in a monolayer.
Pap test results are reported according to the Bethesda System (TBS) , which was first introduced in 1988 and revised in 1991 and 2001 [6–8]. The newly revised TBS will be published in the earlier months of 2015. The intent of TBS is to distinguish between abnormalities that are unlikely to progress to cancer and those that are more likely to indicate a precancerous or cancerous lesion and to standardize and improve the clinical usefulness of Pap test reports.
This chapter will introduce epithelial abnormalities of cervical cytology based on TBS 2014 Classification and include the following categories: atypical squamous cells of undetermined significance (ASC-US), atypical squamous cells-cannot exclude HSIL (ASC-H), low-grade squamous intraepithelial lesion (LSIL), high-grade squamous intraepithelial lesion (HSIL), squamous cell carcinoma, atypical glandular cells-not otherwise specified (AGC-NOS), atypical glandular cells-endocervical (AGC-EC) , atypical glandular cells-endometrial (AGC-EM), endocervical Adenocarcinoma in situ (AIS), adenocarcinoma (endocervical, endometrial, not otherwise specified), and other malignant neoplasms.
Squamous Cell Abnormality
-
Atypical squamous cells
-
Atypical squamous cells of undetermined significance (ASC-US)
-
Atypical squamous cells, cannot exclude hig h-grade squamous intraepithelial lesion (ASC-H)
-
-
Squamous intraepithelial lesions
-
Low-grade squamous intraepithelial les ions (LSIL)
-
High-grade squamous intraepithelial lesions (HSIL)
-
-
Squamous cell carcinoma
Glandular Cell Abnormality
-
Atypical glandular cells (AGC)
-
Atypical glandular cells-NOS (AGC-NOS)
-
Atypical endocervical cells (AGC-EC)
-
Atypical endometrial cells (AGC-EM)
-
-
Cervical adenocarcinoma in situ (AIS)
-
Endocervical adenocarcinoma
-
Endometrial adenocarcinoma
-
Other malignant neoplasms
Squamous Abnormality
Atypical squamous cells (ASC) are defined a s squamous cells with equivocal (uncertain diagnostic) findings that are suggestive for squamous intraepithelial lesions (SIL), which are qualitatively or quantitatively insufficient for a definitive interpretation. ASC is not a single biologic entity but rather includes changes that may be the results of nonneoplastic conditions (inflammation, atrophy, air-drying, etc.) or neoplasia (cervical intraepithelial neoplasia or carcinoma). It is recommended that ASC rate should be kept under 5 % for all Pap smears in a laboratory, and the ASC/SIL ratio should not exceed 3:1. All ASC interpretation should be categorized as either ASC of undetermined significance (ASC-US) or ASC-cannot exclude a high-grade squamous intraepithelial lesion (ASC-H).
ASC-US
Definition
ASC-US represents squamous cells with findings that are either suggestive of low-grade SIL (LSIL) or SIL of indeterminate grade and is recommended to comprise more than 90 % of all ASC interpretations in a laboratory.
Morphology
The area of the nucleus in a normal intermediate squamous cell is approximately 35 μm2, which is used as a comparison for nuclei of atypical squamous cells. ASC-US cells may show some of the following features (Fig. 11.1):

ASC-US (liquid-based preparation, LBP). (a) Mature squamous cells with nuclear enlargement, hyperchromasia, but even chromatin distribution. (b) ASC-US versus LSIL. Squamous cells with binucleation and nuclear enlargement: these are the only cells found on this Pap smear. (c) Squamous cells with multinucleation andFig. 11.1 (continued) nuclear enlargement. (d) ASC-US versus LSIL. Squamous cells with multinucleation, hyperchromasia, nuclear enlargement, and possible perinuclear halo. (e) Atypical parakeratosis. Cluster of squamous cells with irregular hyperchromatic nuclei and dense orangeophilic cytoplasm. (f) Single squamous cell with irregular hyperchromatic nucleus and possible perinuclear halo. (g) ASC-US versus LSIL. Single squamous cell with hyperchromatic nucleus and perinuclear halo. (h) Atypical repair. Single and cluster of cells with features suggestive of repair, but also enlarged nuclei, increased N/C ratio, irregular chromatin distribution, and conspicuous nucleoli
-
1.
Nuclei are about 2½–3 times the area of the nucleus of a normal intermediate squamous cell.
-
2.
Slight increase in nuclear to cytoplasmic ratio (N/C).
-
3.
Nuclear membrane is smooth to slightly irregular.
-
4.
Nuclear hyperchromasia is absent to light.
-
5.
Chromatin is finely granular and evenly distributed.
-
6.
Nucleoli/chromocenters are inconspicuous or absent.
-
7.
Cells present singly and in sheets.
-
8.
Atypical parakeratosis may present as small orangeophilic cells with moderate cellular pleomorphism, slight increase in nuclear size, and vesicular or pyknotic chromatin.
-
9.
Suggestive HPV cytopathic effect and/or binucleation may be present, but fall short of LSIL.
ASC-US includes the following patterns:
-
1.
Mature intermediate squamous cells with changes that resemble koilocytes, but lack all of the features of typical koilocytes (e.g., definite hyperchromasia, sharp perinuclear halos, or binucleation).
-
2.
Atypical parakeratosis with dense orangeophilic cytoplasm, minimal nuclear irregularity, and mild nuclear atypia.
-
3.
Atypical repair cells with features of repair and presence of marked nuclear size variation, prominent nucleoli, and irregular chromatin distribution.
-
4.
Atypia of atrophy with nuclear enlargement, hyperchromasia, or irregular nuclear contours.
-
5.
ASC-US may refer to cells with atypical nuclear features due to air-drying artifact in conventional smears or distorted cells at the rim of liquid-based cytology specimens.
Differential Diagnosis
Reactive Changes
The nucleus in cells with reactive changes may increase up to two times the area of the nucleus of a normal intermediate squamous cell with hypochromasia, fine chromatin, and smooth nuclear contour. The N/C ratio is low, and the cytoplasm is degenerative. Nucleoli may be seen (Fig. 11.2).

Reactive endocervical cells (liquid-based preparation, LBP). (a) Endocervical cells with enlarged nuclei, fine chromatin, regular nuclear contour, and prominent nucleoli arrange in a glandular pattern. (b) Reactive squamous cells in the presence of inflammation. Clusters of squamous cells with enlarged nuclei, regular nuclear contour, and prominent nucleoli
LSIL
The nucleus in LSIL cells is usually more than three times the area of the nucleus of a normal intermediate squamous cell with irregular nuclear shape and contour, hyperchromasia, binucleation/multinucleation, and coarse chromatin. Nucleoli are usually inconspicuous. Typical koilocytes have sharply defined perinuclear halos.
Follow-Up Results
In a s creened US population, approximately 50 % of ASC-US cases are positive for high-risk human papillomavirus (hr-HPV). Approximately 10–20 % of women with ASC-US were proven to have CIN2–3 on biopsy. Approximately 30–50 % of women with ASC-US were proven to have CIN1 on biopsy [9].
Management
The 2012 updated consensus management guidelines recommend that high-risk HPV testing is the preferred method for women ages 25 years or older, although repeat cytology at 1 year is acceptable. Colposcopy is not an option for women with ASC-US in the 2012 updated g uideline. For women ages 21–24 years with ASC-US, repeat cytology at 1 year is the preferred method, although high-risk HPV testing is acceptable.
ASC-H
Definition
ASC-H represents squamous cells with findings that are suggestive of high-grade SIL (HSIL) and accounts for less than 10 % of ASC cases.
Morphology (Fig. 11.3)

ASC-H (liquid-based preparation, LBP ). (a) Single small cell with scant cytoplasm, high N/C ratio, and a dark hyperchromatic nucleus which shows round nuclear contour and irregular chromatin distribution. (b) A loose cluster of cells with metaplastic cytoplasmic change, high N/C ratio, hyperchromatic nuclei, variation in size of nuclei, and minimal irregular nuclear contour. (c) A relatively large cluster of cells with thin rim of cytoplasm, high N/C ratio, and round hyperchromatic nuclei. (d) Single small cell with metaplastic cytoplasmic change, high N/C ratio, and a dark hyperchromatic irregular nucleus and irregular chromatin distribution. (e) A hyperchromatic group of cells with dark nuclei and nuclei overlapping, which are difficult to be ascertain
Small cell pattern (atypical immature squamous metaplasia) : immature (small) squamous cells with high N/C ratio but mild-moderate nuclear atypia
-
1.
Small fragments or individual cells
-
2.
Nuclei size is 1½–2½ times larger than normal intermediate cell nuclei
-
3.
Smooth to slightly irregular nuclear membrane
-
4.
Increased N/C ratio, similar to that of HSIL
-
5.
Finely granular and evenly distributed chromatin
-
6.
Inconspicuous or absent nucleoli
Hyperchromatic crowded group (HCG) pattern :
-
1.
Groups of crowded cells with sharp linear edges
-
2.
Polygonal cells containing nucle i with loss of polarity or difficultly visualized nuclei and dense cytoplasm
Differential Diagnosis
-
1.
Squamous metaplasia : mostly in sheets and cobblestone-like clusters or individual cells with homogenous dense cytoplasm, uniform round to oval nuclei, smooth nuclear membranes, and fine chromatin (Fig. 11.4).
Fig. 11.4 
Squamous metaplasia (liquid-based preparation, LBP ). Individual cells with homogenous dense cytoplasm, uniform round to oval nuclei, smooth nuclear membranes, and fine chromatin
-
2.
Atrophy : sheets/single parabasal cells with abundant cytoplasm, uniform round to oval nuclei, smooth nuclear membranes, and fine chromatin. Cell borders are usually distinct.
-
3.
Repair : flat sheets with maintained polarity (streaming) containing cells with minimal nuclear enlargement (1½–2 times enlargement), smooth nuclear membrane, mild hyperchromasia, finely granular and evenly distributed chromatin, prominent single or multiple nucleoli, dense cytoplasm with polychromasia, or vacuolization in a background of inflammation (Fig. 11.5).
Fig. 11.5 
Repair (liquid-based preparation, LBP). Flat sheets with maintained polarity containing cells with minimal nuclear enlargement, smooth nuclear membrane, mild hyperchromasia, finely granular and evenly distributed chromatin, prominent nucleoli, and dense cytoplasm
-
4.
Radiation : markedly enlarged cells with no significant increase of N/C ratio, bizarre cell shapes, variable nuclear size, binucleation/multinucleation, smudging chromatin, prominent single/multiple nucleoli, and cytoplasmic vacuolization.
-
5.
Histiocytes : streaming single cells with round, ovoid, and bean-shaped nuclei, foamy cytoplasm, a low N/C ratio, and fine cytoplasmic vacuoles.
-
6.
HSIL : cells with conspicuous nuclear atypia, a greater N/C ratio (nuclear size > 2× the size of normal intermediate cells), more pronounced irregular nuclear contours, and marked coarse chromatin.
-
7.
Endometrial cells : small cells with bean-shaped nuclei and smudgy chromatin in 3D clusters (Fig. 11.6).
Fig. 11.6 
Endometrial cells (liquid-based preparation, LBP). (a) A tight cluster of small cells in 3D structure. (b) Small cells with bean-shaped nuclei



Follow-Up Results
Approximately 30–50 % of ASC-H cases prove to have CIN2 or CIN3 on follow-up biopsy, and the incidence is higher in younger patients [10].
Management
The 2012 updated consensus management guidelines recommend women with ASC-H cytology to undergo colposcopy regardless of HPV results. Reflex HPV testing is not recommended. Recent studies and CAP survey results indicate that HPV-positive rate is about 50–60 % in women with ASC-H Pap test.
Follow-up of patients with HPV-negative ASC-H results yielded very low rates of detectible CIN2/3 (1.6 %) and no diagnoses of cervical cancer. Triage of study patients with HPV-negative ASC-H results to routine HPV and cytology co-testing at 1 year was a safe follow-up option [11].
LSIL
Definition
LSIL represents squamous cells with mild dysplasia or koilocytosis caused by both low-risk and high-risk HPV infections. The majority of LSIL represent a transient HPV infection which usually regresses within 1–2 years. Less than 2 % of LSIL will progress to invasive cervical carcinoma if untreated.
Koilocytosis represents HPV-associated cytopathic effect in mature intermediate or superficial cells.
Morphology (Fig. 11.7)


LSIL (liquid-based preparation, LBP). (a) Squamous cells with slightly increased N/C ratio, slightly coarse chromatin, irregular and hyperchromatic nuclei, well-defined perinuclear cavitation, and a dense peripheral rim of cytoplasm. (b) Single squamous cells with slightly enlarged, irregular, and hyperchromatic nuclei, well-defined perinuclear cavitation, and a dense peripheral rim of cytoplasm. (c) A cluster of squamous cells with enlarged, highly irregular, and hyperchromatic nuclei, relatively abundant dense cytoplasm, slightly increased N/C ratio, and well-defined perinuclear cavitation. (d) Single squamous cells with binucleation, well-defined perinuclear cavitation, and relatively abundant dense cytoplasm. (e) Single squamous cells with multinucleation and well-defined folded perinuclear cavitation. (f) Squamous cells with small, but highly hyperchromatic, nuclei and well-defined perinuclear cavitation. (g) LSIL versus ASC-US. Cells with slightly enlarged, slightly hyperchromatic nuclei and binucleation. (h) SIL, grade cannot be determined. Atypical squamous cells with irregular hyperchromatic nuclei, moderate amount of cytoplasm, and slightly increase N/C ratio. Based on the nuclear features, these cells are interpreted as SIL, but not gradable due to moderate amount of cytoplasm and absence of perinuclear halo
-
1.
Singly or sheets of mature/superficial squamous cells with distinct cytoplasmic borders.
-
2.
Slightly increased N/C ratio.
-
3.
Nuclear size >3 times the size of a normal intermediate nucleus.
-
4.
Variable nuclear size and shape.
-
5.
Smooth to slightly irregular nuclear membranes.
-
6.
Variable hyperchromasia.
-
7.
Binucleation or multinucleation may be seen.
-
8.
Slightly coarse but evenly distributed chromatin.
-
9.
Koilocytosis: squamous cells with well-defined perinuclear cavitation and a dense peripheral rim of cytoplasm together with nuclear abnormalities.
-
10.
Other LSIL cells include macrocytes, kite cells with cytoplasmic tails, polka dot cells with cytoplasmic globules, and balloon cells with clear cytoplasm.
Differential Diagnosis
-
1.
Reactive squamous cells with nonspecific halos. Nonspecific perinuclear halos usually show small clearings without nuclear atypia and can be caused by trichomoniasis infection, other inflammatory changes, or artifact during slide preparation (Figs. 11.8 and 11.9).
Fig. 11.8 
Reactive squamous cells in the presence of trichomonas vaginalis. Clusters of squamous cells with enlarged nuclei, regular nuclear contour, and prominent nucleoli on the upper right corner. Trichomonas vaginalis can be seen in the center of the image (liquid-based preparation, LBP)
Fig. 11.9 
Nonspecific clear perinuclear halos can be seen in glycogenated intermediate cells during pregnancy or other conditions. These cells lack typical nuclear features of LSIL (liquid-based preparation, LBP)
-
2.
Reactive endocervical cells can show enlarged nuclei and hyperchromasia which may mimic LSIL cells. However, reactive endocervical cells usually show regular nuclear contour and prominent nucleoli (Fig. 11.10).
Fig. 11.10 
Reactive endocervical cells with enlarged nuclei and hyperchromasia, but regular nuclear contour. A nonspecific clear perinuclear halo is also seen in a reactive squamous cell (liquid-based preparation, LBP)
-
3.
Parakeratosis or atypical parakeratosis (ASC-US). The cells with parakeratosis are much smaller than koilocytes and do not display atypia. The cells with atypical parakeratosis show nuclear atypia but not enough for a diagnosis of LSIL cells (Fig. 11.1).
-
4.
Postpartum changes. Navicular cells found in pregnant women can show empty vacuoles which may mimic perinuclear halos. However, nuclei are round to oval and uniform with fine and evenly distributed chromatin.



Follow-Up Results
Approximately 15–25 % of LSIL cases prove to have histologic CIN2 or CIN3 during follow-up biopsies [12].
Management
The 2012 updated consensus management guidelines recommend women with LSIL cytology and no HPV test or a positive HPV test to undergo colposcopy. If contesting shows HPV-negative LSIL, a repeat co-testing at 1 year is preferred, but colposcopy is acceptable. For women with LSIL who are aged 21–24 years, follow-up with cytology at 12-month intervals is recommended. For pregnant women with LSIL, colposcopy is preferred. HPV-positive rate is about 70–80 % in women with LSIL Pap test. HPV prevalence declines in older age groups. CIN 2/3 follow-up rate was very low in women 50 years and older with HPV-negative LSIL. HPV testing can be an option for old women in the guideline. In recent years, more women with LSIL Pap test had HPV testing result due to the increase of co-testing for women 30 years and older. Some research findings support recent recommendations for repeat co-testing after 1 year as an appropriate option for patients with HPV-negative low-grade squamous intraepithelial lesion (LSIL) [13].
LSIL-H (LSIL-Cannot Exclude HSIL)
LSIL-H represents cases with LSIL that also contain a few cells that are suspicious for, but not diagnostic of, HSIL (Fig. 11.11). Studies have found that these women have a significantly higher likelihood of a high-grade intraepithelial lesion on biopsy than women with LSIL only. The HPV-positive rate is also higher in women with LSIL-H than that in women with LSIL only. LSIL-H is a unique category of cytologic abnormality associated with distinctive HPV and CIN 2/3+ diagnostic rates. LSIL-H is not included in the 2001 TBS category, but has been used by some laboratories [14].

LSIL-H (liquid-based preparation, LBP). LSIL cells (a) were found on this Pap smear together with ASC-H cell (b)
HSIL
Definition
HSIL represents squamous cells with moderate dysplasia, severe dysplasia, and carcinoma in situ. Most HSILs are caused by persistent high-risk HPV infection and hence have increased progressing potential. Approximately 1.4 % of HSIL cases will progress to invasive cervical squamous cell carcinoma.
Morphology (Fig. 11.12)


HSIL (liquid-based preparation, LBP). (a) Small aggregate of small cells with markedly increased N/C ratio, irregular nuclear contours, hyperchromasia and chromatin clumping or granularity, and inconspicuous nucleoli. (b) Small aggregate of small cells with variation in size of nuclei, markedly increased N/C ratio, hyperchromasia, and chromatin clumping. (c) Single small cells with variation in size of nuclei, markedly increased N/C ratio, hyperchromasia, and chromatin clumping. (d) Cells can be large, but also contain enlarged hyperchromatic nuclei with irregular nuclear contour. The markedly increased N/C ratio is maintained. (e) Single HSIL cell with very coarse chromatin and high N/C ratio. (f) Single HSIL cells with variation in size, high N/C ratio, and coarse chromatin. (g) A cluster of hyperchromatic group cells with high N/C ratio, irregular nuclear contour, and coarse chromatin. (h) A small group of HSIL cells with very small nuclei, but markedly high N/C ratio. (i) Large HSIL cells with hyperchromatic nuclei, irregular nuclear contour, and markedly increased N/C ratio. (j) HSIL cells with involvement of endocervical glands. (k) HSIL cells involving endocervical glands can contain vacuoles
-
1.
HSIL cells often occur singly, in small aggregates, or syncytial-like hyperchromatic groups with irregularity of polarity.
-
2.
HSIL cells are typically smaller than LSIL cells, but vary from small basal-type to larger LSIL-like cells.
-
3.
Markedly increased N/C ratio.
-
4.
Irregular nuclear contours, hyperchromasia, and chromatin clumping or granularity.
-
5.
Inconspicuous nucleoli.
Differential Diagnosis
-
1.
LUS: Cells are in cohesive tissue fragments with uniform round/oval and well-ordered nuclei, evenly distributed chromatin, and mildly increased N/C ratio. The nucleoli may be present.
-
2.
Herpes: Cells infected with HSV can be multinucleated or mononuclear cells with nuclei exhibiting ground glass appearance due to intranuclear viral particles and enhancement of the nuclear envelop due to margination of chromatin. Intranuclear inclusions and nuclear molding may be present (Fig. 11.13).
Fig. 11.13 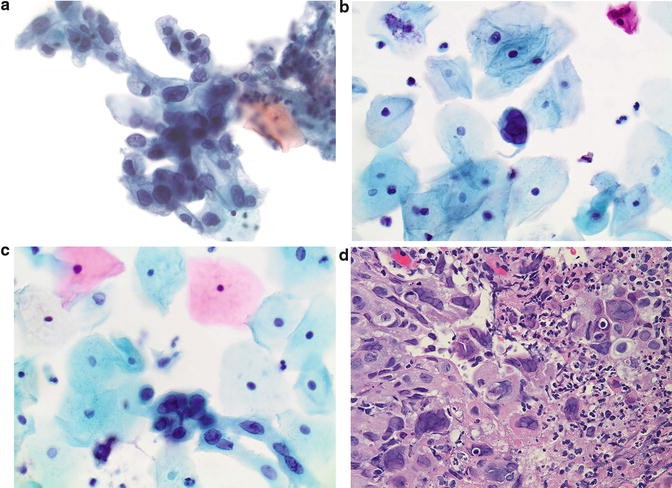
Herpes. (a–c) Liquid-based preparation. (d) H&E stain of biopsy specimen. Mononuclear or multinucleated cells with nuclei exhibiting ground glass appearance, margination of chromatin, and nuclear molding
-
3.
Adenocarcinoma in situ (AIS) cells show atypical nuclei but more glandular differentiation such as nuclear feathering and rosettes.
-
4.
Squamous cell carcinoma cells often show prominent nucleoli and background necrosis.
-
5.
Follicular cervicitis shows small lymphocytes with less hyperchromasia.

Follow-Up Results
Approximately 60 % of HSIL cases prove to have CIN 2+ lesions at colposcopy. Five-year cervical cancer risk is 8 % among women 30 years of age, and older and the risks are modified by HPV test results [15].
Management
The 2012 updated consensus management guidelines recommend that women with HSIL cytology should undergo immediate loop electrosurgical excision or colposcopy is acceptable, except in special populations. Triage using either reflex HPV testing or repeat cytology alone is unacceptable.
Squamous Cell Carcinoma
Definition
Squamous cell carcinoma represents malignant cells with squamous differentiation. Cervical squamous cell carcinoma usually affects women between the ages of 40 and 55 years, about 10 years later than intraepithelial lesions.
Morphology
Keratinizing Squamous Cell Carcinoma (Fig. 11.14)
-
1.
Individual or small clusters with marked variation in cellular size and shape.
-
2.
Caudate and spindle cells can be present with dense orangeophilic cytoplasm, and cells often have ample cytoplasm forming unusual cell shapes such as “tadpole” or “fiber” cells.
-
3.
Keratotic changes including hyperkeratosis or pleomorphic parakeratosis.
-
4.
Nuclei with variable size and shape, irregular membrane, hyperchromasia, coarsely granular and irregularly distributed chromatin with parachromatin clearing, and conspicuous nucleoli but less common than nonkeratinizing squamous cell carcinoma.
-
5.
Background of tumor diathesis (clinging diathesis: necrotic material at the periphery of the cell groups in liquid- based preparation).

Keratinizing squamous cell carcinoma (liquid-based preparation, LBP). (a) Individual or small clusters of squamous cells with marked variation in cellular size and shape, keratotic changes including hyperkeratosis, or pleomorphic parakeratosis with dense orangeophilic cytoplasm. Nuclei with variable size and shape, irregular membrane, hyperchromasia, and coarsely granular and irregularly distributed chromatin. (b) Clusters of squamous cells with marked variation in cellular/nuclear size and shape, keratotic changes, hyperchromasia, and coarse chromatin. (c) Very large bi-/multinucleated cells can be seen. (d) Cytoplasm is usually dense. (e) Tumor diathesis (clinging diathesis in LBP: necrotic material at the periphery of the cell groups in liquid-based preparation) can be seen. (f) Tadpole cell with ample orangeophilic cytoplasm
Nonkeratinizing Squamous Cell Carcinoma (Fig. 11.15)
-
1.
Single or syncytial sheets of cells with poorly defined cell borders
-
2.
Enlarged nuclei with prominent irregular nuclear membrane, coarse and unevenly distributed chromatin with distinct parachromatin clearing, and prominent nucleoli
-
3.
Cyanophilic, vacuolated, or dense cytoplasm
-
4.
Background of tumor diathesis

No nkeratinizing squamous cell carcinoma (liquid-based preparation, LBP). (a) Syncytial sheets of cells with poorly defined cell borders, dense cytoplasm, enlarged nuclei, prominent irregular nuclear membrane, and coarse chromatin. (b) Poorly differentiated squamous cell carcinoma cells with very large nuclei and prominent nucleoli. (c) Single poorly differentiated squamous cell carcinoma cells with very large nuclei, scant cytoplasm, and coarse chromatin. (d) Single poorly differentiated squamous cell carcinoma cell with markedly irregular and large nucleus. (e) Tumor diathesis (clinging diathesis in LBP: necrotic material at the periphery of the cell groups in liquid-based preparation) can be seen
Differential Diagnosis
-
1.
Repair. Reparative cells can be large and hyperchromatic with prominent nucleoli but tend to be arranged in flat cohesive sheets with less haphazardly arranged cells and contain less nuclear atypia.
-
2.
LSIL. LSIL cells especially koilocytes can mimic keratinizing squamous cell carcinoma cells with a lower N/C ratio but tend to have less nuclear atypia without background of tumor diathesis.
-
3.
HSIL. HSIL cells with significant nuclear atypia can mimic nonkeratinizing squamous cell carcinoma but rarely have prominent nucleoli, bizarre cell shapes (tadpole and fiber cells), and a tumor diathesis.
-
4.
Benign endometrial cells. Endometrial cells with blood can mimic small cell nonkeratinizing SCC, but they tend to have uniform bean-shaped nuclei without prominent nucleoli. Clinical history of menstrual period may be helpful.
-
5.
Adenocarcinoma. Cervical adenocarcinoma cells tend to have 3D arrangement with glandular formation with delicate, granular, vacuolated cytoplasm, more prominent nucleoli, and less background tumor diathesis.
Atypical Glandular Cells
Definition
Atypical glandular cells represent glandular cells with morphologic changes which fall short of an interpretation of adenocarcinoma either quantitatively or qualitatively. It can be divided into AGC-NOS (not otherwise specified), AGC-EC (endocervical), and AGC-EM (endometrial). AGC denotes an increased level of risk for neoplasia and not a specific precursor lesion.
Morphology (Fig. 11.16)

Atypical glandular cells (liquid-based preparation, LBP). (a) A group of hyperchromatic cells in a glandular architecture with enlarged nuclei. (b) Sheets endocervical glandular cells with ill-defined cell borders, nuclear crowding/overlapping, increased N/C ratio, and vacuoles. (c) Sheets endocervical glandular cells with ill-defined cell borders, nuclear crowding/overlapping, enlarged nuclei with hyperchromasia, and slightly coarse chromatin.Fig. 11.16 (continued) (d) Strips of endocervical glandular cells with enlarged hyperchromatic nuclei, coarse chromatin, and occasional prominent nucleoli. (e) Strips of endocervical glandular cells with enlarged hyperchromatic nuclei and variation in nuclear size and shape. (f) Small cluster of cells with ill-defined cell borders, scant cytoplasm, enlarged nuclei, and occasional small nucleoli. (g) Rare mitosis can be present. (h) Occasional vacuoles can be present
AGC-EC represents endocervical cells with morphologic changes which fall short of an interpretation of endocervical adenocarcinoma in situ or invasive adenocarcinoma either quantitatively or qualitatively.
-
1.
Sheets or strips of endocervical glandular cells with ill-defined cell borders, nuclear crowding/overlapping
-
2.
Increased N/C ratio, but more cytoplasm than atypical endometrial cells
-
3.
Enlarged nuclei with hyperchromasia, moderately coarse chromatin, and occasional mitosis
-
4.
Rare cell groups with rosetting or feathering
AGC-EM represents endometrial cells with morphologic changes which fall short of an interpretation of endometrial adenocarcinoma either quantitatively or qualitatively.
-
1.
Small groups of cells (usually 5–10 cells per group) with ill-defined cell borders, scant cytoplasm, or occasional vacuoles.
-
2.
Nuclei are slightly enlarged compared to normal endometrial cells with mild hyperchromasia and occasional small nucleoli.
Differential Diagnosis
-
1.
Normal endocervical cells . These cells are in honeycomb/palisading arrangements with delicate cytoplasm, small round uniform nuclei, smooth nuclear membranes, and vesicular and evenly distributed chromatin. Nucleoli may be seen in reactive endocervical cells which may have slightly enlarged nuclei with minimal hyperchromasia.
-
2.
Normal endometrial cells . These cells are present in tight three-dimensional cell clusters or loose cell group arrangements with small round/oval/bean-shaped nuclei, fine and evenly distributed chromatin, and minimal/no nuclear atypia.
-
3.
Tubal metaplasia . It represents columnar cells with cilia and/or terminal bars. These cells are in small groups or pseudostratified/crowded groups with round/oval nuclei which may be enlarged, pleomorphic, and hyperchromatic.
Follow-Up Results
AGC can be associated with benign lesions including polyps and metaplasia, but also with neoplasias including adenocarcinomas of the endometrium, cervix, ovary, fallopian tube, and other sites. Follow-up results showed that approximately 20 % of women with AGC prove to have CIN2+, 3 % prove to have adenocarcinoma in situ, and 5 % prove to have invasive adenocarcinoma [16, 17].
Although the cancer risk is lower in women younger than 35 years of age with AGC, the risk of CIN 2+ is higher, and intensive assessment is warranted at all ages. In the KPNC cohort, CIN 3+ was found in 9 % of women aged 30 years and older with AGC cytology, with cancer in 3 %.
Management
The 2012 updated consensus management guidelines recommend women with all subcategories of AGC except atypical endometrial cells to have colposcopy with endocervical sampling regardless of HPV result. In women 35 years of age and older or women younger than 35 years but at increased risk for endometrial neoplasia with all subcategories of AGC, endometrial sampling is recommended in conjunction with colposcopy and endocervical sampling. For women with atypical endometrial cells, initial evaluation with endometrial and endocervical sampling is preferred, but colposcopy is acceptable either at the initial evaluation or deferred.
Adenocarcinoma In Situ
Definition
Endocervical AIS is an in situ tumor without invasion, and it occurs 10–15 years earlier than invasive adenocarcinoma. Since AIS is also associated with HPV infection, it does coexist with CINs in approximately 20–50 % of patients. A diagnosis of AIS on a Pap test does not exclude invasive adenocarcinoma, and a histological examination is necessary for a definitive diagnosis.
Morphology (Fig. 11.17)

Adenocarcinoma in situ (AIS) (liquid-based preparation, LBP). (a) Strip of endocervical cells with indistinct cell borders, nuclear crowding and stratification, enlarged hyperchromatic nuclei, and inconspicuous nucleoli. (b) Small cluster of glandular cells with elongated nuclei, relatively smooth nuclear membrane,Fig. 11.17 (continued) hyperchromasia, evenly distributed chromatin, nuclear stratification, and feathering. (c) Small cluster of glandular cells with nuclear crowding, stratification, and feathering. (d) Large cluster of hyperchromatic group of cells with elongated nuclei, nuclear overlapping, stratification, and occasional small nucleoli. (e) Large cluster of hyperchromatic group of cells with enlarged elongated nuclei and slightly coarse chromatin. (f) Mitosis can be present. (g) Occasional small prominent nucleoli can be present
-
1.
Cells in groups and strips with rosette formation, feathering, crowding, and/or stratification with indistinct cell borders
-
2.
Finely vacuolated cytoplasm
-
3.
Increased N/C ratio
-
4.
Elongated nuclei with smooth to markedly irregular nuclear membrane, hyperchromasia, evenly distributed fine to coarsely granular chromatin, inconspicuous nucleoli, and variable mitosis
Differential Diagnosis
-
1.
Normal/reactive endocervical cells. These cells are in honeycomb/palisading arrangements with delicate cytoplasm, small round uniform nuclei, smooth nuclear membranes, and vesicular and evenly distributed chromatin. Nucleoli may be seen in reactive endocervical cells.
-
2.
Normal endometrial cells. These cells are usually in tight three-dimensional cell clusters or loose cell group arrangements with small round/oval/bean-shaped nuclei, fine and evenly distributed chromatin, and minimal/no nuclear atypia. Feathering, rosettes, and mitoses are not seen.
-
3.
Tubal metaplasia. These cells are columnar cells with cilia and/or terminal bars in small groups or pseudostratified/crowded groups with round/oval nuclei which may be enlarged, pleomorphic, and hyperchromatic.
-
4.
HSIL. HSIL cells can form hyperchromatic crowded groups and have mitoses as AIS cells. However, features of glandular differentiation and feathering are not seen in HSIL cells.
-
5.
Invasive adenocarcinoma. The finding of prominent nucleoli and tumor diathesis favors a diagnosis of invasive adenocarcinoma.
Follow-Up Results
Besides adenocarcinoma, CINs were also found in approximately 20–50 % of women with AIS cells on Pap smear.
Management
The 2012 updated consensus management guidelines recommend women with all subcategories of AIS to have colposcopy with endocervical sampling regardless of HPV result. In women 35 years of age and older or women younger than 35 years but at increased risk for endometrial neoplasia with AIS, endometrial sampling is recommended in conjunction with colposcopy and endocervical sampling.
Adenocarcinoma
Adenocarcinoma cells detected on Pap tests can be from endocervix, endometrium, or extrauterine in origin (vagina, ovaries, fallopian tubes, and metastasis) (Table 11.1).
Morphology
End ocervical Adenocarcinoma (Fig. 11.18)
-
1.
Strips, sheets, or 3D clusters of glandular cells with distinct cell borders and abundant eosinophilic cytoplasm
-
2.
Enlarged nuclei with thickened and undulating irregular nuclear membrane, coarsely granular, hyperchromatic chromatin, and prominent nucleoli (may be multiple and irregular)
-
3.
Necrotic tumor diathesis and/or blood

Endocervical adenocarcinoma (liquid-based preparation, LBP). (a) Endocervical adenocarcinoma cells with markedly enlarged nuclei, pleomorphic shape, irregular coarse chromatin, and prominent macronucleoli. (b) Endocervical adenocarcinoma cells with markedly enlarged nuclei, variation in size and shape, irregularFig. 11.18 (continued) coarse chromatin, and prominent nucleoli. (c) Endocervical adenocarcinoma cells with markedly enlarged nuclei, variation in size and shape, irregular coarse chromatin, prominent macronucleoli, and plenty cytoplasm. (d) Mitosis can be easily seen. (e) Occasional vacuoles can be seen. (f) Necrotic tumor diathesis and pleomorphic tumor cell. (g) Tighter cluster of poorly differentiated endocervical adenocarcinoma cells with less cytoplasm, enlarged pleomorphic nuclei, and prominent nucleoli and tumor diathesis
Endometrial Adenocarcinoma (Fig. 11.19)
-
1.
Single or well-preserved three-dimensional groups of variably sized glandular cells with anisonucleosis and nuclear overlapping/crowding
-
2.
Vacuolated cytoplasm with frequent large vacuoles and polymorphonuclear engulfment
-
3.
Round up nuclei with thickened nuclear membrane, fine to clumped chromatin, and small nucleoli
-
4.
Watery tumor diathesis


Endometrial adenocarcinoma (liquid-based preparation, LBP). (a) Three-dimensional group of variably sized glandular cells with anisonucleosis and nuclear overlapping/crowding, round nuclei, thickened nuclear membrane, fine to clumped chromatin, and small nucleoli. (b) Three-dimensional groups of glandular cells withFig. 11.19 (continued) nuclear overlapping and crowding. (c) 3D group with papillary projection. (d) Cluster of well-differentiated endometrial endometrioid adenocarcinoma cells with slightly enlarged nuclei, scant cytoplasm, nuclear overlapping, and mild coarse chromatin. (e) Cluster of well-differentiated endometrial endometrioid adenocarcinoma cells with variation in size, scant cytoplasm, and mild coarse chromatin. (f) Small group of moderately differentiated endometrial endometrioid adenocarcinoma cells with enlarged nuclei, scant cytoplasm, high N/C ration, and coarse chromatin. (g) Single poorly differentiated endometrial adenocarcinoma cells with markedly enlarged nuclei, irregular nuclear contour, and markedly coarse chromatin. (h) Large vacuoles can be frequent and push nuclei to the periphery. (i) A small cluster of endometrial adenocarcinoma cells with prominent cytoplasmic vacuoles. (s) Small nucleoli and polymorphonuclear engulfment can be seen
Differential Diagnosis
-
1.
Normal/reactive endocervical cells. These cells are in honeycomb/palisading arrangements with delicate cytoplasm, small round uniform nuclei, smooth nuclear membranes, and vesicular and evenly distributed chromatin. Nucleoli may be seen in reactive endocervical cells.
-
2.
Normal endometrial cells. These cells are usually small round/oval/bean-shaped nuclei, fine and evenly distributed chromatin, and minimal/no nuclear atypia.
-
3.
Tubal metaplasia. These cells are columnar cells with cilia and/or terminal bars in small groups or pseudostratified/crowded groups with round/oval nuclei.
-
4.
AIS. AIS cells can have feathering, but with less atypia and inconspicuous nucleoli. The finding of tumor diathesis favors invasive adenocarcinoma.
Normal Endometrial Cells
The risk of endometrial lesions is very low in young women with normal endometrial cells in Pap test. The age to report the normal endometrial cells has been changed from 40 years and above to 45 years and above in the updated 2014 TBS.
Others
Other malignant neoplasms which can occur in Pap tests include some rare variants of cervical adenocarcinoma [villoglandular adenocarcinoma, minimal deviation adenocarcinoma (adenoma malignum), intestinal-type adenocarcinoma, endometrioid cervical adenocarcinoma, clear cell carcinoma, serous carcinoma, mesonephric adenocarcinoma, adenosquamous cell carcinoma, glassy cell carcinoma, adenoid cystic carcinoma and adenoid basal cell carcinoma] and other types of malignant neoplasm [small cell and large cell neuroendocrine carcinomas, extramammary Paget’s disease, metastatic carcinoma (ovarian, colorectal, breast, and other sites), malignant melanoma, lymphoma, myeloid sarcoma, malignant mixed Müllerian tumor, rhabdomyosarcoma, leiomyosarcoma, Ewing sarcoma, and gestational trophoblastic diseases]. These entities are very rare and are not detailed here.
References
Gustafsson L, Ponten J, Bergstrom R, Adami HO. International incidence rates of invasive cervical cancer before cytological screening. Int J Cancer. 1997;71:159–65.
Gustafsson L, Ponten J, Zack M, Adami HO. International incidence rates of invasive cervical cancer after introduction of cytological screening. Cancer Causes Control. 1997;8:755–63.
Janerich DT, Hadjimichael O, Schwartz PE, et al. The screening histories of women with invasive cervical cancer, Connecticut. Am J Public Health. 1995;85:791.
Abed Z, O’Leary M, Hand K, et al. Cervical screening history in patients with early stage carcinoma of the cervix. Ir Med J. 2006;99:140.
Papanicolaou GN, Traut HF. The diagnostic value of vaginal smears in carcinoma of the uterus. Am J Obstet Gynecol. 1941;42:193.
The 1988 Bethesda System for reporting cervical/vaginal cytological diagnoses. National Cancer Institute Workshop. JAMA 1989;262:931.
Broder S. From the National Institutes of Health. JAMA. 1992;267:1892.
Solomon D, Davey D, Kurman R, et al. The 2001 Bethesda System: terminology for reporting results of cervical cytology. JAMA. 2002;287:2114.
Zhao C, Moriarty AT, Ghofrani M, et al. Human papillomavirus testing and reporting rates in 2012: results of a College of American Pathologists’ National Survey. Arch Pathol Lab Med. 2015;139(6):757–61.
Bandyopadhyay S, Austin RM, Dabbs D, Zhao C. Adjunctive human papillomavirus DNA testing is a useful option in some clinical settings for disease risk assessment and triage of females with ASC-H Papanicolaou test results. Arch Pathol Lab Med. 2008;132(12):1874–81.
Cohen D, Austin RM, Gilbert C, Freij R, Zhao C. Follow-up outcomes in a large cohort of patients with human papillomavirus-negative ASC-H cervical screening test results. Am J Clin Pathol. 2012;138(4):517–23.
Heider A, Austin RM, Zhao C. HPV test results stratify risk for histopathologic follow-up findings of high-grade cervical intra-epithelial neoplasia in women with low-grade squamous intra-epithelial lesion Pap results. Acta Cytol. 2011;55(1):48–53.
Barron S, Austin RM, Li Z, Zhao C. Follow-up outcomes in a large cohort of patients with HPV-negative LSIL cervical screening test results. Am J Clin Pathol. 2015;143(4):485–91.
Barron S, Li Z, Austin RM, Zhao C. Low-grade squamous intraepithelial lesion/cannot exclude high-grade squamous intraepithelial lesion (LSIL-H) is a unique category of cytologic abnormality associated with distinctive HPV and histopathologic CIN 2+ detection rates. Am J Clin Pathol. 2014;141(2):239–46.
Gao FF, Austin RM, Zhao C. Histopathologic follow-up and human papillomavirus DNA test results in 290 patients with high-grade squamous intraepithelial lesion Papanicolaou test results. Cancer Cytopathol. 2011;119(6):377–86.
Zhao C, Florea A, Austin RM. Clinical utility of adjunctive high-risk human papillomavirus DNA testing in women with Papanicolaou test findings of atypical glandular cells. Arch Pathol Lab Med. 2010;134(1):103–8.
Zhao C, Florea A, Onisko A, Austin RM. Histologic follow-up results in 662 patients with Pap test findings of atypical glandular cells: results from a large academic womens hospital laboratory employing sensitive screening methods. Gynecol Oncol. 2009;114(3):383–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Li, Z., Zhao, C. (2016). Cytology of Cervical Precancerous Lesions. In: Fadare, O. (eds) Precancerous Lesions of the Gynecologic Tract. Springer, Cham. https://doi.org/10.1007/978-3-319-22509-8_11
Download citation
DOI: https://doi.org/10.1007/978-3-319-22509-8_11
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-22508-1
Online ISBN: 978-3-319-22509-8
eBook Packages: MedicineMedicine (R0)